Paeds · fetal-neonatal-and-perinatal
Neonatal bacterial infection and sepsis: risk assessment and management
Also known as Neonatal sepsis · Early-onset sepsis · Late-onset sepsis · Neonatal bacterial infection · Neonatal meningitis
Fellowship guide to neonatal bacterial infection and sepsis: early- versus late-onset patterns, maternal and neonatal risk stratification, the clinical assessment of the unwell neonate, blood culture and biomarker interpretation, empiric antibiotic selection with doses, antibiotic stewardship, complications including meningitis, and long-term neurodevelopmental outcomes.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Neonatal bacterial infection is a systemic or localised bacterial disease occurring in the first 28 days of life, and it remains one of the most time-critical diagnoses in paediatrics. The neonate mounts a muted, unreliable inflammatory response, so the window between subtle non-specific signs and catastrophic collapse can be measured in hours rather than days. Early recognition, prompt cultures, and immediate empiric antibiotics are the difference between full recovery and death or lifelong disability. [3]
Clinicians separate neonatal bacterial infection into early-onset sepsis (EOS), presenting within 72 hours of birth and arising from organisms acquired vertically from the maternal genital tract, and late-onset sepsis (LOS), presenting after 72 hours and reflecting nosocomial or community-acquired pathogens. Group B Streptococcus and Escherichia coli dominate the early-onset landscape, while coagulase-negative staphylococci, Staphylococcus aureus, and Gram-negative bacilli are the chief late-onset culprits. [2]
Sepsis in neonates denotes a systemic inflammatory response to proven or suspected infection, and it can progress rapidly to severe sepsis with organ dysfunction and septic shock with persistent hypotension and perfusion failure. The distinction between culture-proven infection and clinically suspected infection matters for epidemiology and stewardship but must never delay treatment, because untreated neonatal sepsis carries a mortality of 10 to 20 per cent even in well-resourced settings. [5]
Epidemiology & Risk Factors
The overall incidence of early-onset sepsis in high-income countries is approximately 0.5 to 1 per 1000 live births, and it has fallen steadily since the introduction of maternal intrapartum antibiotic prophylaxis for group B Streptococcus. Despite this decline, GBS remains the single most common EOS pathogen in term infants, while E. coli has emerged as the leading Gram-negative cause and the dominant cause of EOS mortality in very low birth weight infants. [2]
Late-onset sepsis disproportionately affects premature and hospitalised infants. Among very low birth weight neonates in the NICHD Neonatal Research Network, 21 per cent developed at least one episode of late-onset sepsis, and those with culture-proven LOS had significantly higher mortality than uninfected peers. Coagulase-negative staphylococci accounted for nearly half of all LOS episodes in this population, reflecting the role of central venous catheters and invasive devices. [1]
