Paeds · fetal-neonatal-and-perinatal
Neonatal abstinence and withdrawal syndromes
Also known as Neonatal abstinence syndrome · Neonatal opioid withdrawal syndrome · NOWS · Neonatal drug withdrawal
Fellowship guide to neonatal abstinence and withdrawal syndromes: how chronic in-utero opioid exposure reprograms fetal neurotransmitter circuits so that cord clamping unleashes a hyperadrenergic withdrawal, the Finnegan and Eat Sleep Console assessment paradigms, the non-pharmacologic first-line bundle of rooming-in and breastfeeding, and the pharmacologic ladder from morphine to buprenorphine.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 36-week infant whose mother is on a methadone maintenance programme is admitted to the postnatal ward at 48 hours of age with a high-pitched cry, tremor when handled, and poor feeding. This is the archetypal presentation, and the question is not whether this is withdrawal — it almost certainly is — but how severe it is and whether it needs a drug. Neonatal abstinence syndrome is the clinical syndrome of postnatal withdrawal that follows chronic in-utero exposure to a substance on which the fetus has become physically dependent; when the exposure is an opioid, the term neonatal opioid withdrawal syndrome (NOWS) is used more precisely. [3]
The defining idea is neuroadaptation. Opioids cross the placenta freely, and over weeks of exposure the fetal brain adjusts its receptor density and neurotransmitter tone to maintain equilibrium in the presence of the drug. The opioid itself suppresses the locus coeruleus, the brain's noradrenaline engine, so the fetus compensates by up-regulating noradrenergic and dopaminergic pathways. At birth, the cord is clamped and the opioid supply stops abruptly, but the compensatory up-regulation persists — and the result is an unopposed surge of CNS and autonomic activity that we call withdrawal. [3] [5]
Three facts frame the topic for fellowship. First, it is common and rising — Patrick and colleagues showed that NAS incidence in the United States roughly tripled across the first decade of the 2000s, and it remains a leading driver of neonatal length of stay. [4] Second, it is largely manageable without drugs — a bundled approach of rooming-in, breastfeeding and functional assessment now allows most exposed infants to avoid pharmacotherapy altogether. [7] [9] Third, the harm extends beyond the neonatal stay — maternal opioid use disorder is associated with an elevated risk of postneonatal infant mortality, which is why discharge planning and follow-up are part of treatment, not an afterthought. [12]
Epidemiology & Risk Factors
NAS is overwhelmingly a disease of the opioid-exposed newborn, and its epidemiology tracks the adult opioid epidemic. Patrick's landmark JAMA analysis showed a roughly threefold rise in NAS across United States hospitals from 2000 to 2009, with parallel growth in length of stay and cost — a signal that maternal opioid use had become a population-scale neonatal problem. [4] The same group later demonstrated that NAS is geographically patterned: counties with greater economic disadvantage, fewer clinicians and rural location carry a disproportionate share, which frames the condition as a health-equity issue as much as a clinical one. [11]
The agent that the mother takes is the dominant risk determinant. Methadone is classically associated with more severe and later-peaking withdrawal, while buprenorphine — a partial μ-agonist — tends to produce a milder course in the exposed newborn, a finding consolidated by the MOTHER randomised trial. [5] Importantly, methadone and buprenorphine are the safest options for a pregnant person with opioid use disorder; their use is strongly encouraged, and the risk of neonatal withdrawal is not a reason to discontinue them. [3]
Several factors amplify severity beyond the agent itself. Polysubstance exposure — particularly co-use of nicotine, SSRIs, benzodiazepines or alcohol — deepens and prolongs the course. [3] Higher maternal opioid dose correlates with greater, though imperfectly predicted, severity. Late preterm gestation and prenatal tobacco exposure independently increase risk, while exclusive breastfeeding is one of the strongest protective factors. [9] [10]
Pathophysiology
The mechanism of NAS is the mechanism of neuroadaptation exposed. Opioids act primarily at the μ-opioid receptor, where they dampen neuronal firing and suppress the release of neurotransmitters — most importantly noradrenaline from the locus coeruleus, the principal noradrenergic nucleus. With chronic exposure the fetal brain compensates: it up-regulates μ-receptor density, increases adenylate cyclase signalling, and raises the tonic activity of the locus coeruleus and dopaminergic pathways so that the brain can keep firing in the presence of the suppressive drug. [3] [5]
