Paeds · fetal-neonatal-and-perinatal
Neonatal fluid, electrolyte and nutritional management
Also known as Neonatal fluid and electrolyte management · Neonatal parenteral and enteral nutrition · Neonatal hydration and nutrition · Preterm fluid and nutrition prescription · Neonatal water, electrolyte and substrate balance
Fellowship guide to neonatal fluid, electrolyte and nutritional management: why the neonate is 75% water with an immature kidney and a brain building itself from substrate, the daily fluid ladder by postnatal age, sodium/potassium/calcium/phosphate balance and their derangements, the glucose infusion rate, the parenteral-to-enteral nutrition sequence, and the goal of replicating in-utero growth without overload or catabolism.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a 28-week, 1000-gram infant on day three of life. The neonatal registrar writes a fluid order, an electrolyte panel and a feeding plan — and these are not three independent decisions but one prescription seen from three angles. The volume of water carries the electrolytes, and the electrolytes carry the nutrition substrate. Get one wrong and the others fail with it. [4]
Neonatal fluid, electrolyte and nutritional management is best defined as the daily prescription of water, ions and substrate calibrated to the infant's gestation, postnatal age and growth trajectory, with the explicit goal of replicating in-utero growth without imposing fluid overload or catabolism. [1] [2] That phrasing is deliberate and examiner-friendly: it names the objective (growth), the constraint (immature physiology), and the unit of thinking (the day, reviewed every round). The neonate is not a small adult — total body water is far higher, the kidney cannot concentrate or dilute, insensible losses are large, and the metabolic demand per kilogram dwarfs anything in later life.
The reason these prescriptions exist at all is the postnatal transition. In fetal life the placenta manages water and electrolytes and supplies substrate continuously; at birth that management passes to an immature kidney and to intermittent feeding, while the infant must simultaneously contract its extracellular fluid compartment (the "diuresis" and weight drop) and grow. Most neonatal fluid and nutrition problems are a failure to respect that transition — either overloading the contracting compartment or under-feeding the growing one. [4] [10]
So the examiner's first question is always: what is this infant supposed to do today — lose water, hold water, or grow? That single framing drives the entire daily prescription. [2]
Classification
Begin with the domain, then the postnatal day, then the gestation. [2]
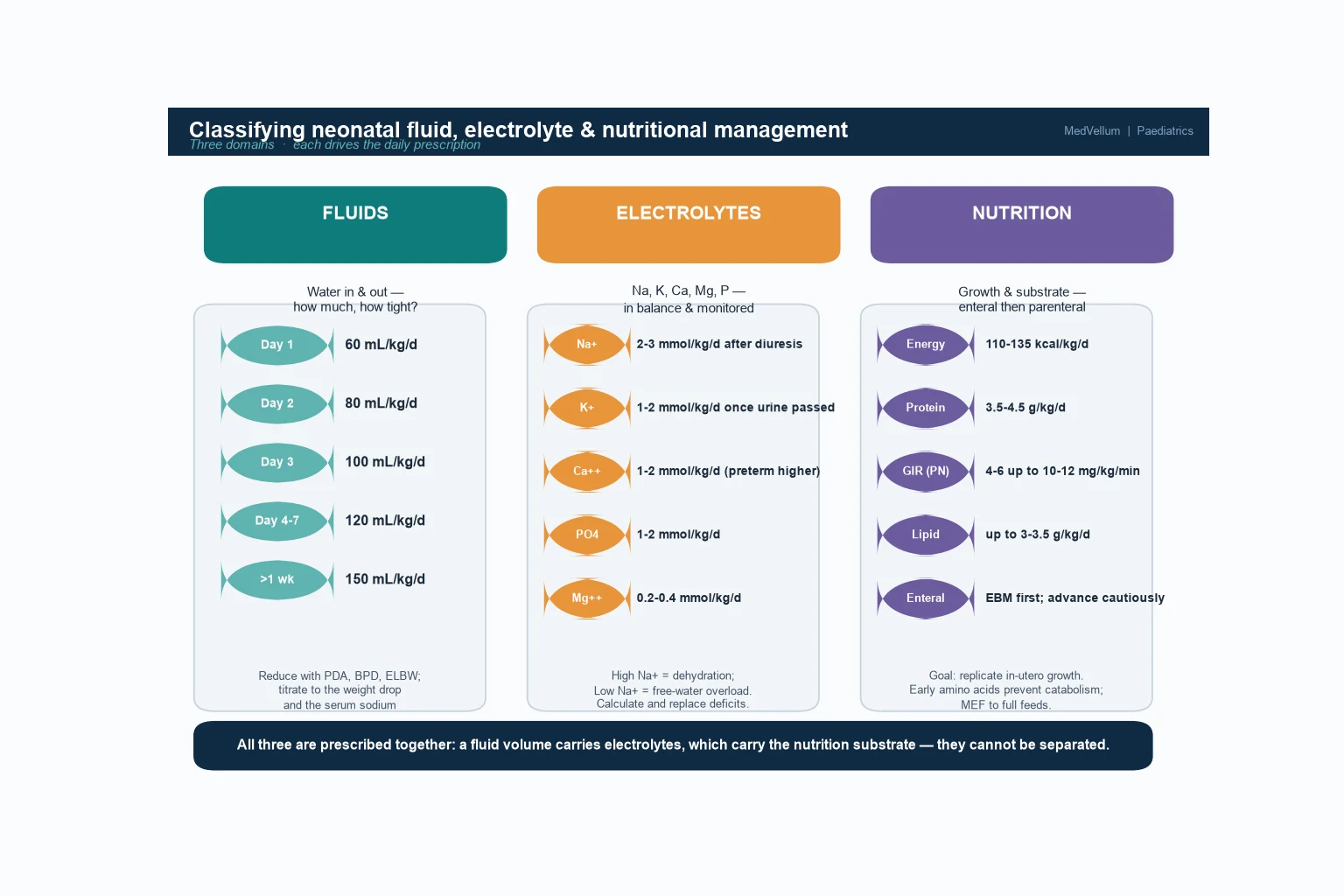
By domain, separate fluids, electrolytes and nutrition — but keep them in one mind. Fluids concern total water in and out and how tightly it is held: the daily mL/kg ladder, insensible loss, urine output, and the allowance for the physiological postnatal weight drop. Electrolytes concern sodium, potassium, calcium, phosphate, magnesium and acid–base balance, each with a daily target and a serum value to chase. Nutrition concerns the substrate for growth — energy, protein, glucose, lipid, vitamins and minerals — given parenterally then enterally, with growth on a Fenton chart as the judge. [1] [2]
By postnatal day, the prescription changes character. In the first 1–3 days the infant is contracting its extracellular fluid — you expect a weight loss of 5–10% (up to 15% in the very preterm), so the fluid allowance is tight (60, 80, 100 mL/kg/day) and sodium is withheld until diuresis begins. From day 3–7 the infant transitions to a growth phase — fluid rises toward 150 mL/kg/day, electrolytes are added and nutrition advances. Beyond a week the infant is growing — full enteral feeds, fortification for the preterm, and the goal of 10–15 g/kg/day weight gain. [10]
By gestation and status, the targets shift. The extremely preterm (under 28 weeks) and very-low-birth-weight infant has the largest body water, the highest insensible loss and the most immature kidney, so fluid is titrated tightly and parenteral nutrition started on day 0. The term infant is more forgiving but still vulnerable to hypernatraemic dehydration from poor lactation and to fluid overload if given excessive maintenance. The critically ill or surgical infant (NEC, gastroschisis) demands a nutrition-first, fluid-restricted parenteral strategy. [9]
