Paeds · fetal-neonatal-and-perinatal
Neonatal respiratory distress: diagnostic approach
Also known as Neonatal respiratory distress: diagnostic approach
Fellowship guide to neonatal respiratory distress: diagnostic approach.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Neonatal respiratory distress is the clinical syndrome of laboured breathing in the first hours to days of life, defined by tachypnoea (respiratory rate persistently above 60 per minute), increased work of breathing (subcostal and intercostal recession, nasal flaring, grunting), and impaired gas exchange manifested as hypoxaemia, hypercapnia, or both. It is the single most common reason for neonatal unit admission, affecting roughly 7% of all liveborn term and near-term infants and the overwhelming majority of very preterm infants. [1]
The diagnostic task at the bedside is not merely to confirm that an infant is in distress but to distinguish among the mechanisms causing it — surfactant-deficient lung disease (respiratory distress syndrome, RDS), retained fetal lung liquid (transient tachypnoea of the newborn, TTN), meconium aspiration, neonatal pneumonia or sepsis, structural thoracic or airway pathology, congenital heart disease, and systemic or metabolic derangements — because each demands a different intervention within the first golden hour. [1] [5]
Epidemiology & Risk Factors
Respiratory distress affects approximately 7% of all term and late-preterm newborns and virtually all infants born below 28 weeks of gestation. The epidemiology is dominated by gestational age: RDS incidence falls from roughly 60% at 26–28 weeks to under 1% at 37 weeks, while TTN rises with elective caesarean section before labour and late-preterm delivery. [1]
Key risk factors stratify by mechanism. For RDS the determinants are prematurity, maternal diabetes (fetal hyperinsulinaemia antagonises surfactant maturation), perinatal asphyxia, and male sex; antenatal corticosteroids and deferred cord clamping reduce both incidence and severity. [1] [7] For TTN the principal risk is elective caesarean section without labour (the thoracic squeeze of vaginal delivery and the catecholamine-driven reabsorption of fetal lung liquid are both bypassed), augmented by maternal asthma, diabetes, and late-preterm gestation. Meconium aspiration is concentrated in term and post-term infants, especially those with fetal distress or a complicated delivery, while neonatal pneumonia is linked to prolonged rupture of membranes, maternal chorioamnionitis, colonisation with group B streptococcus (GBS), and prematurity. [5]
