Paeds · fetal-neonatal-and-perinatal
Neonatal pain assessment and procedural comfort
Also known as Neonatal pain assessment and procedural comfort · Neonatal procedural pain management · Neonatal analgesia and comfort care · Pain assessment in the newborn · Sucrose and non-pharmacological analgesia in neonates
Fellowship guide to neonatal pain assessment and procedural comfort: the neuroscience proving neonates feel pain (Slater EEG, Goksan fMRI), the hyper-excitable preterm brain, the validated pain scores (PIPP/PIPP-R, N-PASS, NFCS, CRIES), and the stepwise comfort ladder from environmental measures through sucrose, breast milk, topical anaesthesia, paracetamol and titrated opioids.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A two-day-old preterm infant grimaces, desaturates and goes rigid the moment the heel-lance device fires. That response is pain. Until the 1980s the dogma held that the immature brain could not feel pain, and neonatal surgery was performed with little or no analgesia; modern neuroscience has refuted that dogma completely, and neonatal pain assessment is now a core standard of care in every nursery and intensive care unit. [1] [8]
Neonatal pain is the subjective sensory and emotional experience of a noxious event in an infant who cannot report it. At the bedside the clinician works with two linked ideas: nociception, the neural processing of a damaging stimulus, and pain, the experience it produces. Because the neonate cannot speak, both are operationally bundled and inferred from behaviour, physiology and context, and graded with a validated score. The task is to recognise the pain, match the comfort to the procedure, and prove the treatment worked by re-scoring. [1]
Classification
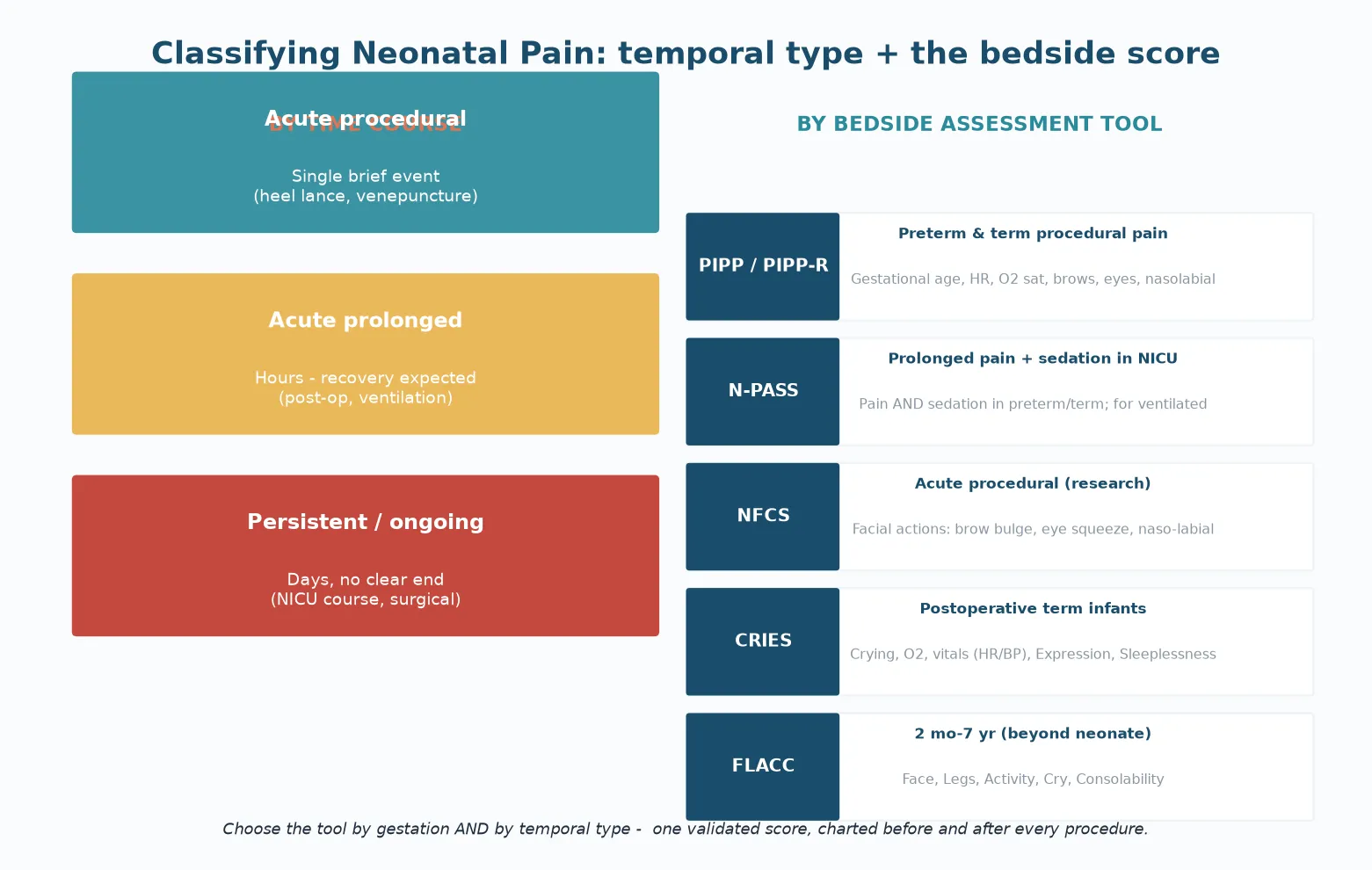
Pain in a newborn sorts first by how long it lasts, because duration decides whether a brief bolus of comfort is enough or whether a sustained strategy is needed. The temporal classes are acute procedural pain - a single brief event such as a heel lance or venepuncture - acute prolonged pain, which runs over hours with an expected recovery, such as postoperative pain or the discomfort of ventilation, and persistent or ongoing pain, which stretches over days without a clear end, such as a prolonged intensive-care course. [1]
The second axis is the bedside score, because each tool was built for a specific gestation and a specific temporal class. The Premature Infant Pain Profile and its revised form (PIPP and PIPP-R) combine gestational age, behavioural state, heart-rate change, oxygen-saturation change, brow bulge, eye squeeze and the nasolabial furrow, and serve preterm and term procedural pain. The Neonatal Pain, Agitation and Sedation Scale (N-PASS) scores both pain and sedation in ventilated preterm and term infants over a prolonged course. NFCS, a facial-action coding system, is used mainly in research. CRIES serves postoperative term infants. FLACC belongs to the older infant beyond the neonatal period. [2]