Epidemiology & Risk Factors
Disorders of neonatal fluid, electrolyte and nutritional balance are among the commonest problems in any neonatal unit. The risk is concentrated in the preterm and low-birth-weight population — over 90% of extremely preterm infants receive parenteral nutrition in the first week, and fluid/electrolyte derangement affects a substantial share of very-low-birth-weight infants during their admission. [4]
The at-risk groups are the ones every candidate must be able to recite, because they define who needs the tightest prescription. They are: the extremely and very preterm infant (large body water, high insensible loss, immature kidney, high surface-area-to-mass ratio), the very-low-birth-weight and growth-restricted infant (low substrate stores, high metabolic demand), the infant under radiant heat or phototherapy (exaggerated insensible loss), the surgical and critically ill infant (NEC, gastroschisis, ileus — nothing by mouth, high losses), the infant of a diabetic mother (electrolyte shifts, hypoglycaemia), and the exclusively breastfed term infant with poor lactation (hypernatraemic dehydration). [6]
Why these infants are vulnerable is the pathophysiology in miniature. The preterm kidney has a low glomerular filtration rate, limited concentrating ability (maximum ~600 mOsm/kg versus the adult's 1200), tubular immaturity with sodium wasting and poor acid excretion, and a high surface area that drives insensible water loss. The very-low-birth-weight infant compounds this with negligible glycogen and fat stores and the highest metabolic demand of any human. [9]
Social determinants shape the term-infant end of the picture. Poor lactation support, late initiation of feeding and limited access to weight monitoring make hypernatraemic dehydration over-represented among first-born infants of primiparous mothers and in communities with reduced postnatal support. [6]
Pathophysiology
To understand why a neonatal fluid order is so easily wrong, follow the water and the substrate. The story is the transition from placental to independent management, and it explains why overload and catabolism are the two great enemies. [4]
The first principle is body composition by gestation. Total body water falls from about 90% at 24 weeks to 75% at term, and extracellular fluid contracts correspondingly. This is why the preterm infant starts life with a larger, looser water compartment — more to lose as insensible loss, and more room to overload into oedema and a symptomatic ductus. The postnatal contraction of extracellular fluid is the physiological diuresis: the infant is meant to lose 5–10% of body weight in the first days as it sheds the extra water, then return to growth. [4] [10]

Against this stands the immature kidney. The low glomerular filtration rate means a water or solute load is excreted poorly, so overload becomes oedema, a patent ductus and heart failure. The limited concentrating ability means a small deficit in intake or a small excess in loss becomes dehydration and hypernatraemia. Tubular immaturity causes sodium wasting and poor hydrogen and ammonium excretion, producing late metabolic acidosis of prematurity — common enough that bicarbonate or acetate is routinely added to parenteral fluids. [8]
The nutrition side of the pathophysiology is the high metabolic demand and the danger of catabolism. The preterm brain is growing and myelinating at a rate unmatched later in life, demanding a continuous supply of glucose, amino acids and lipid. Withhold early amino acids and the infant enters negative nitrogen balance within hours — catabolising its own muscle, losing weight instead of growing, and accumulating extra-uterine growth restriction that is associated with poorer neurodevelopment. This is the rationale for starting parenteral amino acids on day 0 and advancing glucose to a glucose infusion rate that protects the brain. [7] [3]
