Paeds · fetal-neonatal-and-perinatal
Neonatal hypoglycaemia
Also known as Neonatal hypoglycemia · Neonatal low blood glucose · Transitional neonatal hypoglycaemia · Hyperinsulinaemic neonatal hypoglycaemia · Neuroglycopenia of the newborn
Fellowship guide to neonatal hypoglycaemia: why the newborn brain is glucose-dependent, the operational treatment thresholds, classification by duration and cause, recognition of neuroglycopenic signs, the differential of persistent hypoglycaemia with the critical sample, and the stepwise dextrose ladder from feeds to refractory-case adjuncts.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a two-hour-old infant of a diabetic mother, jittery on the postnatal ward, whose pre-feed glucose is 1.6 mmol/L. Before you reach for the cannula or dismiss the reading as "normal for a newborn", hold two ideas separate in your mind: how low is the glucose, and why is it low — is this a failed transition, or a sign of disease? [5]
Neonatal hypoglycaemia is best defined as a blood glucose concentration below the operational threshold at which intervention is warranted, rather than by a single fixed laboratory number. [5] That phrasing is deliberate and examiner-friendly: there is no single glucose value that cleanly predicts brain injury, so thresholds are pragmatic, time-dependent and consensus-derived. The commonly used operational thresholds rise with postnatal age — below 2.0 mmol/L in the first 24 hours, below 2.6 mmol/L from 24 to 48 hours, and below 3.0 mmol/L beyond 48 hours — though local policy (AAP, PES, NICE, ADIPS) varies, and the symptomatic infant is treated at any low value without waiting. [6]
The reason these thresholds exist at all is the newborn brain's absolute dependence on glucose. In fetal life the placenta supplies glucose continuously; at birth that supply stops abruptly and the newborn must transition to intermittent feeding while its own glycogenolysis, gluconeogenesis and counter-regulatory hormones mature. Most neonatal hypoglycaemia is a transient failure of that transition — common and usually benign with feeding. The minority that is persistent, severe or symptomatic marks real disease, and it is that minority the candidate must not miss. [1]
So the examiner's first question is always: is this a low glucose that will resolve with feeds, or one that needs investigation and treatment? That single distinction drives the whole neonatal plan. [7]
Classification
Begin with the duration, then probe the cause. [5]
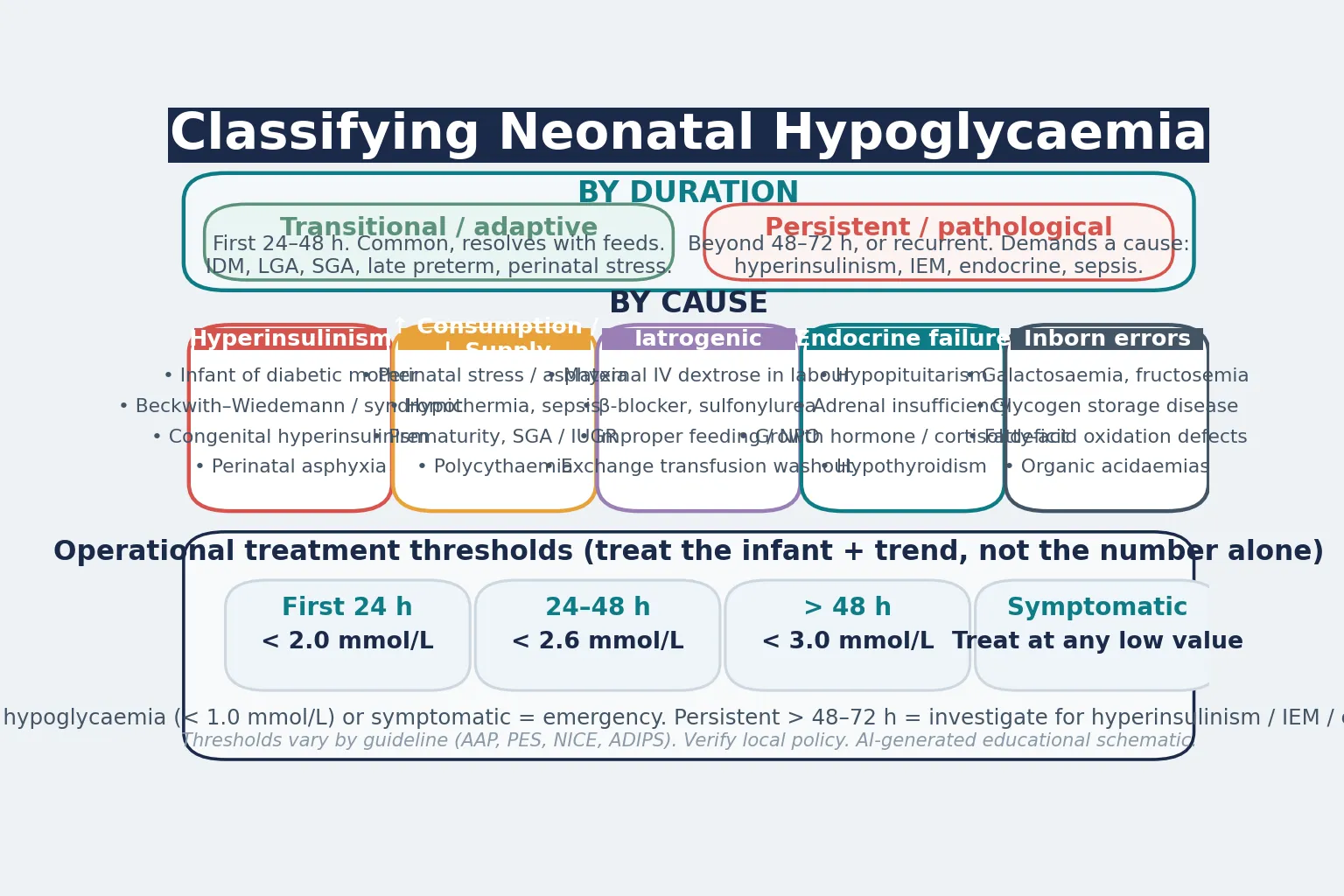
By duration, separate transitional from persistent hypoglycaemia. Transitional (adaptive) hypoglycaemia occurs in the first 24–48 hours in an at-risk infant whose counter-regulation is immature or overwhelmed — it is common, usually asymptomatic, and resolves with feeds. Persistent (pathological) hypoglycaemia lasts beyond 48–72 hours, recurs, or demands a high glucose infusion rate, and it forces the search for a cause. [7]
By cause, five mechanistic categories cover the ground. Hyperinsulinaemic hypoglycaemia — the most dangerous form because insulin suppresses ketogenesis as well as lowering glucose — is seen in the infant of a diabetic mother, perinatal asphyxia, Beckwith–Wiedemann syndrome and congenital hyperinsulinism. Increased glucose consumption or decreased supply covers perinatal stress, hypothermia, sepsis, prematurity, and the small-for-gestational-age or growth-restricted infant with low stores. Iatrogenic causes include maternal intrapartum dextrose, maternal sulfonylurea or β-blocker, exchange transfusion washout, and improper feeding or fasting. Endocrine failure — hypopituitarism, adrenal insufficiency and hypothyroidism — is rare but treatable. Finally, inborn errors of metabolism (galactosaemia, fatty-acid oxidation defects, glycogen storage disease, organic acidaemias) present with persistent or recurrent hypoglycaemia, often with acidosis or hyperammonaemia. [7]