When the cord is clamped the opioid supply ceases, but the compensation does not. The now-up-regulated noradrenergic and dopaminergic circuits fire without restraint, and the clinical result is central nervous system hyperexcitability (tremor, irritability, high-pitched cry, hypertonia, and in the extreme, seizures), autonomic overdrive (sweating, fever, nasal stuffiness, yawning, sneezing, mottling), and gastrointestinal dysregulation (uncoordinated suck, poor feeding, vomiting, diarrhoea). These three streams are the symptom clusters every assessment tool maps onto. [1] [3]
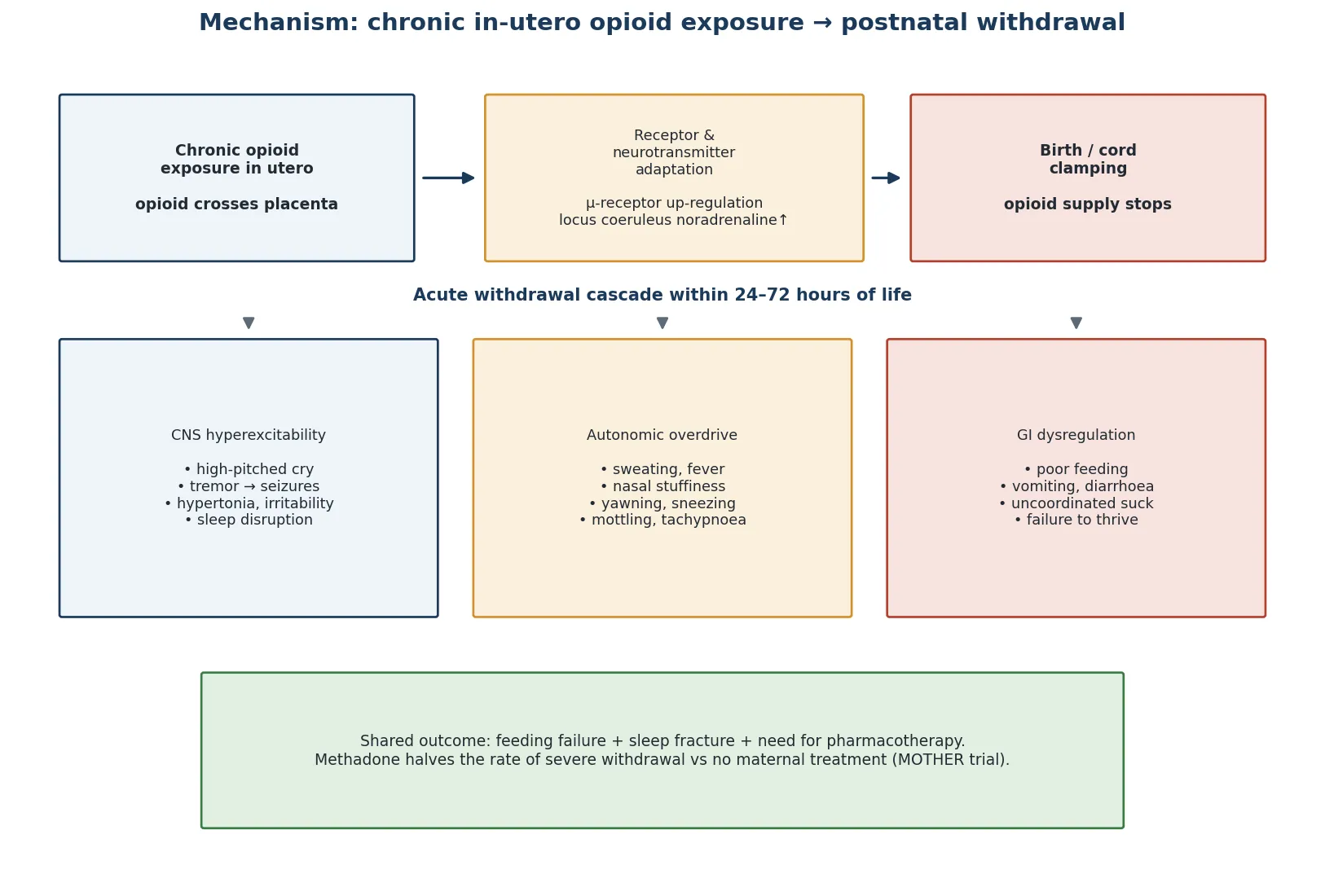
The timing of onset reflects the pharmacokinetics of the offending agent. Short-acting opioids (heroin, prescription oxycodone) produce withdrawal that begins within the first day; methadone, with its long half-life, characteristically peaks at 48 to 72 hours and can declare itself only after the infant has been discharged home. Buprenorphine, with even more complex kinetics, produces a milder and somewhat later course. This pharmacokinetic heterogeneity is why observation for a minimum of 5 to 7 days is standard for methadone-exposed infants. [3] [5]
The same logic explains why non-opioid agents produce overlapping but distinct syndromes. SSRIs produce an irritable, tremulous, sleep-fractured infant within hours — a serotonergic discontinuation rather than a true withdrawal. Nicotine contributes autonomic irritability and feeding difficulty. Benzodiazepines and alcohol add sedation, hypotonia and, with alcohol, a fetal alcohol spectrum overlay. The clinical skill is to recognise that an exposed infant is often withdrawing from several agents at once, and the opioid component is only the most predictable. [3]
Classification
NAS is classified along two axes: what caused it (the agent) and how severe it is (the assessment tool score or functional impairment). Holding both together lets you predict the timing and intensity of withdrawal and decide when to treat. [3]
The agent axis maps each exposure to its expected course. Methadone is the classic severe and late-peaking withdrawal; buprenorphine is milder; short-acting prescription opioids begin early; SSRIs produce a rapid-onset irritability that resolves within days; and polysubstance exposure amplifies and blurs the picture. Naming the agent at the bedside — confirmed by maternal history and, where uncertain, by urine or meconium toxicology — anchors the rest of the plan. [3] [5]
The severity axis is assessed by a tool, and two paradigms dominate. The Modified Finnegan Neonatal Abstinence Scoring System (NASS), built by Finnegan in 1975, is a 21-item weighted instrument across CNS, autonomic and gastrointestinal domains, scored every 3 to 4 hours. Three consecutive scores of 8 or more (or two consecutive scores of 12 or more; equivalently three consecutive scores totalling 24 or more) is the traditional trigger to begin pharmacotherapy. [1] [3] The Lipsitz tool is a shorter 11-item screen in which a score above 4 indicates withdrawal; it is simpler and more practical but less comprehensive. [2]
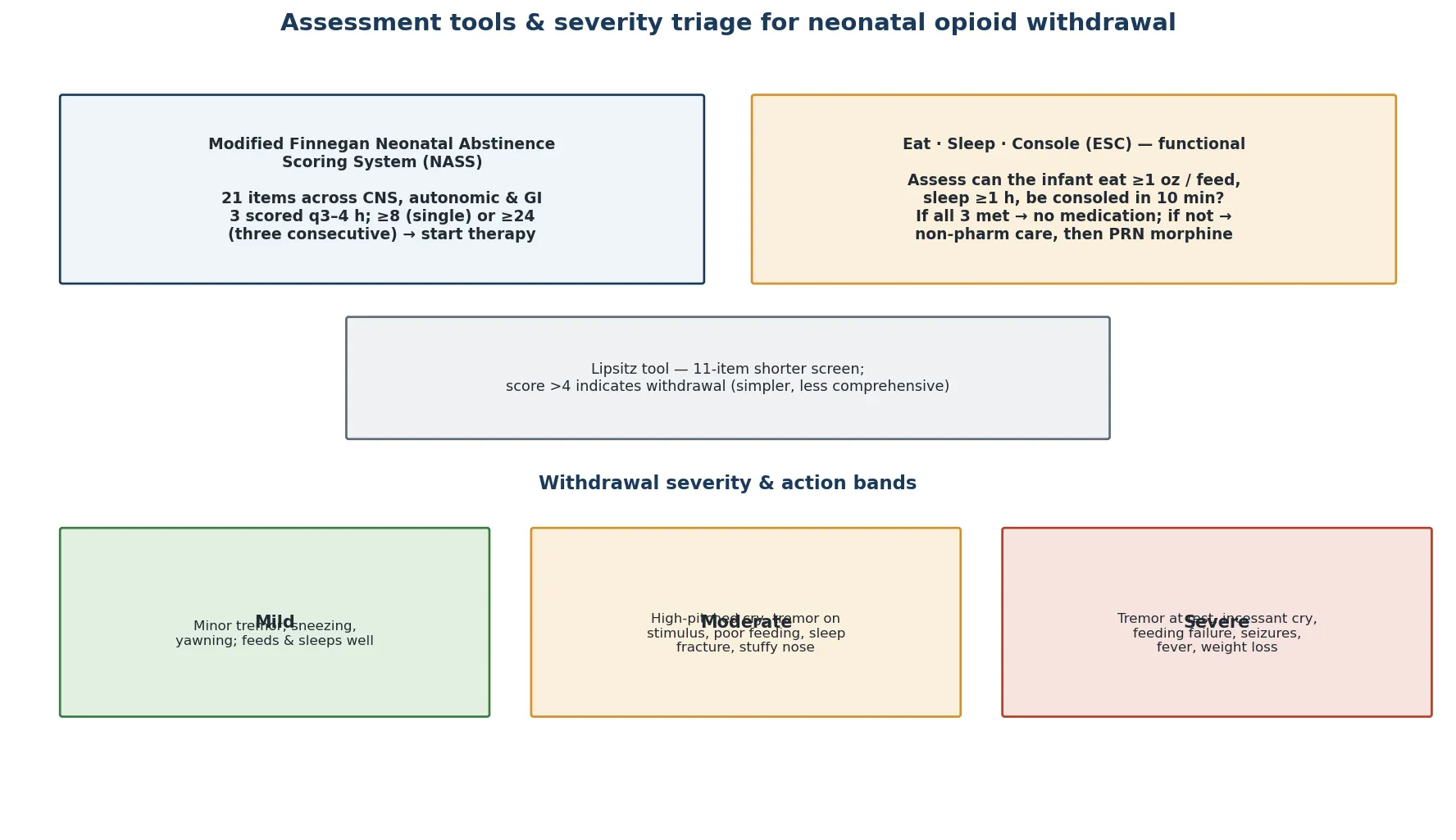
The newer and now dominant paradigm is the Eat, Sleep, Console (ESC) functional assessment. Rather than totalling a numeric score, ESC asks, at every feed, whether the infant can eat at least one ounce, sleep at least one hour, and be consoled within ten minutes. If all three goals are met, the infant needs no medication; if not, non-pharmacologic care is intensified first and a PRN dose of morphine given only when that fails. Grossman argued that the purely score-driven approach over-treats infants who are functionally well, and Blount's quality-improvement work showed that ESC substantially reduced both length of stay and morphine exposure. [7] [8]
Finnegan NASS versus Eat Sleep Console — two assessment philosophies
- 21 weighted items across CNS, autonomic, GI
- Scored q3–4 h; treat if three consecutive scores ≥8 or two consecutive ≥12
- Sensitive; can over-treat a functionally well infant
- Strong evidence base for drug trials
- Three functional goals at every feed: eat, sleep, console
- Medicate only when non-pharm care fails
- Shorter length of stay, less morphine use
- Demands robust rooming-in and staffing
Clinical Presentation
The opioid-exposed newborn looks well at birth and then deteriorates over the first one to three days. The earliest signs are subtle and easy to miss on a busy postnatal ward: a slightly high-pitched cry, sneezing, yawning, and a fine tremor when the infant is stimulated. Over the next 24 to 48 hours the picture deepens into the recognisable tetrad of CNS hyperexcitability, autonomic dysregulation, gastrointestinal dysfunction and disordered sleep. [1] [3]