One mechanism deserves special attention because it is common and dangerous: non-oliguric hyperkalaemia of the preterm. In the first days of life, especially below 28 weeks, potassium shifts out of cells because of immature Na+/K+-ATPase activity and rapid cell turnover — the serum potassium rises even with good urine output, and can reach levels that threaten the heart. This is a developmental phenomenon, not renal failure, but it demands ECG monitoring and treatment. [8]
Clinical Presentation
The neonate with disordered fluid, electrolyte or nutritional balance shows the body struggling with the water or the substrate, and the signs are the consequences. The problem is that the signs are non-specific and often late — which is why daily weight, intake/output and the electrolyte panel are the real monitoring tools, not the bedside examination alone. [6]
The fluid-overload signs are oedema (periorbital then sacral), a weight gain instead of the expected loss, a murmur or bounding pulses of a symptomatic PDA, increasing oxygen need and hepatomegaly. The dehydration signs are sunken fontanelle, dry mucous membranes, reduced skin turgor, oliguria, tachycardia and weight loss exceeding the expected 5–10% (term) or 15% (preterm). The electrolyte signs are the classic ones the candidate must recite: hypernatraemia (irritability, seizures, jitteriness), hyponatraemia (lethargy, seizures), hyperkalaemia (cardiac arrhythmia, ECG changes — peaked T waves, widened QRS), hypocalcaemia (jitteriness, seizures, apnoea) and metabolic acidosis (tachypnoea as compensation). [6]
A hyperkalaemic neonate with ECG changes is the emergency that commands immediate action: cardiac monitoring, calcium gluconate for membrane stabilisation, and measures to shift potassium into cells and remove it — all without delay. [8]
The nutritional failure signs are subtler and chronic: a weight curve falling away from the Fenton centile, poor head growth, and the biochemical markers of inadequate substrate (low urea from protein deficiency, metabolic acidosis, hypoglycaemia, osteopenia of prematurity on imaging). These are the fingerprints of extra-uterine growth restriction, and they accumulate silently over the first weeks if the nutrition prescription is too timid. [1] [7]
Differential Diagnosis
The differential turns on one question: is the derangement a consequence of the prescription, or a sign of disease? The answer is usually given by the trend of weight, intake/output and the electrolyte panel against the expected physiology. [6]
For hypernatraemia, the differential is dehydration from inadequate intake or excess loss (poor lactation in the breastfed term infant, high insensible loss in the preterm, diarrhoea, glycosuria) versus sodium excess from hypertonic fluid or bicarbonate. For hyponatraemia, it is dilution from fluid overload (the common iatrogenic cause in the preterm), sodium wasting from the immature kidney or diuretics, or true sodium depletion from GI or renal loss — and always exclude adrenal insufficiency and SIADH. For hyperkalaemia, distinguish the developmental non-oliguric form (preterm, first days, good urine output) from renal failure, tissue breakdown (haemolysis, NEC) and acidosis. [8]
For metabolic acidosis, the differential is the late metabolic acidosis of prematurity (protein load, tubular immaturity), renal bicarbonate wasting, inadequate perfusion or sepsis (lactic acidosis), and — especially with persistent or severe acidosis — an inborn error of metabolism. For growth failure, distinguish under-prescription of energy and protein (the commonest, correctable cause) from malabsorption, increased losses (stoma, reflux), and increased demand (chronic lung disease, sepsis, congenital heart disease). [9]
The anion gap and the trend separate benign from pathological: a rising anion gap with persistent acidosis, or a derangement that does not correct when the prescription is adjusted, points away from iatrogenic causes and toward disease. [9]
Clinical & Bedside Assessment
Begin with a focused perinatal history that frames the fluid and nutrition risk: gestation and birthweight, day of life, mode of feeding and tolerance, the current fluid and nutrition prescription, losses (stoma, drains, urine, stool), comorbidities (PDA, chronic lung disease, sepsis, NEC, surgery), and the drugs that act on water and electrolytes (diuretics, indomethacin, caffeine). [6]