Epidemiology & Risk Factors
A sick or preterm neonate in the intensive-care unit is exposed to many painful procedures every day, most of them minor bedside events such as heel lancing, suctioning and intravenous cannulation. Across the first weeks of a preterm admission the cumulative number of these procedures reaches into the hundreds, and the sheer frequency of exposure is itself the central epidemiological fact of neonatal pain. [1]
The infants who undergo the most procedures are also those least equipped to recover from them. The extremely preterm infant, the infant on prolonged ventilation, and the surgical infant carry both the highest procedural burden and the greatest vulnerability to its long-term neurological consequences. Under-treatment remains common, and the quality standard that closes the gap is a documented pain score taken before and after every procedure. [1] [3]
Pathophysiology
The nociceptive system is built early, and that early maturation is the whole reason the neonate feels pain at all. Free nerve endings appear in the skin by six to eight weeks' gestation, the spinothalamic tract begins to myelinate around twenty weeks, thalamo-cortical connections form between twenty-four and thirty weeks, and a functional cortical pain response is present by term. The pathways that carry a noxious signal to consciousness are therefore working before a preterm infant is even viable. [7]
What makes the preterm brain special is its balance of excitation and inhibition. Excitatory glutamatergic transmission is predominant early, while the descending GABAergic and brainstem inhibitory modulation that damps a pain signal in the mature brain is immature. A preterm infant therefore does not feel less pain - the preterm infant feels more pain per stimulus, with a lower threshold and a longer recovery. This is why the smallest infant is the most vulnerable, not the most protected. [7] [8]
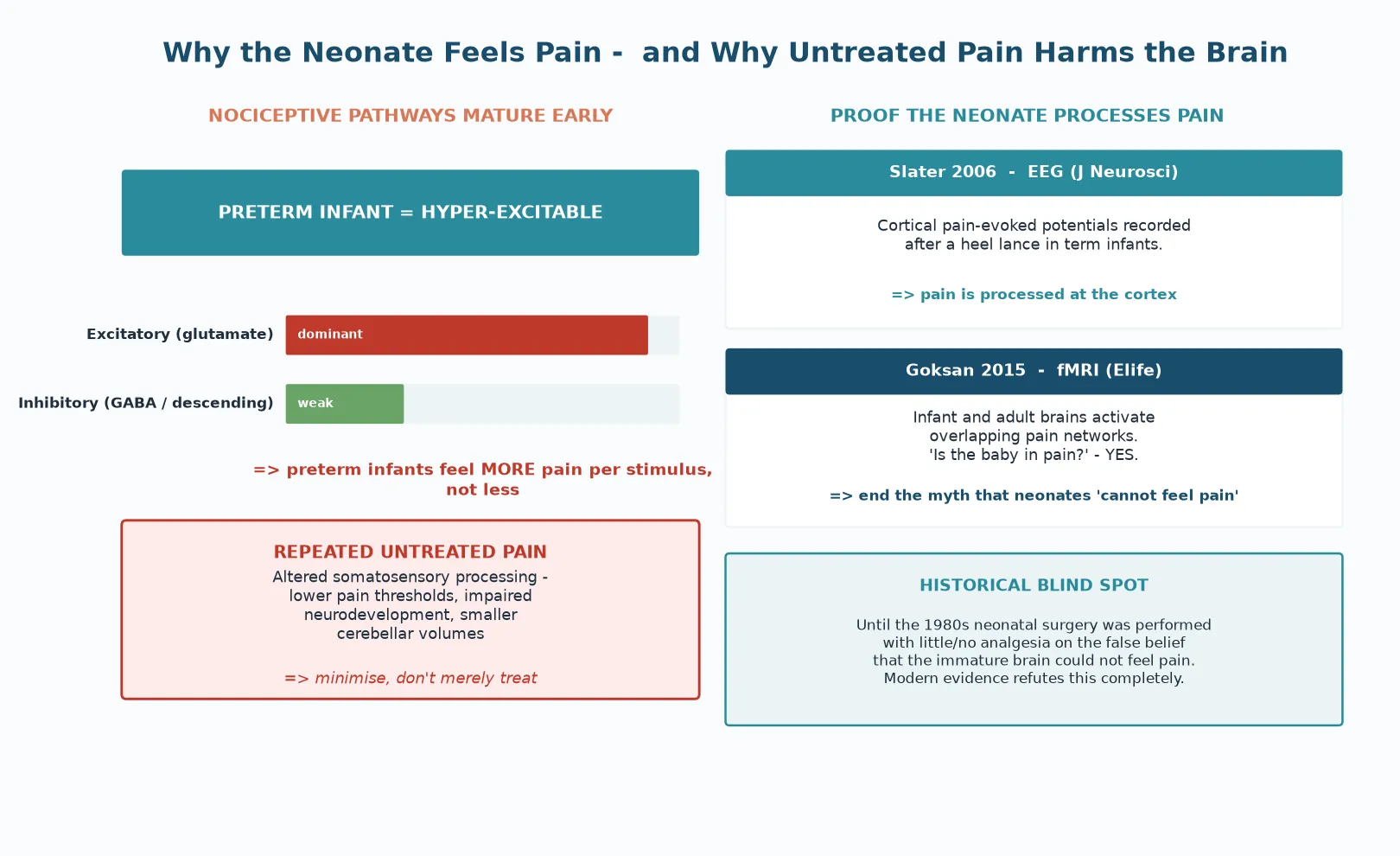
The modern proof that neonates process pain is direct and cortical. Slater and colleagues recorded pain-evoked potentials over the infant cortex after a heel lance, confirming that a noxious stimulus is processed at the level of the brain and not merely as a spinal reflex. Goksan and colleagues then used functional MRI to show that the brain networks activated by pain in infants overlap substantially with those activated in adults - ending, in the authors' words, the assumption that infant pain differs fundamentally from adult pain. [7] [8]
The harm of repeated untreated pain is not theoretical. Sustained exposure to unrelieved procedural pain in the preterm period alters later somatosensory processing, lowers pain thresholds, and is associated with impaired neurodevelopmental outcome and altered brain structure. This is the neurodevelopmental case for the comfort ladder: pain is not merely an acute discomfort to be smoothed over, but an avoidable insult to a developing brain. [1]
Clinical Presentation
