Paeds · fetal-neonatal-and-perinatal
Neonatal cyanosis and collapsed neonate
Also known as Neonatal cyanosis and collapsed neonate · The blue baby · The collapsed newborn · Central cyanosis in the newborn · Duct-dependent collapse
Fellowship guide to the blue or collapsed neonate: recognising central cyanosis and shock, the five-cause differential, the hyperoxia test and pre-/post-ductal saturation split, the first-hour bundle, and the time-critical use of prostaglandin E1 for duct-dependent lesions.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the infant first: a two-day-old term baby, previously feeding well, now dusky and limp in the mother's arms, the tongue and lips a slate blue, breathing fast but not particularly hard. That is the prototypical presentation — central cyanosis, often with surprisingly little respiratory distress, on the second or third day of life. The colour change is not subtle, and the tempo is the clue: a baby who was well hours ago is now blue. The first question is not "what is the diagnosis?" but "is this an emergency?" and the answer is almost always yes. [3]
Cyanosis is the blue discolouration of skin and mucous membranes that appears when the concentration of deoxyhaemoglobin in capillary blood exceeds about 3 g/dL. Two consequences follow that examiners test. First, cyanosis is a late and unreliable sign of hypoxaemia — the infant can be profoundly hypoxic long before looking blue. Second, an anaemic infant may be severely hypoxaemic and never turn blue, because there is not enough haemoglobin to generate the threshold concentration of deoxyhaemoglobin, while a polycythaemic infant looks blue at milder desaturation. The colour, then, is a trigger for action, not a measurement of the oxygen deficit. [2]
The decisive bedside act is to tell central cyanosis from peripheral acrocyanosis. Central cyanosis means the tongue, lips and mucous membranes are blue, signalling arterial desaturation — this is pathological and demands investigation. Peripheral (acro)cyanosis means the hands and feet are blue while the tongue stays pink; it is common and benign in the first 24 hours, caused by slow peripheral flow, and it resolves with warming. The trap is the infant whose tongue the clinician never checks, dismissing the baby as "just a bit cold". Always look at the tongue. [3]
The collapsed neonate is the severe end of the same spectrum — a baby in shock, with tachycardia or bradycardia, weak pulses, a capillary refill over three seconds, cold mottled peripheries, poor tone and a metabolic acidosis. In a term infant, collapse in the first days to weeks is most often a duct-dependent cardiac lesion whose systemic or pulmonary blood flow depended on a now-closing ductus arteriosus; the differential also holds sepsis, hypoxaemia from pulmonary disease, and metabolic collapse. Re-opening the ductus is life-saving, and it cannot wait for the echocardiogram. [2] [3]
Classification
The causes of neonatal cyanosis sort into five groups, and this five-cause frame is the diagnostic backbone. Cardiac causes are the cyanotic and duct-dependent congenital heart lesions — d-transposition of the great arteries, pulmonary atresia, tricuspid atresia, severe tetralogy of Fallot, hypoplastic left heart syndrome, obstructed total anomalous pulmonary venous return, and the obstructive left-sided lesions (coarctation, interrupted arch, critical aortic stenosis). Pulmonary causes are persistent pulmonary hypertension of the newborn (PPHN), respiratory distress syndrome, transient tachypnoea of the newborn, meconium aspiration syndrome, neonatal pneumonia, air-leak (pneumothorax), and congenital diaphragmatic hernia. Central nervous system causes are apnoea of prematurity, seizure, and neuromuscular weakness. Sepsis — chiefly early-onset group B streptococcus and E. coli — is both a direct cause of cyanosis and a cause of collapse. The metabolic and other causes are methaemoglobinaemia, haemoglobin-M disease, and polycythaemia. [2] [3]
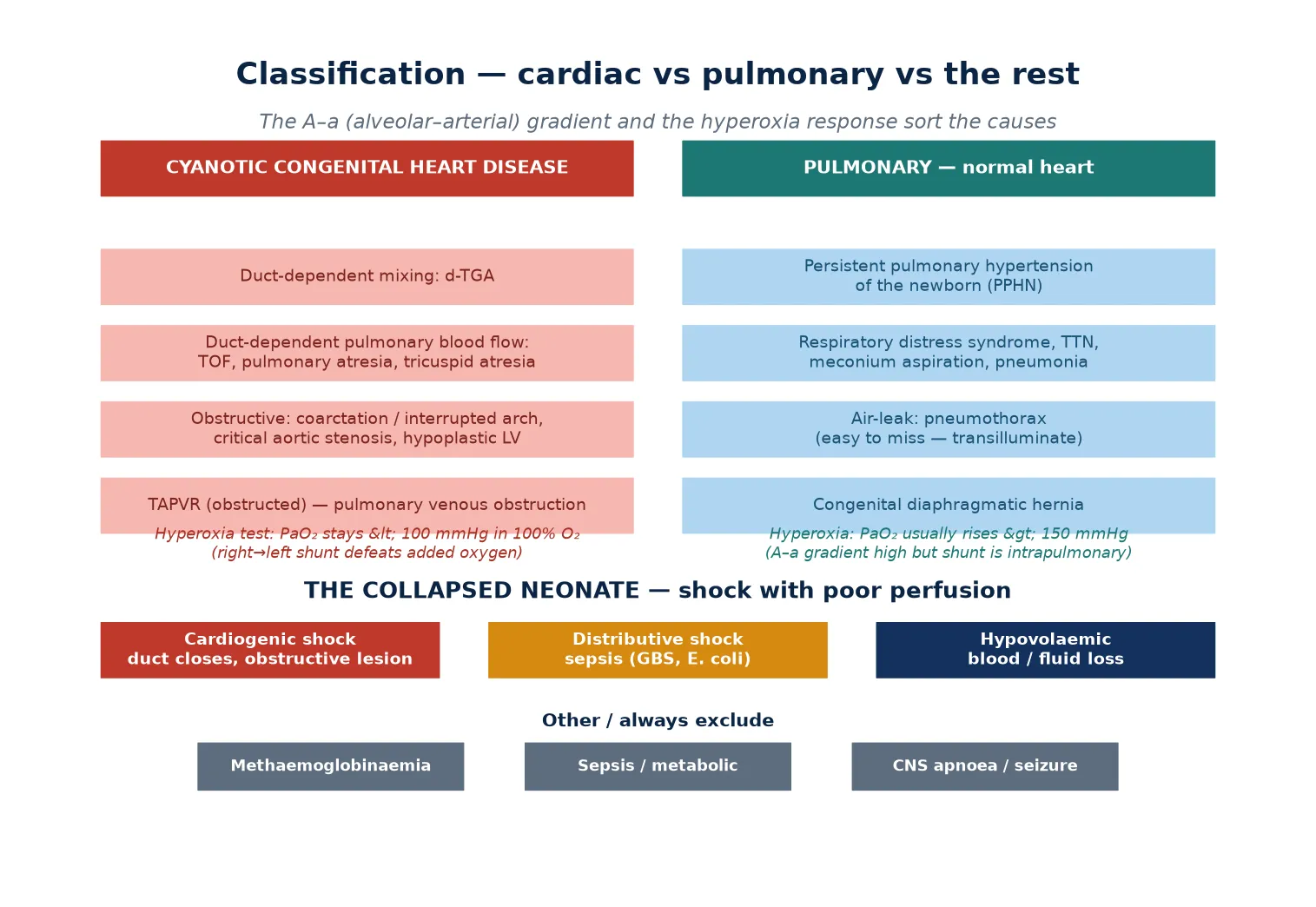
Two operational axes sharpen this frame. The first is the alveolar–arterial oxygen gradient and the hyperoxia response: a cardiac right-to-left shunt keeps PaO2 low even in 100% oxygen, whereas a pure pulmonary cause usually lets PaO2 rise. The second is the shock axis, which separates the cyanotic-but-stable infant from the collapsed one. Cardiogenic shock comes from an obstructive duct-dependent lesion or a failing myocardium; distributive shock comes from sepsis; hypovolaemic shock comes from acute blood or fluid loss. These axes are not mutually exclusive — a septic infant is cyanotic and collapsed — but naming both tells the team where to act first. [3] [8]