The central nervous system signs are the most prominent and the most exam-worthy. A high-pitched, continuous cry, marked tremor that progresses from stimulus-provoked to present at rest, hypertonia, hyperreflexia, irritability and a markedly fractured sleep pattern form the core. In severe cases the infant develops myoclonic jerks or frank seizures, which are a late, severe sign and a clear indication for urgent pharmacotherapy and exclusion of mimics. [3]
The autonomic and gastrointestinal signs complete the picture. Sweating, fever, nasal stuffiness, skin mottling, yawning, sneezing and tachypnoea reflect noradrenergic overdrive. An uncoordinated suck, poor feeding, frequent regurgitation, loose stools and consequent weight loss reflect gut dysregulation and frequently drive the decision to treat because they threaten growth. The combination of a screaming, sweaty, tremulous infant who cannot feed or sleep is unmistakable once seen. [1] [3]
Atypical and delayed presentations are the traps. A methadone-exposed infant may be discharged home well and return days later with withdrawal declared only after discharge — which is why methadone-exposed infants are observed in hospital for at least 5 to 7 days. A breastfed infant whose mother stops feeding abruptly may decompensate as the partial opioid supplied through milk is withdrawn. And an infant with unsuspected polysubstance exposure — alcohol, benzodiazepines, gabapentin — may show disproportionate sedation, hypotonia or a prolonged course that does not fit a pure opioid picture. [3]
Differential Diagnosis
When an exposed infant is irritable, tremulous or feeding poorly, the differential runs in two directions: is this withdrawal, or is this another cause in an infant who happens to be exposed? The disciplined approach is to treat the withdrawal as the likely diagnosis while actively excluding the mimics that can coexist or masquerade. [3]
The mimics that must be excluded are the ones that cause CNS irritability and autonomic instability in any neonate. Hypoglycaemia is the first and most urgent — a glucose check costs nothing and missing a low glucose deepens any brain injury. Hypocalcaemia and hypomagnesaemia produce tremor and irritability. Sepsis and meningitis produce the same dysregulated picture and demand a septic screen when the infant is unwell. Intracranial haemorrhage, hypoxic-ischaemic encephalopathy and structural CNS abnormalities are the surgical and neurological emergencies. [3]
Within the substance-exposure family, the question is which agent is driving the picture. SSRIs produce a serotonergic discontinuation that mimics opioid withdrawal but resolves within days. Nicotine adds autonomic irritability. Benzodiazepine and alcohol withdrawal can produce sedation, hypotonia and seizures that differ from the hyperexcitable opioid picture. The clinical skill is to take a precise maternal medication and substance history, supplemented by maternal urine toxicology and infant meconium or umbilical-cord testing where the history is uncertain or polysubstance use is suspected. [3]
The discriminator that confirms withdrawal as the dominant process is the pattern and the response. A consistent constellation of CNS, autonomic and gastrointestinal signs emerging in the expected time window, with an appropriate maternal exposure, and improving with non-pharmacologic care or opioid-replacement therapy, is withdrawal. Signs that do not fit the pattern, that fail to respond, or that include a hard abnormality (a low glucose, a positive culture, an abnormal neurology) demand that the mimic be pursued. [3]
Clinical & Bedside Assessment
The bedside assessment of an opioid-exposed newborn is a structured, repeated, multidomain evaluation that begins at birth and continues through the observation window. It is not a single examination but a process: every feed is an opportunity to ask how the infant is doing across the three domains of function. [3] [7]
Begin with a precise maternal history. What opioid is the mother taking, at what dose, for how long, and is she stable or escalating? Is she on opioid agonist therapy (methadone or buprenorphine) under supervision — which is protective and supports breastfeeding — or using illicitly? What other substances is she exposed to: tobacco, alcohol, benzodiazepines, SSRIs, gabapentin? Are there mental health, social and child-protection considerations? This history frames the predicted timing, severity and complexity of withdrawal. [3] [10]
The focused examination observes the three symptom clusters in real time. Watch the infant feed: is the suck coordinated, can the infant sustain a feed, is there vomiting or diarrhoea? Observe the cry, tone and tremor at rest and on stimulation. Listen for the high-pitched quality of the cry. Look for autonomic signs — sweating, mottling, fever, nasal stuffiness. Assess the sleep pattern: does the infant wake screaming within minutes, or settle for an hour? These observations, repeated at each feed, are the raw material of both the Finnegan score and the ESC assessment. [1] [7]