Accurate daily weight is the single most important bedside measurement — it is the arbiter of the fluid prescription. Weigh at the same time, on the same scale, naked. Plot on a Fenton growth chart to judge whether the infant is following the centile (good nutrition) or falling away (under-nutrition or illness). Then examine systematically for the consequences: oedema or dehydration, perfusion and pulses (a PDA murmur, bounding or absent pulses), respiratory effort (overload worsens lung disease), and the neurological signs of electrolyte disturbance (jitteriness, seizures, tone). [4]
Bedside intake and output measurement is the practical tool of fluid surveillance: record every mL in (intravenous and enteral) and every mL out (urine, stool, stoma, drains), and calculate the balance against the expected insensible loss. A preterm infant under a radiant warmer can lose 60–100 mL/kg/day insensibly; a term infant in a cot far less. [9]
Finally, synthesise a one-line summary. A good example: "A 28-week, 1000-gram infant on day 4, on 140 mL/kg/day with a sodium of 132 and a weight now 4% below birthweight, tolerating 80 mL/kg/day of enteral feeds and on parenteral nutrition — transitioning well, advance feeds, add sodium, watch the weight." That sentence carries the day, the trajectory and the next move. [2]
Investigations
Neonatal fluid, electrolyte and nutritional management is monitored by the daily bundle — weight, intake/output, the electrolyte panel and the glucose — interpreted together, never in isolation. The role of investigation is to confirm the trend, catch derangement early, and exclude disease when the prescription is correct but the values are wrong. [9]
The cornerstone is the serum electrolyte and acid–base panel: sodium, potassium, chloride, bicarbonate (or a capillary gas), urea and creatinine, and ionised calcium, checked daily in the unstable or preterm infant and less often as the infant stabilises. The glucose is checked frequently in the first days to titrate the glucose infusion rate. Pair these with the weight and the intake/output record and the prescription is grounded. [6]
When derangement persists or is severe, tailor further tests to the pattern. A high potassium with ECG changes needs an urgent ECG and cardiac monitoring. Hypernatraemia needs paired urine and serum osmolality and sodium to localise the water deficit. Persistent metabolic acidosis needs a lactate, and if the anion gap is high or the acidosis disproportionate, a metabolic workup. Growth failure needs the nutritional markers (urea, prealbumin) and a review of the energy and protein prescription against the requirement. Osteopenia of prematurity — suspected on fractures or falling alkaline phosphatase-to-phosphate ratio — needs calcium, phosphate and alkaline phosphatase, with imaging if severe. [9]
Know what to avoid. Do not chase a single abnormal value without the weight, the intake/output and the trend — a sodium of 132 in an over-loaded preterm is treated by restricting water, not by giving hypertonic saline. Do not over-investigate a self-limiting developmental derangement (the non-oliguric hyperkalaemia of the preterm usually resolves). And do not let the electrolyte panel substitute for the growth chart — the nutrition question is answered by growth, not by biochemistry alone. [1]
The daily bundle to review every round
Management — Resuscitation
Most fluid and electrolyte problems do not need resuscitation beyond adjusting the prescription — the danger is assuming that is always true. A hyperkalaemic neonate with ECG changes, a severely dehydrated hypernatraemic infant, or an infant in shock from sepsis or NEC is an emergency that commands the full response. [8]
The resuscitation priorities specific to neonatal fluid and electrolyte crises are circulatory support and membrane/electrolyte stabilisation. For shock, give an isotonic crystalloid bolus (10 mL/kg normal saline, repeated as needed) and treat the cause. For symptomatic hyperkalaemia with ECG changes, give calcium gluconate (0.5 mL/kg of 10% slowly with ECG monitoring) to stabilise the myocardium, then shift potassium into cells with insulin–dextrose or a beta-agonist, and remove it with the kidney or gut. [8]