Epidemiology & Risk Factors
Critical congenital heart disease — the lesions likely to cause death or disability in the first year if undetected — occurs in roughly 1.5 to 2 per 1000 live births, and about half of these are duct-dependent. The signature problem is detection: these lesions are often invisible antenatally and may produce a normal newborn examination, so they declare themselves by collapse as the ductus closes, typically between day 2 and day 7 of life but sometimes later in the first weeks. Early hospital discharge shortens that window, and lower gestational age and failed antenatal detection both raise the chance of late, unexpected presentation. [2] [4]
Newborn pulse-oximetry screening was developed precisely to close this gap. The landmark Swedish prospective study of 39,821 newborns showed that adding pulse oximetry to routine examination detected the duct-dependent lesions that examination missed and reduced the proportion leaving hospital undiagnosed, with a mortality signal in its favour. Screening detects roughly three-quarters of critical congenital heart disease — it is a net cast widely, not a guarantee — so a sick infant is investigated regardless of a passed screen. [4] [5]
The non-cardiac causes carry their own risk profile. Prematurity and surfactant deficiency drive respiratory distress syndrome; meconium-stained liquor raises the risk of meconium aspiration; maternal group B streptococcal colonisation, prolonged rupture of membranes and maternal intrapartum fever raise the risk of early-onset sepsis; and perinatal asphyxia predisposes to PPHN and hypoxic–ischaemic encephalopathy. Methaemoglobinaemia is uncommon but worth remembering as an oxygen-refractory cause: it may be congenital (cytochrome b5 reductase deficiency, haemoglobin-M disease) or acquired from oxidant exposure. [8] [10]
Pathophysiology
To understand why a duct-dependent lesion collapses, follow the blood through the fetal-to-neonatal transition. In utero, the lungs are a high-resistance circuit and the ductus arteriosus shunts the majority of right ventricular output away from them, returning it to the placenta — the single oxygenating organ. A lesion whose systemic flow (hypoplastic left heart, coarctation) or pulmonary flow (pulmonary atresia, severe tetralogy) depends on that ductus is therefore hidden in utero, because the placenta and the duct together do the work the lesion cannot. [2]
At birth two things happen: the placenta is removed, and the ductus begins to close under prostaglandin withdrawal and rising oxygen tension. For most infants this is the intended transition to independent lung oxygenation. For the duct-dependent infant it is the removal of the only viable route for blood. As the duct constricts, systemic or pulmonary flow falls abruptly, the infant becomes profoundly hypoxaemic and acidotic, and shock follows. This is why the collapse is so often sudden and on day 2 to 7 — the ductus has a characteristic closing timetable, and the latent lesion reveals itself when it narrows. [2] [3]
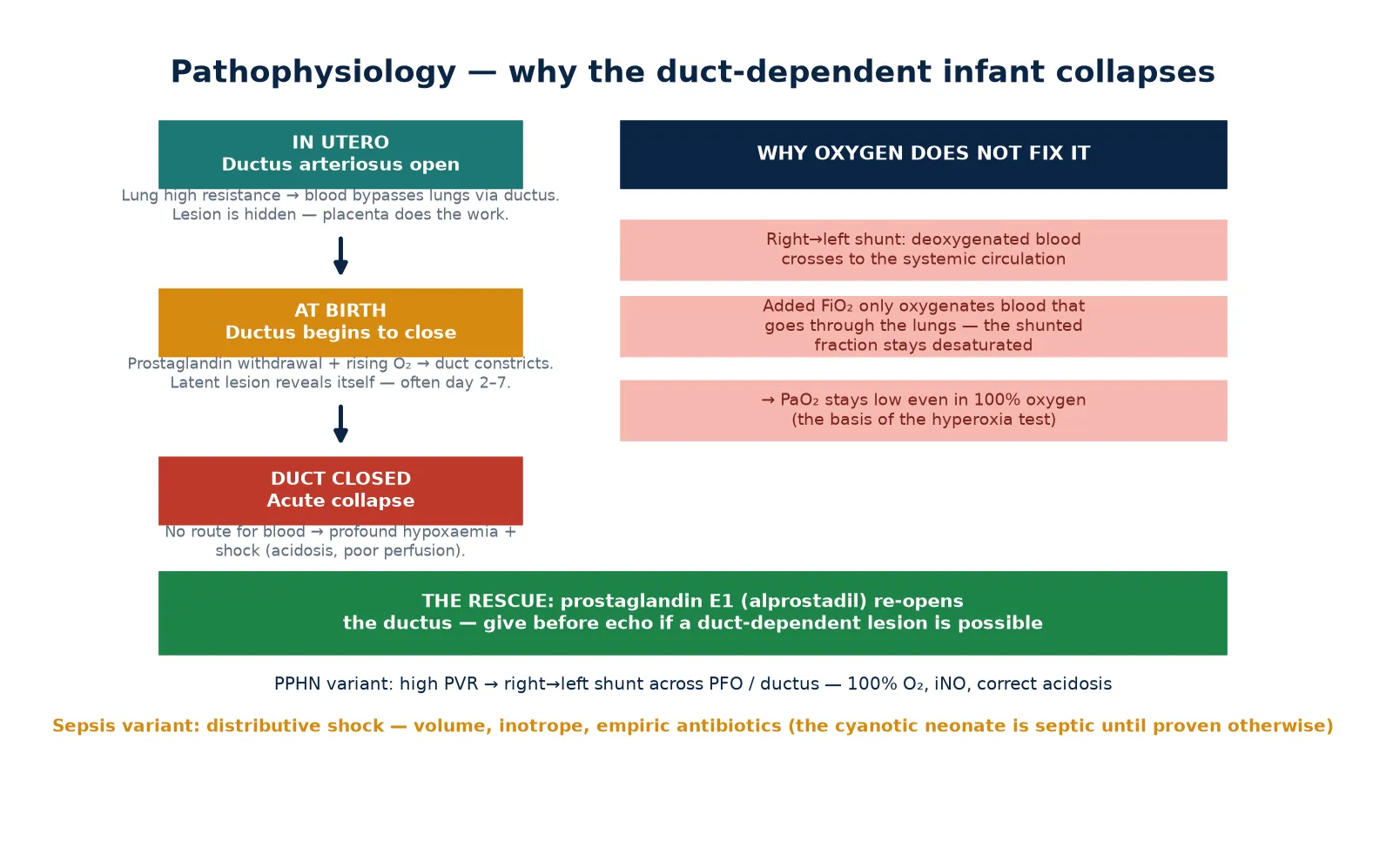
This is also why oxygen cannot rescue a cyanotic cardiac lesion. In a right-to-left shunt, a portion of the deoxygenated venous return crosses to the systemic side without ever passing through the lungs. Raising the inspired oxygen only oxygenates the blood that does perfuse the lung; the shunted fraction stays desaturated, so the arterial PaO2 stays low no matter how much oxygen is given. That failure of PaO2 to rise in 100% oxygen is precisely the hyperoxia test — the bedside demonstration of a fixed right-to-left shunt. [3]
PPHN is the pulmonary mirror of this problem. In PPHN the pulmonary vascular resistance fails to fall at birth, so right-heart pressure stays high and desaturated blood shunts right-to-left across the foramen ovale and the ductus. The result is severe hypoxaemia that can mimic cyanotic heart disease, and the two are often indistinguishable without echocardiography — which is why a structurally normal heart on echo is the confirmation of PPHN. Methaemoglobinaemia, by contrast, defeats oxygen by a different mechanism: the iron in haemoglobin is locked in the ferric state and cannot bind oxygen, so the blood carries less oxygen regardless of alveolar concentration, and the pulse oximeter reads falsely high (around 85%) because it misreads methaemoglobin. [2] [10]
