Paeds · fetal-neonatal-and-perinatal
Necrotising enterocolitis and spontaneous intestinal perforation
Also known as Necrotising enterocolitis · NEC · Spontaneous intestinal perforation · Focal intestinal perforation · Neonatal bowel perforation
Fellowship guide to the two neonatal intestinal emergencies that end in bowel perforation: necrotising enterocolitis (NEC) and spontaneous intestinal perforation (SIP). Covers modified Bell staging, the dysbiosis-inflammation pathophysiology of NEC versus the focal muscularis injury of SIP, radiograph interpretation, the medical bundle, the surgical triggers and the peritoneal-drainage-versus-laparotomy decision, and the prevention bundle.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 26-week, 780 g infant on day 9 of life, established on enteral formula feeds, develops increasing gastric residuals, a distended and tender abdomen, and apnoeic spells. The abdominal radiograph shows bubbly lucency in the bowel wall. This is necrotising enterocolitis (NEC) — the archetypal inflammatory necrosis of the immature intestine, and one of the few remaining killers of preterm infants that prevention, not treatment, has substantially changed. [3]
NEC is defined as transmural inflammatory necrosis of the bowel wall with a characteristic radiological and clinical signature: pneumatosis intestinalis (gas in the bowel wall), a septic systemic course, and a predilection for the terminal ileum and proximal colon. It is overwhelmingly a disease of the preterm infant — prematurity is the single strongest risk factor — and it typically declares itself between the second day and the end of the first month of life, almost always after enteral feeding has begun. [3] [8]
Spontaneous intestinal perforation (SIP), also called focal intestinal perforation, is a separate entity that produces the same dramatic finding — free air in the abdomen — by a different mechanism. It is a single, isolated, often pinpoint perforation, usually at the anti-mesenteric border of the terminal ileum, with little or no surrounding necrosis and minimal inflammation. The infant is frequently haemodynamically stable, and the perforation is often an incidental finding on a radiograph taken for another reason. SIP is concentrated in the extremely-low-birth-weight (ELBW) infant and has become, in some networks, the commonest surgical bowel lesion in that group. [7] [12]
The two are taught together for one reason: both culminate in bowel perforation, and telling them apart at the cot-side changes prognosis, surgical strategy, and counselling. NEC is a disease of the bowel wall that you must stop feeding, treat medically, and operate on for the complication of perforation. SIP is a hole in a focally weak wall that you can often drain and close without the septic inflammation that defines NEC. [7] [13]
Epidemiology & Risk Factors
Prematurity is the engine of both diseases. NEC affects roughly 5–10% of very-low-birth-weight (VLBW) infants and about 1 per 1000 live births overall, with a steep inverse gestational-age gradient: the more premature the infant, the higher the incidence and the higher the mortality. SIP is even more tightly bound to extreme prematurity, clustering in ELBW infants (under 1000 g) in the first week or two of life. [3] [7]
For NEC, the risk factors fall into four groups. Immaturity of the gut is foundational — a thin mucosa, sparse mucus, low secretory IgA, and disordered motility. Enteral substrate matters: formula feeding, rapid feed advancement, hypertonic feeds and medications all raise risk, while human milk is dose-dependently protective. Dysbiosis is the microbiological driver: the preterm gut is colonised by pro-inflammatory Proteobacteria and loses protective bifidobacteria. Hypoxia and ischaemia, a patent ductus arteriosus with steal, indomethacin, exchange transfusion, polycythaemia, and congenital heart disease all add perfusion-related risk. [3] [6]
For SIP the risk profile is narrower and more iatrogenic. The dominant modifiable association is early postnatal indomethacin combined with postnatal glucocorticoid — used together for PDA closure and lung disease, they impair mucosal restitution and mesenteric perfusion at exactly the focally vulnerable terminal ileum. A focal defect or thinning of the muscularis propria underlies the perforation. Importantly, antenatal corticosteroids do not raise SIP risk; the signal is for postnatal indomethacin plus postnatal steroid. [11] [12]