The major maternal risk factors for early-onset sepsis are group B Streptococcus colonisation, clinical chorioamnionitis (maternal fever with fetal tachycardia, uterine tenderness, or purulent liquor), prolonged rupture of membranes for 18 hours or more, and preterm labour. Neonatal risk factors include prematurity, low birth weight, and being born to a mother who received inadequate intrapartum antibiotic prophylaxis. For late-onset sepsis, the key risk factors are prematurity, central venous catheter use, prolonged mechanical ventilation, parenteral nutrition, postsurgical status, and prolonged NICU stay. [2]
Pathophysiology
The newborn immune system is developmentally immature at every level of host defence, and this immaturity is most pronounced in preterm infants. Complement activity and opsonic capacity are reduced, limiting the ability to coat and destroy invading bacteria. Circulating immunoglobulin levels are low, particularly in premature infants who have not yet received the bulk of transplacental maternal IgG transfer that occurs in the third trimester. [3]
Neonatal neutrophils show impaired chemotaxis, phagocytosis, and intracellular killing compared with adult cells, and neonatal bone marrow has a limited pool of stored neutrophils that can be released in response to infection. The cytokine profile skews towards a T-helper-2 phenotype with blunted T-helper-1 responses, reducing the ability to mount an effective defence against intracellular organisms. These deficits explain why neonatal sepsis can escalate from subtle signs to overwhelming bacteraemia within hours. [3]
In early-onset disease, organisms ascend from the vagina through ruptured or occasionally intact membranes, infect the amniotic fluid, and are aspirated or swallowed by the fetus. The bacteria then seed the lungs, bloodstream, or meninges. In late-onset disease, pathogens typically invade through breached skin or mucosal barriers, most commonly at central venous catheter insertion sites, endotracheal tube interfaces, surgical wounds, or disrupted gastrointestinal mucosa with bacterial translocation. [1]
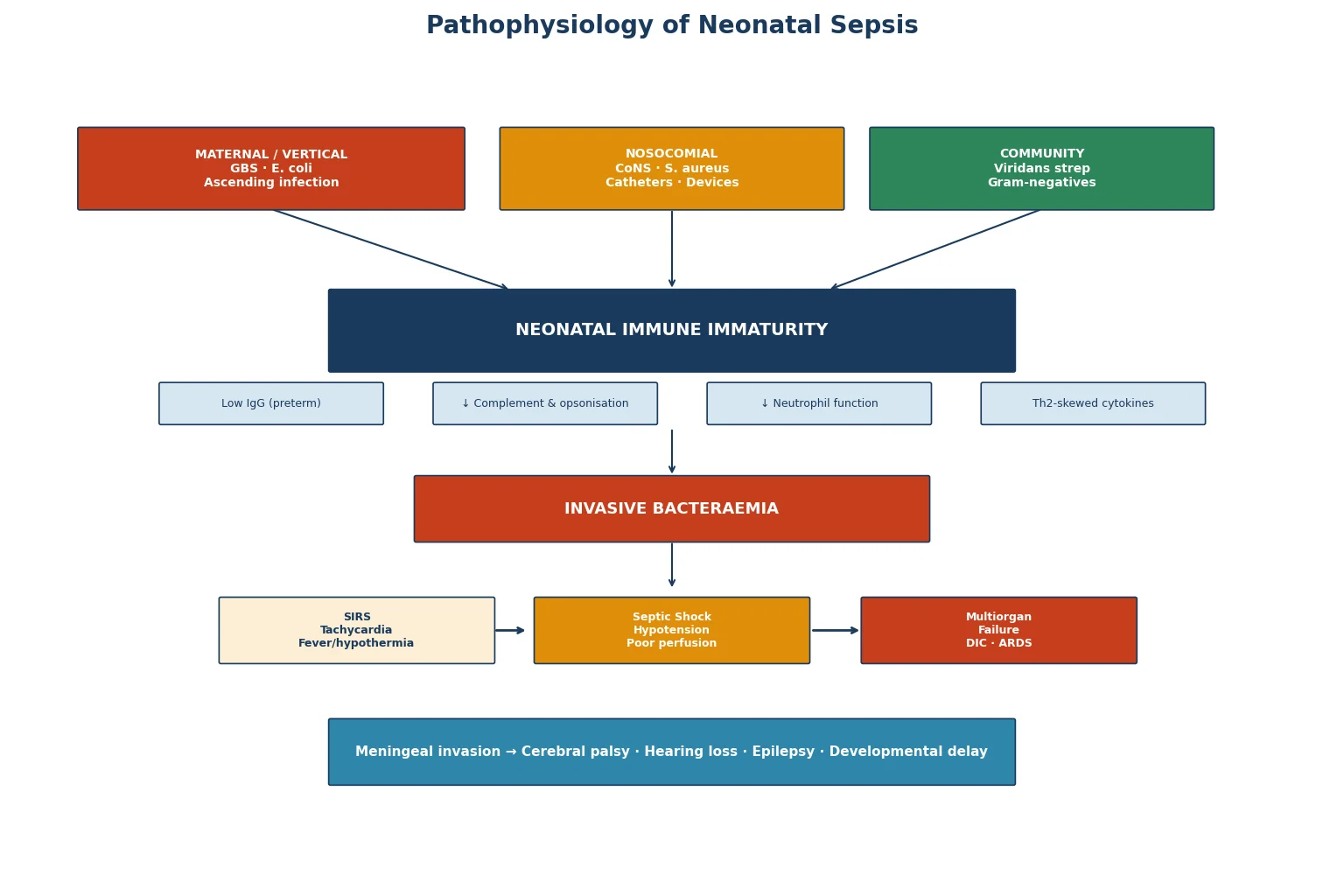
Once bacteraemic, the immature reticuloendothelial system fails to contain the infection, triggering an uncontrolled inflammatory cascade. Endothelial activation, capillary leak, vasodilation, and disseminated intravascular coagulation produce the clinical picture of septic shock with hypotension, metabolic acidosis, pulmonary hypertension, and progressive multiorgan failure. [5]
Classification
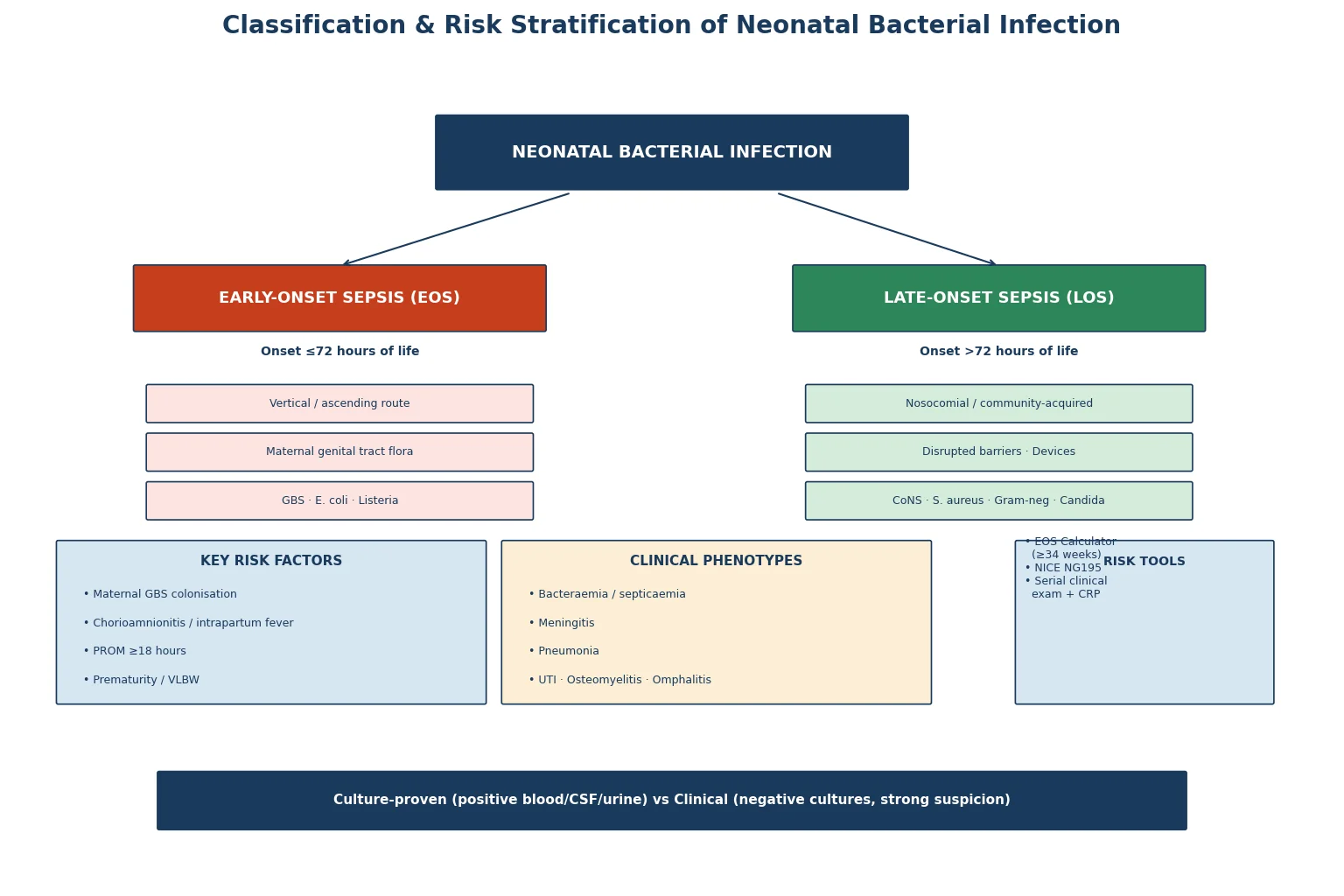
Early-onset infection encompasses pneumonia, bacteraemia without a focus, and meningitis, with the lungs being the most common portal of entry. Late-onset infection includes bacteraemia, meningitis, urinary tract infection, osteomyelitis, septic arthritis, omphalitis, and soft tissue infection. Distinguishing these two categories guides empiric antibiotic selection and helps clinicians anticipate likely organisms and their resistance profiles. [6]
Clinical Presentation
The cardinal feature of neonatal sepsis is non-specificity. Temperature instability, either hypo- or hyperthermia, is the single most common presenting sign. Respiratory distress - grunting, tachypnoea, retractions, nasal flaring, apnoea, or an increasing oxygen requirement - is frequently the first objective abnormality, especially when the lungs are the portal of entry. [2]
