Paeds · fetal-neonatal-and-perinatal
Neonatal jaundice: unconjugated hyperbilirubinaemia
Also known as Neonatal jaundice · Unconjugated hyperbilirubinaemia · Neonatal hyperbilirubinaemia · Physiological jaundice · Breast milk jaundice · Kernicterus
Fellowship guide to neonatal unconjugated hyperbilirubinaemia: bilirubin metabolism and pathophysiology, physiological versus pathological jaundice, hour-specific risk assessment using the Bhutani nomogram, phototherapy and exchange transfusion thresholds from the 2022 AAP guideline, haemolytic causes including ABO and Rh incompatibility and G6PD deficiency, breastfeeding jaundice, acute bilirubin encephalopathy and kernicterus prevention, and regional guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Neonatal jaundice, characterised by a yellow discolouration of the skin and sclerae from elevated bilirubin, is the single most common clinical problem in the newborn period, visible in approximately 60 per cent of term and 80 per cent of preterm infants. Unconjugated hyperbilirubinaemia accounts for the overwhelming majority of cases, arising from an imbalance between bilirubin production and hepatic clearance of this lipid-soluble heme degradation product. While most jaundice is benign and self-limiting, the potential for unconjugated bilirubin to cross the blood-brain barrier and cause irreversible neurological damage makes systematic assessment and risk stratification essential in every newborn. [3]
The clinical task is not merely to detect jaundice but to distinguish the common, benign physiological pattern from the minority of infants whose bilirubin will rise to dangerous levels. The key conceptual framework is that bilirubin toxicity is a function of both the total serum bilirubin concentration and the infant's vulnerability, which is amplified by prematurity, illness, haemolysis, hypoalbuminaemia, and acidosis. The goal of management is to prevent bilirubin from reaching levels at which acute bilirubin encephalopathy and its chronic sequela, kernicterus, can occur. [4]
The 2022 American Academy of Pediatrics guideline revision superseded the 2004 guideline with updated, gestational-age-specific phototherapy and exchange transfusion thresholds, revised risk factor definitions, and an increased emphasis on universal predischarge bilirubin screening with structured follow-up. Despite these advances, kernicterus remains a persistent, largely preventable cause of devastating neurological disability, and cases continue to occur due to failures in recognition, escalation, and follow-up. [2]
Epidemiology & Risk Factors
Visible jaundice occurs in approximately 55 to 60 per cent of term infants and up to 80 per cent of preterm infants during the first week of life. The bilirubin level exceeds 250 micromol per litre in about 5 per cent of term infants and reaches exchange transfusion thresholds in fewer than 1 per 10,000 term infants. Severe hyperbilirubinaemia with bilirubin levels exceeding 425 micromol per litre occurs in approximately 1 per 700 to 1 per 2000 term infants, with higher rates in populations with prevalent G6PD deficiency and haemolytic disorders. [3]
The major risk factors for severe hyperbilirubinaemia cluster into increased bilirubin production and decreased clearance. Predischarge risk assessment should systematically evaluate gestational age less than 38 weeks, jaundice in the first 24 hours, a previous sibling with jaundice requiring phototherapy, exclusive breastfeeding (particularly with inadequate intake or excessive weight loss), macrosomia or infant of a diabetic mother, cephalohaematoma or significant bruising, East Asian ethnicity, and a predischarge TSB or TcB near or above the 95th percentile. [2]
The hour-specific bilirubin nomogram developed by Bhutani and colleagues remains the cornerstone of predischarge risk stratification. In their landmark study of 2840 healthy term and near-term newborns, a predischarge total serum bilirubin in the high-risk zone at or above the 95th percentile predicted subsequent significant hyperbilirubinemia with a sensitivity of approximately 40 per cent and a likelihood ratio of 14, while a low-risk zone value below the 40th percentile had a negative predictive value approaching 100 per cent. [1]