The protective factors are the prevention bundle in miniature, and they are the evidence points the examiner rewards: own mother's milk (dose-dependent protection; donor human milk also reduces NEC versus formula), antenatal corticosteroids, standardised feeding protocols, and — with strain-specific and regional caution — probiotics. The incidence of NEC has fallen over three decades on the back of exactly this bundle. [6] [9]
Pathophysiology
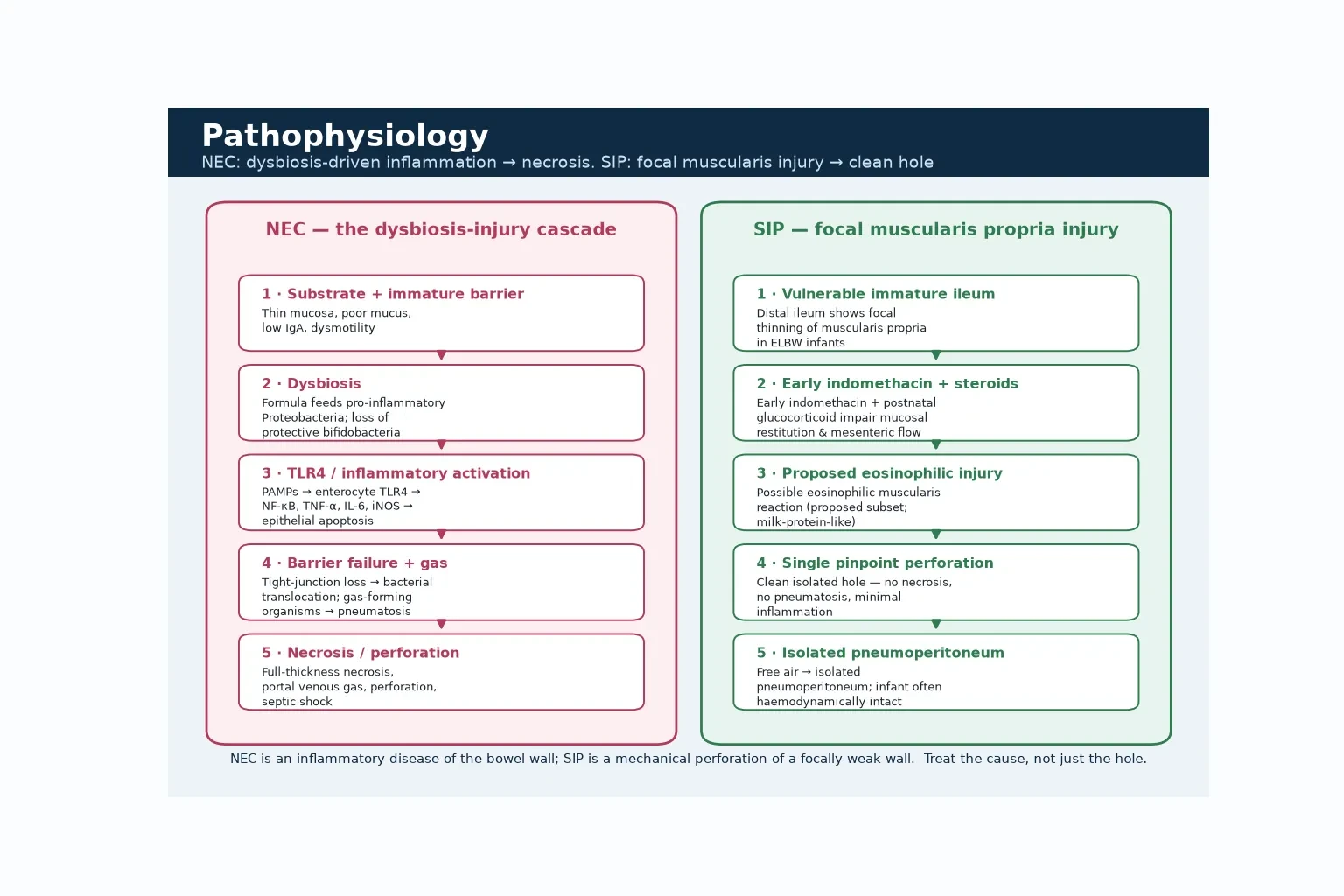
NEC is the convergence of an immature gut, an abnormal microbiome, and a substrate that feeds the wrong organisms, igniting an innate immune response that destroys the bowel wall. Hold that cascade in your head and every clinical and radiological sign becomes predictable. [3]
The preterm gut is structurally and functionally unready. The mucosa is thin, the mucus layer sparse, secretory IgA low, and motility disordered. The immature enterocyte expresses high levels of TLR4, the receptor for bacterial lipopolysaccharide. When dysbiosis delivers pro-inflammatory organisms — classically Proteobacteria — alongside a formula substrate that feeds them, TLR4 is activated, driving NF-κB-mediated inflammation and release of TNF-α, IL-6, IL-1β and inducible nitric oxide synthase. The result is epithelial apoptosis, tight-junction disruption, vasoconstriction and ischaemic necrosis. [3]
Two radiological signs fall straight out of this mechanism. Pneumatosis intestinalis — gas in the bowel wall — forms when gas-forming organisms enter the submucosa and subserosa through the disrupted mucosa. Portal venous gas forms when intramural gas enters the mesenteric venous system and tracks into the portal tree. Both are signs that the wall is breached; portal gas additionally marks severe, often pan-intestinal disease. [3] [1]
SIP is a different story. Here the problem is a focal weakness of the muscularis propria at the terminal ileum — described as focal thinning or a defect — compounded by early postnatal indomethacin (impaired mucosal restitution and mesenteric vasoconstriction) and postnatal glucocorticoid. A proposed eosinophilic, milk-protein-like muscularis reaction is described in a subset. The perforation is therefore a single, clean, isolated hole rather than a field of necrosis, which is why there is no pneumatosis, no portal gas, and often minimal systemic sepsis. [11] [12]
The clinical tempo follows the mechanism. NEC worsens over hours as inflammation and ischaemia extend through the wall, producing the toxic, septic, deteriorating infant. SIP declares itself more discretely — the perforation happens, free air escapes, and the infant may look well apart from that one catastrophic radiograph finding. [7] [3]
Classification
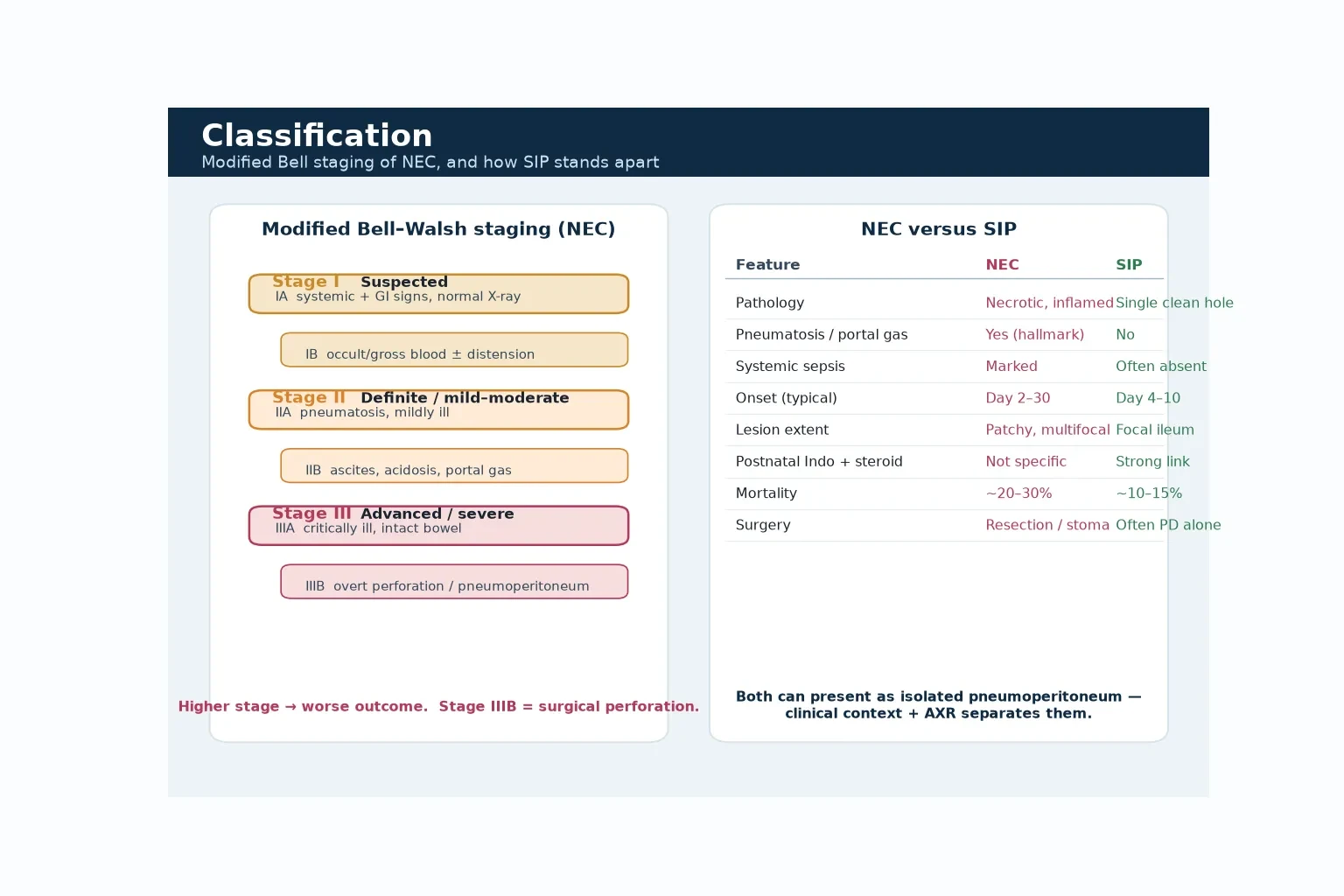
The classification that the examiners expect is the modified Bell staging system (Bell 1978, modified by Walsh and Kliegman 1986), which grades NEC by the depth of clinical and radiological involvement. It is the framework that decides escalation, and it pairs the systemic, gastrointestinal and radiological features at each level. [1] [2]
Stage I — Suspected NEC. Systemic signs (temperature instability, apnoea, lethargy) and gastrointestinal signs (gastric residuals, distension, occult or gross blood) with a normal or nonspecific radiograph. This is the infant you stop feeding and start investigating. [1]
Stage II — Definite NEC. Pneumatosis intestinalis appears on the radiograph — the hallmark. IIA is mild disease (intact bowel, mildly ill infant); IIB is moderate disease with ascites, acidosis, portal venous gas, a palpable abdominal mass or a fixed loop. This is the stage where the medical bundle is intensive and surgical review begins. [2]
Stage III — Advanced NEC. Critically ill. IIIA is severe disease with an intact bowel (shock, acidosis, peritonitis, DIC); IIIB is overt bowel perforation with pneumoperitoneum — the surgical stage. The suffix logic is important: A denotes an intact bowel (medical), B denotes perforation or gas requiring surgical intervention. [1] [2]
SIP does not sit on the Bell ladder — it is a separate diagnosis — but the practical point is that an isolated pneumoperitoneum in a well infant is SIP, whereas the same pneumoperitoneum in a toxic infant with pneumatosis is Stage IIIB NEC. Mislabelling one as the other changes everything. [7] [12]
NEC versus SIP — the bedside discriminator
- Inflammatory, patchy, transmural necrosis
- Pneumatosis and portal venous gas hallmark
- Septic, toxic, deteriorating infant
- Onset day 2–30; multifocal disease
- Laparotomy with resection; mortality ~20–30%
- Single clean isolated hole, terminal ileum