I RRITABLE — the symptom domains of neonatal opioid withdrawal
The environmental and family assessment is as important as the infant examination. Who is at the bedside — is the mother present, supported and able to room-in? Are there safe-sleep, child-protection and social-work considerations? Is there a plan for ongoing maternal treatment, and will breastfeeding be possible? These factors determine whether non-pharmacologic care can succeed, because rooming-in and breastfeeding — the most effective interventions — depend entirely on the mother being present, well and supported. [3] [9]
Investigations
NAS is a clinical diagnosis made from the maternal exposure history and the structured infant assessment — there is no laboratory test that confirms it. The role of investigation is to exclude the mimics, identify co-morbidity, and where the exposure history is uncertain, confirm the agent. [3]
The bedside glucose is the single non-negotiable test, both because hypoglycaemia is a mimic and because the feeding dysfunction of withdrawal itself threatens glucose homeostasis. Check it at the first sign of irritability or feeding difficulty, and recheck during treatment. A serum electrolyte panel — calcium, magnesium, sodium — excludes the metabolic mimics of tremor and irritability. A full blood count and inflammatory markers, with blood culture when indicated, address sepsis, which is the dangerous mimic in any unwell neonate. [3]
Where the maternal history is uncertain or polysubstance exposure is suspected, toxicology confirms the agent. Maternal urine toxicology gives a recent-use snapshot; infant meconium or umbilical-cord tissue testing reflects exposure across the later second and third trimesters and is more sensitive for chronic use. These tests are most useful when the clinical picture does not fit a disclosed opioid exposure — for example, disproportionate sedation suggesting benzodiazepines or alcohol. [3]
Imaging is reserved for the atypical case. A cranial ultrasound is indicated when seizures, an abnormal neurological examination or a coagulopathy raise the possibility of intracranial haemorrhage. An electroencephalogram distinguishes true seizures from jitteriness or myoclonus when the clinical event is ambiguous. The principle is that investigations follow the clinical question — is this pure opioid withdrawal, is there a mimic, or is there co-morbidity? — and a typical, well-fitting NAS picture needs few tests beyond the glucose and electrolytes. [3]
Management — Resuscitation
There is no "resuscitation" in the conventional sense for NAS — the opioid-exposed newborn is typically vigorous at birth and rarely needs delivery-room intervention. The immediate priority is to establish the observation pathway, optimise the non-pharmacologic environment, and identify the infant who is deteriorating. [3]
For every opioid-exposed newborn, begin the non-pharmacologic foundation at birth: admit mother and infant together for rooming-in wherever possible, promote skin-to-skin contact and demand breastfeeding (provided the mother is stable on treatment and there is no contraindication), swaddle the infant, minimise environmental stimulation — low light, quiet, gentle handling — and plan lactation support. These measures are first-line for every exposed infant and substantially reduce the need for any drug. [9] [10]
When withdrawal escalates — the infant cannot eat, sleep or be consoled, or the Finnegan threshold is met — the resuscitation step is to start first-line pharmacotherapy promptly. First-line agents are oral morphine or, increasingly, sublingual buprenorphine. The goal is to control the CNS and autonomic signs rapidly enough to restore feeding and sleep, then wean. Delay in treating severe withdrawal prolongs suffering and risks seizures, weight loss and the disruption of early bonding. [3] [6]
Management — Definitive & Stepwise
The definitive management of NAS is a layered, escalating pathway that begins with non-pharmacologic care for every exposed infant and reserves drug therapy for those who fail to thrive on that foundation. Holding the whole ladder in mind is the answer to every management question. [3] [7]
The first tier — non-pharmacologic care — is the most evidence-based and most underused. Rooming-in keeps mother and infant together and reduces the need for pharmacotherapy; demand breastfeeding supplies partial opioid, caloric intake and comfort; swaddling, low-stimulation environments and skin-to-skin contact settle the hyperexcitable infant. The Welle-Strand cohort showed that breastfeeding substantially reduced the proportion of opioid-exposed infants needing withdrawal treatment. [9] [10]