Breastfed infants are at significantly higher risk of both early-onset breastfeeding jaundice, driven by suboptimal intake and caloric deprivation, and late-onset breast milk jaundice, which persists beyond two weeks in up to 30 per cent of predominantly breastfed infants. The natural history study by Maisels and colleagues demonstrated that transcutaneous bilirubin levels remain at or above 85 micromol per litre in approximately 34 per cent of predominantly breastfed infants at four weeks of age, and clinical jaundice persists in 20 to 30 per cent at three to four weeks. [7]
Pathophysiology
Bilirubin is the end product of heme catabolism, produced when senescent red blood cells are broken down by the reticuloendothelial system. Heme oxygenase cleaves the porphyrin ring of heme to produce biliverdin, which is rapidly reduced to unconjugated bilirubin by biliverdin reductase. This unconjugated bilirubin is lipid-soluble, transported in plasma bound to albumin, and delivered to the liver where it must be conjugated by the enzyme uridine diphosphate glucuronosyltransferase 1A1 (UGT1A1) into water-soluble bilirubin glucuronides for excretion in bile. [4]
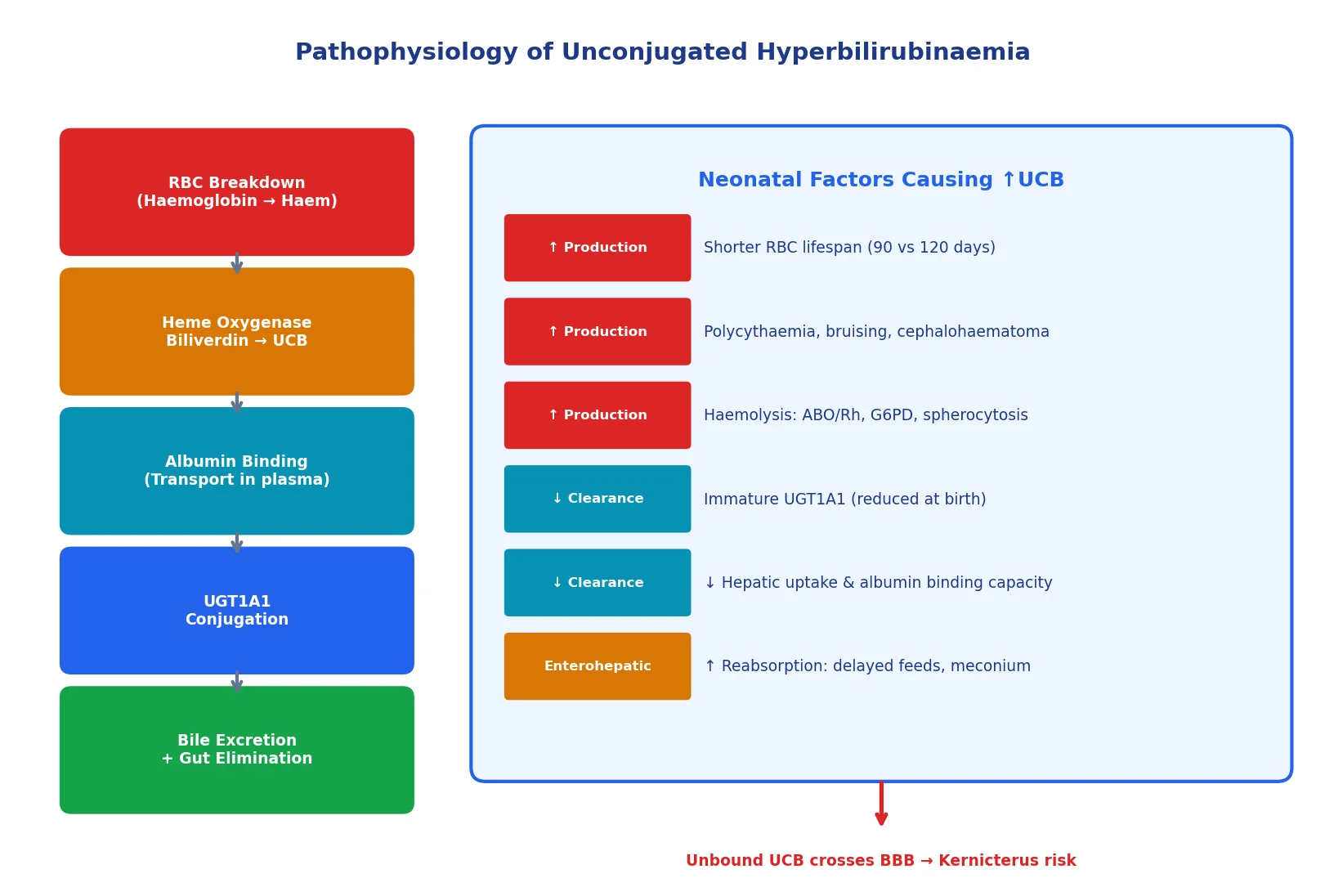
Neonates are uniquely predisposed to unconjugated hyperbilirubinaemia because of several physiological features. Red blood cell lifespan is shorter in neonates at approximately 85 days compared with 120 days in adults, and neonates have a higher red cell mass per kilogram. The hepatic enzyme UGT1A1 activity at birth is less than 1 per cent of adult levels, reaching adequate capacity only after several weeks. Hepatic uptake of bilirubin from plasma is reduced due to low concentrations of the carrier protein ligandin, and increased enterohepatic circulation occurs because the sterile neonatal gut lacks the bacteria that normally reduce conjugated bilirubin to urobilinogen, allowing deconjugation back to unconjugated bilirubin that is reabsorbed. [3]
The neurological danger of unconjugated bilirubin arises from its lipid solubility and ability to cross the blood-brain barrier. When albumin binding capacity is exceeded or when bilirubin is displaced from albumin by competing substances, free unconjugated bilirubin enters neurons and causes mitochondrial dysfunction, oxidative stress, excitotoxicity, and apoptosis. The basal ganglia, cochlear nuclei, hippocampus, and cerebellum are preferentially affected, producing the characteristic clinical and radiological findings of kernicterus. Premature infants are particularly vulnerable because of immature blood-brain barrier integrity, reduced albumin binding capacity, and concurrent illness that potentiates bilirubin toxicity. [4]
Classification
Neonatal jaundice is broadly divided into physiological jaundice, which is a normal developmental phenomenon, and pathological jaundice, which reflects an underlying disorder requiring investigation. Physiological jaundice in term infants appears after 24 hours of age, peaks between days 3 and 5 at levels generally below 250 micromol per litre, and resolves within two weeks. In preterm infants, the peak is higher (below 220 micromol per litre) and later (days 5 to 7), resolving by three weeks. [3]
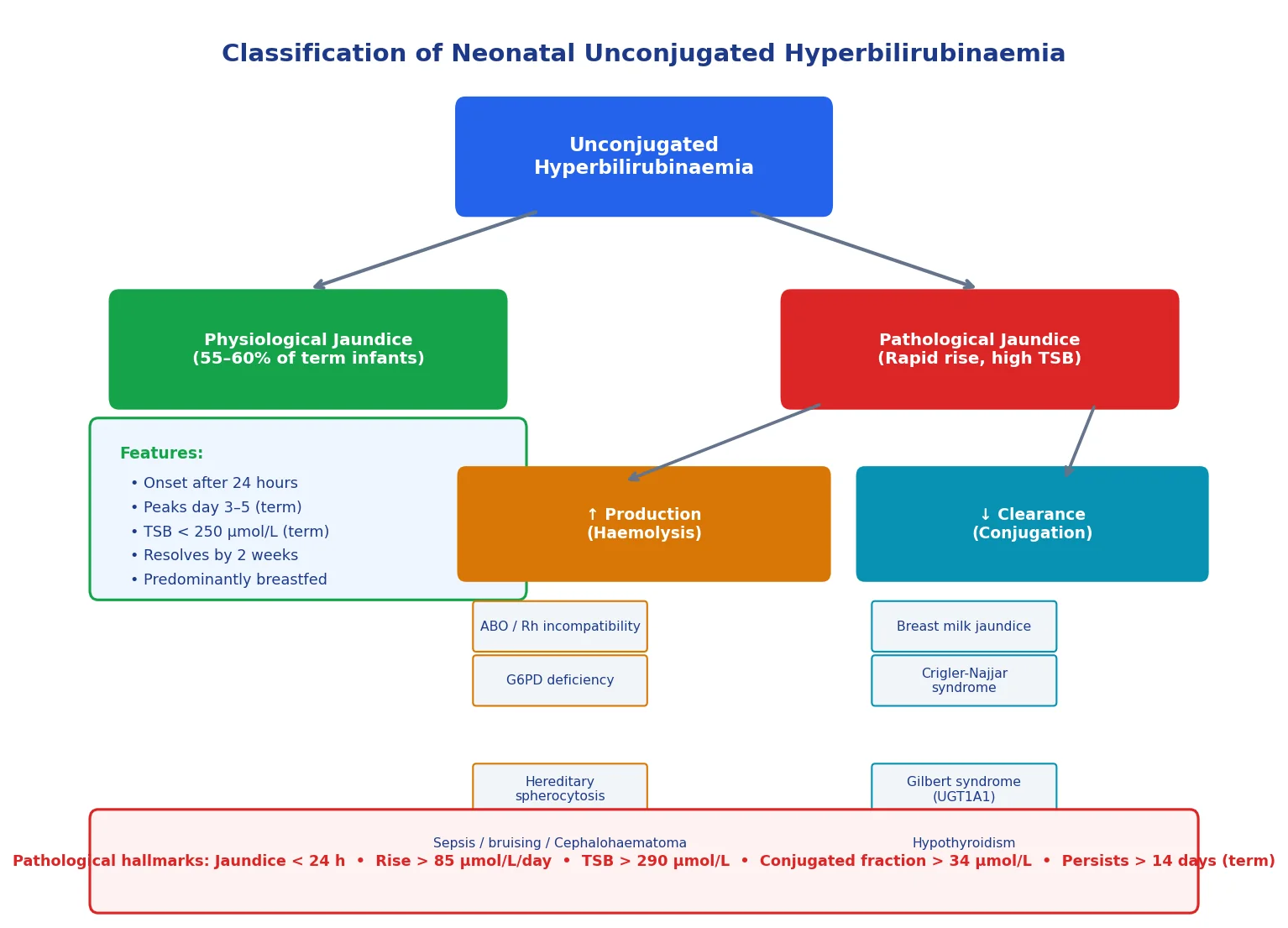
Pathological jaundice is identified by any of the following criteria: jaundice within the first 24 hours of life, a rate of rise exceeding 85 micromol per litre per day, a total serum bilirubin above 290 micromol per litre in a term infant, a conjugated bilirubin fraction exceeding 34 micromol per litre, or clinical jaundice persisting beyond 14 days in a term infant or 21 days in a preterm infant. The pathological causes can be classified mechanistically into increased bilirubin production (haemolysis, bruising, polycythaemia, reabsorption from enclosed haemorrhage) and decreased bilirubin clearance (breast milk jaundice, hypothyroidism, Crigler-Najjar syndrome, Gilbert syndrome, galactosaemia). [2]