- No pneumatosis, no portal gas
- Infant often haemodynamically stable
- Onset day 4–10; focal disease
- Often peritoneal drainage alone; mortality ~10–15%
Clinical Presentation
The classical NEC presentation is the preterm infant who was feeding and now isn't. The earliest signs are feeding intolerance and increasing gastric residuals, followed by abdominal distension, tenderness, and bilious or bloody aspirates and stools. Systemic instability appears early: temperature instability, apnoea and bradycadia, and lethargy. The picture is of an infant who is becoming septic in front of you, with an abdomen that is the source. [3] [1]
As NEC progresses, the abdominal signs become striking. Look for abdominal wall erythema and oedema, a palpable mass (the fixed, necrotic loop), absent bowel sounds, and a tender, shiny abdomen. Systemically the infant develops hypotension, metabolic acidosis, thrombocytopenia, coagulopathy and oliguria — the picture of septic shock with peritonitis. In the extreme, the abdomen becomes discoloured and the infant is in extremis. [1] [3]
SIP presents differently and that difference is the diagnostic clue. The ELBW infant, typically day 4 to 10, is found to have a pneumoperitoneum on a radiograph taken for another reason — often a baby who is otherwise stable, on minimal support, with little systemic upset. There may be mild abdominal distension, but the dramatic toxicity of NEC is absent. The examiner wants exactly this contrast: the well infant with an unexpected hole. [7] [12]
NEC onset — feed, fail, flare
Atypical presentations keep the differential honest. A term infant with congenital heart disease, or an infant in the days after cardiac surgery, may develop an ischaemic NEC driven by low gut perfusion rather than dysbiosis; mortality is high. Cow's-milk-protein enterocolitis in a term infant can mimic early NEC with bloody stools and distension, but the infant is systemically well and the treatment is dietary exclusion, not antibiotics and surgery. [3]
Differential Diagnosis
When a preterm infant develops feeding intolerance and abdominal distension, NEC sits at the top of a structured list — but the other members must be held in parallel, because the treatment diverges. The disciplined approach is to ask first whether this is surgical or medical, then whether it is inflammatory or obstructive, then whether it is septic or allergic. [3] [1]
The common differentials are late-onset sepsis with ileus (no pneumatosis, positive blood culture), viral enteritis (rotavirus, norovirus, adenovirus — a unit outbreak is the clue), cow's-milk-protein allergy (well infant, bloody stools, responds to exclusion), and constipation. The surgical mimics are Hirschsprung-associated enterocolitis, malrotation with volvulus (bilious vomiting, proximal obstruction, a paucity of distal gas), and intestinal atresia. Metabolic acidosis of any cause can produce a similar picture of instability. [3]
The NEC-versus-SIP discrimination is the highest-yield differential in the topic, and it rests on three axes. Radiology: pneumatosis and portal gas mean NEC; an isolated pneumoperitoneum with a clean bowel wall favours SIP. Systemic state: a toxic, septic, deteriorating infant is NEC; a stable infant is SIP. Timing and risk: day 2–30 after feeds in a formula-fed preterm is NEC; day 4–10 in an ELBW infant exposed to early indomethacin and steroid is SIP. [7] [12]
A free-air pitfall worth naming: pneumoperitoneum can be tracked respiratory air from a lung air-leak rather than gut perforation. A paracentesis showing air under tension, or bile or faecal material, points to the gut and warrants surgery; otherwise the tracked air is absorbed. The infant with a lung leak is usually well, like SIP, but the mechanism and the chest signs separate them. [3]
Clinical & Bedside Assessment
The focused assessment of a suspected NEC infant follows a fixed order so that escalation is never delayed. Inspect the abdomen for distension, asymmetry, wall erythema, oedema and discolouration. Palpate gently for tenderness, guarding, a palpable mass (the fixed loop) and abdominal wall fullness. Auscultate for bowel sounds, which diminish or disappear as the ileus of NEC deepens. Then assess perfusion: capillary refill, blood pressure, pulse quality and temperature of the peripheries. [1] [3]