Pain in a neonate declares itself through behaviour, physiology and context, and the clinician reads all three together. The behavioural cues are crying or a grimace, the facial actions of brow bulge, eye squeeze and the deepened nasolabial furrow, limb withdrawal or body posturing, sleep disturbance, and a reduced ability to be consoled. The physiological cues are a racing or plunging heart rate, an oxygen desaturation, blood-pressure lability, pallor or mottling, and a change in the breathing pattern. [2]
The context is the third clue and often the most decisive. An infant who becomes suddenly more agitated or harder to settle immediately after a procedure, a line change, or an environmental disturbance is in pain until the score proves otherwise. The temporal link between an event and a change in the infant is the bedside signal that triggers scoring rather than a default assumption of hunger or sepsis. [1]
Differential Diagnosis
Not every cry in a neonate is pain, and the trap is to treat agitation as pain without considering the alternatives. Hunger produces crying that resolves with feeding and a normal examination, with no temporal link to a procedure. Sepsis or necrotising enterocolitis produce abnormal vital signs, abdominal signs, feeding intolerance and raised inflammatory markers, and they are excluded with the appropriate screen rather than an extra dose of sucrose. [1]
Neonatal abstinence syndrome can mimic pain with autonomic and gastrointestinal dysregulation, but its timing follows maternal opioid exposure and it is measured with a withdrawal-specific score rather than a pain tool. Hypoglycaemia, electrolyte disturbance, a full or soiled nappy, and overstimulation from an uncontrolled, brightly lit, noisy environment each produce distress that resolves when the cause is addressed. The discipline is to score the pain, treat it, and still run the differential - because sucrose given for sepsis is a delayed diagnosis wearing the disguise of comfort. [1]
[1]Clinical & Bedside Assessment
Bedside assessment is the act that turns a suspicion of pain into a measured, treatable number. The clinician identifies whether a procedure or clinical change has just occurred, observes the behavioural and physiological cues, and scores the pain with a validated tool chosen for the gestation and the temporal type. The score is documented before the procedure and again after the comfort intervention, so that the response to treatment is provable rather than assumed. [2]
The Premature Infant Pain Profile, developed and validated by Stevens and colleagues, combines three contextual factors - gestational age, behavioural state before the stimulus - with a heart-rate change and an oxygen-saturation change, and three facial actions: brow bulge, eye squeeze and the nasolabial furrow. The revised PIPP-R adjusts the scoring of the sleeping or awake state so that a sleeping infant is not falsely scored as pain-free. PIPP and PIPP-R are the workhorse tools for procedural pain in preterm and term infants. [2]