Clinical Presentation
The clinical hallmark of neonatal jaundice is the progressive cephalocaudal yellow discolouration of the skin and sclerae. Jaundice typically begins on the face, where a TSB of approximately 85 to 120 micromol per litre produces visible yellowness, and progresses caudally as the bilirubin rises: the trunk yellows at approximately 170 micromol per litre, the lower abdomen and thighs at 200 to 250 micromol per litre, and the palms and soles at levels exceeding 300 micromol per litre. However, this cephalocaudal progression is an imprecise clinical tool, and visual estimation cannot reliably replace a measured bilirubin. [7]
Most infants with unconjugated hyperbilirubinaemia are otherwise clinically well, feeding normally, and growing appropriately. The absence of systemic signs is reassuring but does not exclude dangerous bilirubin levels, particularly in the late-preterm or haemolysing infant whose bilirubin may rise rapidly between observations. Any deviation from wellness, including lethargy, poor feeding, temperature instability, or weight loss exceeding 10 per cent, should heighten concern for pathological jaundice. [3]
The critical clinical presentation to recognise is acute bilirubin encephalopathy, the acute manifestation of bilirubin neurotoxicity. Early signs include lethargy, hypotonia, poor suck, and a high-pitched cry, which are subtle and easily missed. Progression brings hypertonia, especially with retrocollis and opisthotonos, fever, irritability, and seizures. In the chronic phase known as kernicterus, the child develops athetoid cerebral palsy, sensorineural hearing loss, gaze palsies (especially upward gaze palsy), and intellectual disability. [4]
Cephalocaudal progression by approximate TSB
Face and sclerae: TSB ~85-120 µmol/L (5-7 mg/dL)
Trunk: TSB ~170 µmol/L (10 mg/dL)
Lower abdomen and thighs: TSB ~200-250 µmol/L (12-15 mg/dL)
Arms and lower legs: TSB ~255-290 µmol/L (15-17 mg/dL)
Palms and soles: TSB above 300 µmol/L (above 18 mg/dL)
Differential Diagnosis
The primary task when evaluating a jaundiced neonate is to determine whether the hyperbilirubinaemia is unconjugated (indirect-reacting) or conjugated (direct-reacting). This single distinction transforms the differential diagnosis and the urgency of management. Conjugated hyperbilirubinaemia, defined as a direct fraction above 34 micromol per litre or above 20 per cent of total bilirubin, is always pathological and mandates urgent investigation for biliary atresia, neonatal hepatitis, sepsis, metabolic disease, and TORCH infections. Pale or acholic stools are the cardinal sign of conjugated hyperbilirubinaemia. [3]
For unconjugated hyperbilirubinaemia, the major differential categories are haemolytic disease, breast milk jaundice, sepsis, bruising or enclosed haemorrhage, polycythaemia, hypothyroidism, and inherited conjugation disorders. The most common haemolytic causes are ABO incompatibility, Rh (D) disease (now rare with anti-D prophylaxis), G6PD deficiency, hereditary spherocytosis, and pyruvate kinase deficiency. Sepsis may present with jaundice as the sole sign, though this is more typical of late-onset infection. [9]
Crigler-Najjar syndrome type 1 is a rare but critical cause of severe unconjugated hyperbilirubinaemia, caused by complete absence of UGT1A1 activity, and typically presents with bilirubin levels above 340 micromol per litre in the first days of life that are refractory to phototherapy. Gilbert syndrome, caused by a reduced-expression UGT1A1 promoter polymorphism, is a benign condition that may contribute to prolonged jaundice but does not cause severe hyperbilirubinaemia alone. [4]
Clinical & Bedside Assessment