Serial observation is how you detect the slide towards perforation. Measure abdominal girth at a marked point at each assessment — it is non-specific but a rising trend is a warning. Monitor gastric residuals and their character (bilious, bloody), but recognise that residuals are unreliable in healthy infants and must be interpreted with the whole picture. Trend the platelet count, acid-base status, CRP and gas exchange; falling platelets, worsening acidosis and rising ventilator need are the biochemical signature of deterioration. [3]
The decision to escalate to surgery rests on the surgical trigger: a new pneumoperitoneum, a fixed and persistent loop with clinical deterioration, abdominal wall discolouration with shock, or a positive diagnostic paracentesis. The discipline is to re-examine on a schedule (often every 6 to 12 hours in established NEC) and to image and re-image with that trigger in mind. [1] [13]
SIP declares itself by exception. The ELBW infant with an incidental pneumoperitoneum who is otherwise stable — perfusing well, ventilating comfortably, no acidosis — is the SIP pattern, and the absence of the NEC toxicity is itself the finding. Recognising this spares the infant an aggressive NEC workup and an over-cautious family conversation. [7] [12]
Communication is part of the bedside skill, not an add-on. When an infant is deteriorating towards perforation, brief the surgical team early, update the nurse coordinator, and begin the family conversation before the operating theatre is the only option. NEC and SIP carry very different prognoses, and an accurate working diagnosis shapes what you say. [13]
Investigations
The abdominal radiograph is the principal investigation and the one the examiner will probe. The hallmark sign is pneumatosis intestinalis — bubbly or linear lucency within the bowel wall, most often in the terminal ileum and proximal colon. Portal venous gas appears as branching lucency over the liver and marks severe disease. Ascites, a dilated asymmetrical bowel gas pattern, and a fixed loop (a loop that looks identical on serial films) are the supporting signs. [3] [1]
The fixed loop deserves emphasis because it is under-recognised and high-yield. A dilated loop of bowel that does not change position or calibre on serial radiographs over 24 hours indicates full-thickness necrosis — the loop is paralysed because its wall is dead — and it is a marker of impending perforation even before free air appears. Seeing a fixed loop should prompt urgent surgical review. [1] [13]
Pneumoperitoneum confirms perforation. On a supine film look for Rigler's football sign (a large oval lucency outlining the abdomen), lucency over the right liver edge, the falciform ligament sign, and, in males, scrotal air. When the supine film is equivocal, a lateral decubitus or cross-table lateral view with the right side up lets free air collect over the liver and become visible. [3]
Laboratory tests support severity rather than diagnosing NEC. Look for metabolic acidosis, thrombocytopenia, neutropenia or a left shift, rising CRP, coagulopathy and hyponatraemia. Blood, CSF and stool cultures guide antibiotic choice and duration, and inflammatory markers trend with the course. Abdominal ultrasound, in experienced hands, shows a thickened hyperechoic bowel wall, intramural gas, ascites and absent Doppler flow in necrotic segments — a useful adjunct when radiography is equivocal. [3]
The key timing principle is that imaging does not delay resuscitation or surgical review. The deteriorating infant with peritonitis is a clinical Stage III; the radiograph confirms perforation but the call to the surgeon is made on the clinical picture and the fixed loop, not on waiting for free air. [1] [13]
Management — Resuscitation
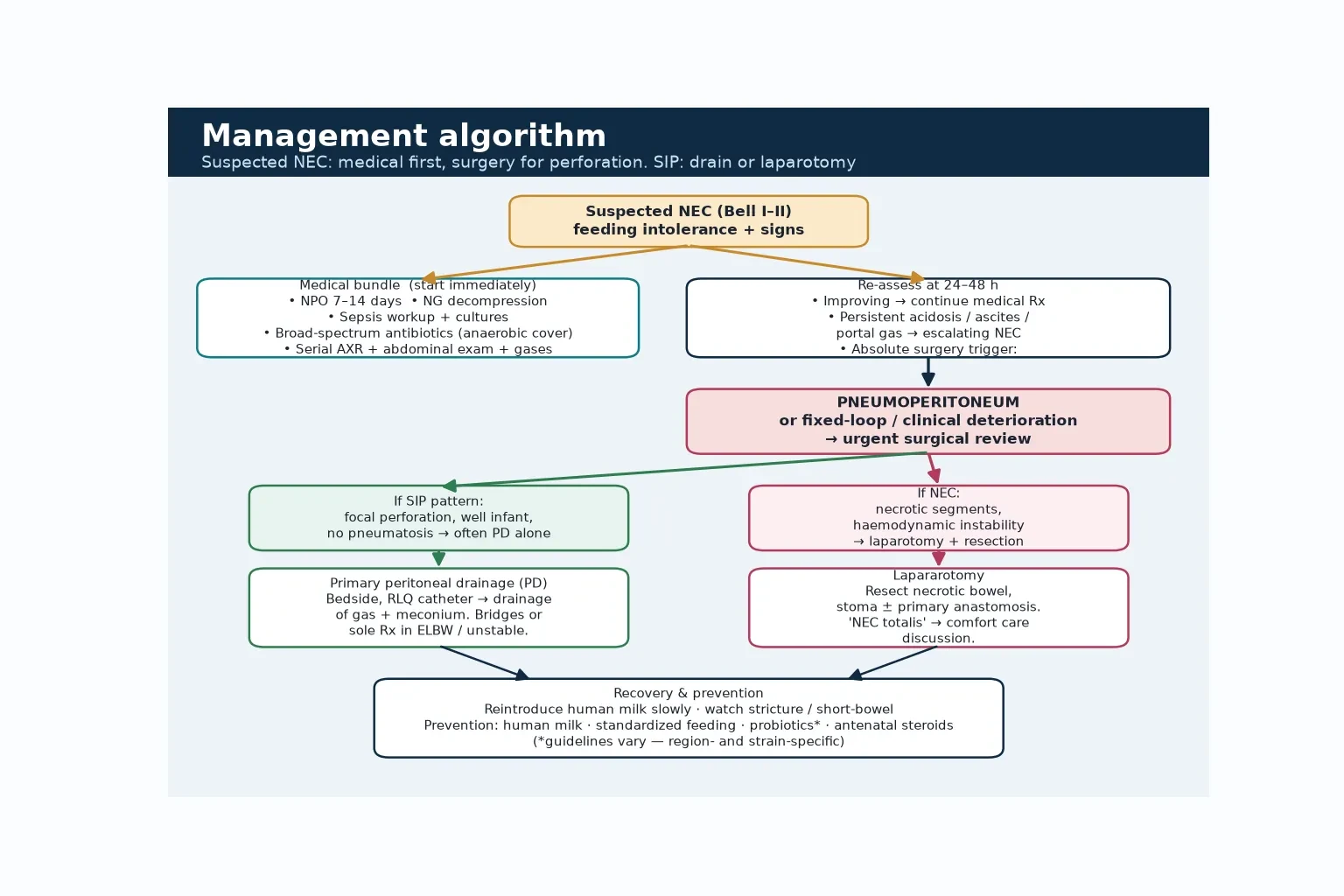
The moment NEC is suspected, start the medical bundle and do not wait for radiographic confirmation. Make the infant nil by mouth (NPO) for 7 to 14 days depending on stage, pass a large-bore nasogastric tube for free drainage and decompression, take blood, CSF and urine cultures, and start broad-spectrum antibiotics with anaerobic cover. [1] [3]
Antibiotic choice must cover the organisms that translocate through a necrotic wall: a broad gram-negative agent plus anaerobic cover with metronidazole or clindamycin, adjusted to local resistance patterns and to any positive cultures. The duration mirrors the stage — typically 7 to 14 days for established NEC — and is prolonged if perforation or ongoing sepsis is present. [3]
Resuscitate the shocked NEC infant in parallel. Give isotonic fluid boluses (10 mL/kg normal saline, repeated to effect), add inotropes for hypotension, correct acidosis and coagulopathy with bicarbonate and blood products, and provide respiratory support for the infant who is tiring or apnoeic. The goal is to stabilise perfusion so that, if surgery is needed, the infant is a viable candidate. [1] [3]