Epidemiology & Risk Factors
Neonatal hypoglycaemia is the commonest metabolic disturbance of the newborn. Depending on the threshold used and the population screened, up to half of "at-risk" infants have at least one low reading in the first days of life — though the great majority are asymptomatic and resolve with feeds. [6]
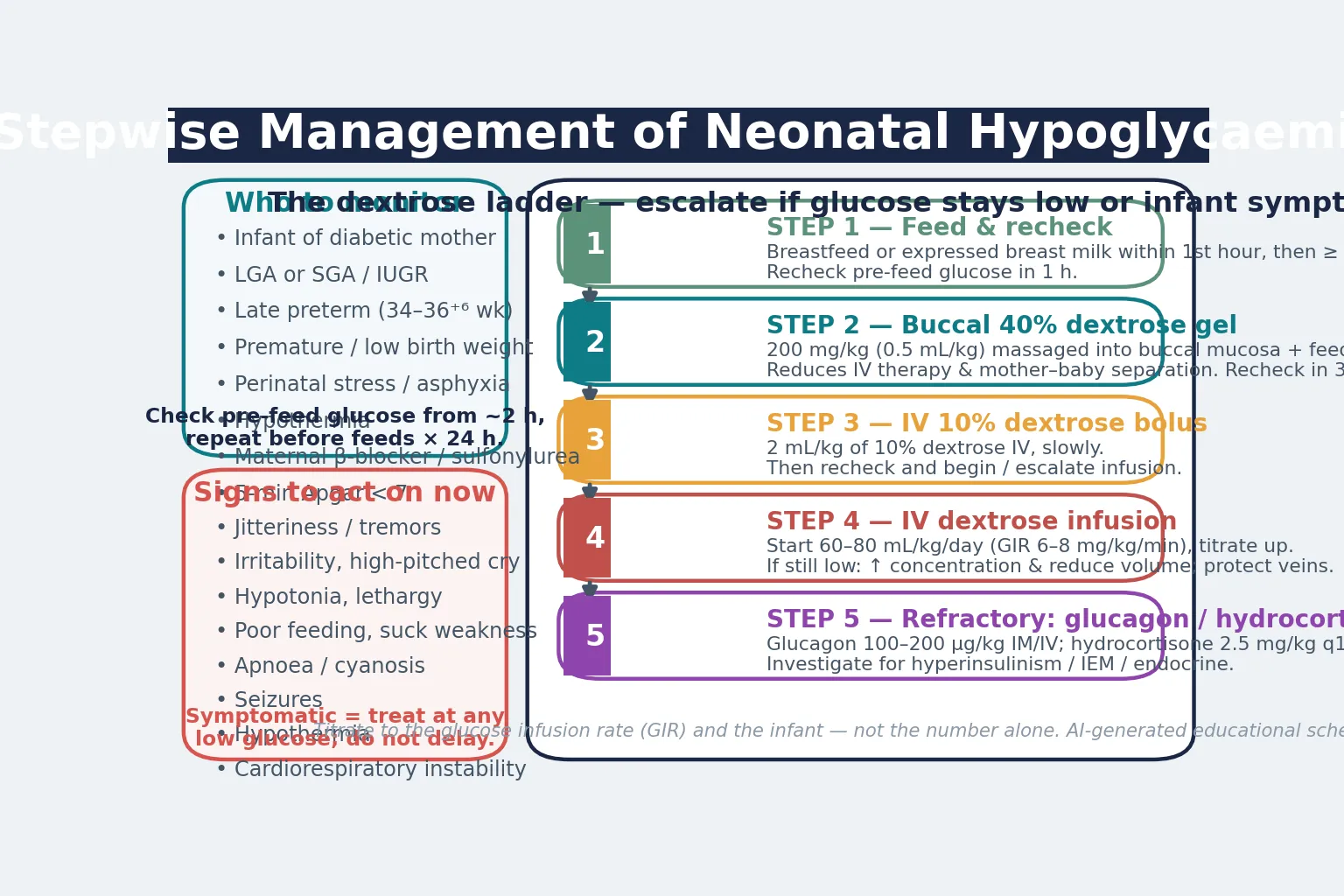
The at-risk groups are the ones every candidate must be able to recite, because they define who gets routine bedside surveillance. They are: the infant of a diabetic mother (the highest-risk single group, because of persistent hyperinsulinaemia), large-for-gestational-age and small-for-gestational-age or growth-restricted infants, the late-preterm infant (34 to 36+6 weeks) and the premature or low-birth-weight infant, infants with perinatal stress or asphyxia, hypothermia, infants exposed to maternal β-blockers or sulfonylureas, and any infant with a 5-minute Apgar below 7. [6]
Why these infants are vulnerable is the pathophysiology in miniature. The infant of a diabetic mother arrives hyperinsulinaemic from chronic intrauterine glucose exposure. The preterm and growth-restricted infant has immature counter-regulation, low glycogen and fat stores, and limited gluconeogenic capacity, so the nadir is deeper and longer. Perinatal stress and hypothermia raise glucose consumption while suppressing the response. [6]
Social determinants shape the whole picture. Gestational diabetes, obesity, food insecurity and reduced antenatal access raise both the prevalence of the at-risk state and the severity of the dip, so hypoglycaemia is over-represented among socioeconomically disadvantaged families and in communities with high diabetes prevalence. [8]
Pathophysiology
To understand why a low glucose is an emergency in a newborn, follow the fuel. The story is the brain's absolute glucose dependence, and it explains why hypoglycaemia injures here and now. [5]
Glucose is the obligatory cerebral fuel in the immediate newborn period, and the brain carries essentially no glycogen reserve of its own. When blood glucose falls below the brain's needs, glucose transport into neurons (via GLUT transporters) fails, intracellular ATP production collapses, and the neuronal fuel starvation begins. [5] Energy failure disables the membrane sodium–potassium pump, producing cytotoxic oedema; glutamate-mediated excitotoxicity and apoptosis then complete the injury. The occipital and parietal cortex are preferentially affected — which is why visual impairment, seizures and posterior-predominant changes on imaging are the signatures of significant neonatal hypoglycaemic brain injury. [1]
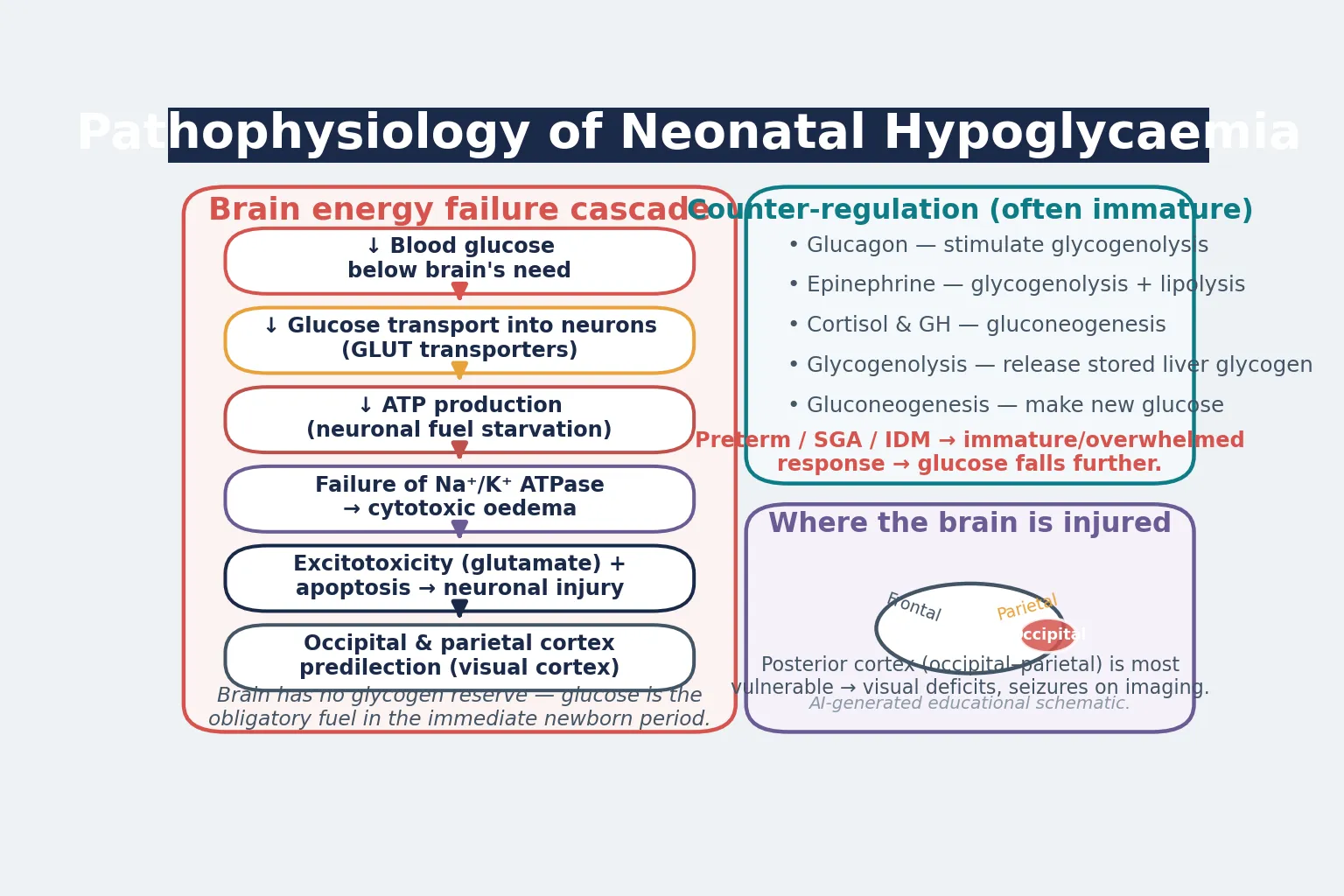
Against this stands the counter-regulatory response, which is often immature in the newborn. Glucagon drives glycogenolysis, epinephrine drives glycogenolysis and lipolysis, and cortisol and growth hormone drive gluconeogenesis; together with hepatic glycogenolysis, gluconeogenesis and ketogenesis they defend the blood glucose. In the preterm, small-for-gestational-age and infant of a diabetic mother these defences are immature or overwhelmed, so the glucose falls further and the brain is exposed longer. [6]