The Neonatal Pain, Agitation and Sedation Scale (N-PASS) answers a different question - how much pain or sedation does a ventilated infant have over a prolonged course? It scores both pain and sedation across five domains: crying or irritability, behavioural state, facial expression, extremities and tone, and vital signs, with adjustments for prematurity. N-PASS suits the infant on a prolonged intensive-care course where the goal is to balance adequate analgesia against over-sedation. [2]
Across Australia, New Zealand and the United Kingdom, PIPP or PIPP-R is preferred for procedural pain in preterm and term infants, N-PASS is preferred for prolonged pain and sedation in the ventilated NICU infant, CRIES is used for postoperative term infants, and FLACC is reserved for the older infant beyond the neonatal period. NFCS remains primarily a research tool. The unifying rule is that one validated score is chosen for the patient, charted before and after every procedure, and used to drive the comfort decision. [1] [2]
Investigations
Pain in a neonate is a clinical diagnosis, and there is no blood test or imaging study that confirms or excludes it. Heart rate and oxygen saturation are supporting cues read inside the validated score, not laboratory measurements that stand alone. The clinician who understands this resists the reflex to 'investigate the pain' and instead measures it with the tool and treats it. [1]
Objective measures of neonatal pain do exist, but they live in research rather than at the bedside. Cortical electroencephalography and pain-evoked potentials, skin-conductance algometry, and salivary cortisol each capture a facet of the nociceptive response, and they underpin the neuroscience. None has displaced the bedside score for routine use, because each is harder to deploy, slower to interpret, and less directly actionable in a busy nursery. [7] [8]
When a pain score stays abnormal despite adequate comfort, the investigation is directed at the cause, not at the pain. The search is for sepsis, necrotising enterocolitis, a blocked or infiltrated vascular line, a full bladder, a surgical complication, or a metabolic derangement. A persistent score is a signal to find and fix the source of the ongoing noxious stimulus. [1]
Management - Resuscitation
The first move in neonatal pain management is to do no harm, and that means reducing the number of times the infant is hurt in the first place. Procedures are clustered so that handling is bundled rather than repeated, the environment is kept calm with low light and low noise, and a stable infant is not woken for a non-urgent test. Every procedure that is avoided is a pain episode that never happens. [1] [6]
Before any planned procedure, an immediate comfort bundle is applied. The infant is contained and supported with facilitated tucking or swaddling, offered non-nutritive sucking, and held skin-to-skin where feasible. A validated pain score is taken before the procedure and again after, and the documented score drives whether further analgesia is required. This bundle is the resuscitation of neonatal pain - it is applied first, fast, and to every infant. [6]