The second tier — structured assessment — is the decision engine. Using ESC, every feed asks whether the infant eats at least one ounce, sleeps at least one hour and is consoled within ten minutes; using Finnegan, a score is totalled every 3 to 4 hours. The assessment paradigm chosen determines when and whether the infant crosses into pharmacotherapy. [1] [7]
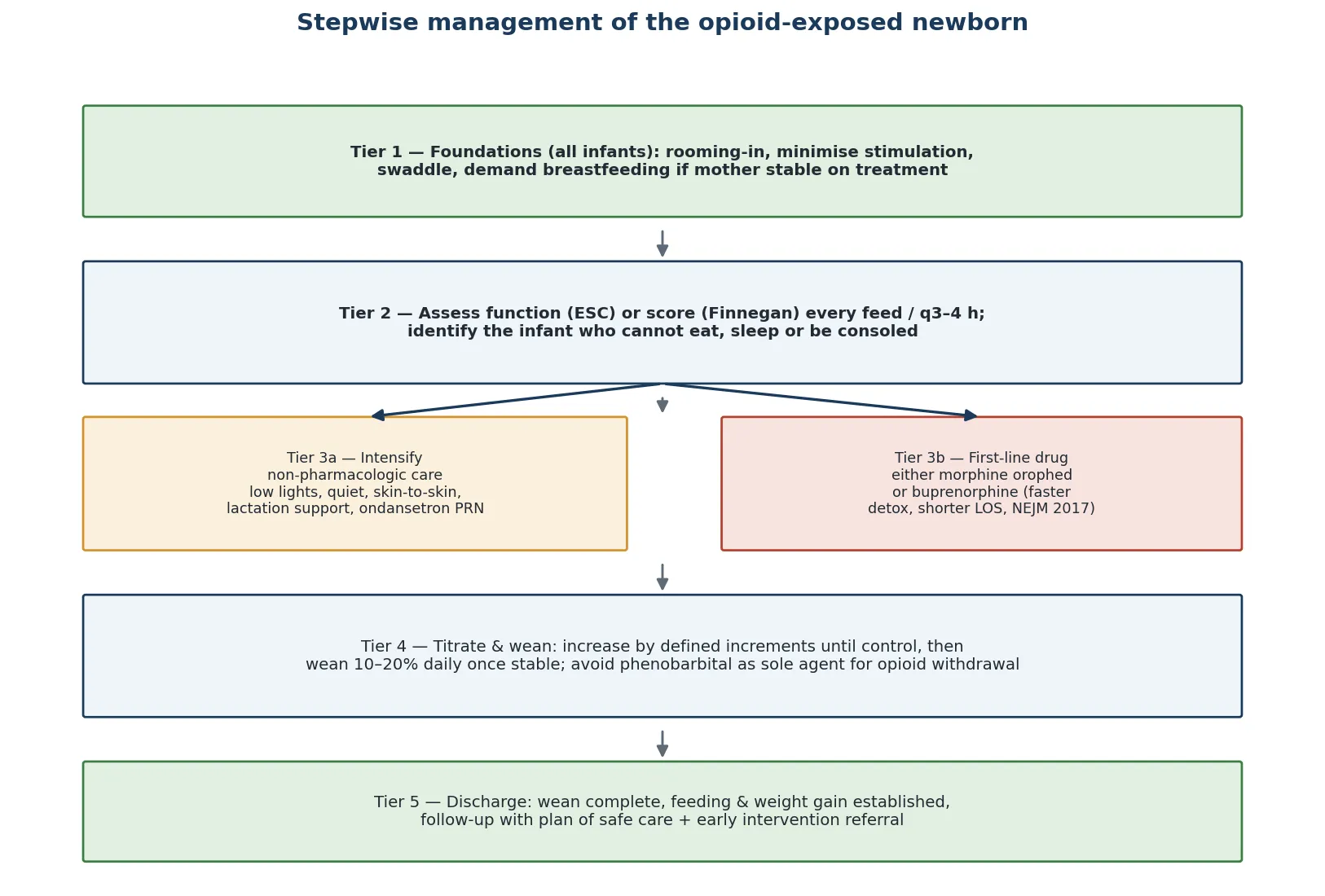
The third tier — first-line pharmacotherapy — is reached when the infant cannot eat, sleep or be consoled despite maximal conservative care, or when the Finnegan threshold is met. The two evidence-based options are oral morphine — the long-standing first line — and sublingual buprenorphine, which the Kraft NEJM 2017 randomised trial showed shortened the duration of treatment relative to morphine. [3] [6] Morphine is started at a defined initial dose and titrated upward in set increments until the infant is settled and feeding; buprenorphine offers a faster wean but requires attention to its complex pharmacology and the absence of a commercial neonatal preparation. [6]
Morphine (oral) — first-line
Dose
Neonatal morphine solution typically 0.05 mg/kg/dose every 3–4 h; titrate upward by increments of 0.05 mg/kg/dose until control
Buprenorphine (sublingual)
Dose
~0.15 mg/kg/day in divided doses (e.g. q6 h), titrated to control
The fourth tier — titration and weaning — stabilises the infant and then reduces the drug. The opioid dose is increased until the infant can eat, sleep and be consoled, and once stable for 24 to 48 hours the dose is weaned by 10 to 20 percent daily. Phenobarbital should not be used as a sole agent for pure opioid withdrawal — it does not treat the opioid deficiency and prolongs sedation — though it has an adjunctive role when polysubstance, especially alcohol or benzodiazepine, withdrawal dominates. [3] [6]
Stepwise management of the opioid-exposed newborn
Rooming-in, swaddle, low-stimulation environment, skin-to-skin and demand breastfeeding from birth
Assess at every feed: can the infant eat ≥1 oz, sleep ≥1 h, be consoled in 10 min (ESC) or total the Finnegan score q3–4 h
If function met: continue conservative care, observe for the agent-specific window (≥5–7 days for methadone)
If function fails: intensify non-pharmacologic care first (quiet room, lactation support, ondansetron for vomiting)
If function still fails: start first-line morphine or buprenorphine, titrate to a calm, feeding, sleeping infant
Once stable 24–48 h: wean opioid by 10–20% daily; add phenobarbital only for polysubstance/alcohol-dominant withdrawal
Discharge: wean complete, feeding and weight gain established, plan of safe care and early-intervention follow-up arranged
The fifth tier — discharge and follow-up — closes the loop. Discharge is appropriate when the opioid wean is complete (or a stable low-dose wean is achievable at home with close support), the infant is feeding and gaining weight, and the family is supported. A plan of safe care — addressing maternal treatment, safe sleep, child protection and social support — is mandatory. Because maternal opioid use disorder carries an elevated risk of postneonatal infant mortality, ongoing paediatric and social follow-up is part of treatment. [3] [12]
Specific Subtypes & Scenarios
The methadone-exposed infant is the classic, highest-yield scenario. Methadone, with its long half-life, produces withdrawal that peaks at 48 to 72 hours and can declare only after the routine discharge window — which is why methadone-exposed infants are observed in hospital for at least 5 to 7 days. Severity is greater than with short-acting opioids, and the proportion needing pharmacotherapy is higher. The management is the full ladder, with a low threshold for pharmacotherapy and a planned, supervised wean. [3]
The buprenorphine-exposed infant is the milder counterpart. The MOTHER trial showed that maternal buprenorphine, compared with methadone, produced significantly less neonatal opioid use and a shorter course — a finding that has driven the shift toward buprenorphine in pregnancy where feasible. The buprenorphine-exposed infant still needs the full observation and assessment pathway, but the predicted course is milder. [5]
The polysubstance-exposed infant is the complex case. Co-use of nicotine, SSRIs, benzodiazepines, alcohol or gabapentin deepens and prolongs withdrawal and may produce a clinical picture — sedation, hypotonia, atypical seizures — that does not fit pure opioid withdrawal. Phenobarbital has a genuine adjunctive role here, particularly for the alcohol or benzodiazepine component. A precise substance history and, where needed, meconium or cord toxicology guide the choice of agent. [3]
The breastfeeding mother on opioid agonist therapy is the scenario in which non-pharmacologic care is most powerful. A mother stable on methadone or buprenorphine, HIV-negative and without other contraindications, should be actively supported to breastfeed — it measurably reduces the infant's need for pharmacotherapy, supports bonding, and is endorsed by the AAP and the Academy of Breastfeeding Medicine. The decision to stop breastfeeding should be made deliberately, not abruptly, as sudden cessation can precipitate or worsen infant withdrawal. [9] [10]