Every newborn should be assessed for jaundice at every examination during the birth hospitalisation and at follow-up visits. Visual assessment should be performed in good light, preferably natural daylight, by blanching the skin with gentle pressure on a bony prominence and observing the underlying colour. Begin at the face and progress caudally, as the cephalocaudal progression correlates approximately with bilirubin level. However, visual estimation is imprecise and systematically underestimates bilirubin in darker-pigmented infants, so any visible jaundice in the first 24 hours mandates a measured bilirubin. [2]
Transcutaneous bilirubin (TcB) measurement is a useful, non-invasive screening tool that correlates well with total serum bilirubin for values below 250 micromol per litre, and its use reduces the need for blood sampling. However, TcB becomes less reliable at higher levels and after phototherapy has been initiated, so a TcB value within 50 micromol per litre of the phototherapy threshold or any value above 250 micromol per litre should be confirmed with a total serum bilirubin measurement. [2]
The predischarge risk assessment combines the bilirubin level plotted on an hour-specific nomogram with clinical risk factors. The 2022 AAP guideline recommends universal predischarge bilirubin screening (TSB or TcB) for all infants of 35 weeks gestation or more, combined with assessment of risk factors including gestational age, haemolysis risk, exclusive breastfeeding, previous sibling with jaundice, cephalohaematoma or bruising, and maternal age above 25 years. The result guides the timing and intensity of follow-up. [2]
Investigations
The total serum bilirubin (TSB) with fractionation into unconjugated (indirect) and conjugated (direct) components is the essential investigation. The TSB must be interpreted in the context of the infant's postnatal age in hours and gestational age, and plotted on the hour-specific percentile nomogram. In infants requiring phototherapy or exchange transfusion, repeat TSB should be measured at appropriate intervals: every 4 to 6 hours during intensive phototherapy and immediately before any exchange transfusion decision. [2]
The haemolytic workup should be performed when there is a rapid rate of rise, early-onset jaundice, significant anaemia, a positive family history, or an infant whose mother is Rh negative or blood group O. The direct antiglobulin test (DAT, also known as direct Coombs test) detects antibody or complement coating the infant's red cells and is the primary screen for immune-mediated haemolysis. A peripheral blood film assesses for spherocytes (suggestive of ABO incompatibility or hereditary spherocytosis), fragmented cells, and red cell morphology. A full blood count with reticulocyte count identifies anaemia and the compensatory erythropoietic response. [3]
G6PD deficiency screening should be considered in at-risk populations, including infants of Mediterranean, African, Middle Eastern, South Asian, Southeast Asian, or Oceanian heritage, particularly when jaundice is severe or unexpected. It is important to note that a G6PD assay performed during an acute haemolytic episode may be falsely normal because the most enzyme-deficient cells have been lysed, and the assay should be repeated after recovery. Maternal and infant blood group and Rh status should always be documented. [9]
Additional investigations are guided by the clinical picture. Thyroid function testing (newborn bloodspot screening) excludes congenital hypothyroidism, a rare but treatable cause of prolonged jaundice. Septic workup (blood culture, urine culture, CRP) is warranted if the infant appears unwell or if infection is suspected, since late-onset sepsis can present with jaundice as the sole sign. Urine reducing substances assess for galactosaemia in the jaundiced infant with hepatomegaly. [3]
Management - Resuscitation
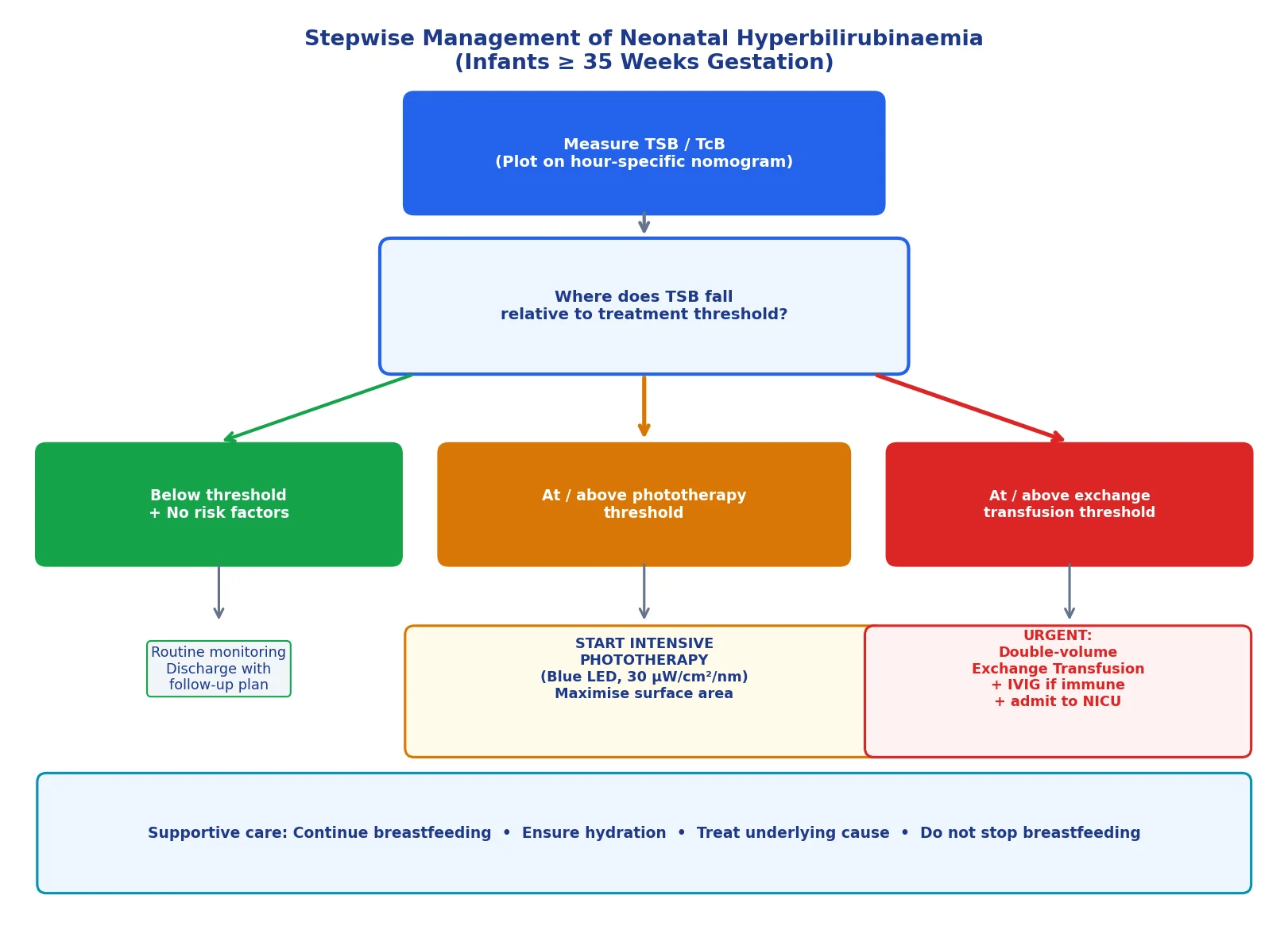
