Paeds · fetal-neonatal-and-perinatal
Neonatal anaemia, polycythaemia and thrombocytopenia
Also known as Neonatal anaemia · Neonatal polycythaemia · Neonatal thrombocytopenia · Neonatal alloimmune thrombocytopenia · Neonatal hyperviscosity
Fellowship guide to the three major neonatal haematological disorders: anaemia (haemolytic disease, blood loss, underproduction and transfusion thresholds), polycythaemia and hyperviscosity syndrome (diagnosis and the controversy over partial exchange transfusion), and thrombocytopenia (neonatal alloimmune thrombocytopenia, maternal ITP, sepsis-related causes, platelet transfusion thresholds and intracranial haemorrhage prevention).
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Neonatal haematological disorders encompass three distinct but overlapping disturbances of the red cell and platelet compartments that present in the first 28 days of life: anaemia, polycythaemia, and thrombocytopenia. Each can produce rapidly progressive, life-threatening complications, and all three may coexist in the sick preterm or asphyxiated infant. A firm grasp of the cell-line-specific thresholds, causes, and transfusion principles is essential for any clinician caring for newborns. [8]
Neonatal anaemia is defined as a venous haemoglobin concentration below 130 g per litre in a term infant or below 140 g per litre in a preterm infant in the first week of life. It arises from three broad mechanisms: haemolysis (immune-mediated destruction such as rhesus or ABO incompatibility, red cell enzyme defects, or inherited membrane disorders), acute blood loss (fetomaternal haemorrhage, twin-twin transfusion, or peripartum bleeding), and underproduction (the physiological anaemia of prematurity, bone marrow suppression from infection, or rare congenital syndromes). [2]
Neonatal polycythaemia is defined as a venous haematocrit above 65 per cent, and it becomes clinically significant when the elevated haematocrit produces hyperviscosity with sluggish microvascular flow. The primary causes are chronic intrauterine hypoxia (intrauterine growth restriction, maternal hypertension, or high altitude), passive transfer of red cells (infant of a diabetic mother, delayed cord clamping, or twin-twin transfusion recipient), and less commonly chromosomal disorders such as trisomy 21. [6]
Neonatal thrombocytopenia is defined as a platelet count below 150 times 10 to the 9 per litre. It affects up to 1 per cent of term infants and 35 per cent of those admitted to the neonatal intensive care unit, and the dominant early-onset cause is neonatal alloimmune thrombocytopenia, in which maternal antibodies against paternally inherited human platelet antigens destroy fetal platelets. Late-onset thrombocytopenia is most often secondary to sepsis or necrotising enterocolitis, and severe thrombocytopenia carries the risk of intracranial haemorrhage. [7]
Classification
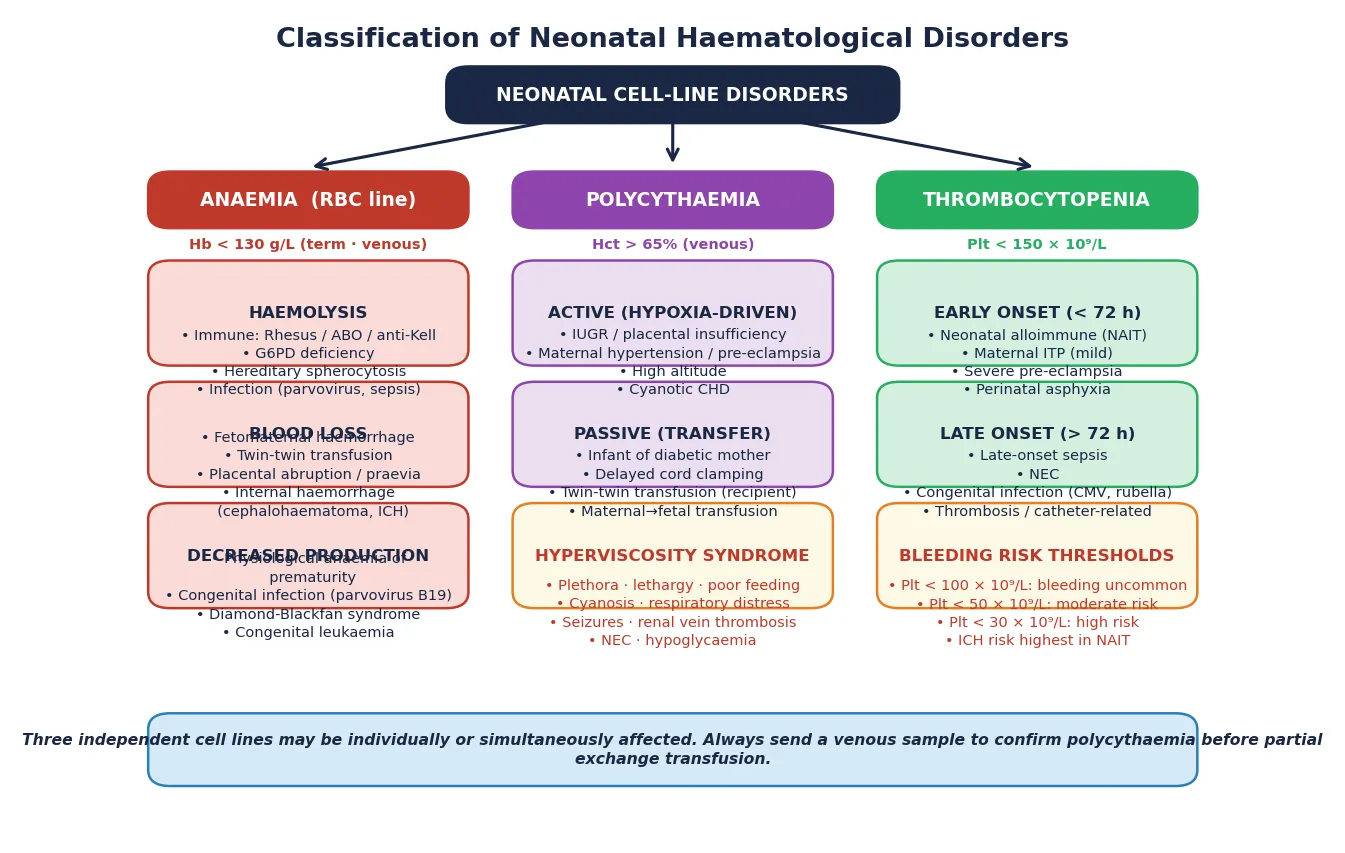
The three disorders map neatly onto the three formed blood elements. Anaemia reflects loss or destruction of red cells, polycythaemia reflects an excess of red cells, and thrombocytopenia reflects loss or underproduction of platelets. Each condition further splits by mechanism and onset timing, which drives both investigation and treatment decisions. [8]
[7]Anaemia divides further by mechanism: haemolytic causes include rhesus and ABO incompatibility, glucose-6-phosphate dehydrogenase deficiency, hereditary spherocytosis, and congenital infection. Blood loss causes include fetomaternal haemorrhage, twin-twin transfusion, placental abruption, and internal haemorrhage from birth trauma. Decreased production causes include physiological anaemia of prematurity, congenital parvovirus B19 infection, Diamond-Blackfan anaemia, and congenital leukaemia. [2]
Epidemiology & Risk Factors
Anaemia affects virtually all extremely preterm infants during their NICU stay, driven by a combination of immature erythropoiesis, phlebotomy losses, and a shortened red cell lifespan. The physiological nadir of haemoglobin in term infants occurs at 8 to 12 weeks at approximately 95 to 110 g per litre, while in preterm infants it occurs earlier at 4 to 8 weeks and falls lower to 70 to 90 g per litre. Iron deficiency and repeated phlebotomy losses compound the problem in sick neonates. [2]