The infant with withdrawal seizures is the emergency scenario. Seizures are a late, severe sign of withdrawal, but they are also the presentation of hypoglycaemia, hypocalcaemia, sepsis, intracranial haemorrhage and metabolic disease. The approach is to check glucose and electrolytes, perform a septic screen, control the seizures, start pharmacotherapy for withdrawal, and image where indicated. A seizing opioid-exposed infant is never simply "severe withdrawal" until the mimics are excluded. [3]
The infant with social complexity — parental instability, out-of-home care, intergenerational substance use — is the scenario in which discharge planning dominates. The plan of safe care integrates maternal addiction treatment, child protection, social work, safe-sleep education and follow-up. The clinical team manages the withdrawal; the system manages the family, and both are needed for a good outcome. [3] [12]
Complications & Pitfalls
The immediate complications of untreated or severe NAS are the direct consequences of CNS hyperexcitability and autonomic overdrive: seizures, feeding failure with dehydration and weight loss, sleep deprivation, fever, and the disruption of early mother-infant bonding that comes from a screaming, dysregulated infant. These are the reasons pharmacotherapy is started — to control the signs and restore feeding and sleep. [3]
The treatment-related complications are the ones the examiner probes. Over-sedation from excessive opioid produces apnoea, hypotension and feeding failure that can be mistaken for worsening withdrawal — the disciplined response is to hold the dose, not increase it. A prolonged wean traps the infant in hospital for weeks; this is where buprenorphine and a structured 10 to 20 percent daily wean earn their place. Inappropriate use of phenobarbital as a sole agent for opioid withdrawal fails to replace the missing opioid, prolongs sedation, and is a common error. [3] [6]
The longer-term complications are developmental and social. NAS is associated with an elevated risk of behavioural and developmental concerns in early childhood, though disentangling the effect of withdrawal from the effect of the social and environmental context of opioid use disorder is difficult. Maternal opioid use disorder itself is associated with an elevated risk of postneonatal infant mortality, which is why the plan of safe care and close follow-up are part of treatment. [12]
The classic errors each have a name. Premature discharge of a methadone-exposed infant who has not yet reached peak withdrawal. Failing to check the glucose in an irritable exposed infant. Over-treating a functionally well infant on the basis of a score alone. Using phenobarbital as a sole agent for pure opioid withdrawal. Stopping breastfeeding abruptly and precipitating worsening withdrawal. Each is avoidable by holding the full ladder and the functional assessment in mind. [3] [7]
Prognosis & Disposition
The short-term prognosis of NAS is overwhelmingly good: with structured assessment, non-pharmacologic care and appropriately escalated pharmacotherapy, the vast majority of infants settle, wean and discharge within one to three weeks. Outcome is determined by the severity and duration of withdrawal (driven by the agent, dose and polysubstance exposure), the success of non-pharmacologic care (driven by the mother's presence and ability to room-in and breastfeed), and the social context (which determines the safety and sustainability of the discharge plan). [3] [9]
The length of stay has fallen markedly with the adoption of ESC and bundled non-pharmacologic care. Blount's quality-improvement work showed that the ESC approach substantially reduced both length of stay and morphine exposure without a rise in adverse events — a finding that has driven the shift away from a purely score-driven, drug-heavy paradigm. [8] The buprenorphine RCT similarly shortened the duration of pharmacotherapy relative to morphine. [6]
The disposition decision hinges on the wean and the family. Discharge is appropriate when the opioid wean is complete (or a stable, safe low-dose home wean is feasible with close support), feeding and weight gain are established, and the plan of safe care — maternal treatment, child protection, safe sleep, follow-up — is in place. Methadone-exposed infants who have not yet reached their peak are not discharged; infants with social complexity may need a delayed or supported discharge. [3]