One mechanism deserves special attention because it is the most dangerous: hyperinsulinaemic hypoglycaemia. In the infant of a diabetic mother, maternal glucose crossing the placenta drove the fetal pancreas to secrete high insulin throughout pregnancy; at cord clamp the glucose supply stops abruptly but insulin persists, driving glucose into cells and — critically — suppressing ketogenesis, so the brain is deprived of both glucose and its ketone fallback fuel. This is why hyperinsulinaemic hypoglycaemia is the deepest, most persistent and most injurious form, and why congenital hyperinsulinism demands urgent specialist care. [9]
Clinical Presentation
The hypoglycaemic neonate shows the brain running out of fuel, and the signs are the brain's distress. The problem is that the signs are non-specific — which is why a glucose check is mandatory in any at-risk or unwell neonate, and why relying on signs alone misses the asymptomatic majority. [5]
The neuroglycopenic signs are the headline: jitteriness and tremors, irritability, a high-pitched cry, hypotonia, lethargy, poor feeding with a weak suck, apnoea, cyanosis, and in the worst case seizures and altered consciousness. The autonomic or adrenergic signs — tachycardia, pallor, vomiting, and (rarely in the neonate) sweating — round out the picture but are inconsistent. [6]
A seizing hypoglycaemic neonate is the emergency that commands immediate action: intravenous dextrose without delay, alongside airway and breathing support and seizure control. Do not wait for a confirmatory laboratory glucose in a symptomatic infant — treat on the point-of-care reading and send the laboratory sample concurrently. [1]
Two patterns deserve mention. An infant with chronic intrauterine hypoglycaemia — a severely growth-restricted baby, for example — may have down-regulated its adrenergic response and present with few warning signs, looking deceptively well until a routine glucose check reveals a very low value. Conversely, the asymptomatic at-risk infant with a low screening reading is the commonest presentation of all, and is exactly the case where structured pre-feed monitoring prevents progression to symptoms and injury. [6]
Differential Diagnosis
The differential turns on one question: is this a failed transition, or a pathological cause? The answer is usually given by time and behaviour — a transient dip that resolves with feeds in the first day is almost always adaptive, while hypoglycaemia that is persistent, recurrent, severe, or needs a high glucose infusion rate demands a cause. [7]
When hypoglycaemia persists or recurs beyond 48–72 hours, the pathological causes to exclude are congenital hyperinsulinism, the inborn errors of metabolism (galactosaemia, fatty-acid oxidation defects, glycogen storage disease, organic acidaemias), endocrine deficiency (hypopituitarism, adrenal insufficiency, hypothyroidism), and sepsis. The tool that separates them is the critical (hypoglycaemic) sample — blood drawn while the glucose is genuinely low — read for insulin, free fatty acids, ketones, lactate, ammonia, cortisol, growth hormone and the metabolic screen. [7]
The glucagon response is a bedside discriminator: a brisk glycaemic rise after glucagon indicates hyperinsulinaemia (the liver is primed with glycogen and insulin is blocking its release), whereas a flat response points to depleted stores or a storage disorder. [9] A careful drug and birth history excludes the iatrogenic causes — maternal intrapartum dextrose, sulfonylurea, β-blocker, or an exchange transfusion — which are reversible and easily missed. [6]
Clinical & Bedside Assessment
Begin with a focused antenatal and perinatal history that frames the glucose risk: maternal diabetes type and glycaemic control (HbA1c, third-trimester trend, medications), gestation, birthweight and centile, perinatal distress or asphyxia, maternal drugs (insulin, sulfonylurea, β-blocker), the intrapartum glucose control, and the feeding plan. [6] An infant of a poorly controlled diabetic delivered for suspected macrosomia is a very different patient from a constitutionally small, well, late-preterm infant of a non-diabetic mother.