An infant presenting with severe hyperbilirubinaemia at or near the exchange transfusion threshold requires immediate intervention. The priority is to initiate intensive phototherapy without delay while preparing for potential exchange transfusion if the bilirubin does not respond. Place the infant under high-intensity blue LED phototherapy with maximal skin surface exposure, using a reflective blanket or additional lights underneath to increase the irradiated surface area to approximately 80 to 90 per cent of the total body surface area. [2]
Ensure adequate hydration and caloric intake, as dehydration and poor feeding worsen hyperbilirubinaemia by increasing enterohepatic circulation. Continue breastfeeding wherever possible; supplementation with expressed breast milk or formula may be needed if intake is inadequate. Intravenous fluids should be reserved for infants who are dehydrated or unable to feed, as routine supplemental IV fluids do not improve bilirubin clearance and may separate mother and infant. [2]
For the infant with clinical signs of acute bilirubin encephalopathy or a bilirubin level at or above the exchange transfusion threshold, proceed to double-volume exchange transfusion as an emergency. The exchange should use blood cross-matched against both the infant and mother, reconstituted to a haematocrit of approximately 40 to 50 per cent. Intravenous immunoglobulin (IVIG) at 0.5 to 1 g per kg over 2 hours can reduce the need for exchange transfusion in immune-mediated haemolysis when the bilirubin is rising despite intensive phototherapy. [3]
Management - Definitive & Stepwise
The 2022 AAP guideline introduced a new framework using three threshold lines — phototherapy, exchange transfusion, and a discontinue phototherapy line — plotted on gestational-age-specific charts for infants of 35 weeks or more gestation. The thresholds are now presented as graphs rather than a single table, with separate curves for infants at higher risk (neurotoxicity risk factors: gestational age less than 38 weeks, albumin below 3 g per dL, instability, or significant haemolysis) and lower risk (term, well, no haemolysis). [2]
Phototherapy is the first-line treatment for moderate to severe hyperbilirubinaemia and works by converting bilirubin in the skin into water-soluble photoisomers that can be excreted in bile and urine without conjugation. Effective phototherapy requires light in the blue-green spectrum (430 to 490 nm), sufficient irradiance (at least 30 microwatts per square centimetre per nanometre), and maximal skin exposure. The eyes must be protected with opaque patches to prevent retinal damage, and the temperature should be monitored to prevent hypothermia or hyperthermia. The response to phototherapy is typically a bilirubin decline of 17 to 34 micromol per litre within the first 4 to 6 hours. [8]
Phototherapy delivery checklist
Confirm TSB meets threshold for gestational age and risk group
Use blue LED light at 430-490 nm with irradiance above 30 µW/cm²/nm
Expose maximal skin surface area (80-90 per cent), use reflective blanket
Protect eyes with opaque patches; monitor temperature
Ensure adequate hydration; continue breastfeeding
Check TSB at 4-6 hours; assess rate of decline
Discontinue when TSB is below the gestational-age-specific threshold
The number needed to treat with phototherapy varies enormously depending on the infant's characteristics. Newman and colleagues demonstrated that phototherapy is highly effective overall (adjusted odds ratio 0.16 for preventing exchange transfusion) but the NNT ranges from as low as 10 for a less-than-24-hour-old, 36-week boy to over 3000 for a three-day-old, 41-week girl. This underscores the importance of targeting phototherapy to infants most likely to benefit, as specified in the guideline thresholds. [8]
Exchange transfusion is indicated when the TSB reaches the exchange transfusion threshold for the infant's gestational age and risk profile, or when intensive phototherapy fails to halt a rapid rise. The procedure involves removing and replacing approximately twice the infant's blood volume (160 to 180 mL per kg) with donor red cells, and it reduces the bilirubin by approximately 50 per cent. Complications include thrombocytopenia, hypoglycaemia, hypocalcaemia, acidosis, necrotising enterocolitis, and catheter-related complications, making it a procedure of last resort that should be performed in a tertiary neonatal unit. [3]