Cardiovascular signs include tachycardia, poor peripheral perfusion, skin mottling, prolonged capillary refill of three seconds or more, hypotension, and metabolic acidosis. Gastrointestinal manifestations range from poor feeding and vomiting to abdominal distension and bloody stools, the latter overlapping with necrotising enterocolitis. Neurological deterioration may manifest as lethargy, irritability, hypotonia, seizures, or a full or bulging fontanelle suggesting meningitis. [3]
Presenting signs by frequency
Temperature instability (hypo- or hyperthermia)
Respiratory distress, apnoea, increasing oxygen need
Poor feeding, vomiting, abdominal distension
Lethargy, hypotonia, irritability, seizures
Mottling, prolonged capillary refill, hypotension
Petechiae, purpura, grey or dusky appearance
Differential Diagnosis
The differential diagnosis for a non-specific, unwell neonate is broad and includes both infectious and non-infectious conditions that can mimic sepsis with identical clinical features. Respiratory distress syndrome from surfactant deficiency and transient tachypnoea of the newborn can both mimic early-onset pneumonia. Congenital heart disease, especially duct-dependent lesions presenting with shock or left-heart outflow obstruction causing poor perfusion, is a critical non-infectious mimic that must not be missed. [3]
Metabolic disease, particularly inborn errors of metabolism presenting with lethargy, poor feeding, metabolic acidosis, or hyperammonaemia, can mimic sepsis precisely and require specific assays for diagnosis. Hypoglycaemia produces identical non-specific signs and must be checked at the bedside in every unwell neonate. Necrotising enterocolitis presents with abdominal distension and bloody stools. [3]
Viral infections are important mimics and co-pathogens: enterovirus and parechovirus can cause a sepsis-like illness with hepatitis and myocarditis; herpes simplex virus can present with vesicular skin lesions, hepatitis, or encephalitis; and respiratory syncytial virus causes bronchiolitis with apnoea in young infants. Fungal infection with Candida species is a consideration in preterm infants with prolonged antibiotic exposure and central venous catheters. [5]
Clinical & Bedside Assessment
Begin every assessment with an overall gestalt judgement: does this infant look sick or well? The sick neonate appears lethargic, mottled, poorly perfused, and may have a high-pitched or feeble cry. Measure temperature, heart rate, respiratory rate, blood pressure, and capillary refill time. Examine the anterior fontanelle for fullness or bulging, which suggests raised intracranial pressure from meningitis. Assess tone, spontaneous activity, and response to stimulation. [4]
Examine the skin for petechiae, purpura, pustules, cellulitis, and a grey or dusky colour. Inspect the umbilicus for redness, discharge, or foul odour suggesting omphalitis. Auscultate the chest for crackles, wheeze, or decreased air entry. Palpate the abdomen for distension, tenderness, or absent bowel sounds. Review the maternal and perinatal history for GBS colonisation status, chorioamnionitis, duration of membrane rupture, intrapartum fever, and adequacy of intrapartum antibiotic prophylaxis. [4]