Accurate anthropometry sets the at-risk status: weigh the baby, measure length and head circumference, and plot on a gestation- and sex-specific chart to identify LGA, SGA or growth restriction. Then examine systematically for the cause and the consequences — temperature (hypothermia raises consumption), perfusion and tone, feeding competence and suck, and the neuroglycopenic signs (jitteriness, tremor, hypotonia, irritability, altered consciousness). [5]
Bedside point-of-care glucose testing is the practical tool of surveillance. Check the first glucose at around two hours of age in an at-risk infant (after the first feed), and repeat before feeds through the first 24 hours and longer if readings are low or the infant is symptomatic. [6] Confirm a critical reading with a laboratory measurement when persistent or severe, but never delay treatment of a symptomatic infant for confirmation. [1]
Finally, synthesise a one-line summary. A good example: "A two-hour-old, 39-week infant of a diabetic mother, jittery with a pre-feed glucose of 1.6 mmol/L after a breastfeed — symptomatic transitional hypoglycaemia in an IDM, treat up the ladder." That sentence carries the category, the severity and the first move. [3]
Investigations
Neonatal hypoglycaemia is diagnosed and surveilled at the bedside — the role of investigation is to define the cause when hypoglycaemia is persistent, recurrent, severe, or unusually refractory. [7]
The cornerstone of surveillance is scheduled point-of-care glucose monitoring: a first check around two hours of age in at-risk infants, repeated before each feed through the first 24 hours (and longer if low). A single normal reading never clears an at-risk infant — the nadir of the IDM's hyperinsulinaemia peaks over the first hours, so repeated pre-feed checks are essential to catch it. [6]
The critical (hypoglycaemic) sample is the key investigation of persistent hypoglycaemia, drawn while the glucose is genuinely low (ideally below 2.6 mmol/L) and before treatment raises it. It includes glucose, insulin, C-peptide, free fatty acids, β-hydroxybutyrate (ketones), lactate, ammonia, cortisol, growth hormone, and a blood gas. The diagnostic fingerprint of hyperinsulinaemic hypoglycaemia is an inappropriately non-suppressed insulin with low free fatty acids and ketones — insulin both lowers glucose and suppresses the alternative fuels the brain needs. [7]
Tailor further tests to the pattern. A blood gas, lactate and ammonia screen for the inborn errors; plasma amino acids, acylcarnitines and urine organic acids for the metabolic disorders; a galactosaemia screen (and urinary reducing substances) when jaundice and liver dysfunction accompany hypoglycaemia; thyroid function and cortisol for endocrine deficiency; and genetics and an 18-fluorodopa PET scan to localise focal congenital hyperinsulinism before surgery. After a significant symptomatic event, a cranial ultrasound or MRI looks for the posterior-cortical injury that is the signature of severe hypoglycaemic brain damage. [9]
Know what to avoid. Do not delay treatment of a symptomatic infant for a confirmatory laboratory glucose. Do not investigate a simple transient dip that resolves with feeds — that over-medicalises a well infant and undermines breastfeeding. And do not let a single normal reading close the surveillance window on an at-risk neonate. [1]
The at-risk groups to monitor
Management — Resuscitation