Immediate comfort bundle before a procedure
Minimise: cluster cares; avoid waking a stable infant for a non-urgent procedure
Calm the environment: low light, low noise, containment
Position: facilitated tucking or swaddling
Offer non-nutritive sucking; skin-to-skin where feasible
Score the pain (PIPP-R / N-PASS) before the procedure
Give sucrose or breast milk 2 min before a brief painful procedure
Re-score after the procedure; document the response
Management - Definitive & Stepwise
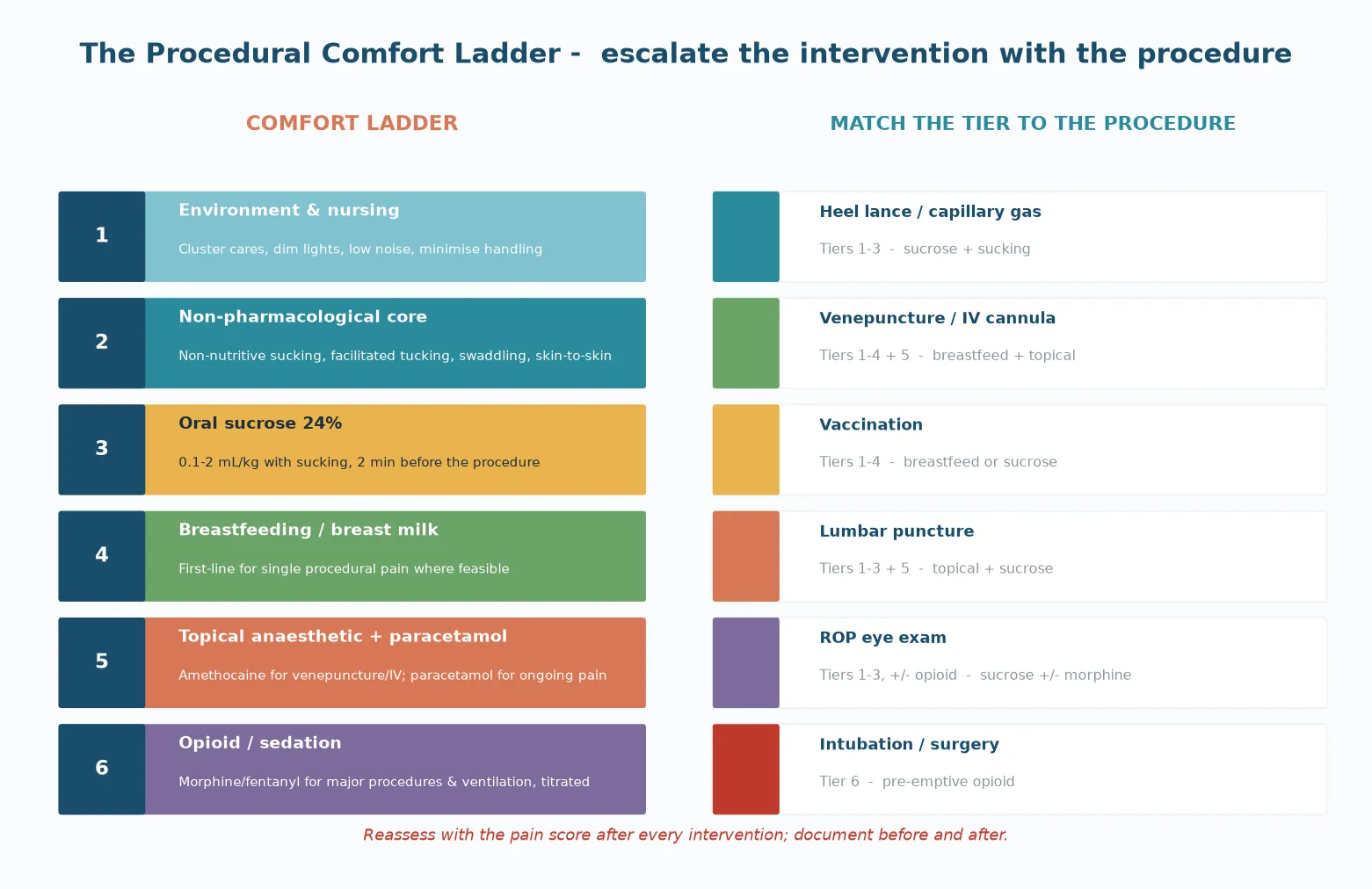
Definitive management is a ladder, and the clinician climbs it as far as the procedure demands. The base is the environmental and nursing layer; the non-pharmacological core of sucking, tucking, swaddling and skin-to-skin sits above it; oral sucrose and breast milk form the next tier for brief procedural pain; topical anaesthesia and paracetamol serve sustained pain; and opioids are reserved for major procedures, surgery and ventilation. Each tier is matched to the procedure, and each intervention is checked with a re-score. [4] [6]
Oral sucrose is the best-evidenced sweet-taste analgesic for brief procedural pain. The regimen is 24% sucrose at 0.1 to 2 mL total (not per kg; size-adjusted, max ~2 mL) given by mouth together with non-nutritive sucking approximately two minutes before the procedure. The Stevens 2016 Cochrane review confirmed that sucrose reduces behavioural pain indicators during single brief procedures, and the Gibbins 2002 study established its efficacy and safety in both preterm and term neonates. Sucrose is for procedural pain, and it is not a substitute for opioid analgesia when the pain is major. [4] [9]
Breastfeeding or expressed breast milk is now first-line analgesia for single procedural pain such as venepuncture or vaccination where breastfeeding is feasible. The Shah 2023 Cochrane review confirmed that breast milk reduces procedural pain behaviours, and it carries the additional benefit of maternal presence and the non-pharmacological effect of sucking. Where breastfeeding is not possible, sucrose with non-nutritive sucking is the standard alternative. [5]
Oral sucrose 24%
Dose
0.1–2 mL total (size-adjusted, max ~2 mL)
Topical anaesthesia with amethocaine (Ametop) or eutectic lidocaine-prilocaine (EMLA) reduces the pain of venepuncture and intravenous cannulation. Repeated prilocaine exposure in small infants carries a methaemoglobinaemia risk, so amethocaine is generally preferred for repeated access. Paracetamol has a role in sustained or ongoing pain, as confirmed by the Ohlsson 2020 Cochrane review, and bridges the gap between brief procedural analgesia and opioid therapy. [10]