Escalate to a higher level of care when any of these is present: severe hypernatraemia (above 150 mmol/L) or hyponatraemia (below 125 mmol/L) with seizures, hyperkalaemia above 7.0 mmol/L or with ECG changes, metabolic acidosis with bicarbonate below 16 mmol/L, shock, or failure of the standard prescription to correct the derangement. [9]
The resuscitation errors to avoid are predictable: correcting hypernatraemia too rapidly (cerebral oedema and seizures — correct no faster than 0.5 mmol/L/hour or 10–12 mmol/L per day); giving hypertonic sodium for a dilutional hyponatraemia that needs water restriction; and chasing the number without the trend. Correct slowly, treat the cause, and monitor. [6]
Management — Definitive & Stepwise
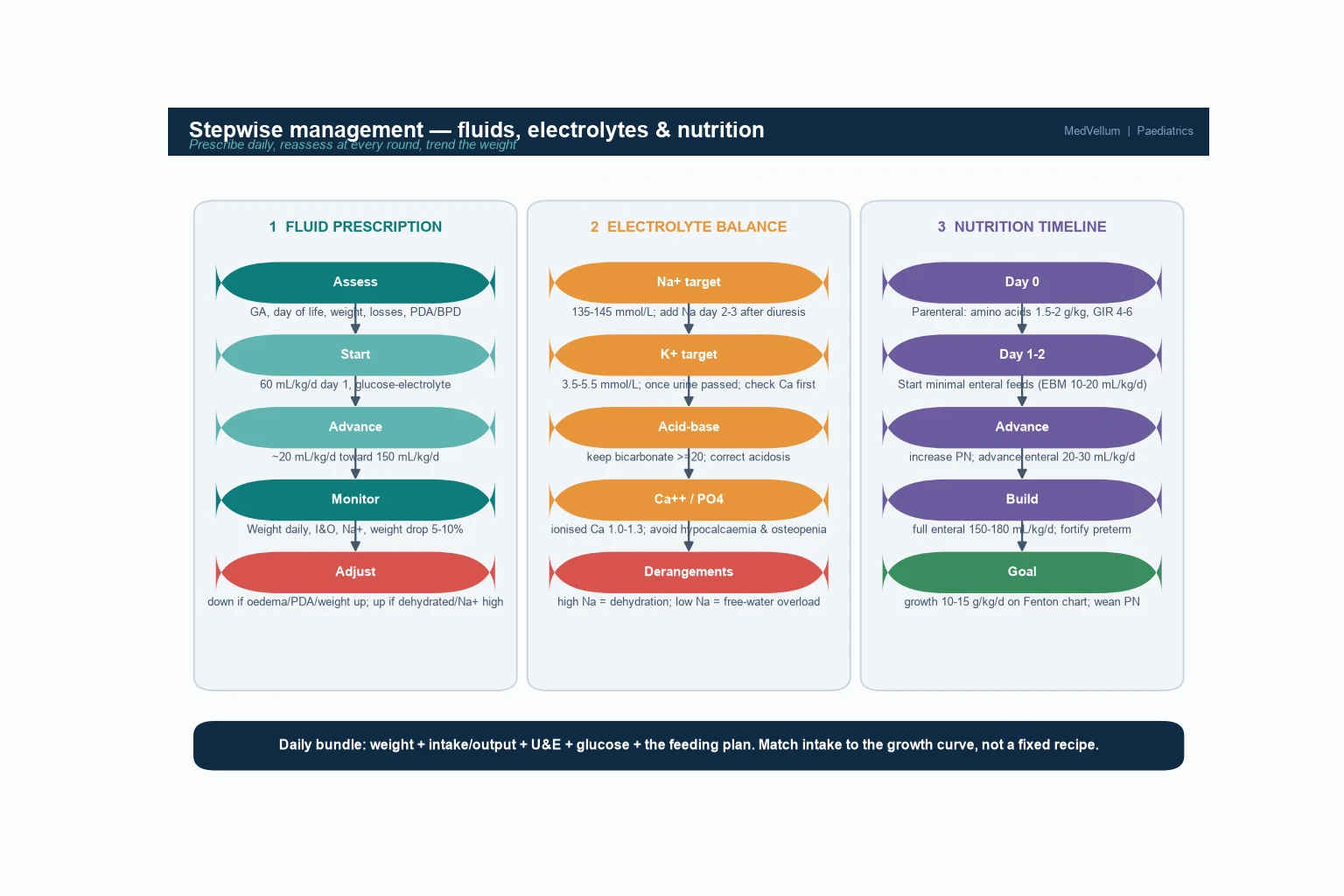
Once stable, definitive care is a sequence you can rehearse: prescribe the fluid by postnatal day, balance the electrolytes, advance the nutrition from parenteral to enteral, monitor the daily bundle, and grow the infant on the chart. [2]
- Prescribe the fluid by postnatal day. Start at 60 mL/kg/day on day 1 and advance by about 20 mL/kg/day toward 150 mL/kg/day (term) or 130–150 (preterm, lower with PDA/BPD). Restrict if there is oedema, a symptomatic PDA or unexpected weight gain; increase if there is dehydration, hypernatraemia or excessive weight loss. The fluid allowance is a starting point, not a rule — titrate to the infant. [4]
- Balance the electrolytes. Add sodium (2–3 mmol/kg/day) from day 2–3 once diuresis begins; add potassium (1–2 mmol/kg/day) only after urine output is established and only after calcium is checked. Give calcium (1–2 mmol/kg/day, higher in preterm), phosphate (1–2 mmol/kg/day) and magnesium (0.2–0.4 mmol/kg/day) parenterally at first, then enterally. Keep bicarbonate above 20 — add acetate or bicarbonate for late metabolic acidosis of prematurity. [2]
- Supply glucose at a glucose infusion rate (GIR) that protects the brain. Start at 4–6 mg/kg/min and advance as tolerated toward 10–12 mg/kg/min in the preterm; the GIR is the metric that matters, not the dextrose concentration. Hypoglycaemia injures the brain and hyperglycaemia drives osmotic diuresis and glycosuria — titrate to normoglycaemia. [7]
- Start parenteral nutrition on day 0 and advance deliberately. Begin amino acids at 1.5–2 g/kg/day from birth to prevent catabolism, advance lipid toward 3–3.5 g/kg/day, and provide the energy (110–135 kcal/kg/day for growth) and micronutrients (calcium, phosphate, trace elements, vitamins). The ESPGHAN guidelines frame this as the standard of care for the preterm. [2] [3]
- Start and advance enteral nutrition. Begin minimal enteral feeds (10–20 mL/kg/day of expressed breast milk) as soon as the infant is stable — the "trophic" or priming effect protects the gut and reduces the time to full feeds. Advance by 20–30 mL/kg/day in the stable preterm (slower if at risk of NEC), aiming for full enteral feeds at 150–180 mL/kg/day, with fortification of human milk for the preterm to meet protein and mineral needs. Breast milk is first-line. [1]
- Wean parenteral nutrition as enteral feeds build, and monitor for cholestasis (rising conjugated bilirubin and liver enzymes) with prolonged parenteral nutrition. The aim is full enteral feeds with growth on the Fenton chart. [9]
- Monitor the daily bundle and grow the infant. Review weight, intake/output, electrolytes, glucose and the feeding plan together every round. The goal is growth of 10–15 g/kg/day with head growth following — if the infant is not growing, the prescription is wrong, so increase energy and protein, not fluid alone. [7]
The first week of a 1000-gram preterm
Day 0 — start parenteral nutrition (amino acids 1.5–2 g/kg, GIR 4–6) and minimal enteral feeds
Prevent catabolism; prime the gut
Days 1–3 — fluid 60–100 mL/kg/day, expect weight drop 5–15%
Withhold sodium until diuresis; check K+ for non-oliguric hyperkalaemia
Days 3–7 — add sodium/potassium, advance fluid to 140 mL/kg/day and enteral feeds 20–30 mL/kg/d
Titrate to weight and electrolytes
Week 2 — build to full enteral feeds, fortify human milk, wean PN
Watch for cholestasis; start phosphate/calcium for bone
Goal — growth 10–15 g/kg/day on Fenton chart, full enteral feeds
The chart is the judge
Specific Subtypes & Scenarios