BILI-RUBIN approach to management
Specific Subtypes & Scenarios
ABO incompatibility is the most common cause of immune haemolytic neonatal jaundice, occurring when the mother has blood group O and the infant has blood group A or B. Unlike Rh disease, ABO incompatibility can affect the first pregnancy because anti-A and anti-B antibodies are naturally occurring. The DAT may be positive but is often weakly or falsely negative, and the peripheral film typically shows spherocytes. The condition is usually mild to moderate, but severe cases requiring exchange transfusion do occur. [3]
Rh (D) haemolytic disease, once the leading cause of severe neonatal hyperbilirubinaemia and kernicterus, has become rare in countries with universal antenatal anti-D prophylaxis. However, it should be considered in any infant born to an Rh-negative mother who is not immunised, or in settings where anti-D prophylaxis is incomplete. Rh disease typically worsens with successive pregnancies, presents with early and severe anaemia and jaundice, and may cause hydrops fetalis in extreme cases. [3]
G6PD deficiency is the most common inherited enzyme deficiency worldwide and a major cause of severe neonatal hyperbilirubinaemia. Infants with G6PD deficiency are approximately four times more likely to develop significant hyperbilirubinemia than those without, and the hyperbilirubinaemia can be sudden and unpredictable due to episodic haemolysis triggered by oxidative stressors. Up to 20 per cent of kernicterus cases in registry data involve G6PD-deficient infants. The pathophysiology is not purely haemolytic — impaired bilirubin conjugation through UGT1A1 promoter polymorphisms (Gilbert syndrome) interacting with G6PD deficiency plays an important role. Screening should be performed in high-prevalence populations including those of African, Mediterranean, Middle Eastern, and Asian heritage. [9]
Breast milk jaundice affects up to 30 per cent of breastfed infants and is characterised by prolonged unconjugated hyperbilirubinaemia persisting beyond the second week. The proposed mechanism involves factors in breast milk, particularly beta-glucuronidase, that increase enterohepatic circulation by deconjugating bilirubin in the gut. It is a diagnosis of exclusion, made only after pathological causes have been ruled out, and the management is continued breastfeeding. A 12 to 24 hour temporary interruption of breastfeeding with a diagnostic rise in bilirubin confirming the diagnosis is now considered unnecessary and counterproductive. [7]
Prolonged jaundice, defined as clinical jaundice persisting beyond 14 days in a term infant or 21 days in a preterm infant, requires systematic evaluation. The first step is to fractionate the bilirubin. If unconjugated, evaluate for breast milk jaundice, hypothyroidism (check bloodspot screen), G6PD deficiency, and occult infection. If conjugated, urgent referral for evaluation of biliary atresia is mandatory, as the Kasai procedure has a critical time window of less than 60 days. [3]
[9]Complications & Pitfalls
The most devastating complication of severe unconjugated hyperbilirubinaemia is bilirubin-induced neurologic dysfunction (BIND), which ranges from subtle neurodevelopmental impairment to the full clinical syndrome of kernicterus. Acute bilirubin encephalopathy presents in three phases: early (lethargy, hypotonia, poor suck, high-pitched cry), intermediate (hypertonia, fever, retrocollis, opisthotonos, irritability), and advanced (apnoea, seizures, coma). Infants who survive the acute phase may develop chronic kernicterus with athetoid cerebral palsy, sensorineural hearing loss, upward gaze palsy, dental enamel dysplasia, and cognitive impairment. [4]