For infants born at 34 weeks gestation or more, the Neonatal Early-Onset Sepsis Calculator provides a validated, quantitative risk stratification tool that combines maternal risk factors with the infant's clinical presentation to estimate the probability of EOS and guide decisions about evaluation, empiric antibiotics, and observation. The updated 2024 version uses a contemporary cohort reflecting current epidemiology and intrapartum antibiotic practices. [7]
Investigations
Blood culture is the cornerstone diagnostic test and must be obtained before starting antibiotics whenever possible, using strict aseptic technique with an adequate volume of at least 1 mL to maximise yield. A single positive blood culture with a recognised pathogen confirms bacteraemia, while coagulase-negative staphylococci in a single culture require clinical judgement to distinguish true bacteraemia from contamination. [6]
The complete blood count with differential provides supportive data. Neutropenia, defined as an absolute neutrophil count below the age-appropriate reference range, is a concerning finding. An elevated immature-to-total neutrophil ratio above 0.2 is supportive of infection but has imperfect sensitivity and specificity. Thrombocytopenia is a late and non-specific marker. These haematological indices should never be used in isolation to decide whether to start or stop antibiotics. [6]
C-reactive protein trends over 24 to 48 hours carry more diagnostic weight than any single value. A normal CRP at baseline and again at 24 hours carries a negative predictive value exceeding 99 per cent for excluding early-onset sepsis, making it a powerful stewardship tool for safely discontinuing antibiotics in culture-negative, well-appearing infants. Procalcitonin has higher early sensitivity but requires age-specific reference ranges. Biomarker meta-analyses confirm that combining maternal and neonatal markers improves early diagnostic accuracy. [10]
Lumbar puncture for cerebrospinal fluid analysis is indicated when meningitis is suspected clinically, when the blood culture is positive, or when the infant is critically unwell. CSF should be sent for cell count, differential, protein, glucose, Gram stain, and culture. A normal CSF cell count does not fully exclude meningitis, particularly early in the course, and repeat LP may be needed if clinical suspicion persists. Urine culture obtained by suprapubic aspiration or sterile catheterisation is essential for evaluating late-onset infection. [6]
Management - Resuscitation
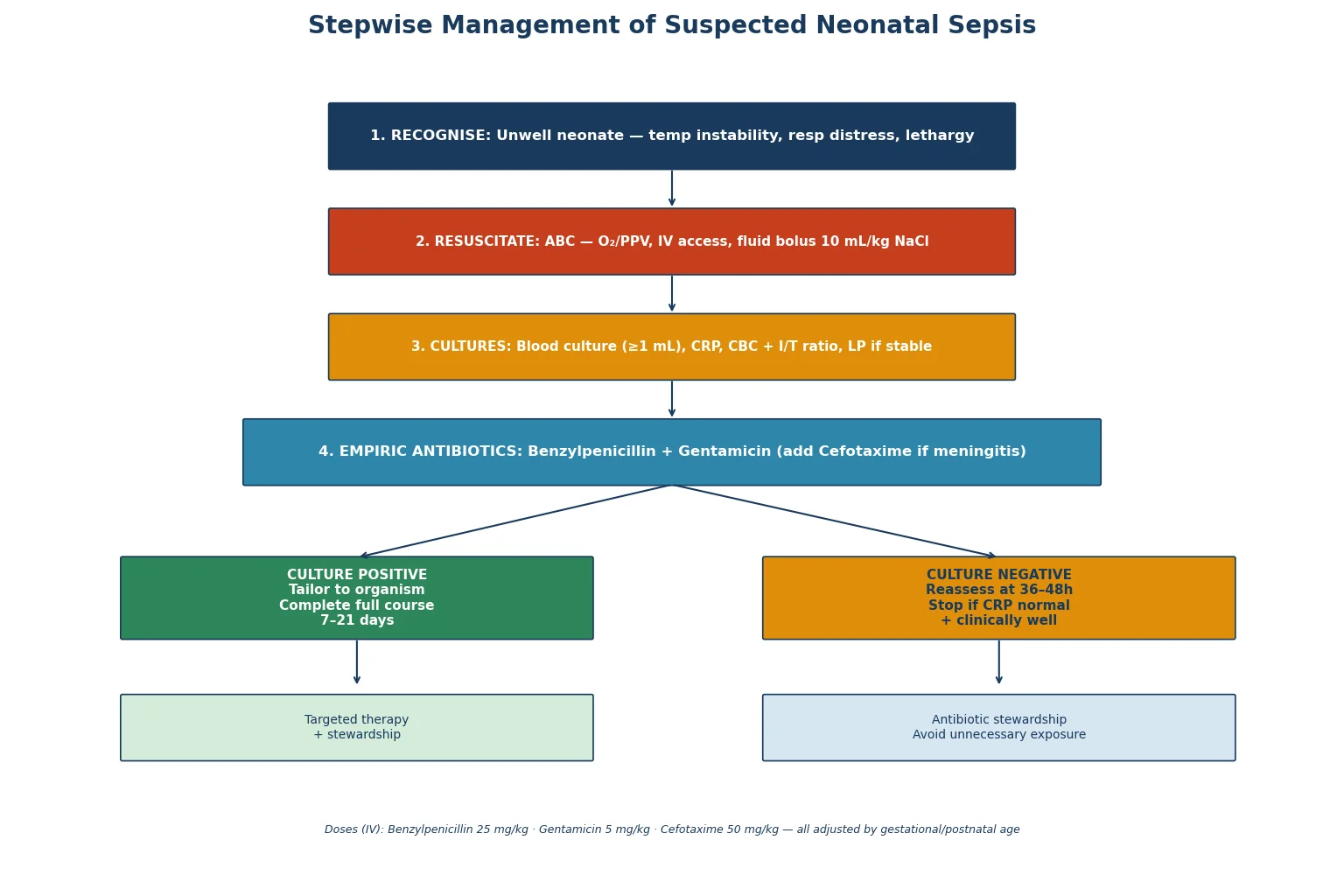
An infant with suspected sepsis and signs of shock requires immediate resuscitation using the ABC approach. Secure the airway and provide supplemental oxygen or positive-pressure ventilation for apnoea, grunting, or respiratory failure. Establish intravenous or intraosseous access rapidly - do not delay more than a few minutes attempting peripheral access before moving to intraosseous. [4]