Clinical Presentation
The cyanotic neonate is recognised first by colour and then by effort. Central cyanosis shows as a slate-blue tongue and lips, duskiness of the face, and — often — a discrepancy between the severity of the colour and the amount of respiratory effort. A baby who is deeply blue but breathing comfortably, with little recession or grunting, is the classic cardiac presentation: the heart, not the lungs, is the problem. A baby who is blue and working hard — tachypnoeic, grunting, with intercostal and subcostal recession and nasal flaring — points to a pulmonary cause. The effort–colour mismatch is a high-yield bedside observation. [3]
The collapsed neonate shows shock on top of cyanosis. Look for tachycardia (or bradycardia as a pre-arrest sign), weak or absent peripheral and femoral pulses, a capillary refill over three seconds, cold and mottled peripheries, poor tone and lethargy, and a rising or falling temperature. The blood gas shows a metabolic acidosis. The lesson is that cyanosis and collapse can coexist (the duct-dependent infant who has gone beyond simple cyanosis into shock) and that collapse without cyanosis still demands the same cardiac-and-sepsis work-up. [3] [8]
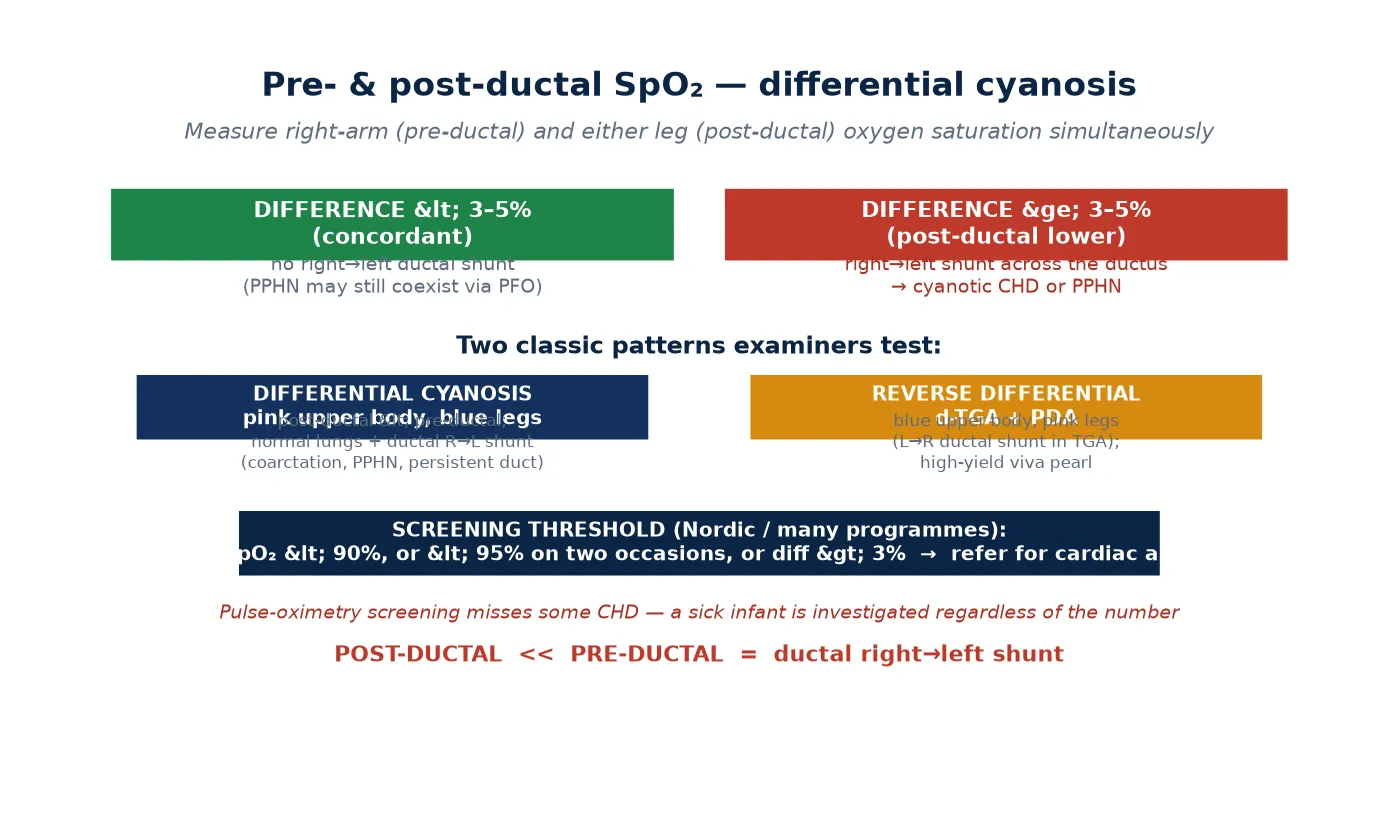
Specific features reweight the differential toward a cardiac cause. Differential cyanosis — a pink upper body with blue legs — signals a right-to-left ductal shunt (coarctation, interrupted arch, PPHN with ductal shunting). Weak or absent femoral pulses, or a blood-pressure gradient between the upper and lower limbs, point to coarctation or interrupted arch. A single or loud second heart sound, a heart murmur (frequently absent in the most critical lesions), hepatomegaly, and a chest X-ray showing pulmonary oligaemia or abnormal cardiac silhouette all push toward the heart. The absent murmur is itself a trap: the most dangerous lesions are often the quietest. [2] [3]
Differential Diagnosis
The differential is built in one move at the bedside and refined by three tests. The move is to assign the cause to one of the five groups using the effort–colour relationship, the pulses, and the presence or absence of shock. The three tests that refine it are the pre- and post-ductal saturation difference, the chest X-ray, and the hyperoxia response. Together they answer the pivotal question: is the heart the problem? [3]
For the cardiac group, the discriminating anatomy matters because it predicts the presentation. Lesions that depend on the duct for mixing (d-TGA) present with profound cyanosis and little distress. Lesions that depend on the duct for pulmonary blood flow (pulmonary atresia, severe tetralogy, tricuspid atresia) present with cyanosis and pulmonary oligaemia on X-ray. Lesions that depend on the duct for systemic flow (hypoplastic left heart, coarctation, interrupted arch, critical aortic stenosis) present as shock with weak pulses and acidosis as the duct closes. Obstructed total anomalous pulmonary venous return presents with cyanosis and pulmonary venous congestion. [2] [3]
The must-not-miss diagnoses are the ones whose delay harms the infant. A duct-dependent cardiac lesion must have the duct re-opened with prostaglandin before the echo. A tension pneumothorax must be decompressed immediately. Sepsis must be covered empirically. And methaemoglobinaemia — uncommon but classic — must be suspected when cyanosis is unresponsive to oxygen and the pulse oximeter reads around 85% without climbing; a methaemoglobin level confirms it. The PPHN mimic is the most common source of diagnostic doubt: severe hypoxaemia with a structurally normal heart, resolved by echocardiography. [3] [10]
Clinical & Bedside Assessment
Bedside assessment runs in two layers — an immediate stabilisation and a focused, structured examination. Stabilisation comes first and runs in parallel with assessment: secure the airway, give bag-mask ventilation if the effort is inadequate, apply oxygen, check the glucose and temperature, and establish intravenous access. Do not let examination delay resuscitation. [1] [3]
The focused examination is built to answer "is the heart the problem?" Assess the work of breathing first — recessions, grunting, nasal flaring — and compare it with the severity of cyanosis (the effort–colour mismatch). Check the colour centrally (tongue) and peripherally, and look for differential cyanosis. Feel the brachial and femoral pulses together and measure four-limb blood pressure, looking for a gradient. Examine the precordium for heaves, listen for heart sounds (a single or loud second sound is significant) and murmurs, assess the capillary refill and perfusion, palpate the liver, assess tone and alertness, and transilluminate the chest for a pneumothorax. Each finding moves the probability toward a group. [3]