Preterm infants are at particularly high risk of bilirubin neurotoxicity, and acute bilirubin encephalopathy in this population may manifest subtly, sometimes presenting primarily as recurrent apnoeic events. Low-bilirubin kernicterus continues to be reported in preterm neonates and is often associated with marked hypoalbuminaemia, emphasising that total bilirubin levels alone do not define risk in this population. Multiple cellular and molecular cascades underlie bilirubin-induced neuronal injury, including plasma membrane perturbations, excitotoxicity, neuroinflammation, oxidative stress, and cell cycle arrest. [5]
Major clinical pitfalls include relying on visual estimation rather than a measured bilirubin, particularly in darker-pigmented infants where jaundice is systematically underestimated; failing to recognise jaundice within the first 24 hours as always pathological; not plotting the bilirubin on an hour-specific nomogram; using inappropriate phototherapy thresholds for gestational age or risk group; and discharging an at-risk infant without adequate follow-up arrangements. Additional traps include treating prolonged unconjugated jaundice without checking the conjugated fraction (missing biliary atresia), stopping breastfeeding unnecessarily, and failing to perform G6PD screening in at-risk populations. [3]
Prognosis & Disposition
Most infants with unconjugated hyperbilirubinaemia have an excellent prognosis with full resolution and no long-term sequelae. The key determinant of outcome is whether the bilirubin is identified and treated before it reaches neurotoxic levels. Infants treated with phototherapy alone, who respond appropriately and have no neurological signs at presentation, recover completely without sequelae. [3]
The prognosis after acute bilirubin encephalopathy is guarded. Infants who receive exchange transfusion during the early phase may recover with minimal or no sequelae, but those who progress to the intermediate or advanced phase have a high probability of chronic kernicterus with athetoid cerebral palsy, deafness, and developmental disability. Long-term follow-up studies confirm that bilirubin-induced neurological damage is largely irreversible, making prevention the only effective strategy. [4]
Disposition decisions depend on the severity of hyperbilirubinaemia and the response to treatment. Infants whose bilirubin is below the phototherapy threshold can be managed with monitoring and appropriate follow-up. Those started on phototherapy should have TSB repeated at 4 to 6 hours to confirm a response, and phototherapy can be discontinued once the bilirubin is below the gestational-age-specific discontinuation threshold, with a rebound check 12 to 24 hours after cessation. Infants requiring exchange transfusion or those with acute bilirubin encephalopathy require NICU admission and long-term developmental follow-up including audiology assessment. [2]
Special Populations
Preterm infants of less than 35 weeks gestation are managed with different, lower thresholds than term infants because of their increased vulnerability to bilirubin neurotoxicity. The 2012 consensus approach by Maisels and colleagues provides operational thresholds for this population based on expert opinion rather than high-quality evidence. For infants at 28 to 34 weeks gestation, phototherapy is typically initiated at bilirubin levels of 120 to 170 micromol per litre and exchange transfusion at 220 to 270 micromol per litre, adjusted for gestational age and clinical status. These thresholds are consensus-based and individualised to the infant's clinical condition. [6]
Infants with G6PD deficiency require special attention due to the risk of sudden, unpredictable haemolytic crises that can precipitate exponential bilirubin rises. Parents of G6PD-deficient infants should receive education about avoiding known oxidative triggers including fava beans, naphthalene (mothballs), henna, certain medications (sulphonamides, primaquine, nitrofurantoin), and infections. These infants require close monitoring during any intercurrent illness and rapid response to any rising bilirubin. [9]