The introduction of maternal anti-D prophylaxis has dramatically reduced the incidence of severe rhesus haemolytic disease of the newborn, but it has not eliminated it entirely, and non-rhesus antigens such as anti-Kell and ABO incompatibility remain clinically important. Fetomaternal haemorrhage sufficient to cause neonatal anaemia occurs in approximately 1 in 1000 births, and glucose-6-phosphate dehydrogenase deficiency affects up to 7 per cent of the global population, making it the most common enzymatic red cell defect worldwide. [4]
Polycythaemia occurs in 1 to 5 per cent of term infants, and the incidence rises substantially in specific at-risk groups. Infants of diabetic mothers have a polycythaemia rate of 20 to 40 per cent, those with intrauterine growth restriction and placental insufficiency are also at high risk, and delayed cord clamping increases the risk if the infant is held below the level of the placenta for more than 60 seconds. [6]
Thrombocytopenia is detected in 1 to 5 per cent of all term newborns at birth and in up to 35 per cent of NICU admissions, with the highest rates seen in the smallest and sickest infants. Neonatal alloimmune thrombocytopenia has an incidence of approximately 1 in 1000 live births and is the most common cause of severe isolated thrombocytopenia in an otherwise healthy term neonate. Maternal autoimmune thrombocytopenia affects roughly 1 in 1000 pregnancies and typically causes milder neonatal thrombocytopenia than the alloimmune form. [7]
Pathophysiology
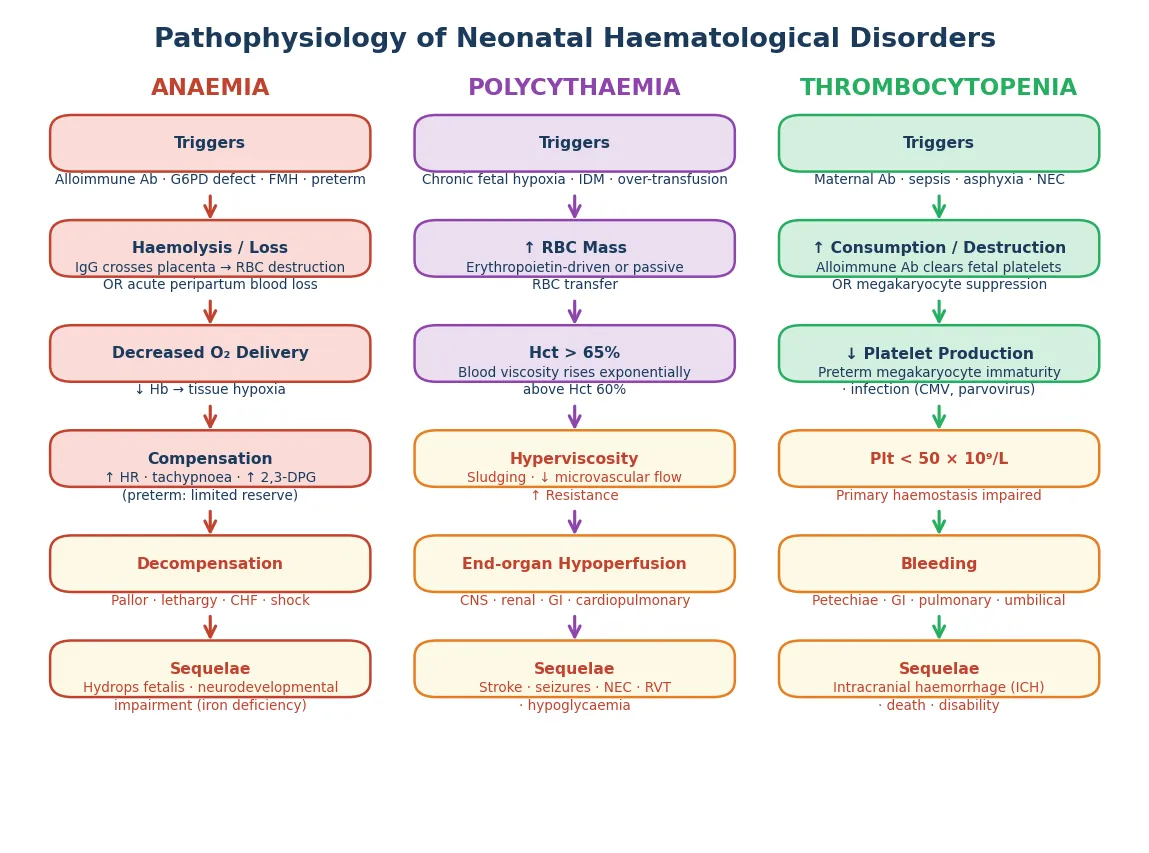
The pathophysiology of neonatal anaemia depends on the underlying mechanism. In haemolytic disease, maternal immunoglobulin G antibodies cross the placenta and bind fetal red cell antigens, triggering extravascular destruction by splenic macrophages. In rhesus disease this produces a predominantly extravascular, progressively severe haemolysis that can lead to hydrops fetalis from severe anaemia and secondary heart failure. In ABO incompatibility the haemolysis is milder and predominantly intravascular, as anti-A and anti-B antibodies are naturally occurring immunoglobulin M molecules that cross the placenta poorly. [4]
The anaemia of prematurity is a distinct physiological entity. Preterm infants are born before the bulk of transplacental iron transfer that occurs in the third trimester, they have a shorter red cell lifespan of 60 to 80 days compared with 120 days in adults, their erythropoietin response is blunted because the liver rather than the kidney is the primary site of production, and iatrogenic blood loss from phlebotomy can exceed 10 mL per kg per day in the first weeks of life. Iron deficiency in early infancy has measurable effects on brain myelination and neurotransmitter synthesis, and early iron supplementation is now recommended for preterm infants. [2]
Glucose-6-phosphate dehydrogenase deficiency causes episodic haemolysis when red cells are exposed to oxidative stress. The enzyme normally maintains reduced glutathione, which protects haemoglobin from oxidative denaturation. Deficient red cells cannot regenerate nicotinamide adenine dinucleotide phosphate fast enough under oxidative challenge from fava beans, certain medications (sulphonamides, primaquine, naphthalene), or infection, and oxidised haemoglobin precipitates as Heinz bodies that damage the red cell membrane and triggers splenic clearance. [3]
Polycythaemia pathophysiology centres on the exponential relationship between haematocrit and blood viscosity. Blood viscosity rises gradually until a haematocrit of approximately 60 per cent and then increases steeply, so small increases in haematocrit above this threshold produce large increases in viscosity. Hyperviscocious blood flows sluggishly through the microcirculation, causing sludging, impaired tissue oxygen delivery paradoxically worsened by the high haematocrit, thrombus formation, and end-organ hypoperfusion affecting the brain, kidneys, gastrointestinal tract, and lungs. [5]
Neonatal thrombocytopenia has two principal mechanisms: accelerated platelet destruction or consumption, and impaired platelet production. In neonatal alloimmune thrombocytopenia, the mother is platelet-antigen-negative (most commonly human platelet antigen 1a) and the fetus inherits the paternally derived antigen. Maternal immunoglobulin G antibodies cross the placenta and bind fetal platelets, which are then cleared by reticuloendothelial macrophages. The fetal megakaryocyte mass cannot compensate, producing platelet counts that can fall below 10 times 10 to the 9 per litre and placing the infant at risk of intracranial haemorrhage. [9]