The extremely preterm and very-low-birth-weight infant. The most demanding patient — the largest body water, the highest insensible loss, the most immature kidney and the highest metabolic demand. Start parenteral amino acids on day 0, titrate fluid tightly, watch for non-oliguric hyperkalaemia in the first days, and advance enteral feeds cautiously (often slower than 30 mL/kg/day if NEC risk is high) with human milk. The goal is to avoid both early overload (PDA, BPD) and the extra-uterine growth restriction that blights this group. [9]
The late-preterm infant. More mature but still vulnerable to feeding difficulty, dehydration and hypoglycaemia. Fluid is more forgiving than in the extreme preterm, but poor lactation and slow feeding can tip the infant into hypernatraemic dehydration — monitor weight and feeding closely and support breastfeeding. [6]
The exclusively breastfed term infant with hypernatraemic dehydration. A largely preventable problem of poor lactation and intake. Sodium is typically above 150 mmol/L with weight loss exceeding 10%. Rehydrate carefully and slowly (correction no faster than 0.5 mmol/L/hour to avoid cerebral oedema), support lactation with expression and supplementation, and follow weight and sodium. [6]
The surgical and critically ill infant (NEC, gastroschisis). Nothing by mouth with high stoma and drain losses — nutrition is entirely parenteral, often fluid-restricted, so concentrate the parenteral nutrition to deliver protein and energy in a small volume. Measure every loss and replace it, and start enteral feeds only once the gut recovers. [9]
Infant with a symptomatic PDA or evolving bronchopulmonary dysplasia. Restrict fluid (the evidence from the Cochrane review supports liberal versus restricted fluid strategies, with restriction reducing PDA and necrotising enterocolitis), use diuretics judiciously in established BPD, and provide enough energy for growth despite the restriction by concentrating feeds. [4]
The infant with osteopenia of prematurity. Inadequate calcium, phosphate and vitamin D against the high bone-mineral demand of the preterm. Prevent with adequate parenteral and enteral calcium, phosphate and vitamin D; diagnose on a falling alkaline-phosphatase-to-phosphate ratio or fractures; and treat by increasing mineral intake. [5]
Complications & Pitfalls
Short-term, expect fluid overload (oedema, PDA, heart failure), dehydration and hypernatraemia, hyperkalaemia with arrhythmia, metabolic acidosis, hypoglycaemia and hyperglycaemia, and parenteral nutrition cholestasis with prolonged use. Long-term, the great complication is extra-uterine growth restriction — falling away from the growth centile with poor head growth — which is associated with worse neurodevelopment, alongside osteopenia of prematurity and the neurodevelopmental consequences of severe electrolyte disturbance. [4] [7]
The pitfalls are predictable, and worth naming so you avoid them. Treating the expected weight drop as abnormal — adding fluid when the infant is simply doing its physiological diuresis, precipitating overload. Overloading the preterm in the first days — the classic cause of PDA and worsening BPD. Withholding early amino acids for fear of intolerance — condemning the infant to catabolism and growth failure. [3] Correcting hypernatraemia too rapidly — cerebral oedema and seizures. Chasing a single electrolyte value without the weight and trend — a sodium of 132 in an overloaded infant is treated by restricting water, not by giving salt. And forgetting the growth chart — the nutrition question is answered by growth, not by the electrolyte panel alone. [6]
Prognosis & Disposition
Outcome is driven by the gestation, the presence of comorbidity (BPD, PDA, sepsis, NEC), and the success of the nutrition prescription in achieving growth — not by any single electrolyte value. Most self-limiting developmental derangements (non-oliguric hyperkalaemia, late metabolic acidosis) resolve with maturation and minor adjustment. The risk concentrates in the extremely preterm, where extra-uterine growth restriction and its neurodevelopmental consequences are the long shadow of inadequate early nutrition. [7]
The evidence that makes early aggressive parenteral nutrition worthwhile is the growing body linking early optimal parenteral nutrition to better neurodevelopment in very preterm infants — adequate early amino acids and energy protect brain growth, which is why starting parenteral nutrition on day 0 is now the standard of care rather than over-cautious. [7]