Give a 10 mL/kg bolus of isotonic crystalloid (0.9 per cent sodium chloride) for hypotension or poor perfusion, reassessing the infant after each bolus. Watch for hepatomegaly and increasing oxygen requirement as signs of volume overload, particularly in preterm infants. Repeat boluses up to a total of 30 to 60 mL/kg may be required in septic shock, but excessive fluid resuscitation can worsen outcomes in preterm infants. [4]
Start broad-spectrum empiric antibiotics immediately after obtaining cultures, but never delay antibiotics if cultures cannot be obtained promptly. The standard first-line empiric regimen for suspected early-onset sepsis is intravenous benzylpenicillin or ampicillin combined with an aminoglycoside (gentamicin). Add a third-generation cephalosporin (cefotaxime) if meningitis is suspected, as it achieves therapeutic CSF concentrations. Correct hypoglycaemia and electrolyte disturbances, and monitor continuously for progression to septic shock requiring inotrope support. [4]
Resuscitation sequence for the septic neonate
Assess ABC: airway, breathing, circulation - provide oxygen or PPV as needed
Establish IV or IO access within minutes
Draw blood culture, CRP, CBC, and glucose before antibiotics
Fluid bolus 10 mL per kg 0.9 per cent NaCl for shock - reassess after each
Empiric antibiotics: benzylpenicillin and gentamicin (add cefotaxime if meningitis)
Monitor continuously: heart rate, BP, perfusion, glucose, urine output
Management - Definitive & Stepwise
Empiric antibiotic therapy for suspected early-onset sepsis in an infant of 34 weeks or more is benzylpenicillin 25 mg/kg intravenously combined with gentamicin 5 mg/kg intravenously, with dosing intervals adjusted for gestational and postnatal age. For suspected meningitis, use cefotaxime 50 mg/kg intravenously 6-hourly plus ampicillin or benzylpenicillin to cover Listeria. Tailor therapy once culture and sensitivity results are available, typically at 36 to 48 hours. [4]
Treatment duration depends on the confirmed diagnosis and organism. Uncomplicated bacteraemia requires 7 to 10 days of targeted therapy. Group B Streptococcus meningitis requires 14 to 21 days, while Gram-negative meningitis requires at least 21 days and often longer. Urinary tract infection typically needs 7 to 14 days. Therapeutic drug monitoring for aminoglycosides ensures adequate peak levels for efficacy and non-toxic trough levels to protect renal and auditory function. [6]
The antibiotic stewardship principle is central to modern neonatal sepsis management. Reassess every treated infant at 36 to 48 hours. If cultures are negative, CRP has normalised, and the infant is clinically well, stop antibiotics. This approach reduces unnecessary antibiotic exposure, length of stay, and antibiotic-associated complications such as necrotising enterocolitis and fungal colonisation without increasing missed infections. [8]
STOP stewardship criteria
Supportive care runs in parallel with antimicrobial therapy. Maintain normothermia, as both hypothermia and hyperthermia worsen outcomes. Manage fluids and electrolytes carefully, providing adequate nutrition via enteral or parenteral routes. Ensure glycaemic stability, as both hypoglycaemia and hyperglycaemia are harmful. Remove infected central venous catheters promptly in confirmed catheter-related bloodstream infection. [8]