Clinical Presentation
Anaemic neonates present with pallor, tachycardia, tachypnoea, and poor perfusion. The severity of symptoms correlates with both the degree of anaemia and the rapidity of onset: an infant who loses blood acutely through fetomaternal haemorrhage will be symptomatic at a higher haemoglobin than one with slowly developing haemolysis. In severe anaemia, signs of cardiac compensation progress to decompensation with gallop rhythm, hepatomegaly, and congestive cardiac failure. Jaundice accompanies haemolytic anaemia and may be the presenting feature, while splenomegaly suggests ongoing haemolysis or hydrops. [2]
Polycythaemic neonates classically appear plethoric with a red-purple or duskily cyanotic complexion that may be most visible in the face, mucous membranes, and distal extremities. The clinical features of hyperviscosity syndrome are non-specific and overlap with many neonatal conditions: lethargy, poor feeding, hypotonia, irritability, tremors, and seizures reflect central nervous system involvement; respiratory distress, cyanosis, and tachypnoea reflect pulmonary vascular congestion; and poor urine output, haematuria, and abdominal distension may reflect renal vein thrombosis or necrotising enterocolitis. Hypoglycaemia is a frequent metabolic complication. [6]
Thrombocytopenic neonates present with bleeding manifestations proportional to the platelet deficit and the underlying cause. Petechiae and purpura are the most common cutaneous signs, often concentrated at pressure points or the presenting part. Mucosal bleeding, oozing from venepuncture or heel-prick sites, gastrointestinal bleeding, pulmonary haemorrhage, and haematuria may all occur. The most feared complication is intracranial haemorrhage, which can present with seizures, apnoea, bulging fontanelle, or rapid neurological deterioration. [8]
Presenting signs by disorder
Anaemia: pallor, tachycardia, tachypnoea, poor feeding, jaundice (haemolysis)
Polycythaemia: plethora, lethargy, cyanosis, tremor, poor feeding, hypoglycaemia
Thrombocytopenia: petechiae, purpura, bleeding from puncture sites, seizures (ICH)
Shared red flags: heart failure, shock, necrotising enterocolitis, renal vein thrombosis
The three conditions may coexist in sepsis, asphyxia, or extreme prematurity
Differential Diagnosis
The differential for a pale neonate extends beyond haematological causes to include congenital heart disease presenting with poor perfusion, sepsis with distributive shock, metabolic acidosis from inborn errors, and asphyxia. A full blood count, blood gas, lactate, and capillary refill assessment help distinguish anaemia from these mimics, and a rapid haemoglobin measurement is the definitive discriminator. [2]
For neonatal polycythaemia, the key differential is between the plethoric but well infant (who needs observation) and the symptomatic hyperviscous infant (who may benefit from intervention). Cyanotic congenital heart disease can produce secondary polycythaemia and must be excluded, and sepsis can mimic the lethargy and poor perfusion of hyperviscosity syndrome. [6]
The differential for neonatal thrombocytopenia is organised by onset timing. Early-onset thrombocytopenia (present at birth or within 72 hours) is most commonly caused by placental insufficiency or IUGR, maternal pre-eclampsia or hypertension, perinatal asphyxia, and congenital infection; neonatal alloimmune thrombocytopenia and maternal ITP are less frequent overall but are the key causes of severe isolated thrombocytopenia in an otherwise well term infant. Late-onset thrombocytopenia (after 72 hours) is most commonly caused by late-onset sepsis, necrotising enterocolitis, congenital infection, and catheter-related thrombosis. Distinguishing these aetiologies requires careful maternal history, examination, and targeted laboratory investigation. [8]
Clinical & Bedside Assessment
Begin with an overall assessment of whether the infant is sick or well, using the same gestalt approach as for any neonatal presentation. Measure temperature, heart rate, respiratory rate, blood pressure, and capillary refill time. An anaemic infant may show tachycardia with a weak pulse and prolonged capillary refill; a polycythaemic infant may appear ruddy with respiratory distress; and a thrombocytopenic infant should be examined for petechiae, purpura, and bleeding. [2]