The focused history reweights the differential in minutes. Ask about the antenatal scans and the newborn pulse-oximetry screen result (a passed screen lowers but does not exclude the probability of critical CHD); about gestation, birth weight and birth events; about meconium-stained liquor; about maternal group B streptococcus status, prolonged rupture of membranes and intrapartum fever (sepsis risk); about a family history of congenital heart disease; and about the day and tempo of onset — sudden collapse on day 2 to 7 is the duct-dependent signature. [2] [8]
Investigations
The first-hour bundle is fixed and runs in parallel with resuscitation. Take simultaneous pre- and post-ductal pulse oximetry; an arterial or capillary blood gas with glucose and lactate; a full blood count and CRP; and blood cultures before antibiotics. Send a chest X-ray early — it shows pulmonary oligaemia or plethora, the cardiac silhouette and size, lung disease, a pneumothorax, or a congenital diaphragmatic hernia. Measure four-limb blood pressure for a gradient. The electrocardiogram is secondary but adds myocardial and rhythm information. [3] [8]
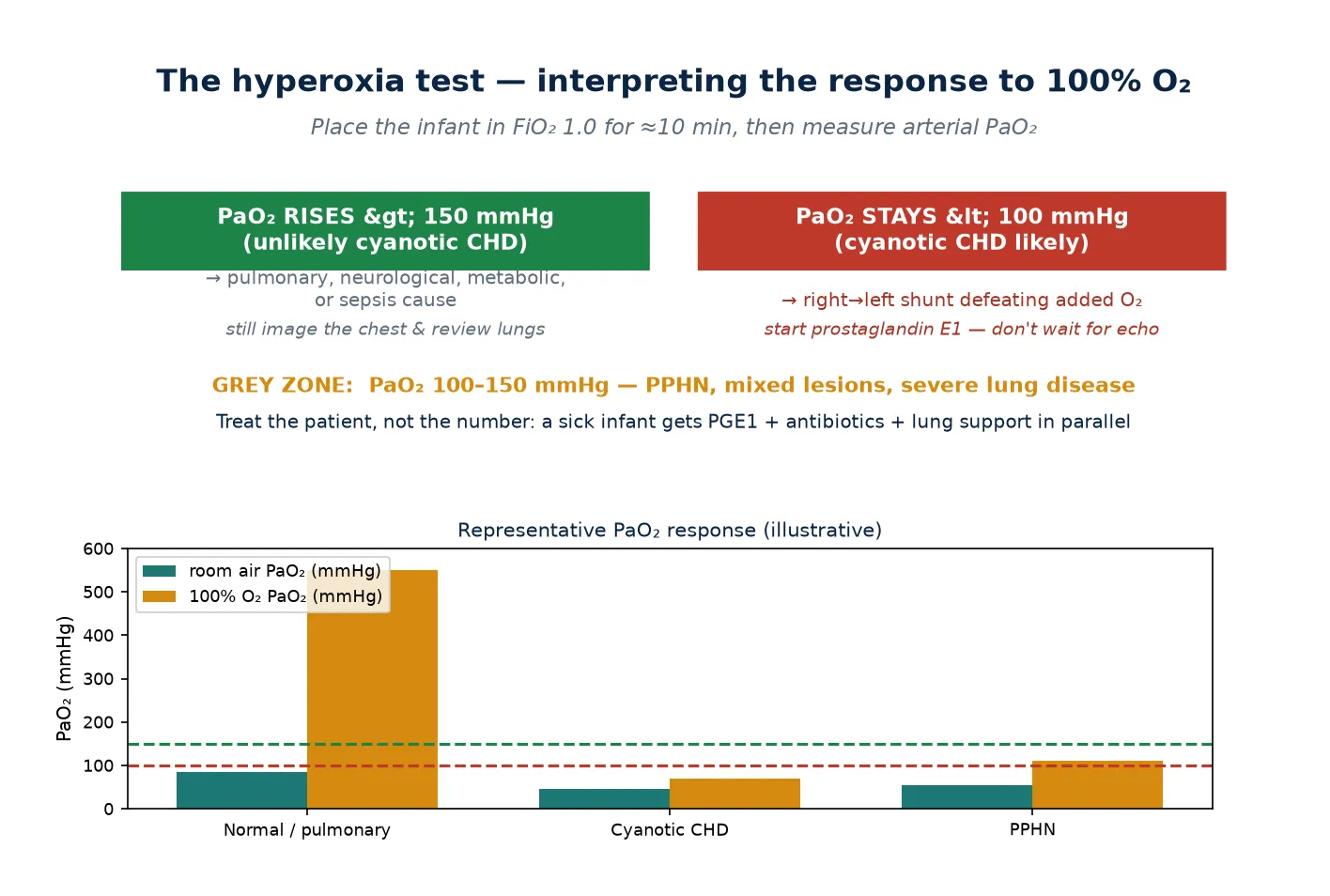
The hyperoxia test is the bedside discriminator between a fixed cardiac shunt and a pulmonary cause. Place the infant in 100% oxygen for about ten minutes and measure the arterial PaO2. A PaO2 that rises above 150 mmHg argues strongly against cyanotic heart disease and points to a pulmonary, neurological, metabolic or septic cause. A PaO2 that stays below 100 mmHg supports a right-to-left shunt and cyanotic heart disease. The 100–150 mmHg grey zone includes PPHN, mixed lesions and severe lung disease — treat the patient, not the number. [3]
The definitive cardiac investigation is urgent echocardiography, which defines the anatomy and confirms or refutes a duct-dependent lesion and PPHN — but prostaglandin therapy must not wait for it. For the sepsis work-up, the neonatal early-onset sepsis risk calculator quantifies the risk from maternal risk factors and the infant's clinical state and helps guide the decision to treat or observe, though a sick infant receives empiric antibiotics regardless. For the metabolic and haematological causes, send a methaemoglobin level (methaemoglobinaemia), a venous haematocrit (polycythaemia), and a haemoglobinopathy screen when haemoglobin-M disease is suspected. [3] [9]
Management — Resuscitation
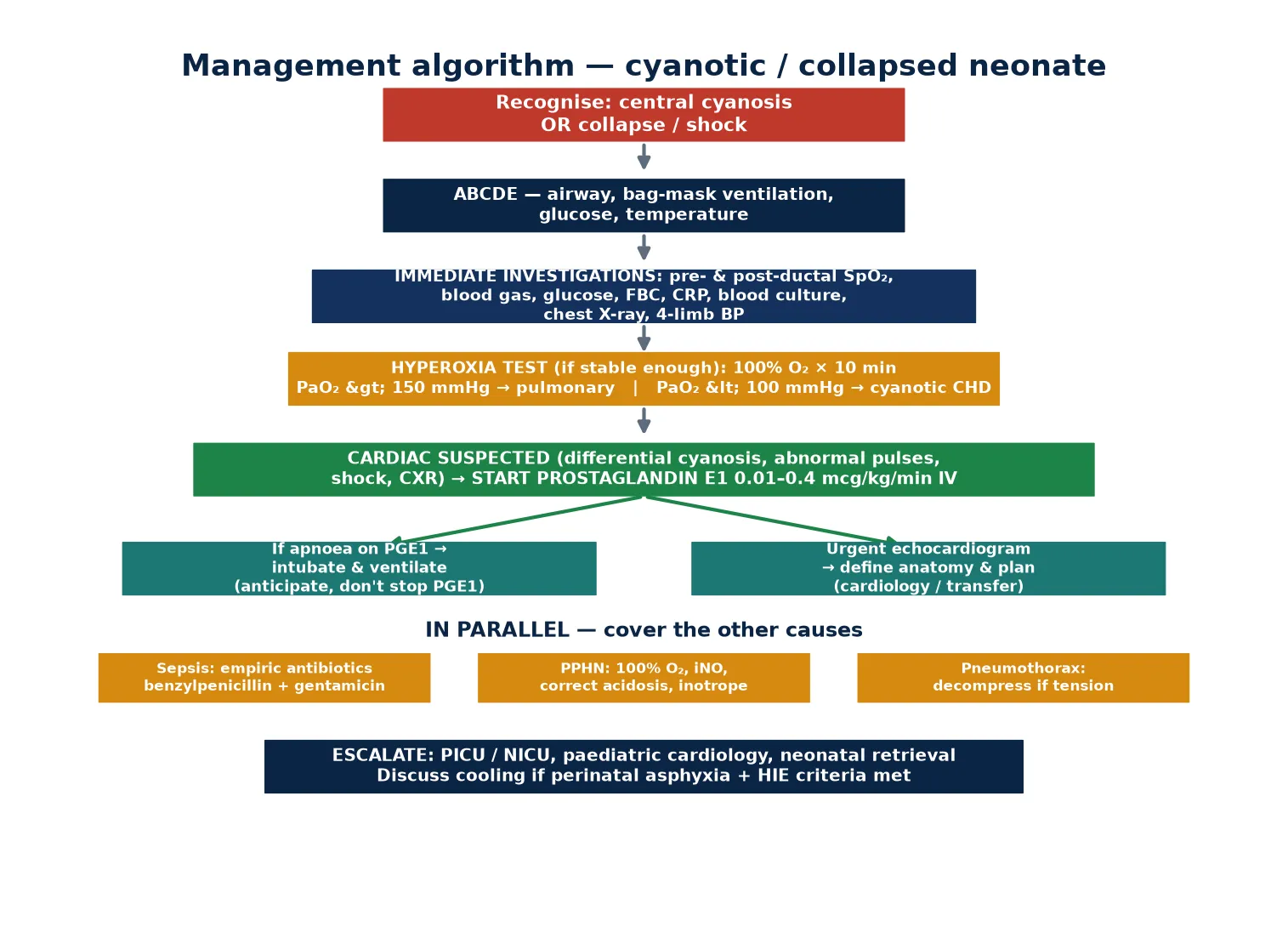
Resuscitation follows ABCDE with three neonatal-specific priorities: support ventilation in the cyanotic or apnoeic infant, re-open the ductus if a duct-dependent lesion is possible, and cover sepsis. Begin with the airway and bag-mask ventilation for apnoea or inadequate effort, applying oxygen to reach target saturations and then weaning to avoid hyperoxia. Check and correct the glucose and temperature — hypothermia and hypoglycaemia worsen pulmonary vasoconstriction and acidosis — and establish intravenous access. [1] [3]
The time-critical drug is prostaglandin E1 (alprostadil). The principle is absolute: if a duct-dependent lesion is possible, start it before the echocardiogram, because re-opening the ductus is life-saving and the risk of an unnecessary infusion is far lower than the risk of a closed duct. Cover sepsis at the same time — the cyanotic neonate is septic until proven otherwise — with blood cultures followed by empiric benzylpenicillin plus an aminoglycoside such as gentamicin, adjusted to local antimicrobial guidance and weight. [3] [8]
Correct the reversible drivers of deterioration in parallel. Decompress a tension pneumothorax immediately (needle decompression, then an intercostal drain). Correct hypoglycaemia, acidosis and hypothermia, each of which increases pulmonary vascular resistance and worsens the right-to-left shunt of PPHN. If perinatal asphyxia is in the history and the infant meets the criteria for hypoxic–ischaemic encephalopathy, initiate therapeutic hypothermia within the therapeutic window. [1] [8]
Immediate management of the cyanotic or collapsed neonate
Assess ABCDE; airway, bag-mask ventilation for apnoea or inadequate effort; oxygen to target saturations