The SIP resuscitation is usually lighter because the infant is often stable. The priority is to drain the pneumoperitoneum — frequently by primary peritoneal drainage — and to give targeted antibiotics, with less of the profound sepsis resuscitation that NEC demands. Diagnostic paracentesis is reserved for the infant where the diagnosis is unclear: brown or bile-stained fluid, or bacteria on Gram stain, indicates necrotic or perforated bowel and pushes towards laparotomy. [4] [12]
Management — Definitive & Stepwise
Definitive management follows a stepwise ladder built on the modified Bell stage and on the surgical trigger. The rungs are: intensive medical management for Stage I and II, surgical review at the trigger, and a choice between primary peritoneal drainage (PD) and laparotomy for the infant with perforation or a deteriorating fixed loop. [1] [4]
Intensive medical management is the treatment for Stage I and most Stage II disease: NPO, gastric decompression, broad-spectrum antibiotics with anaerobic cover, meticulous fluid and perfusion management, and serial clinical and radiological reassessment. Many infants with Stage IIB disease recover without surgery, and the discipline is to re-examine and re-image on a schedule that catches the slide towards perforation. [3]
Surgery is required for Stage IIIB (perforation) and for the deteriorating Stage IIIA infant with a fixed loop or positive paracentesis. The choice between primary peritoneal drainage and laparotomy is individualised, and the evidence is more nuanced than the algorithm suggests. The NET trial (Rees 2008) randomised ELBW infants with perforated NEC to PD or laparotomy and found that PD did not improve survival or short-term outcomes compared with laparotomy — the choice rests on size, stability, likely diagnosis and surgeon preference. [4] [5]
Primary peritoneal drainage is a bedside procedure: a catheter placed in the right lower quadrant drains gas and meconium, relieving the perforation and buying time. It is used as a bridge to laparotomy or as sole therapy in ELBW or unstable infants. Laparotomy allows resection of necrotic bowel, stoma formation, or a primary anastomosis in selected cases, and is the definitive operation for established NEC. NEC totalis — pan-intestinal necrosis — has a grim prognosis and prompts a comfort-care discussion with the family. [4] [13]
Management ladder for suspected NEC and SIP
Suspect NEC on feeding intolerance + signs: NPO 7–14 days, large-bore NG decompression, cultures, broad-spectrum antibiotics with anaerobic cover
Resuscitate the shocked infant: 10 mL/kg saline boluses, inotropes, correct acidosis and coagulopathy, respiratory support
Serial reassessment: abdominal exam and girth, bloods (platelets, gas, CRP), abdominal radiograph every 6–12 h
Meet the surgical trigger (pneumoperitoneum, fixed deteriorating loop, wall discolouration with shock, positive paracentesis): call the surgeon in parallel with resuscitation
For perforation: choose primary peritoneal drainage (bedside; ELBW / unstable) versus laparotomy (resection, stoma) — individualise using the NET trial evidence
For a well ELBW infant with isolated pneumoperitoneum (SIP): PD alone is often definitive; anaerobic-cover antibiotics
Recovery: slow re-introduction of human milk; watch for stricture and short-bowel syndrome
Apply the prevention bundle: own mother's milk, standardised feeding, probiotics (strain/region-specific), antenatal steroids, cautious feed advancement
The prevention bundle is the closing answer in every viva and the one the examiner rewards. State it as a list: own mother's milk (the single most evidence-based prevention, dose-dependent), standardised feeding protocols (reduce practice variation and NEC), probiotics (strain-specific; meta-analyses show benefit but probiotic sepsis and regional caution limit universal use), antenatal corticosteroids, and cautious feed advancement with avoidance of hypertonic feeds and medications. [6] [9]
The escalation pathway has defined triggers. A persistent or worsening metabolic acidosis, rising ventilator need, falling platelets, a fixed loop, or new pneumoperitoneum each warrant escalation of both the medical intensity and the surgical involvement. Infants needing surgery, especially those with perforated NEC or NEC totalis, must be managed in (or retrieved to) a tertiary surgical NICU. [13]
Specific Subtypes & Scenarios