Examine the skin carefully for pallor, plethora, petechiae, purpura, bruising, and jaundice. Palpate the abdomen for hepatosplenomegaly, which suggests haemolysis, congenital infection, or hydrops. Assess the anterior fontanelle for fullness or bulging. Listen to the heart for a gallop rhythm or murmur suggesting cardiac compromise from severe anaemia or hyperviscosity. Check for abnormal movements, irritability, or altered tone that may indicate intracranial haemorrhage or cerebral hypoperfusion. [7]
The maternal and perinatal history provides critical aetiological clues. For anaemia, ask about maternal blood group and antibody screen, anti-D prophylaxis, gestational diabetes, blood loss at delivery, and twin pregnancy. For polycythaemia, inquire about maternal diabetes, hypertension or pre-eclampsia, intrauterine growth restriction, high altitude, and cord clamping timing. For thrombocytopenia, the most important question is the maternal platelet count and whether any previous sibling had neonatal thrombocytopenia or unexplained intracranial haemorrhage, as this strongly suggests neonatal alloimmune thrombocytopenia. [9]
Investigations
The full blood count is the foundational investigation for all three conditions and provides the haemoglobin, haematocrit, mean corpuscular volume, reticulocyte count, platelet count, and white cell differential. A peripheral blood film gives crucial morphological information: spherocytes suggest hereditary spherocytosis or ABO incompatibility, bite cells and Heinz bodies suggest glucose-6-phosphate dehydrogenase deficiency, and schistocytes suggest microangiopathic haemolysis or disseminated intravascular coagulation. [8]
For anaemia, a direct antiglobulin test identifies antibody-coated red cells and confirms immune-mediated haemolysis. Serum bilirubin (both total and direct fractions) quantifies the degree of haemolysis. A Kleihauer-Betke test or flow cytometry for fetal haemoglobin in the maternal circulation detects significant fetomaternal haemorrhage. Glucose-6-phosphate dehydrogenase enzyme assay should be considered in male infants of appropriate ethnic backgrounds with unexplained haemolysis, though assay results are unreliable during an acute haemolytic episode because the most deficient cells have already been destroyed. [3]
For thrombocytopenia, confirming the platelet count on a peripheral smear excludes pseudothrombocytopenia from clumping. The maternal platelet count distinguishes alloimmune from autoimmune causes. Human platelet antigen genotyping of both parents and maternal antibody screening confirm neonatal alloimmune thrombocytopenia. A cranial ultrasound should be performed in any neonate with a platelet count below 50 times 10 to the 9 per litre or any neurological signs, to detect intracranial haemorrhage. Blood cultures, inflammatory markers, and coagulation studies investigate sepsis and disseminated intravascular coagulation. [9]
For polycythaemia, the critical investigation is a confirmed venous haematocrit, as capillary samples are unreliable. A central venous or arterial sample should be drawn if the heel-prick haematocrit is above 65 per cent. Additional investigations include blood glucose (hypoglycaemia), serum calcium, bilirubin, and renal function tests, and a cranial ultrasound in symptomatic infants to evaluate for thrombosis or ischaemia. [5]
Management — Resuscitation
The anaemic neonate in shock requires immediate resuscitation following the airway, breathing, circulation approach. Secure the airway and provide supplemental oxygen or positive-pressure ventilation for respiratory distress or apnoea. Establish intravenous access rapidly. If the haemoglobin is critically low and the infant is in heart failure or shock, an emergency red cell transfusion of 10 to 20 mL per kg of cytomegalovirus-negative, irradiated, leucodepleted packed red cells is given over 2 to 4 hours. In the moribund infant, uncrossmatched O-negative blood may be used while a full crossmatch is performed. [1]
For the polycythaemic infant with severe hyperviscosity symptoms such as seizures, respiratory failure, or signs of thrombosis, the immediate priority is to reduce the haematocrit while maintaining haemodynamic stability. Partial exchange transfusion replaces a calculated volume of the infant's blood with normal saline, lowering the haematocrit to approximately 55 per cent. The procedure must be performed with careful monitoring of blood pressure, glucose, and temperature, as complications include hypoglycaemia, thrombocytopenia, and necrotising enterocolitis. [5]