Check and correct glucose and temperature; establish IV access
Simultaneous pre-/post-ductal SpO2; blood gas with glucose/lactate; FBC, CRP, blood cultures; chest X-ray; four-limb BP
If a duct-dependent lesion is possible — start prostaglandin E1 before the echo
Give empiric antibiotics (benzylpenicillin + aminoglycoside) after cultures
Perform the hyperoxia test if the infant is stable enough
Obtain urgent echocardiography; refer to cardiology / NICU / PICU / retrieval
Escalate: intubate if PGE1 causes apnoea or CO2 rises; discuss cooling if HIE criteria met
Management — Definitive & Stepwise
Definitive management is layered: stabilise the infant, re-open the ductus, define the anatomy, and start cause-specific therapy. Prostaglandin E1 (alprostadil) is infused intravenously, starting low at 0.01–0.05 mcg/kg/min and titrating up to 0.1–0.4 mcg/kg/min to reopen and keep the ductus patent; the dose is held at the lowest that maintains adequate oxygenation and perfusion to minimise side-effects. The drug works by relaxing ductal smooth muscle and restoring the fetal flow route that the lesion depends on. [3] [6]
Prostaglandin E1 (alprostadil)
Dose
Start 0.01–0.05 mcg/kg/min IV continuous; titrate up to 0.1–0.4 mcg/kg/min to the lowest effective dose
The two side-effects that change practice are apnoea and the gastrointestinal effects. Apnoea occurs with prostaglandin therapy and is anticipated, not feared — if it occurs, intubate and ventilate, but do not stop the infusion, because stopping sacrifices the ductal rescue. Evidence supports transporting newborns with suspected duct-dependent disease on low-dose prostaglandin without routine mechanical ventilation where the infant maintains adequate oxygenation and ventilation, reserving intubation for those who develop apnoea or fail to maintain their gas exchange. The cumulative dose matters too: gastrointestinal adverse effects, including gastric-outlet obstruction and necrotising-enterocolitis-like changes, rise with the total prostaglandin dose over time, so the infusion is held at the minimum effective dose and surgery or catheter intervention is expedited. [6] [7]
For the non-cardiac causes, definitive therapy runs in parallel. PPHN is managed with oxygen, correction of acidosis, inhaled nitric oxide, inotropes, and extracorporeal membrane oxygenation if refractory. The pulmonary causes receive their specific therapy — surfactant and lung-protective ventilation for respiratory distress syndrome, decompression for pneumothorax, and surgical management for congenital diaphragmatic hernia. Symptomatic methaemoglobinaemia is treated with methylene blue (1–2 mg/kg IV), with specialist input and caution in glucose-6-phosphate dehydrogenase deficiency. Sepsis is treated with targeted antibiotics and haemodynamic support per the neonatal septic-shock parameters — early vascular access, fluid boluses titrated to perfusion, and inotropes for fluid-refractory shock. [8] [10]
Definitive pathway after prostaglandin
Specific Subtypes & Scenarios
The duct-dependent cyanotic lesion — for example d-transposition of the great arteries or pulmonary atresia — presents on day 2 to 7 with profound cyanosis and often surprisingly little respiratory distress, as the duct narrows and mixing or pulmonary flow falls. The infant is blue but not initially shocked; the hyperoxia test shows a PaO2 stuck below 100 mmHg, and prostaglandin produces a gratifying rise in saturation as the duct reopens. The urgent echocardiogram defines the anatomy, and a balloon atrial septostomy may be needed for d-TGA with a restrictive atrial communication. [2] [3]
The obstructive duct-dependent lesion — coarctation of the aorta, interrupted arch, hypoplastic left heart syndrome, critical aortic stenosis — presents as shock rather than isolated cyanosis, with weak or absent femoral pulses, a blood-pressure gradient between the upper and lower limbs, hepatomegaly and a metabolic acidosis, as systemic flow collapses with the duct. This is the cohort in which the diagnosis is missed as "sepsis" or "metabolic acidosis" and the infant arrests before the heart is considered. Start prostaglandin on suspicion of shock-with-weak-pulses and confirm with echo. [3]