Most at-risk infants do not need resuscitation beyond early feeding — the danger is assuming that is always true. A seizing or profoundly lethargic hypoglycaemic neonate is an emergency that commands the full response: secure the airway and breathing, give intravenous dextrose without delay, and control seizures. [1]
The two resuscitation priorities specific to neonatal hypoglycaemia are early feeding and glucose. Establish breastfeeding or expressed breast milk within the first hour, keep the baby warm and normothermic (hypothermia worsens hypoglycaemia), and check a pre-feed glucose in the at-risk groups. [6]
Escalate to a higher level of care when any of these is present: symptomatic hypoglycaemia (seizures, apnoea, cyanosis, altered consciousness), persistent hypoglycaemia despite feeds and buccal dextrose gel, glucose below 1.0 mmol/L at any time, a requirement for intravenous dextrose or a high glucose infusion rate, or any sign of an underlying metabolic or endocrine cause. [3]
The resuscitation errors to avoid are predictable: withholding treatment while awaiting a confirmatory laboratory glucose in a symptomatic infant; treating the number rather than the infant and the trend; and giving a hypertonic glucose bolus that rebounds into hyperglycaemia and osmotic injury. Treat the infant, confirm concurrently, and titrate. [5]
Management — Definitive & Stepwise
Once stable, definitive care is a sequence you can rehearse: feed, monitor, treat the low glucose up the ladder, investigate the persistent case, support feeding, and follow up. [3]
- Early and frequent feeding. Establish breastfeeding or expressed breast milk within the first hour, then feed at least every 2–3 hours. Breast milk is first-line; the aim is a steady exogenous glucose supply to support the transition. [6]
- Scheduled glucose monitoring. Check pre-feed glucose on a schedule through the first day, and longer if low or symptomatic. Treat the infant and the trend, not the number alone. [5]
- Buccal 40% dextrose gel. If glucose is low, give buccal 40% dextrose gel at 200 mg/kg (approximately 0.5 mL/kg) massaged into the buccal mucosa, with a feed, and recheck in 30 minutes. The Sugar Babies trial established this as effective first-line treatment that reduces intravenous therapy and mother–baby separation, and the Cochrane reviews confirmed its prophylactic and treatment role. [3] [4]
- Intravenous 10% dextrose bolus. If glucose stays low or the infant is symptomatic, give an intravenous bolus of 10% dextrose at 2 mL/kg, slowly, then recheck. [1]
- Escalating dextrose infusion. Begin an intravenous dextrose infusion titrated to a glucose infusion rate (GIR) of 6–8 mg/kg/min, escalating the concentration while protecting the veins and reducing volume if needed. A requirement above 10–12 mg/kg/min signals hyperinsulinaemia and warrants investigation. [9]
- Refractory-case adjuncts. For hypoglycaemia that persists despite a high glucose infusion rate, add glucagon (100–200 µg/kg intramuscularly or intravenously) and hydrocortisone (2.5 mg/kg every 12 hours), and investigate urgently for hyperinsulinism, inborn errors and endocrine deficiency. [7]
- Investigate and refer persistent disease. Persistent or recurrent hypoglycaemia triggers the critical sample, a metabolic and endocrine workup, and referral to paediatric endocrinology and genetics — for congenital hyperinsulinism that may mean diazoxide, octreotide, 18-FDOPA imaging and surgery. [9]
Plan discharge once the baby is glucose-stable on full enteral feeds without treatment, feeding competently, thermally stable, with an acceptable weight trend and confident parents who know the signs to return for. [3]