In Indigenous and migrant populations across Australia and New Zealand, higher rates of G6PD deficiency, later presentation to health services, and cultural and linguistic barriers to follow-up all contribute to increased risk of severe hyperbilirubinaemia and kernicterus. Culturally safe care, interpreter access, and clear discharge communication with a documented follow-up plan are essential. In low- and middle-income countries, limited access to phototherapy, blood for exchange transfusion, and laboratory testing, combined with higher rates of G6PD deficiency and sepsis, dramatically increase the incidence of kernicterus. [9]
[9]Evidence, Guidelines & Regional Differences
The 2022 AAP clinical practice guideline revision represents the most significant update in neonatal hyperbilirubinaemia management since 2004. It replaced the categorical risk zones of the 2004 guideline with continuous gestational-age-specific threshold curves, introduced a neurotoxicity risk modifier (higher versus lower risk), lowered phototherapy thresholds for lower-risk infants to reduce readmissions while maintaining safety, and provided clear discontinuation thresholds. This approach has been shown to safely reduce the number of infants requiring phototherapy while ensuring that high-risk infants receive timely treatment. [2]
The 2004 AAP guideline, now superseded, established the framework of universal predischarge bilirubin screening, hour-specific nomogram-based risk assessment, and structured follow-up. It was instrumental in raising awareness that kernicterus remained a preventable problem and in standardising risk assessment across centres. The key elements — universal screening, systematic assessment, and targeted follow-up — remain embedded in the 2022 revision. [3]
[2]Controversies and active research areas include the role of automated free bilirubin measurement as a more accurate predictor of neurotoxicity than total bilirubin, the appropriate thresholds for preterm infants below 35 weeks, whether home phototherapy is safe and effective for selected infants, the long-term neurodevelopmental outcomes of infants treated at the revised 2022 thresholds, and the development of pharmacological agents to enhance bilirubin conjugation (such as tin mesoporphyrin) as alternatives to phototherapy. The interaction between genetic polymorphisms (UGT1A1, G6PD, SLCO genes) and environmental factors in determining hyperbilirubinaemia severity is an active area of investigation. [4]
Exam Pearls
KERNICTERUS prevention
References
- [1]Bhutani VK Predictive ability of a predischarge hour-specific serum bilirubin for subsequent significant hyperbilirubinemia in healthy term and near-term newborns. Pediatrics, 1999.PMID 9917432
- [2]Kemper AR Clinical Practice Guideline Revision: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation. Pediatrics, 2022.PMID 35927462
- [3]American Academy of Pediatrics Subcommittee on Hyperbilirubinemia Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics, 2004.PMID 15231951
- [4]Watchko JF Bilirubin-induced neurologic damage--mechanisms and management approaches. N Engl J Med, 2013.PMID 24256380
- [5]Watchko JF Bilirubin-Induced Neurotoxicity in the Preterm Neonate. Clin Perinatol, 2016.PMID 27235209
- [6]Maisels MJ An approach to the management of hyperbilirubinemia in the preterm infant less than 35 weeks of gestation. J Perinatol, 2012.PMID 22678141
- [7]Maisels MJ The natural history of jaundice in predominantly breastfed infants. Pediatrics, 2014.PMID 25049352
- [8]Newman TB Numbers needed to treat with phototherapy according to American Academy of Pediatrics guidelines. Pediatrics, 2009.PMID 19403502
- [9]Kaplan M Glucose-6-phosphate dehydrogenase deficiency and severe neonatal hyperbilirubinemia: a complexity of interactions between genes and environment. Semin Fetal Neonatal Med, 2010.PMID 19942489