The thrombocytopenic neonate with active bleeding requires urgent platelet transfusion. The standard dose is 10 to 15 mL per kg of platelet concentrate, which typically raises the platelet count by 40 to 60 times 10 to the 9 per litre. In neonatal alloimmune thrombocytopenia, human platelet antigen 1a-negative platelets are preferred if available; if not, intravenous immunoglobulin combined with random donor platelets is used. Any infant with confirmed intracranial haemorrhage and thrombocytopenia requires immediate platelet transfusion to a target above 100 times 10 to the 9 per litre. [9]
Resuscitation sequence for neonatal haematological emergencies
Assess ABC: airway, breathing, circulation - provide oxygen or PPV as needed
Establish IV access and send urgent full blood count and blood gas
Anaemia in shock: emergency red cell transfusion 10-20 mL per kg
Polycythaemia with seizures: partial exchange transfusion with saline
Thrombocytopenia with bleeding: urgent platelet transfusion 10-15 mL per kg
Monitor: heart rate, blood pressure, glucose, perfusion, neurological status
Management — Definitive & Stepwise
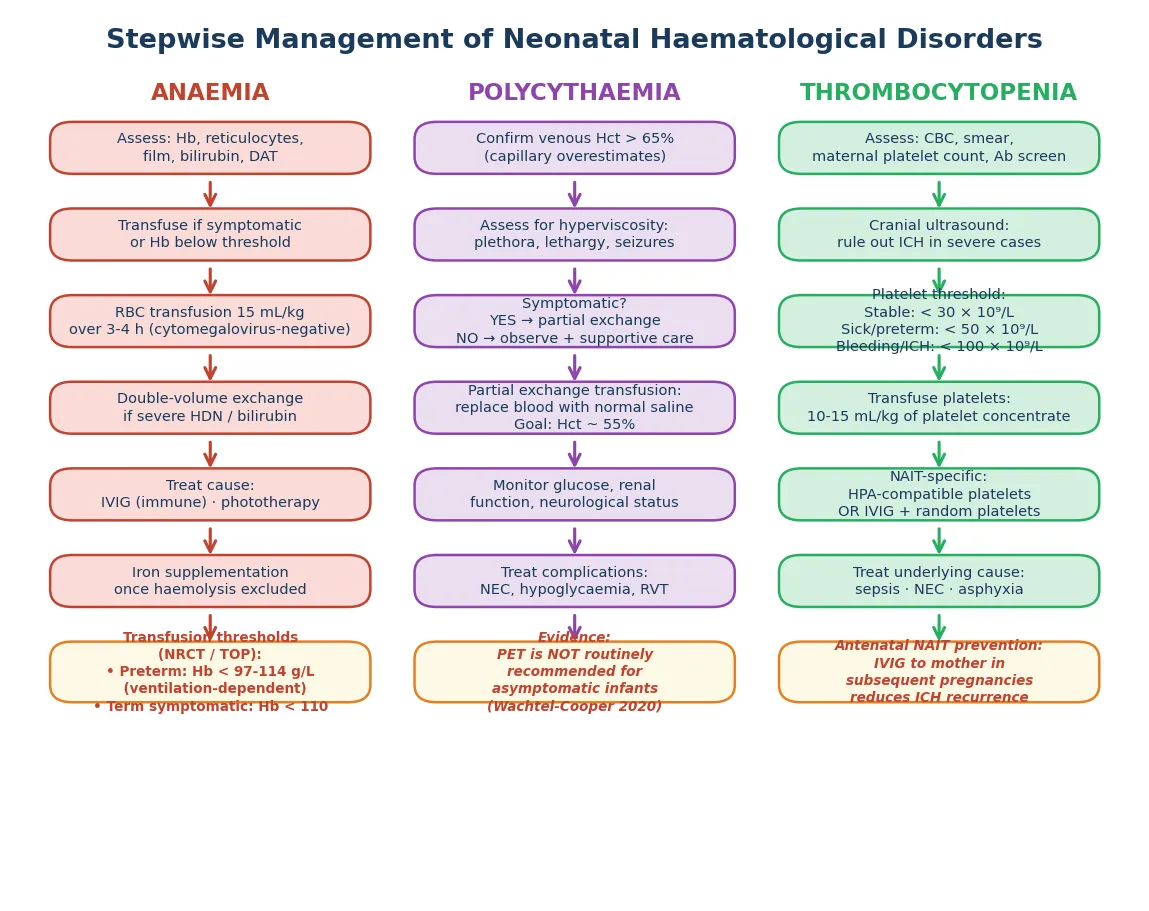
Red cell transfusion in preterm infants follows evidence-based thresholds derived from the multicentre transfusion trials. The largest of these compared a higher haemoglobin transfusion threshold strategy against a lower threshold strategy in extremely low birth weight infants and found no significant difference in the composite primary outcome of death or major morbidity, supporting a restrictive transfusion approach. Typical restrictive thresholds for preterm infants on the first day of life are a haemoglobin of 110 g per litre for those on mechanical ventilation, decreasing to 97 to 100 g per litre for stable infants. Term infants are transfused when symptomatic with a haemoglobin below 70 to 80 g per litre, or for acute blood loss causing haemodynamic compromise. [1]
Packed red blood cell transfusion
Dose
10-20 mL per kg
For haemolytic anaemia, treatment is cause-specific. Rhesus and other severe immune haemolytic diseases require phototherapy, intravenous immunoglobulin at 0.5 to 1 g per kg, and double-volume exchange transfusion when bilirubin approaches exchange levels or the anaemia is severe. Glucose-6-phosphate dehydrogenase deficiency management is supportive: stop the offending trigger, maintain hydration, and transfuse only if the haemoglobin falls dangerously low. The physiological anaemia of prematurity is managed with iron supplementation at 2 to 4 mg per kg per day starting at 2 to 4 weeks of age, and recombinant erythropoietin is used in some units to reduce transfusion exposure though its role remains debated. [2]
IV immunoglobulin (IVIG)
Dose
0.5-1 g per kg
The management of neonatal polycythaemia remains an area of active controversy. Partial exchange transfusion lowers the haematocrit effectively, but systematic reviews have found no consistent long-term neurodevelopmental benefit compared with symptomatic treatment alone. Current evidence-based practice reserves partial exchange transfusion for symptomatic infants with a confirmed venous haematocrit above 65 per cent, while asymptomatic infants receive supportive care with hydration, glucose monitoring, and observation. [5]
For thrombocytopenia, platelet transfusion thresholds are guided by the underlying condition and the infant's clinical status. The standard approach transfuses stable neonates at a platelet count below 30 times 10 to the 9 per litre, sick or preterm infants at below 50 times 10 to the 9 per litre, and any neonate with active bleeding or confirmed intracranial haemorrhage at below 100 times 10 to the 9 per litre. In neonatal alloimmune thrombocytopenia, human platelet antigen-compatible platelets (typically HPA 1a-negative) are the treatment of choice, supplemented by intravenous immunoglobulin when compatible platelets are not immediately available. [7]
Platelet transfusion
Dose
10-15 mL per kg
PLATELET transfusion thresholds
Specific Subtypes & Scenarios