Plan follow-up from discharge: monitor growth and feeding, offer neurodevelopmental and visual surveillance after a severe or recurrent event, and ensure the metabolic-endocrine pathway is in place for any infant being investigated for persistent disease. [2]
The first two hours
Identify at-risk infant (IDM, LGA, SGA, late preterm, perinatal stress)
Set up pre-feed glucose monitoring from ~2 h
Feed within the first hour and keep warm
Breast milk first-line; aim normothermia
Check pre-feed glucose at ~2 h, repeat before feeds
Single normal reading does not clear the infant
If low → buccal 40% dextrose gel 200 mg/kg + feed + recheck
Escalate if glucose stays low or infant symptomatic
Symptomatic or persistent → IV 10% dextrose 2 mL/kg bolus, then infusion
Investigate persistent/refractory disease
Specific Subtypes & Scenarios
Transitional hypoglycaemia of the at-risk infant. The commonest form — an asymptomatic low reading in the first day in an IDM, LGA, SGA or late-preterm infant. Manage with early and frequent feeding, buccal dextrose gel as needed, and scheduled monitoring; it resolves and the infant stays with mother. [3]
Infant of a diabetic mother. The highest-risk single group, because of persistent hyperinsulinaemia. Predict an early, steep glucose fall; schedule pre-feed monitoring from the first feed; and use feeds and buccal gel first, escalating to intravenous dextrose if low or symptomatic. [6]
Late-preterm and small-for-gestational-age infant. Compounded risk from immaturity and low stores — the nadir is deeper and longer, feeding is harder, and the threshold for monitoring and intravenous therapy is lower. Provide dedicated feeding support and a low threshold for transitional care or NICU. [6]
Persistent hypoglycaemia beyond 48–72 hours. Pursue a pathological cause with the critical sample and a structured metabolic and endocrine workup. Do not manage persistent hypoglycaemia as a failed transition — it is a sign of disease. [7]
Congenital hyperinsulinism. Severe persistent hypoglycaemia with a high glucose requirement, suppressed ketones and a brisk glucagon response. Refer urgently to paediatric endocrinology for a diazoxide trial and possible 18-FDOPA imaging and surgery — early diagnosis and treatment change the neurological outcome. [9]
Inborn error of metabolism. Galactosaemia, fatty-acid oxidation defects and glycogen storage disease present with persistent hypoglycaemia, often with acidosis, hyperammonaemia or liver dysfunction. Identify by the metabolic pattern, stop the offending substrate (galactose-free feed in galactosaemia), and involve the metabolic service. [7]
Rural and remote setting. Plan early feeding, point-of-care glucose and buccal gel, and retrieval before deterioration. A seizing hypoglycaemic neonate away from intravenous access is an avoidable crisis — escalate and retrieve early. [8]
Complications & Pitfalls
Short-term, expect recurrent or refractory hypoglycaemia, the need for intravenous dextrose, seizures, and the disturbance that an underlying metabolic or endocrine cause produces. Long-term, severe or recurrent neonatal hypoglycaemia is associated with neurodevelopmental sequelae — occipital cortical injury, visual impairment, epilepsy and cognitive impairment — which is exactly why pre-empting and treating it is evidence-based rather than over-cautious. [1] [2]