The follow-up reflects the longer horizon. Because NAS is associated with elevated risks of developmental, behavioural and social concerns, and because maternal opioid use disorder carries an elevated postneonatal mortality risk, ongoing paediatric, developmental and social follow-up is part of the treatment plan. Early-intervention referral, developmental surveillance and integration with the maternal addiction team are the safety net that turns a successful neonatal stay into a successful childhood. [12]
Special Populations
The infant of a mother in a medication-assisted treatment programme is the prototypical case and the one in which modern, evidence-based care shines. The mother on stable methadone or buprenorphine under supervision should be actively supported to room-in and breastfeed, and the infant managed with the ESC or Finnegan pathway. This is the group in which non-pharmacologic care has the greatest effect and in which the proportion needing pharmacotherapy has fallen furthest. [9] [10]
The preterm opioid-exposed infant is a distinct and milder subgroup. Preterm infants exposed to opioids tend to show less severe withdrawal, partly because of immature receptor systems and a shorter cumulative exposure; however, they are vulnerable to the complications of prematurity and to the over-sedation that aggressive pharmacotherapy can cause. Assessment must account for prematurity, and pharmacotherapy titrated cautiously. [3]
The infant with polysubstance and alcohol exposure carries the dual burden of opioid withdrawal and the neurodevelopmental and dysmorphic features of fetal alcohol spectrum disorder. Withdrawal may be atypical — sedation, hypotonia, seizures — and phenobarbital may be needed as an adjunct for the alcohol or benzodenzepine component. The longer-term developmental prognosis is guarded and early intervention is essential. [3]
The socially complex family — parental instability, out-of-home care, intergenerational substance use, poverty — is the population in which the clinical team must work hardest on the system around the infant. The plan of safe care integrates child protection, maternal addiction treatment, social work and follow-up, and the clinical team is one node in a network. NAS in this context is as much a child-rights and equity issue as a medical one. [3] [11]
In rural, remote and economically disadvantaged communities, the burden of NAS is disproportionate — Patrick's county-level analysis showed that economic disadvantage, clinician supply and rural location each independently predicted NAS. Access to medication-assisted treatment, to lactation support, and to the social infrastructure that makes rooming-in feasible are health-equity priorities. [11]
Evidence, Guidelines & Regional Differences
The evidence base for NAS management has been transformed in the last decade by three threads: the move from score-driven to functional assessment, the demonstration that buprenorphine shortens treatment, and the consolidation of non-pharmacologic care as first-line for every exposed infant. The Finnegan NASS, developed in 1975, remains the most validated scoring instrument and the backbone of drug trials, but the purely score-driven paradigm has been challenged for over-treating functionally well infants. [1] [7]
The Eat, Sleep, Console paradigm, articulated by Grossman in 2017, reframes assessment around three functional goals and has been shown in quality-improvement work (Blount 2019) to substantially reduce both length of stay and morphine exposure. [7] [8] The buprenorphine RCT (Kraft, NEJM 2017) demonstrated that sublingual buprenorphine shortened the duration of pharmacotherapy relative to morphine — a genuine advance in first-line therapy. [6] And the MOTHER trial (Jones, NEJM 2010) established that maternal buprenorphine produces a milder neonatal course than methadone. [5]
Kraft 2017 — Buprenorphine versus morphine (NEJM)
Multicentre, double-blind, double-dummy randomised trial
Population: Term infants ≥37 weeks with NAS needing pharmacotherapy
Key finding
Buprenorphine shortened the duration of treatment (median ~15 vs ~32 days) and length of stay compared with morphine
Practice change
Buprenorphine is a valid first-line option for NOWS pharmacotherapy where extemporaneous preparation is feasible
On the non-pharmacologic side, the breastfeeding evidence is strong. Welle-Strand's cohort showed that breastfeeding substantially reduced the proportion of opioid-exposed infants needing withdrawal treatment, and the Academy of Breastfeeding Medicine protocol (Holmes) endorses breastfeeding in stable mothers on opioid agonist therapy. [9] [10] The AAP clinical report (Hudak 2012) remains the foundational guidance document, covering assessment, pharmacotherapy, breastfeeding and discharge planning. [3]
The epidemiological evidence frames the scale and the equity dimension. Patrick's JAMA 2012 analysis documented the threefold rise in NAS and its cost, and the 2019 county-level analysis showed that economic disadvantage, clinician supply and rural location each independently predicted NAS incidence — a health-equity signal. [4] [11] Grossarth's 2023 analysis linked maternal opioid use disorder to elevated postneonatal infant mortality, extending the horizon of harm well beyond the neonatal stay. [12]