Neonatal alloimmune thrombocytopenia is the most important thrombocytopenia subtype because of its severity and recurrence risk. It occurs when a platelet-antigen-negative mother carries a platelet-antigen-positive fetus, producing IgG antibodies that cross the placenta and destroy fetal platelets. The mother's own platelet count is normal, distinguishing it from maternal autoimmune thrombocytopenia. Severe thrombocytopenia below 50 times 10 to the 9 per litre at birth, petechiae within hours, and the absence of other illness in a term infant are the hallmark presentation. Intracranial haemorrhage occurs in 10 to 20 per cent of affected infants and may be the presenting feature. Management requires human platelet antigen-compatible platelets, and all future pregnancies require antenatal monitoring and treatment with maternal intravenous immunoglobulin to prevent recurrence. [9]
Rhesus haemolytic disease, though greatly reduced by antenatal and postnatal anti-D prophylaxis, remains the classic severe immune haemolytic anaemia. Anti-D immunoglobulin G crosses the placenta and binds D-positive fetal red cells, triggering progressive extravascular haemolysis that can cause severe anaemia, compensatory extramedullary haematopoiesis with hepatosplenomegaly, and hydrops fetalis with generalised oedema, ascites, and pleural effusions. Modern management includes antenatal middle cerebral artery peak systolic velocity monitoring to detect fetal anaemia, intrauterine transfusion for severely affected fetuses, and postnatal intensive phototherapy, intravenous immunoglobulin, and exchange transfusion as needed. [4]
ABO incompatibility causes a milder, often unpredictable haemolysis. It typically occurs in group A or B infants of group O mothers, who naturally produce immunoglobulin G anti-A and anti-B antibodies. Unlike rhesus disease, ABO incompatibility can affect the first pregnancy, produces a weaker and more variable haemolysis, and is rarely severe enough to cause hydrops. The direct antiglobulin test may be weakly positive, and the blood film shows spherocytes. Management is primarily supportive with phototherapy. [4]
Glucose-6-phosphate dehydrogenase deficiency is an X-linked disorder affecting hundreds of millions worldwide, with the highest prevalence in Mediterranean, African, Middle Eastern, and Southeast Asian populations. Affected males develop episodic haemolysis after exposure to oxidative triggers including fava beans, naphthalene (mothballs), sulphonamides, primaquine, and sepsis. In the neonate, it is an important cause of significant hyperbilirubinaemia requiring phototherapy or exchange transfusion, and screening is recommended in high-prevalence populations. [3]
The infant of a diabetic mother deserves special mention because polycythaemia, hypoglycaemia, hypocalcaemia, and respiratory distress commonly coexist. The chronic fetal hyperinsulinaemia and hypoxia of poorly controlled maternal diabetes drive erythropoietin production and red cell mass expansion, producing polycythaemia rates of 20 to 40 per cent. These infants need routine haematocrit screening, glucose monitoring, and a low threshold for confirming a venous haematocrit if the capillary value is elevated. [6]
[3]Complications & Pitfalls
The principal complication of untreated neonatal anaemia is progressive cardiac decompensation leading to congestive heart failure and shock. In the extreme preterm infant, repeated phlebotomy losses and inadequate iron replacement lead to iron deficiency anaemia, which has been associated with adverse long-term neurodevelopmental outcomes including impaired cognitive function and behavioural difficulties that may persist despite later iron repletion. The developing brain is particularly vulnerable to iron deficiency during periods of active myelination and neurotransmitter synthesis. [2]
The complications of polycythaemia and hyperviscosity result from end-organ hypoperfusion and thrombosis. Symptomatic hyperviscosity syndrome can produce seizures, stroke, renal vein thrombosis, necrotising enterocolitis, persistent pulmonary hypertension, and hypoglycaemia. However, the most important pitfall is over-treatment: performing partial exchange transfusion on asymptomatic infants or on the basis of an unconfirmed capillary haematocrit exposes the infant to procedural risks including thrombosis, infection, haemodynamic instability, and necrotising enterocolitis, without evidence of long-term benefit. [5]