SIP in the well ELBW infant on day 5 is the scenario the examiners love because it tests the discriminator. The infant is relatively stable, the radiograph shows an isolated pneumoperitoneum, and there is no pneumatosis or portal gas. The right answer is to recognise SIP, drain it (often definitively with PD), give targeted antibiotics, and counsel the family on a markedly better prognosis than perforated NEC. Over-treating this infant with an aggressive NEC laparotomy is the trap. [7] [12]
NEC totalis is the other extreme. Pan-intestinal necrosis — the entire small bowel dusky and dead at laparotomy — carries a mortality approaching 100% and a survivor outcome of catastrophic short-bowel syndrome. The recognition point is the rapidly deteriorating infant with severe acidosis, profound shock, and a diffuse abdominal radiograph. The management decision, made with the family, is whether to operate at all; a comfort-care pathway is a legitimate and often correct choice. [3] [13]
The term infant with congenital heart disease, or the infant days after cardiac surgery, develops an ischaemic NEC driven by low gut perfusion rather than dysbiosis. The presentation is similar but the mechanism differs, the mortality is high, and the prevention and management lean on haemodynamic optimisation as much as on feeding strategy. [3]
In a low-resource setting, the challenge is diagnostic and infrastructural. Clinical diagnosis replaces serial radiography, drainage is improvised where surgical capacity is limited, and the emphasis shifts to the prevention bundle — human milk, antenatal steroids, and standardised feeding — which does not depend on expensive technology. [3] [6]
The infant with an indwelling central line and thrombocytopenia may have catheter-related sepsis with ileus that coexists with early NEC. The discipline is to treat both possibilities: take the cultures, remove the line if infected, start the NEC medical bundle, and reassess with serial imaging. [3]
The retrieval or transport of a ventilated infant with suspected NEC requires specific preparation: maintain NPO, secure gastric decompression, continue antibiotics, stabilise perfusion before departure, and transport to a tertiary surgical NICU. Careful handling avoids extending a contained perforation. [13]
Complications & Pitfalls
The early complications of NEC are the surgical and septic consequences of a perforated, necrotic bowel: perforation with peritonitis, septic shock, disseminated intravascular coagulation, and acute kidney injury. Operative complications include wound infection, stoma complications (retraction, prolapse, necrosis) and intra-abdominal sepsis. The infant who survives the acute episode then faces the late consequences. [3] [13]
The late complications drive long-term morbidity. Intestinal strictures develop in roughly 10 to 20% of surgical survivors, presenting weeks later with obstruction and requiring contrast study and resection. Short-bowel syndrome and intestinal failure follow extensive resection, with dependence on parenteral nutrition, line sepsis, and cholestasis from prolonged TPN. Neurodevelopmental impairment is common and worse than in gestational-age-matched controls without NEC. [3]
The classic errors each have a name and a consequence. Labelling an incidental isolated pneumoperitoneum as perforated NEC over-treats a SIP infant and misleads the family — the well infant with a clean pneumoperitoneum is SIP. Missing an early fixed loop delays surgical review; the loop that does not change on serial films is dead bowel. Failing to get anaerobic cover undertreats the translocating organisms. Waiting for a "classic" football sign before calling the surgeon delays the operation. [1] [7]
The medicolegal and safety pitfall is failing to document. The serial abdominal exams, the radiograph findings, the decision to operate (or not), the surgical trigger that was met, and the family discussion — especially in NEC totalis — must all be recorded. In a case that later comes to review, the contemporaneous record that the trigger was recognised and the family was counselled is the defence. [13]
Prognosis & Disposition
Outcome is determined by four factors: gestational age (the more premature, the worse), the extent of disease (pan-necrosis versus localised), the speed of recognition and surgery, and the complications of prematurity (IVH, PDA, sepsis) that travel alongside. Overall NEC mortality is roughly 20 to 30%, higher in ELBW and surgical disease; SIP mortality is lower, around 10 to 15%. [3] [7]