Specific Subtypes & Scenarios
Early-onset GBS disease typically presents within the first 24 hours of life with respiratory distress, grunting, and a rapidly progressive course to shock. The classic radiographic picture resembles respiratory distress syndrome, and the infant may deteriorate despite surfactant administration. Prompt recognition and empiric antibiotics are essential, as the mortality of untreated GBS pneumonia and septicaemia exceeds 10 per cent even in term infants. [2]
Escherichia coli early-onset infection is more common in preterm infants and carries a higher case fatality rate than GBS disease. The rising prevalence of ampicillin-resistant E. coli strains, partly driven by widespread intrapartum antibiotic prophylaxis, has important implications for empiric therapy. Listeria monocytogenes is rare but distinctive, causing a characteristic granulomatous rash known as infantiseptica, and requires ampicillin plus gentamicin as third-generation cephalosporins are ineffective against Listeria. [2]
Late-onset GBS disease frequently presents as meningitis, with up to 30 per cent of late-onset GBS cases involving the central nervous system. Coagulase-negative staphylococcal late-onset sepsis in the preterm infant with a central venous catheter is typically less fulminant but requires prompt catheter removal for persistent bacteraemia. Staphylococcus aureus and Gram-negative organisms cause more aggressive late-onset disease with higher rates of metastatic infection and shock. [1]
Neonatal herpes simplex virus infection, though viral, is the most critical non-bacterial mimic to consider. It presents with vesicular skin lesions, fulminant hepatitis, or encephalitis, and requires intravenous aciclovir. Consider HSV in any neonate with CSF pleocytosis and negative bacterial cultures, particularly if maternal history is suggestive or if skin vesicles are present. Focal infections such as osteomyelitis, septic arthritis, and cellulitis require prolonged targeted therapy and orthopaedic involvement. [9]
[5]Complications & Pitfalls
Mortality from neonatal sepsis ranges from approximately 5 per cent in term infants to 20 per cent in very low birth weight infants. Gram-negative early-onset sepsis carries the highest case fatality, and infants requiring inotrope support or mechanical ventilation have significantly worse outcomes. The dominant long-term concern is the neurodevelopmental impact of neonatal meningitis: long-term follow-up studies show that serious neonatal bacterial infections are associated with increased rates of cerebral palsy, epilepsy, cognitive impairment, and developmental delay. [9]
After neonatal meningitis, approximately 25 per cent of survivors have moderate-to-severe neurodevelopmental disability. Sensorineural hearing loss occurs in up to 10 per cent of survivors and may be progressive, mandating audiology assessment at discharge and ongoing developmental surveillance. Epilepsy develops in approximately 10 per cent, and cognitive impairment affects 15 to 20 per cent. These outcomes underscore the importance of prevention, early treatment, and comprehensive follow-up. [9]