PPHN presents with severe hypoxaemia, often with differential cyanosis and a loud or single second heart sound, in a term or late-preterm infant — frequently after a perinatal stress such as asphyxia, meconium aspiration or sepsis. The chest X-ray may be clear, and the hyperoxia test sits in the grey zone. Echocardiography confirms structurally normal heart with elevated pulmonary pressures and right-to-left shunting. The management — oxygen, correction of acidosis, inhaled nitric oxide, and inotropes — is detailed in the dedicated PPHN leaf, but the recognition point here is that PPHN is the most common mimic of cyanotic heart disease and the two are separated by the echo. [2]
The septic collapsed neonate — classically early-onset group B streptococcus or E. coli — presents with cyanosis, temperature instability, lethargy and shock, often with maternal risk factors. The metabolic and other causes round out the frame: methaemoglobinaemia (congenital cytochrome b5 reductase deficiency, haemoglobin-M disease, or acquired oxidant exposure) produces cyanosis unresponsive to oxygen with a pulse oximeter stuck around 85%; polycythaemia exaggerates cyanosis; and haemoglobin-M disease is the rare haemoglobinopathy to name when cyanosis is lifelong and oxygen-refractory. [8] [10]
Complications & Pitfalls
The complications of prostaglandin therapy define its safe use. Apnoea is the commonest and the most operationally important — anticipate it, have a low threshold to intubate, and never stop the infusion for it. Hypotension, fever and irritability are also frequent. The gastrointestinal effects — gastric-outlet obstruction and necrotising-enterocolitis-like changes — rise with the cumulative dose, which is why the infusion is held at the lowest effective dose and definitive repair is expedited. [6] [7]
The diagnostic pitfalls are the ones examiners press. Dismissing central cyanosis as benign acrocyanosis because the tongue was never checked. Waiting for an echo before starting prostaglandin, during which the duct closes further. Failing to recognise differential or reverse-differential cyanosis, which carry specific anatomical implications. Over-relying on pulse oximetry in methaemoglobinaemia, where the reading is falsely high and stuck around 85%. And forgetting that the most critical lesions are often the quietest — a normal murmur does not exclude critical CHD. [3] [10]
The resuscitation pitfalls compound the diagnostic ones. Giving unmonitored 100% oxygen without watching for hyperoxia, which carries its own risks. Missing a tension pneumothorax that a transillumination would have caught. Forgetting sepsis cover while chasing the heart. And delaying therapeutic hypothermia in the asphyxiated infant who also meets the criteria for hypoxic–ischaemic encephalopathy — cooling has a time window, and the cyanotic collapse may be the presentation of HIE. [1]
Prognosis & Disposition
The prognosis of duct-dependent congenital heart disease is set by two things — the specific lesion and the timeliness of ductal rescue. Late collapse from a closed duct carries significant mortality and morbidity from hypoxaemia, acidosis and end-organ injury, and the neurological outcome is poorer when resuscitation is delayed. This is the clinical justification for pulse-oximetry screening and for the rule of starting prostaglandin on suspicion: early detection and early prostaglandin rescue convert a potentially fatal collapse into a stabilised infant awaiting elective repair. [2] [4]
Newborn pulse-oximetry screening reduces late detection of critical congenital heart disease and carries a mortality signal in its favour, which is why it is embedded in routine newborn care across many programmes. The septic and asphyxial causes carry prognosis set by the insult and the speed of resuscitation — early antibiotics and haemodynamic support in septic shock, and timely therapeutic hypothermia in HIE, are the modifiable determinants. [4] [8]
Disposition follows the diagnosis. A confirmed or suspected duct-dependent lesion goes to a tertiary or cardiac neonatal/paediatric intensive care unit with urgent echocardiography and cardiology, continuing prostaglandin until definitive surgery or catheter intervention, and coordinated retrieval — intubating before transfer if prostaglandin has caused apnoea. The safety-net is a clear written plan with escalation triggers, structured reassessment, and honest family communication about the suspected diagnosis, the need for transfer, and the next steps. [6]
Special Populations
The late-preterm and term infant straddles the pulmonary and cardiac worlds — prematurity-related lung disease (respiratory distress syndrome, apnoea of prematurity) coexists with the same duct-dependent and PPHN presentations as in the term infant, and the smaller the baby, the easier it is to attribute cyanosis to "immature lungs" and miss a cardiac cause. Investigate the cyanotic late-preterm infant with the same five-cause frame. [2] [3]