The poor-outcome predictors are the variables the examiner wants named: lower gestational age, surgical rather than medical disease, portal venous gas, severe metabolic acidosis, thrombocytopenia, the need for inotropes, and pan-necrosis. SIP carries a better outlook precisely because it lacks the septic, inflammatory burden of NEC. [3] [12]
The disposition follows the surgical capability required. A ventilated infant with NEC needs a tertiary surgical NICU. An ELBW infant with SIP managed by PD may be managed in a surgical-capable unit with retrieval available if deterioration occurs. After recovery, the infant enters growth and nutrition monitoring (for short-bowel syndrome), neurodevelopmental follow-up, and surgical review for stricture (a contrast study if obstructive symptoms appear) and stoma reversal planning. [13]
Recovery is slow. After 7 to 14 days of NPO, human milk is reintroduced cautiously and advanced slowly, watching for recurrence or obstruction. Re-operation is triggered by stricture, stoma complications, or failure to wean from parenteral nutrition. The long-term neurodevelopmental outlook is worse than for gestational-age-matched controls without NEC, and these infants enter the standard high-risk preterm follow-up programme. [3]
Special Populations
The extremely preterm and ELBW infant is the population in whom both NEC and SIP concentrate, and where SIP has become proportionally dominant as NEC prevention has improved. The risk is highest, the mortality is highest, and the surgical decision is most often peritoneal drainage first. This is the infant the topic is really about. [3] [7]
The term infant with congenital heart disease or post-cardiac surgery develops an ischaemic NEC pattern with a different mechanism — low gut perfusion rather than dysbiosis — a high mortality, and a management emphasis on haemodynamic optimisation. The prevention and feeding strategy must account for the cardiac lesion. [3]
The growth-restricted or gut-ischaemic infant carries impaired mesenteric perfusion that adds to NEC risk; antenatal growth restriction is a contributor to the risk profile alongside prematurity. [3]
The infant requiring retrieval needs NPO and decompression maintained, antibiotics continued, perfusion stabilised before departure, and transport to a surgical NICU. Altitude and pressure changes in air transport can expand a pneumoperitoneum, so a functioning drain must be in place before flight if there is free air. [13]
In a low-resource setting, the approach relies on clinical diagnosis and on the prevention bundle that does not depend on expensive technology: human milk, antenatal steroids, and standardised feeding. The equity gap in access to neonatal surgery is a real determinant of outcome. [6]
For Indigenous and remote-area preterm populations in ANZ, higher preterm birth rates and reduced access to tertiary surgical care compound risk. The transport logistics and the equity of access to a surgical NICU are legitimate exam points and advocacy themes. [6] [13]
Evidence, Guidelines & Regional Differences
The evidence base for NEC prevention is one of the strongest in neonatology. Donor human milk versus formula reduces NEC in VLBW and very-preterm infants, with a roughly halved risk in the Cochrane review (Quigley 2024) — supporting human milk as the cornerstone of prevention, whether own mother's milk or pasteurised donor milk. [6]
The probiotic evidence is positive but contested. Meta-analyses show reduced NEC and all-cause mortality with probiotic supplementation (Abdullahi 2025), but probiotic sepsis in preterm neonates (Kulkarni 2022) has driven strain-specific and regional caution. Australia, Aotearoa New Zealand and Canada have particularly guarded positions on specific strains, and the probiotic question is exactly the kind of "name the evidence and the controversy" probe the examiner uses. [9] [10]
On surgery, the NET trial (Rees 2008) and its follow-up (Rees 2010) established that primary peritoneal drainage did not stabilise ELBW infants with perforated bowel or improve outcomes versus laparotomy — the choice is individualised, and drainage is a bedside option for the smallest or most unstable infant rather than a superior strategy. [4] [5]
Regional guidance aligns on the prevention bundle and the surgical-trigger principle but differs in detail. ANZ leans on human-milk-based, parent-directed prevention and a strong neonatal retrieval network; the UK emphasises neonatal networks and quality-improvement initiatives around standardised feeding and NEC reduction; the US (AAP) supports human milk and standardised feeding; Canada (CPS) has been particularly cautious on probiotic strains. [6] [9]