The feared complication of neonatal thrombocytopenia is intracranial haemorrhage, which occurs most often in neonatal alloimmune thrombocytopenia but can complicate any severe thrombocytopenia. Intracranial haemorrhage in the neonate carries a mortality of up to 15 per cent and produces long-term neurodevelopmental disability including cerebral palsy, epilepsy, cognitive impairment, and sensorineural hearing loss in 25 to 50 per cent of survivors. The risk is greatest when the platelet count falls below 30 times 10 to the 9 per litre, and prophylactic platelet transfusion at appropriate thresholds is the primary prevention strategy. [9]
Major clinical pitfalls include failing to confirm polycythaemia with a venous sample before proceeding to partial exchange, treating asymptomatic polycythaemic infants unnecessarily, missing neonatal alloimmune thrombocytopenia in an otherwise healthy term neonate with isolated severe thrombocytopenia, using the wrong platelet product in NAIT (random donor platelets are less effective than HPA-compatible platelets), delaying iron supplementation in preterm infants, and failing to counsel families about the recurrence risk of NAIT in future pregnancies. [8]
Prognosis & Disposition
The prognosis for neonatal anaemia depends on the underlying cause and the speed of correction. Acute blood loss from fetomaternal haemorrhage, once corrected with transfusion, carries an excellent prognosis if the infant did not suffer a prolonged hypoxic insult. Haemolytic anaemia from rhesus disease has a good prognosis with modern antenatal management and postnatal intensive care, though severe cases complicated by hydrops carry higher mortality. The long-term prognosis of iron deficiency anaemia in preterm infants is the principal concern, as early iron deficiency has been linked to persistent neurodevelopmental deficits. [2]
For polycythaemia, the short-term prognosis for asymptomatic infants is excellent, and the majority recover without sequelae as the haematocrit falls naturally over the first weeks of life. Symptomatic infants with hyperviscosity syndrome are at risk of neurological and gastrointestinal complications, and long-term studies show variable outcomes with some reporting increased rates of neurodevelopmental delay regardless of whether partial exchange transfusion was performed. [5]
The prognosis after neonatal thrombocytopenia depends on whether intracranial haemorrhage occurred. Infants without intracranial haemorrhage recover fully as the platelet count normalises over days to weeks. Those who suffered intracranial haemorrhage require long-term neurodevelopmental follow-up, and approximately 25 to 50 per cent have detectable disability. Every infant treated for neonatal alloimmune thrombocytopenia requires referral for future pregnancy counselling and antenatal management planning. [9]
Disposition decisions require confirmation that the underlying disorder has been addressed or stabilised, that the haemoglobin, haematocrit, or platelet count is trending in the right direction, and that the infant is feeding adequately and maintaining normal glucose and temperature. Arrange structured outpatient follow-up with repeat blood counts, developmental surveillance for any infant with intracranial haemorrhage, and genetic or haematology referral for inherited disorders. [7]
Special Populations
Preterm and extremely low birth weight infants are the highest-risk group for all three disorders. Their immature erythropoietic and megakaryocytic systems, shortened red cell lifespan, iatrogenic blood loss from frequent phlebotomy, and prolonged hospitalisation with central venous catheters all increase the risk of anaemia and thrombocytopenia. The physiological anaemia of prematurity is universal, and virtually all extremely preterm infants receive at least one red cell transfusion during their NICU stay. Restrictive transfusion thresholds guided by trial evidence minimise unnecessary exposure. [1]
Infants of diabetic mothers are a specific high-risk group for polycythaemia, with rates of 20 to 40 per cent, alongside their well-known risks of hypoglycaemia, hypocalcaemia, respiratory distress, and congenital anomalies. These infants require routine haematocrit screening and proactive management of the metabolic complications that accompany polycythaemia. Twin pregnancies complicated by twin-twin transfusion syndrome produce both a polycythaemic recipient and an anaemic donor, and both twins require haematological assessment at birth. [6]