Opioids - morphine and fentanyl - are reserved for major procedures, surgery and ventilation, and are titrated with full monitoring. The NEOPAIN trial (Simons 2003) is the boundary evidence here: routine morphine infusion in ventilated preterm infants did not improve outcomes and is not standard practice. Opioids treat the individual patient's documented pain or procedural need; they are not infused routinely across a ventilated cohort. [3]
Specific Subtypes & Scenarios
The common minor bedside procedures - heel lance, capillary gas sampling, and suctioning - are managed with environmental measures plus oral sucrose and non-nutritive sucking. Where a blood sample allows it, venepuncture is preferred over heel lance because venepuncture is the less painful route, and sucrose with sucking covers the residual discomfort. [4] [9]
Venepuncture and intravenous cannulation combine several tiers: breastfeeding or breast milk as first-line where feasible, with a topical anaesthetic for the skin puncture, and sucrose with non-nutritive sucking as an adjunct. Lumbar puncture adds topical anaesthesia and careful positioning with sucrose and sucking, and the infant is monitored throughout for the physiological cost of the procedure. [5] [10]
[4] [5]Retinopathy-of-prematurity eye examination is a sustained, unpleasant procedure. Sucrose with non-nutritive sucking forms the base, and a judicious opioid is added where the discomfort of the speculum and the duration of the assessment require it. Intubation and surgery sit at the top of the ladder: a pre-emptive opioid - morphine or fentanyl - is given and titrated, with full monitoring, because these are genuinely major painful events that a sweet taste cannot reach. [3] [4]
Complications & Pitfalls
The complication of under-treatment is the one this topic exists to prevent: the acute physiological instability of an unrelieved painful event, and the long-term altered somatosensory processing and impaired neurodevelopment that follow repeated untreated pain in the preterm. Every unrecognised and unscored pain episode is a preventable insult to a developing brain. [1]
The complication of over-treatment lies mainly with the opioids. Respiratory depression, hypotension, tolerance and dependence, and ileus are the predictable costs of unchecked opioid use, and the NEOPAIN trial established that routine morphine infusion in ventilated preterm infants did not improve outcome. Sucrose has its own pitfall: it is a procedural analgesic, and using it as a substitute for opioid therapy in major pain both fails the patient and delays adequate analgesia. [3] [9]
The assessment pitfalls round out the list. A single normal heart rate never excludes pain; a sick or preterm infant may be behaviourally flat and still hurt; and a tool validated for an older age band, or an adult pain scale, has no place at the neonatal cot. The score must fit the gestation and the temporal type, and it must be charted both before and after the intervention. [2]
Prognosis & Disposition