Major clinical pitfalls include delaying antibiotics to obtain cultures in a deteriorating infant, sending an inadequate blood culture volume producing false-negative cultures, failing to perform lumbar puncture when meningitis is plausible, and treating culture-negative well-appearing infants with prolonged unnecessary antibiotics. Additional traps include not removing an infected central venous catheter, missing herpes simplex encephalitis in an infant with CSF pleocytosis and negative bacterial cultures, and failing to recognise that normal initial inflammatory markers do not exclude sepsis. [8]
Prognosis & Disposition
Term infants with promptly treated early-onset sepsis who respond clinically within 48 to 72 hours generally have an excellent prognosis with full recovery. The key determinant of outcome is the speed of recognition and treatment, as delays in antibiotic administration are independently associated with increased mortality and morbidity. Premature and very low birth weight infants have significantly worse outcomes at every stage. [9]
The neurodevelopmental outcome after meningitis is the principal long-term concern. All infants treated for meningitis or severe sepsis require structured outpatient follow-up including audiology assessment, developmental surveillance, and neurological examination. Arrange early intervention services for infants showing signs of developmental delay. Counsel families about the importance of prompt presentation for any future illness, as infants who have had one episode of sepsis may be at increased risk of recurrence. [9]
Disposition after treatment requires confirming that the infant is feeding adequately, maintaining temperature stability in an open cot, and demonstrating sustained weight gain before discharge. Ensure that families understand warning signs and have a clear safety-net plan for re-presentation. Arrange multidisciplinary follow-up for any infant with a complicated course, particularly those who required prolonged ventilation, inotropes, or treatment for meningitis. [9]
Special Populations
Preterm and very low birth weight infants are the highest-risk group for neonatal sepsis. Their immature immune defences, prolonged hospitalisation, invasive devices, and dependence on parenteral nutrition all increase the risk of late-onset sepsis. Coagulase-negative staphylococci and Candida species are particularly important pathogens in this population. Empiric antibiotic regimens for suspected LOS in preterm infants often include vancomycin or flucloxacillin for staphylococcal cover, tailored to local resistance patterns and unit protocols. [1]
Infants with congenital anomalies such as neural tube defects, congenital heart disease, or urinary tract abnormalities are predisposed to specific infections that may present with sepsis. Immunocompromised neonates, including those with severe combined immunodeficiency or congenital neutropenia, present unique diagnostic and management challenges and require involvement of immunology and infectious diseases specialists. [5]