The pitfalls are predictable, and worth naming so you avoid them. Relying on clinical signs alone when many hypoglycaemic neonates are asymptomatic — in an at-risk infant, check the glucose. A single normal reading falsely reassuring you — the IDM's insulin peaks over the first hours, so schedule repeated pre-feed checks. [6] Treating the number rather than the infant — an asymptomatic at-risk infant just below threshold who feeds and rechecks upward is different from a seizing one. Failing to investigate persistent hypoglycaemia — missing congenital hyperinsulinism or a treatable inborn error. Over-treating with hypertonic boluses — rebound hyperglycaemia and osmotic injury. And displacing breastfeeding with unnecessary formula or admission — most at-risk infants are managed with mother with feeds and buccal gel. [5]
Prognosis & Disposition
Outcome is driven by the severity, persistence and symptomatic burden of the hypoglycaemia, and the promptness of treatment — not by the lowest single number. Most transient, asymptomatic hypoglycaemia resolves with feeds without sequelae. The risk concentrates in the severe, recurrent, symptomatic and hyperinsulinaemic cases. [1]
The evidence that makes surveillance worthwhile is the McKinlay work on neonatal glycaemia: severe or recurrent hypoglycaemia is associated with adverse neurodevelopment at 2 and 4.5 years, which is why pre-empting the dip from the first feed, monitoring on a schedule, and treating promptly are evidence-based, not over-cautious. [1] [2] For congenital hyperinsulinism, early diagnosis and treatment meaningfully change the neurological outcome. [9]
Disposition follows the risk. A well at-risk infant feeding and normoglycaemic stays with mother with scheduled glucose checks. A moderate-risk infant needing buccal gel or observation goes to transitional care. A severe, symptomatic, or refractory infant — seizures, glucose below 1.0 mmol/L, persistent disease, or needing a high glucose infusion rate — goes to NICU with the neonatal team involved and, in the rural setting, retrieval activated early. [3]
Special Populations
Indigenous and socioeconomically disadvantaged families carry a higher burden of gestational diabetes, obesity and access barriers, raising both the prevalence of the at-risk state and the severity of the dip. Provide culturally safe antenatal and postnatal care, address nutrition and lifestyle directly, and ensure the surveillance and follow-up loop does not drop. [8]
Rural and remote settings must plan feeding, point-of-care glucose, buccal dextrose gel and retrieval before deterioration. A hypoglycaemic neonate born away from intravenous access and specialist support is an avoidable crisis — escalate and retrieve early, and support the family with telehealth in the interim. [8]
Late-preterm and small-for-gestational-age infants compound prematurity and low stores — RDS-like respiratory distress, hypothermia, feeding difficulty and hypoglycaemia all stack, lowering the threshold for monitoring and transitional care or NICU admission. [6]
Out-of-home-care and migrant-refugee infants need deliberate continuity — confirm growth monitoring, metabolic and neurodevelopmental follow-up are transferred, not lost, across moves. [2]
Congenital hyperinsulinism and complex metabolic disease run on a specialist, technology-dependent pathway — diazoxide, octreotide, 18-FDOPA imaging, surgery, genetics — coordinated by paediatric endocrinology and the metabolic service. [9]
Families of infants needing prolonged glucose support need clear parent education, breastfeeding support, and explicit safety-netting on the neuroglycopenic signs to return for. [3]
Evidence, Guidelines & Regional Differences
The foundational evidence for the danger of neonatal hypoglycaemia is the McKinlay programme: the 2015 trial established that severe or recurrent hypoglycaemia is associated with adverse neurodevelopment at 2 years, [1] and the 2017 follow-up extended that association to 4.5 years. [2] These are the studies that justify proactive monitoring and treatment.