The infant who passed newborn pulse-oximetry screening yet still collapses deserves a special mention, because the false reassurance is the danger. Screening detects roughly three-quarters of critical congenital heart disease, which means a meaningful minority are missed, and a passed screen does not exclude critical CHD in a sick infant. Investigate on the clinical presentation, not the screening result. [4] [5]
The rural or remote neonate and the retrieval implications are an exam favourite. Transporting a cyanotic or collapsed infant on prostaglandin is the practical challenge: evidence supports low-dose prostaglandin without routine mechanical ventilation where the infant maintains adequate oxygenation and ventilation, with selective intubation for apnoea or ventilation failure, so that the retrieval does not automatically mean an intubated, ventilated transfer. The retrieval team needs the prostaglandin running, monitoring in place, and a clear handover plan to the receiving cardiac centre. [6]
The anaemic and polycythaemic infants sit at opposite ends of the cyanosis detection problem. The anaemic infant may be severely hypoxaemic and never turn blue, because there is insufficient haemoglobin to generate the deoxyhaemoglobin threshold — cyanosis is a late or absent sign, and the diagnosis rests on the blood gas. The polycythaemic infant looks blue at milder desaturation, because a higher total haemoglobin reaches the deoxyhaemoglobin threshold sooner. In both, treat the gas and the perfusion, not the colour. [2] [3]
Evidence, Guidelines & Regional Differences
The evidence base for this presentation is anchored in neonatal resuscitation, cardiovascular physiology, screening and prostaglandin practice. The 2020 International Consensus on Neonatal Life Support sets the oxygen and ventilation approach for the newborn — when to start, what saturation to target, and when to escalate — and is the reference for the resuscitation steps in this topic. The perinatal cardiovascular physiology literature explains why duct-dependent lesions are hidden in utero and revealed at birth, and frames the recognition of critical CHD. [1] [2]
The screening evidence is the Swedish prospective study of 39,821 newborns (de-Wahl Granelli 2009), which showed that pulse oximetry added to routine examination detected the duct-dependent lesions that examination missed and reduced late discharge without diagnosis, with a mortality signal. The Nordic proposal that followed (de-Wahl Granelli 2014) set out uniform screening thresholds — any limb below 90%, or below 95% on two occasions, or a pre-/post-ductal difference over 3% — that many programmes have adopted, though exact thresholds and timing vary by region and by whether screening is paired with antenatal ultrasound. [4] [5]
In Australia and New Zealand, newborn pulse-oximetry screening is increasingly embedded in routine newborn care alongside antenatal ultrasound, with referral thresholds broadly aligned to the Nordic proposal. Empiric neonatal sepsis cover is typically benzylpenicillin plus gentamicin, adjusted to local antimicrobial stewardship and gestation-specific dosing. Retrieval of suspected duct-dependent infants on low-dose prostaglandin follows the transport model of selective intubation for apnoea or ventilation failure. [5] [6]
The prostaglandin transport and dose evidence is pragmatic and registry-based. The Browning Carmo study (2007) established that newborns with suspected duct-dependent disease can be transported on low-dose prostaglandin without routine mechanical ventilation, reserving intubation for those who need it. The Ofek Shlomai cohort (2023) showed that the cumulative prostaglandin dose determines the gastrointestinal adverse effects, lending weight to the principle of the lowest effective dose and expedited definitive repair. The sepsis evidence is represented by the ACCCM neonatal septic-shock parameters (Davis 2017) and the neonatal early-onset sepsis risk calculator (Kuzniewicz and Puopolo 2017), which together frame the parallel sepsis work-up that must never be omitted from the cyanotic-neonate pathway. [6] [7] [9]