Disposition follows the risk. A stable growing preterm stays in the neonatal unit with daily monitoring until full enteral feeds and a steady growth trajectory. A surgical or critically ill infant needs intensive parenteral nutrition support and surgical collaboration. A term infant with hypernatraemic dehydration may need admission for slow rehydration and lactation support. In all cases, the growth chart sets the disposition — an infant not growing is not ready for discharge. [9]
Special Populations
Extremely preterm and very-low-birth-weight infants are the population in whom fluid and nutrition management most determines outcome. Provide day-0 parenteral amino acids, tight fluid titration, vigilant electrolyte monitoring (especially potassium in the first days), cautious enteral advancement with human milk and fortification, and track growth on the Fenton chart obsessively — every gram of growth matters for the brain. [7]
Indigenous and socioeconomically disadvantaged families carry a higher burden of preterm birth and reduced access to antenatal and postnatal support, raising the risk of poor lactation, hypernatraemic dehydration and inadequate nutrition follow-up. Provide culturally safe care, active lactation and feeding support, and ensure the growth-monitoring and follow-up loop does not drop after discharge. [6]
Rural and remote settings must plan for the fluid and nutrition needs of the preterm or unwell neonate from the first hours — accurate weight and intake/output, a basic electrolyte panel, a glucose infusion rate that protects the brain, and early retrieval before deterioration. A dehydrated or hyperkalaemic neonate born away from specialist support is an avoidable crisis — escalate and retrieve early, and support the family with telehealth in the interim. [9]
Surgical and complex infants (NEC, gastroschisis, short bowel) run on a nutrition-first, often fluid-restricted pathway — concentrated parenteral nutrition, meticulous loss replacement, and a deliberate, supervised transition to enteral feeds as the gut recovers, coordinated by the surgical and nutrition teams. [9]
Families of infants on prolonged parenteral nutrition need clear education on the feeding plan, the growth targets, the signs of cholestasis, and the safety-netting for readmission, with explicit community follow-up arranged before discharge. [1]
Evidence, Guidelines & Regional Differences
The foundational evidence for the fluid side is the Cochrane review of restricted versus liberal water intake in preterm infants (Bell & Acarregui): liberal fluid intake increases the risk of patent ductus arteriosus and necrotising enterocolitis without improving outcomes, so a restricted, titrated approach is the standard — the infant is expected to lose weight in the first days. [4] The Hartnoll randomised trial of postnatal sodium supplementation (2000) established that delayed sodium — given after the diuresis, not during it — produces better body composition in the preterm, which is why sodium is withheld until the weight drop begins. [10]
The nutrition evidence is the ESPGHAN guidelines. The 2022 enteral nutrition position paper (Embleton & Domellöf) sets the protein and energy targets and the advancement rates for preterm enteral feeding, [1] while the 2018 parenteral nutrition guidelines — energy (Joosten) [2] and amino acids (van Goudoever) [3] — set the targets and the rationale for early aggressive parenteral nutrition. The AAP clinical report on calcium and vitamin D (Abrams) sets the bone-mineral targets for enterally fed preterm infants. [5] The ESPGHAN position paper on nutritional management of the critically ill neonate (Moltu) frames the integrated approach for the surgical and unstable infant. [9]
The outcomes evidence is the Tesser (2025) study linking early optimal parenteral nutrition to neurodevelopmental outcomes in very preterm infants, which is the contemporary justification for not withholding early substrate. [7] The developmental electrolyte problems — non-oliguric hyperkalaemia (Aoki) [8] and hypernatraemic dehydration of the breastfed term infant (Sarin) [6] — round out the evidence base for the common derangements.