All four regions converge on human milk, antenatal steroids and standardised feeding as prevention, and on the surgical trigger for pneumoperitoneum or a fixed deteriorating loop. The divergence is on probiotics: meta-analytic benefit is tempered by probiotic-sepsis case reports, and ANZ and Canada have been the most cautious about specific strains. For exams, cite the human-milk Cochrane evidence and name the regional probiotic caution. [9] [10]
The diagnostic-terminology controversy is worth knowing. "Spontaneous intestinal perforation" and "focal intestinal perforation" are used variably for the same entity, and the distinction from NEC matters for prognosis and counselling. The well ELBW infant with an isolated clean perforation has SIP, with a markedly better outlook than perforated NEC — and the name you give it shapes the conversation with the family. [7] [12]
Exam Pearls
The mechanism one-liner: NEC is inflammatory necrosis of the bowel wall driven by dysbiosis and TLR4 signalling; SIP is a single clean perforation of a focally weak muscularis — both end in a hole, but the cause changes everything. [3] [11]
The modified Bell staging one-liner: Stage I suspected, Stage II definite (IIA mild, IIB moderate with portal gas), Stage III advanced (IIIA severe intact bowel, IIIB perforation). The A/B suffix separates intact bowel from perforation. [1] [2]
The radiograph one-liners: pneumatosis intestinalis is the hallmark of NEC; portal venous gas marks severe disease; a fixed loop means dead bowel; pneumoperitoneum confirms perforation. [3]
The discriminator one-liner: a toxic preterm with pneumatosis and sepsis is NEC; a well ELBW infant with an isolated pneumoperitoneum is SIP. Name it before you treat it. [7] [12]
The SIP exposure one-liner: early postnatal indomethacin plus postnatal glucocorticoid is the modifiable risk — antenatal steroids do not raise SIP risk. [11]
The surgery one-liner: pneumoperitoneum, a fixed deteriorating loop, or a positive paracentesis is the trigger; PD is the bedside option in ELBW or unstable infants; the NET trial showed no survival advantage of PD over laparotomy. [4] [5]
The prevention one-liner: own mother's milk (dose-dependent) is the single most evidence-based prevention, with standardised feeding, probiotics (strain and region-specific), antenatal steroids, and cautious feed advancement completing the bundle. [6] [9]
The classic viva trap: labelling an incidental isolated pneumoperitoneum in a well ELBW infant as perforated NEC. The counter-trap is missing an early fixed loop and delaying surgery. [7] [1]
References
- [1]Bell MJ Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg, 1978.PMID 413500
- [2]Walsh MC Necrotizing enterocolitis: treatment based on staging criteria. Pediatr Clin North Am, 1986.PMID 3081865
- [3]Neu J Necrotizing enterocolitis. N Engl J Med, 2011.PMID 21247316
- [4]Rees CM Peritoneal drainage or laparotomy for neonatal bowel perforation? A randomized controlled trial. Ann Surg, 2008.PMID 18580206
- [5]Rees CM Peritoneal drainage does not stabilize extremely low birth weight infants with perforated bowel: data from the NET Trial. J Pediatr Surg, 2010.PMID 20152345
- [6]Quigley M Donor human milk for preventing necrotising enterocolitis in very preterm or very low-birthweight infants. Cochrane Database Syst Rev, 2024.PMID 39239939
- [7]Swanson JR Spontaneous intestinal perforation (SIP) will soon become the most common form of surgical bowel disease in the extremely low birth weight infant. J Perinatol, 2022.PMID 35177793
- [8]Gordon PV Can a national dataset generate a nomogram for necrotizing enterocolitis onset? J Perinatol, 2014.PMID 25078862
- [9]Abdullahi AM Efficacy of probiotic supplementation in preventing necrotizing enterocolitis in preterm infants: a systematic review and meta-analysis. J Matern Fetal Neonatal Med, 2025.PMID 40204632
- [10]Kulkarni T Probiotic sepsis in preterm neonates - a systematic review. Eur J Pediatr, 2022.PMID 35348825
- [11]Attridge JT New insights into spontaneous intestinal perforation using a national data set (3): antenatal steroids have no adverse association with spontaneous intestinal perforation. J Perinatol, 2006.PMID 17024144
- [12]Gordon PV Understanding clinical literature relevant to spontaneous intestinal perforations. Am J Perinatol, 2009.PMID 19067283
- [13]Bethell GS Surgeons and neonatologists views about surgical decision-making in necrotising enterocolitis. Arch Dis Child Fetal Neonatal Ed, 2025.PMID 40280739