In populations with high prevalence of glucose-6-phosphate dehydrogenase deficiency, including Mediterranean, Middle Eastern, Southeast Asian, and West African communities, neonatal screening and parental education about trigger avoidance are essential. Severe neonatal hyperbilirubinaemia from glucose-6-phosphate dehydrogenase deficiency remains a significant cause of kernicterus in these populations, and early recognition with phototherapy and exchange transfusion when indicated is critical. In Indigenous and migrant communities in Australia and New Zealand, access to antenatal screening, blood typing, and specialised blood products may be limited, necessitating proactive planning. [3]
[3]Evidence, Guidelines & Regional Differences
The evidence base for neonatal transfusion thresholds has been transformed by large multicentre randomised controlled trials. The largest of these compared higher versus lower haemoglobin transfusion thresholds in extremely low birth weight infants and found no significant difference in death or major morbidity between strategies, supporting a restrictive approach that minimises donor exposure. These findings underpin current guidelines from the American Academy of Pediatrics, the British Committee for Standards in Haematology, and equivalent bodies worldwide. [1]
The management of neonatal polycythaemia and hyperviscosity remains controversial. Systematic reviews of partial exchange transfusion versus expectant management have found that while the procedure lowers the haematocrit, it does not consistently improve long-term neurodevelopmental outcomes, and it carries procedural risks. Current practice in most units reserves partial exchange transfusion for symptomatic infants, while acknowledging the limited evidence base. [5]
For neonatal thrombocytopenia, platelet transfusion thresholds remain an area of evolving evidence. The platelet transfusion thresholds in premature neonates trial compared a high threshold (50 times 10 to the 9 per litre) versus a low threshold (25 times 10 to the 9 per litre) strategy and found that the higher threshold was associated with more major bleeding and mortality, challenging conventional practice and supporting a more restrictive approach. International consensus recommendations for neonatal alloimmune thrombocytopenia provide standardised diagnostic and treatment algorithms, including antenatal intravenous immunoglobulin for at-risk pregnancies. [7]
[7]Ongoing controversies and research priorities include the optimal iron supplementation regimen and timing for preterm infants, the role of recombinant erythropoietin in reducing transfusion exposure, the long-term neurodevelopmental effects of early iron deficiency, the best platelet transfusion strategy for sick and preterm neonates, whether partial exchange transfusion for polycythaemia has any long-term benefit, and strategies to prevent neonatal alloimmune thrombocytopenia in subsequent pregnancies. Antenatal non-invasive testing for fetal platelet antigens using cell-free fetal DNA is an emerging technology that may improve the targeted management of at-risk pregnancies. [2]
Exam Pearls
ABC of neonatal blood disorders
References
- [1]Kirpalani H Higher or Lower Hemoglobin Transfusion Thresholds for Preterm Infants. N Engl J Med, 2020.PMID 33382931
- [2]Gisslen T Anemia, Iron Supplementation, and the Brain. Clin Perinatol, 2023.PMID 37866852
- [3]Luzzatto L Glucose-6-Phosphate Dehydrogenase Deficiency. Hematol Oncol Clin North Am, 2016.PMID 27040960
- [4]de Haas M Anti-D prophylaxis: past, present and future. Transfus Med, 2014.PMID 25121157
- [5]Schimmel MS Neonatal polycythemia: is partial exchange transfusion justified? Clin Perinatol, 2004.PMID 15325537
- [6]Bashir BA Neonatal polycythaemia. Sudan J Paediatr, 2019.PMID 31969734
- [7]Stanworth SJ How I diagnose and treat neonatal thrombocytopenia. Blood, 2023.PMID 36787503
- [8]Roberts I Neonatal thrombocytopenia: causes and management. Arch Dis Child Fetal Neonatal Ed, 2003.PMID 12937037
- [9]Lieberman L Fetal and neonatal alloimmune thrombocytopenia: recommendations for evidence-based practice, an international approach. Br J Haematol, 2019.PMID 30828796
- [10]Society for Maternal-Fetal Medicine Society for Maternal-Fetal Medicine (SMFM) clinical guideline #7: nonimmune hydrops fetalis. Am J Obstet Gynecol, 2015.PMID 25557883