The prognosis of an individual treated pain episode is good: a comfort measure matched to the procedure, checked with a re-score and documented, relieves the acute distress and closes the loop. The harm lies in the unrecognised, untreated and unmonitored pain - the episode that was never scored and therefore never acted upon. [1]
At the population level, repeated untreated neonatal pain is associated with altered pain processing, lower pain thresholds and adverse neurodevelopmental outcome, concentrated in the extremely preterm infant who carries the highest procedural burden. The disposition is therefore not a one-off analgesic dose but a unit-wide pain and comfort protocol: a standard tool, a standard ladder, and a standard expectation that every procedure is scored and comforted. [1] [8]
Special Populations
The extremely preterm infant is the population in whom neonatal pain matters most. The procedural burden is highest, the nociceptive system is hyper-excitable, and the long-term neurological stakes are greatest. Dose precision matters - the sucrose volume is weight-based and the smallest infant is the one in whom cumulative dosing and stability are watched most closely - and environmental redesign through single-family-room care and protected sleep is part of the treatment, not a luxury. [7] [8]
The surgical infant needs structured perioperative analgesia, built on paracetamol and titrated opioids, with a planned transition from the intra-operative regimen to the postoperative course. N-PASS is the natural tool here, because it measures prolonged pain and sedation together across the days of recovery. The infant of an opioid-dependent mother presents the reverse trap: neonatal abstinence syndrome mimics pain and is measured with a withdrawal-specific score, and the task is to treat the withdrawal adequately without over-sedating. [3]
Evidence, Guidelines & Regional Differences
The framework that ended the 'neonates cannot feel pain' myth is the Anand 2001 International Consensus Statement for the prevention and management of pain in the newborn, which set the expectation that neonatal pain is real, measurable and treatable. Two Cochrane reviews carry the procedural-comfort evidence: the Stevens 2016 review of sucrose for analgesia in newborn infants undergoing painful procedures, and the Shah 2023 review of breastfeeding or breast milk for procedural pain. The Pillai Riddell 2015 review anchors the non-pharmacological core of sucking, swaddling, tucking and skin-to-skin. [1] [4] [5] [6]
The boundary of the opioid evidence is the Simons 2003 NEOPAIN trial. Routine morphine infusion in ventilated preterm infants did not improve the composite outcome of death or severe intraventricular haemorrhage, and routine infusion is therefore not the standard; opioids are titrated to the individual patient's documented pain or procedural need. The Ohlsson 2020 Cochrane review supports paracetamol for sustained pain, rounding out the pharmacological ladder. [3] [10]