Across regions, the disease is the same and the drugs are the same, but screening thresholds, oxygen-targeting in resuscitation, empiric antibiotic choices and retrieval infrastructure differ. Where access to cardiac surgery and retrieval is limited — in remote or resource-constrained settings — the penalty for late detection is greater, which is why the principle of starting prostaglandin on suspicion and covering sepsis empirically is the universal, transferable safety-net. [1] [8]
Current controversies include the optimal screening thresholds and timing; the balance between the neonatal early-onset sepsis calculator and empiric antibiotics (the calculator guides risk but a sick infant is treated regardless); oxygen-targeting in neonatal resuscitation to avoid both hypoxia and hyperoxia; and equity of access to cardiac surgery and retrieval for remote and disadvantaged infants. These are not academic points — they are the decisions that determine whether a duct-dependent infant is detected early or presents in avoidable collapse. [4] [9]
Exam Pearls
The one-sentence answer: a blue or collapsed newborn has central cyanosis or shock, and the first act is to confirm central cyanosis, recognise collapse as duct-dependent until proven, start prostaglandin E1 before the echo, and cover sepsis — using the hyperoxia test, the pre-/post-ductal difference and the chest X-ray to decide whether the heart is the problem. [3]
BLUE
The frequently-misremembered facts, correctly stated. Acrocyanosis is benign and central cyanosis is pathological — the difference is the tongue. Cyanosis is a late sign, and the anaemic infant may never turn blue. A passed pulse-oximetry screen does not exclude critical congenital heart disease in a sick infant. The most critical cardiac lesions are often the quietest — a normal murmur does not exclude critical CHD. And the hyperoxia test cut-points are 150 mmHg (rises = not cyanotic CHD) and 100 mmHg (stays low = cyanotic CHD), with a grey zone for PPHN and mixed disease. [3] [4]
The high-yield drugs and dosing, each with its source. Prostaglandin E1 (alprostadil) 0.01–0.05 mcg/kg/min IV starting, titrating to 0.1–0.4 mcg/kg/min to the lowest effective dose — with the anticipation that apnoea may require intubation but must not stop the infusion. Empiric neonatal sepsis cover with benzylpenicillin plus an aminoglycoside (gentamicin) after blood culture, adjusted to local protocol and weight. Methylene blue 1–2 mg/kg IV for symptomatic methaemoglobinaemia, with specialist input and caution in glucose-6-phosphate dehydrogenase deficiency. The screening thresholds — any limb below 90%, or below 95% on two occasions, or a pre-/post-ductal difference over 3% — trigger cardiac referral. [6] [8] [10]
References
- [1]Wyckoff MH; Wyllie J; Aziz K; de Almeida MF; et al Neonatal Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation, 2020.PMID 33084392
- [2]Singh Y; Lakshminrusimha S Perinatal Cardiovascular Physiology and Recognition of Critical Congenital Heart Defects. Clin Perinatol, 2021.PMID 34353581
- [3]Strobel AM; Lu le N The Critically Ill Infant with Congenital Heart Disease. Emerg Med Clin North Am, 2015.PMID 26226862
- [4]de-Wahl Granelli A; Wennergren M; Sandberg K; Mellander M; et al Impact of pulse oximetry screening on the detection of duct dependent congenital heart disease: a Swedish prospective screening study in 39,821 newborns. BMJ, 2009.PMID 19131383
- [5]de-Wahl Granelli A; Meberg A; Ojala T; Steensberg J; et al Nordic pulse oximetry screening--implementation status and proposal for uniform guidelines. Acta Paediatr, 2014.PMID 25060211
- [6]Browning Carmo KA; Barr P; West M; Nicholl M; et al Transporting newborn infants with suspected duct dependent congenital heart disease on low-dose prostaglandin E1 without routine mechanical ventilation. Arch Dis Child Fetal Neonatal Ed, 2007.PMID 16905574
- [7]Ofek Shlomai N; Lazarovitz G; Koplewitz B; Eisenkop M; et al Cumulative Dose of Prostaglandin E1 Determines Gastrointestinal Adverse Effects in Term and Near-Term Neonates Awaiting Cardiac Surgery: A Retrospective Cohort Study. Children (Basel), 2023.PMID 37761532
- [8]Davis AL; Carcillo JA; Aneja RK; Deymann AJ; et al American College of Critical Care Medicine Clinical Practice Parameters for Hemodynamic Support of Pediatric and Neonatal Septic Shock. Crit Care Med, 2017.PMID 28509730
- [9]Kuzniewicz MW; Puopolo KM; Fischer A; Walsh EM; et al A Quantitative, Risk-Based Approach to the Management of Neonatal Early-Onset Sepsis. JAMA Pediatr, 2017.PMID 28241253
- [10]Lyle ANJ; Spurr R; Kirkey D; Maglinte D; et al Case report of congenital methemoglobinemia: an uncommon cause of neonatal cyanosis. Matern Health Neonatol Perinatol, 2022.PMID 36114590