Two live areas of debate: the optimal rate of enteral feed advancement in the very preterm and growth-restricted infant (fast enough to grow, slow enough to avoid NEC — the evidence supports moderate advancement with human milk); and the best strategy to prevent extra-uterine growth restriction — early aggressive parenteral nutrition, fortification of human milk, and growth-chart vigilance together, rather than any single intervention. [1] [7]
Exam Pearls
- Neonatal fluid, electrolytes and nutrition are one prescription in three voices — water volume, ionic balance and growth substrate, all anchored to the postnatal day and the gestation. [2]
- The fluid ladder: 60 mL/kg/day on day 1, advancing ~20 mL/kg/day toward 150 mL/kg/day — restrict with PDA, BPD, overload; increase with dehydration and hypernatraemia. [4]
- The infant is meant to lose 5–10% of weight (up to 15% in the very preterm) in the first days — that is the physiological diuresis, do not "treat" it with extra fluid. [4]
- Sodium is withheld until diuresis begins (day 2–3); potassium is added only after urine output is established and calcium is checked. [10]
- The glucose infusion rate (GIR) is the metric that matters (4–6 mg/kg/min, up to 10–12 in the preterm) — not the dextrose concentration. [7]
- Start parenteral amino acids on day 0 (1.5–2 g/kg/day) to prevent catabolism and extra-uterine growth restriction — the brain is growing now. [3]
- The Cochrane review (Bell & Acarregui) found liberal fluid increases PDA and NEC — restricted, titrated fluid is the standard. [4]
- Hypernatraemic dehydration of the breastfed term infant is corrected slowly (no faster than 0.5 mmol/L/hour) to avoid cerebral oedema. [6]
- Non-oliguric hyperkalaemia of the preterm is a developmental phenomenon (immature Na+/K+-ATPase), not renal failure — monitor the ECG and treat severe or symptomatic cases. [8]
- Growth on the Fenton chart is the judge: 10–15 g/kg/day with head growth following. If the infant is not growing, the prescription is wrong — increase energy and protein, not fluid alone. [1] [7]
References
- [1]Embleton ND, Domellöf M, ESPGHAN Committee on Nutrition Enteral nutrition in preterm infants (2022): a position paper from the ESPGHAN Committee on Nutrition. Journal of Pediatric Gastroenterology and Nutrition, 2023.PMID 36705703
- [2]Joosten K, van Goudoever JB, ESPGHAN/ESPEN/ESPR/CSPEN working group ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: energy. Clinical Nutrition, 2018.PMID 30078715
- [3]van Goudoever JB, ESPGHAN/ESPEN/ESPR/CSPEN working group ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: amino acids. Clinical Nutrition, 2018.PMID 30100107
- [4]Bell EF, Acarregui MJ Restricted versus liberal water intake for preventing morbidity and mortality in preterm infants. Cochrane Database of Systematic Reviews, 2008.PMID 18253981
- [5]Abrams SA, AAP Committee on Nutrition Calcium and vitamin D requirements of enterally fed preterm infants. Pediatrics, 2013.PMID 23629620
- [6]Sarin A, Yaklin CW Neonatal hypernatremic dehydration. Pediatric Annals, 2019.PMID 31067335
- [7]Tesser F, Verlato G Early optimal parenteral nutrition during NICU stay and neurodevelopmental outcomes in very preterm infants. Nutrients, 2025.PMID 39861362
- [8]Aoki K, Akaba K Characteristics of nonoliguric hyperkalemia in preterm infants: a case-control study. Pediatrics International, 2020.PMID 31863677
- [9]Moltu SJ, ESPGHAN Committee on Nutrition Nutritional management of the critically ill neonate: a position paper of the ESPGHAN Committee on Nutrition. Journal of Pediatric Gastroenterology and Nutrition, 2021.PMID 33605663
- [10]Hartnoll G, Bédu A, Modi N Randomised controlled trial of postnatal sodium supplementation on body composition in 25 to 30 week gestational age infants. Archives of Disease in Childhood — Fetal and Neonatal Edition, 2000.PMID 10634837