Across ANZ, the UK, Europe and North America the consensus is consistent: minimise procedures, lead with breast milk or sucrose and the non-pharmacological core for procedural pain, and reserve titrated opioids for major procedures and ventilation. Regional variation sits in the choice of the dominant prolonged-pain tool (N-PASS in most units), the availability of single-family-room environmental redesign, and the degree of opioid-sparing protocolisation. The shared rule is that one validated score is chosen, charted before and after every procedure, and used to drive the comfort decision. [1] [4]
The active controversies are few but real: the long-term safety of repeated sucrose in the extremely preterm infant; the best single tool for prolonged pain; whether single-family-room environmental redesign improves or complicates outcomes; and the correct balance between opioid sparing and adequate analgesia. The neuroscience underpinning all of them - that neonates feel pain and that the preterm brain is the most vulnerable - is settled. [8]
Exam Pearls
PIPP components - 'G-B-Heartsat-BEN'
References
- [1]Anand KJ; International Evidence-Based Group for Neonatal Pain Consensus statement for the prevention and management of pain in the newborn. Arch Pediatr Adolesc Med, 2001.PMID 11177093
- [2]Stevens B; Johnston C; Petryshen P; Taddio A Premature Infant Pain Profile: development and initial validation. Clin J Pain, 1996.PMID 8722730
- [3]Simons SH; van Dijk M; van Lingen RA; Roofthooft D; Duivenvoorden HJ; Jongeneel N; Bunkers C; Smink E; Anand KJ; van den Anker JN; Tibboel D Routine morphine infusion in preterm newborns who received ventilatory support: a randomized controlled trial. JAMA, 2003.PMID 14612478
- [4]Stevens B; Yamada J; Ohlsson A; Haliburton S; Shorkey A Sucrose for analgesia in newborn infants undergoing painful procedures. Cochrane Database Syst Rev, 2016.PMID 27420164
- [5]Shah PS; Torgalkar R; Shah VS Breastfeeding or breast milk for procedural pain in neonates. Cochrane Database Syst Rev, 2023.PMID 37643989
- [6]Pillai Riddell RR; Racine NM; Gennis HG; Turcotte K; Uman LS; Horton RE; Ahola Kohut S; Hillgrove Stuart J; Stevens B; Lisi DM Non-pharmacological management of infant and young child procedural pain. Cochrane Database Syst Rev, 2015.PMID 26630545
- [7]Slater R; Cantarella A; Gallella S; Worley A; Boyd S; Meek J; Fitzgerald M Cortical pain responses in human infants. J Neurosci, 2006.PMID 16597720
- [8]Goksan S; Hartley C; Emery F; Cockrill N; Poorun R; Moultrie F; Rogers R; Campbell J; Sanders M; Adams E; Clare S; Jenkinson M; Tracey I; Slater R fMRI reveals neural activity overlap between adult and infant pain. Elife, 2015.PMID 25895592
- [9]Gibbins S; Stevens B; Hodnett E; Pinelli J; Ohlsson A; Darlington G Efficacy and safety of sucrose for procedural pain relief in preterm and term neonates. Nurs Res, 2002.PMID 12464757
- [10]Ohlsson A; Shah PS Paracetamol (acetaminophen) for prevention or treatment of pain in newborns. Cochrane Database Syst Rev, 2020.PMID 31985830