All regions now converge on rooming-in, breastfeeding and functional or structured assessment as the foundation, with pharmacotherapy reserved for the infant who cannot eat, sleep or be consoled. ANZ neonatal networks emphasise the ESC or modified Finnegan pathway, rooming-in wherever possible, and a strong multidisciplinary discharge plan. UK (BAPM, RCPCH) guidance endorses the AAP framework, prioritises non-pharmacologic care, and integrates with perinatal mental-health and substance-use services. US (AAP) guidance is the most cited globally and sets the Finnegan and ESC paradigms alongside the pharmacologic ladder. Canada (CPS) guidance mirrors the AAP approach and emphasises the plan of safe care. The regions differ in the precise drug preparation and wean schedule — which should always be checked against the local neonatal unit protocol — but agree on the principles. [3] [7] [6]
The evidence is still moving in three areas. The optimal agent — morphine versus buprenorphine — depends on local preparation availability, infant factors and unit protocol. The role of clonidine as an adjunct or alternative is promising but less mature than the morphine and buprenorphine evidence. The long-term developmental outcome of NOWS, disentangled from its social and environmental context, remains an active research question. [3] [6]
Exam Pearls
The definition one-liner: neonatal abstinence syndrome (NAS), or neonatal opioid withdrawal syndrome (NOWS), is the postnatal withdrawal syndrome following chronic in-utero opioid exposure, peaking at 24 to 72 hours, driven by unopposed noradrenergic and CNS hyperactivity after cord clamping. [3] [5]
The mechanism one-liner: chronic opioid exposure up-regulates μ-receptors and locus-coeruleus noradrenaline; cord clamping removes the brake and unleashes CNS hyperexcitability, autonomic overdrive and gastrointestinal dysregulation. [3]
The assessment one-liner: Finnegan NASS (21 items, treat if three consecutive scores ≥8 or two consecutive ≥12) is the score-driven tool; Eat, Sleep, Console is the functional alternative — medicate only when the infant cannot eat, sleep or be consoled. [1] [7]
The management one-liner: rooming-in, breastfeeding, swaddling and low stimulation for every exposed infant first; morphine or buprenorphine only for the infant who fails non-pharmacologic care; wean 10 to 20 percent daily; phenobarbital only as an adjunct for polysubstance or alcohol-dominant withdrawal. [3] [6]
The breastfeeding one-liner: breastfeeding in a stable mother on opioid agonist therapy reduces the need for pharmacotherapy and is endorsed by the AAP and ABM — it is treatment, not a lifestyle choice. [9] [10]
The timing one-liner: methadone peaks at 48 to 72 hours and can declare after discharge — observe methadone-exposed infants for at least 5 to 7 days. [3]
The classic viva traps: mistaking hypoglycaemia or sepsis for withdrawal; over-treating a functionally well infant on a score alone; using phenobarbital as a sole agent for opioid withdrawal; and stopping breastfeeding abruptly. The counter-trap is mistaking opioid over-sedation for worsening withdrawal and escalating the dose. [3] [7]
References
- [1]Finnegan LP Neonatal abstinence syndrome: assessment and management. Addict Dis, 1975.PMID 1163358
- [2]Lipsitz PJ A proposed narcotic withdrawal score for use with newborn infants. A pragmatic evaluation of its efficacy. Clin Pediatr (Phila), 1975.PMID 1126108
- [3]Hudak ML Neonatal drug withdrawal. Pediatrics, 2012.PMID 22291123
- [4]Patrick SW Neonatal abstinence syndrome and associated health care expenditures: United States, 2000-2009. JAMA, 2012.PMID 22546608
- [5]Jones HE Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med, 2010.PMID 21142534
- [6]Kraft WK Buprenorphine for the Neonatal Abstinence Syndrome. N Engl J Med, 2017.PMID 28877016
- [7]Grossman MR Neonatal Abstinence Syndrome: Time for a Reappraisal. Hosp Pediatr, 2017.PMID 28137921
- [8]Blount T Reduction in Length of Stay and Morphine Use for NAS With the Eat, Sleep, Console Method. Hosp Pediatr, 2019.PMID 31285356
- [9]Welle-Strand GK Breastfeeding reduces the need for withdrawal treatment in opioid-exposed infants. Acta Paediatr, 2013.PMID 23909865
- [10]Holmes AP Breastfeeding Considerations for Mothers of Infants with Neonatal Abstinence Syndrome. Pharmacotherapy, 2017.PMID 28488805
- [11]Patrick SW Association Among County-Level Economic Factors, Clinician Supply, Metropolitan or Rural Location, and Neonatal Abstinence Syndrome. JAMA, 2019.PMID 30694320
- [12]Grossarth S Maternal Opioid Use Disorder and the Risk of Postneonatal Infant Mortality. JAMA Pediatr, 2023.PMID 37155175