In Indigenous and remote communities across Australia and New Zealand, higher rates of GBS colonisation, later presentation to health services, and reduced access to tertiary neonatal care all contribute to increased incidence and severity of neonatal sepsis. Culturally safe, family-centred care with interpreter access and clear discharge communication is essential. In low- and middle-income countries, limited diagnostic capacity, higher rates of multidrug-resistant organisms, and reduced access to neonatal intensive care dramatically worsen outcomes, with neonatal sepsis mortality exceeding 20 per cent in many settings. [5]
[5]Evidence, Guidelines & Regional Differences
The American Academy of Pediatrics 2018 clinical practice guideline for management of suspected EOS in infants born at 35 weeks gestation or more provides the current standard of care in North America. This guideline uses a risk factor-based algorithm incorporating the Neonatal Early-Onset Sepsis Calculator, serial physical examination over 48 hours, and biomarker trends with CRP measured at 6 to 24 hours. The updated 2024 calculator utilises a contemporary cohort reflecting current epidemiology. [7]
This approach has significantly reduced empiric antibiotic use compared with older categorical risk-factor algorithms, without increasing missed infections. The NICE guideline NG195 in the United Kingdom provides complementary recommendations for the early recognition, investigation, and management of neonatal infection, emphasising the role of maternal risk factors and serial infant observation. [4]
[4]Controversies and active research areas include the optimal role of procalcitonin-guided antibiotic duration, whether well-appearing at-risk infants can be safely observed without empiric antibiotics, the appropriate duration of culture-negative sepsis treatment, the choice between universal and risk-based GBS screening strategies, and the rising threat of antimicrobial resistance, especially from extended-spectrum beta-lactamase-producing E. coli. Ongoing global surveillance and antimicrobial stewardship programmes are essential to preserve the effectiveness of current first-line agents. [8]
Exam Pearls
FEVER approach
References
- [1]Stoll BJ Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics, 2002.PMID 12165580
- [2]Stoll BJ Early onset neonatal sepsis: the burden of group B Streptococcal and E. coli disease continues. Pediatrics, 2011.PMID 21518717
- [3]Shane AL Neonatal sepsis: progress towards improved outcomes. J Infect, 2014.PMID 24140138
- [4]Puopolo KM Management of Neonates Born at >=35 0/7 Weeks' Gestation With Suspected or Proven Early-Onset Bacterial Sepsis. Pediatrics, 2018.PMID 30455342
- [5]Fleischmann-Struzek C The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Respir Med, 2018.PMID 29508706
- [6]Polin RA Management of neonates with suspected or proven early-onset bacterial sepsis. Pediatrics, 2012.PMID 22547779
- [7]Kuzniewicz MW Update to the Neonatal Early-Onset Sepsis Calculator Utilizing a Contemporary Cohort. Pediatrics, 2024.PMID 39314183
- [8]Kuzniewicz MW Antibiotic stewardship for early-onset sepsis. Semin Perinatol, 2020.PMID 33221072
- [9]Thomas R Long-term impact of serious neonatal bacterial infections on neurodevelopment. Clin Microbiol Infect, 2024.PMID 37084940
- [10]van Leeuwen LM Diagnostic value of maternal, cord blood and neonatal biomarkers for early-onset sepsis: a systematic review and meta-analysis. Clin Microbiol Infect, 2024.PMID 38467246