The treatment evidence is the Sugar Babies trial (Harris 2013), which established buccal 40% dextrose gel as effective first-line treatment that reduces intravenous therapy and mother–baby separation, [3] and the Cochrane reviews (Edwards 2021 and 2023) that confirmed its role in both prophylaxis and treatment of at-risk neonates. [4] [10] The hPOD trial (Harris 2021) tested prophylactic dextrose gel in at-risk infants and informed but did not settle the question of routine prophylaxis. [8]
The threshold and persistent-disease frameworks come from the AAP postnatal glucose homeostasis guidance (Adamkin 2011), [6] the Pediatric Endocrine Society recommendations for persistent hypoglycaemia (Thornton 2015), [7] and the foundational operational thresholds concept of Cornblath (2000). [5] Congenital hyperinsulinism is summarised in the Orphanet review (Banerjee 2022). [9]
Two live controversies: the operational threshold itself — there is no single glucose value that cleanly predicts brain injury, hence thresholds are pragmatic and time-dependent; and universal versus targeted screening — whether to screen all newborns or only the at-risk groups, balancing missed cases against over-medicalising well infants. [5]
Exam Pearls
- Neonatal hypoglycaemia is an operational treatment threshold, not a single number — first 24 h below 2.0, 24–48 h below 2.6, beyond 48 h below 3.0 mmol/L; treat the symptomatic infant at any low value. [5]
- The brain has no glycogen reserve and glucose is its obligatory fuel — low glucose is neuroglycopenia and energy failure, preferentially in the occipital–parietal cortex. [1]
- The dextrose ladder: feed → buccal 40% dextrose gel 200 mg/kg → IV 10% dextrose 2 mL/kg bolus → escalating infusion (GIR 6–8 mg/kg/min) → glucagon/hydrocortisone for refractory. [3]
- A single normal glucose does not clear the at-risk infant — schedule repeated pre-feed checks. [6]
- Persistent hypoglycaemia beyond 48–72 h = take the critical sample. Inappropriately high insulin with low ketones = hyperinsulinaemic (the most dangerous form, because insulin suppresses ketogenesis). [7]
- The glucagon response is brisk in hyperinsulinaemia (glycogen-rich liver, insulin blocking release) and flat in depleted stores or storage disorders. [9]
- Acidosis or hyperammonaemia with hypoglycaemia = inborn error of metabolism; stop the offending substrate and involve the metabolic service. [7]
- The Sugar Babies trial (Harris 2013) made buccal dextrose gel first-line; the McKinlay studies (2015, 2017) are the evidence that surveillance and prompt treatment prevent neurodevelopmental harm. [3] [1]
References
- [1]McKinlay CJ Neonatal glycemia and neurodevelopmental outcomes at 2 years. New England Journal of Medicine, 2015.PMID 26465984
- [2]McKinlay CJD Association of neonatal glycemia with neurodevelopmental outcomes at 4.5 years. JAMA Pediatrics, 2017.PMID 28783802
- [3]Harris DL Dextrose gel for neonatal hypoglycaemia (the Sugar Babies Study): a randomised, double-blind, placebo-controlled trial. Lancet, 2013.PMID 24075361
- [4]Edwards T Oral dextrose gel to prevent hypoglycaemia in at-risk neonates. Cochrane Database of Systematic Reviews, 2021.PMID 33998668
- [5]Cornblath M Controversies regarding definition of neonatal hypoglycemia: suggested operational thresholds. Pediatrics, 2000.PMID 10790476
- [6]Adamkin DH Postnatal glucose homeostasis in late-preterm and term infants. Pediatrics, 2011.PMID 21357346
- [7]Thornton PS Recommendations from the Pediatric Endocrine Society for evaluation and management of persistent hypoglycemia in neonates, infants, and children. Journal of Pediatrics, 2015.PMID 25957977
- [8]Harris DL Evaluation of oral dextrose gel for prevention of neonatal hypoglycemia (hPOD): a multicenter, double-blind randomized controlled trial. PLoS Medicine, 2021.PMID 33507929
- [9]Banerjee I Congenital hyperinsulinism in infancy and childhood: challenges, unmet needs and the perspective for the future. Orphanet Journal of Rare Diseases, 2022.PMID 35183224
- [10]Edwards T Oral dextrose gel to prevent hypoglycaemia in at-risk neonates. Cochrane Database of Systematic Reviews, 2023.PMID 38014716