Pathophysiology
The unifying pathophysiology of respiratory distress is a failure of the lung to achieve and sustain functional residual capacity and efficient gas exchange after the transition from placental to pulmonary respiration. In the healthy term newborn, three events occur in sequence: clearance of fetal lung liquid (initially by transepithelial reabsorption driven by labour catecholamines and amiloride-sensitive sodium channels, then by the mechanical squeeze of delivery), establishment of alveolar surfactant, and the sharp fall in pulmonary vascular resistance at the first breaths that diverts the right-heart output from the placenta to the lungs. [1] [6]
RDS is the archetype of surfactant deficiency: type II pneumocytes begin producing surfactant around 24 weeks with a surge at 34–36 weeks, so the preterm lung has low surfactant stores and high alveolar surface tension. The result is progressive atelectasis at end-expiration, falling compliance, ventilation–perfusion mismatch, intrapulmonary shunting, and a combined respiratory and metabolic acidosis that drives pulmonary vasoconstriction and may precipitate persistent pulmonary hypertension of the newborn (PPHN). [1] The infant's grunt is a compensatory manoeuvre — exhalation against a partially closed glottis that generates physiological positive end-expiratory pressure to splint alveoli open. [5]
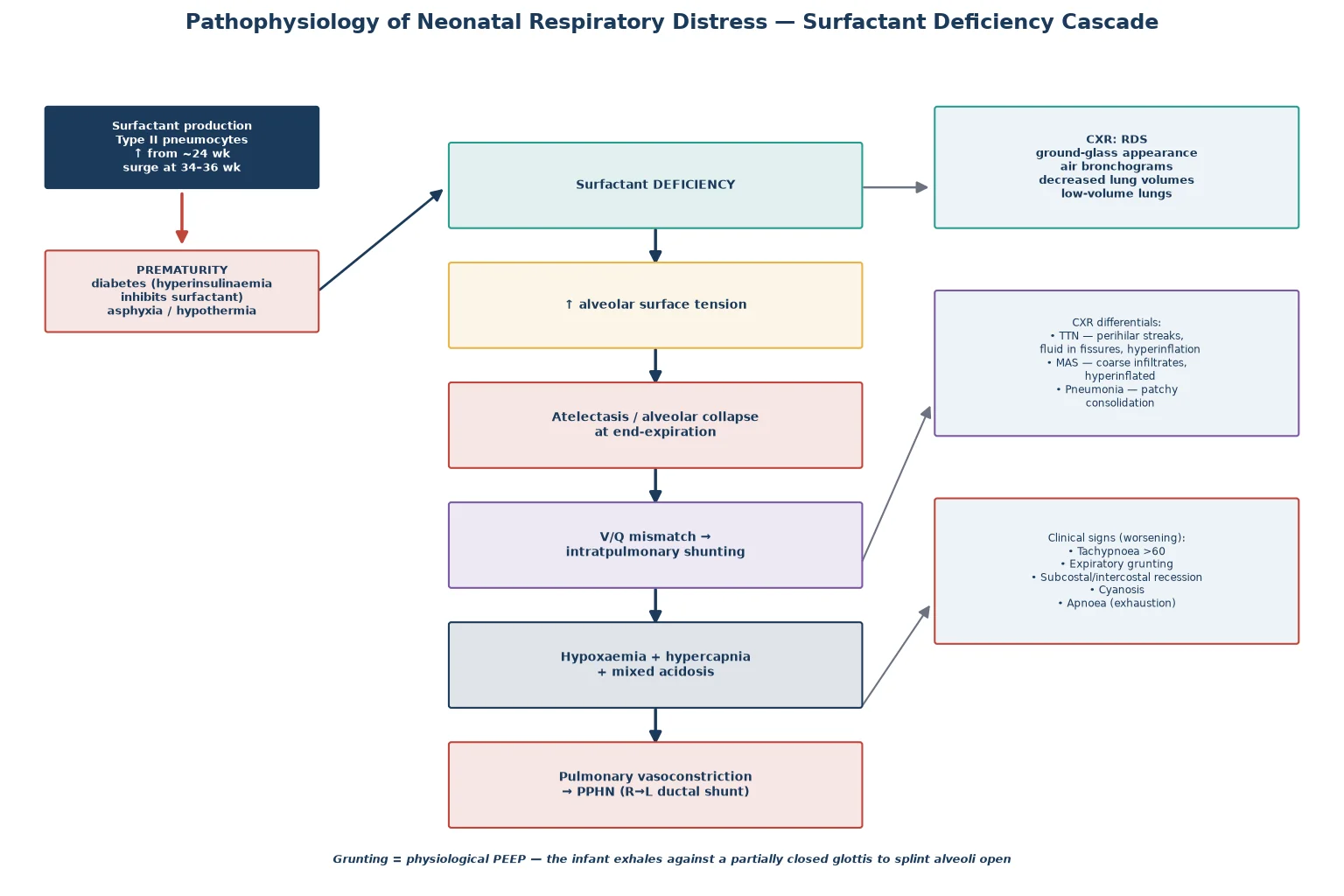
TTN arises when the liquid clearance mechanism fails — the lung retains fluid, lymphatic drainage is overwhelmed, and compliant airways trap fluid, producing a self-limiting picture of tachypnoea with a generally preserved gas exchange that resolves over 24 to 72 hours. Meconium aspiration injures the lung by mechanical airway obstruction (ball-valve effect causing hyperinflation and air leak), chemical pneumonitis, and surfactant inactivation, frequently complicated by PPHN. Neonatal pneumonia causes patchy consolidation and a systemic inflammatory response that can be indistinguishable from RDS in the preterm infant, which is why maternal risk factors and the septic screen drive early empiric antibiotics. [5] [6]
Classification
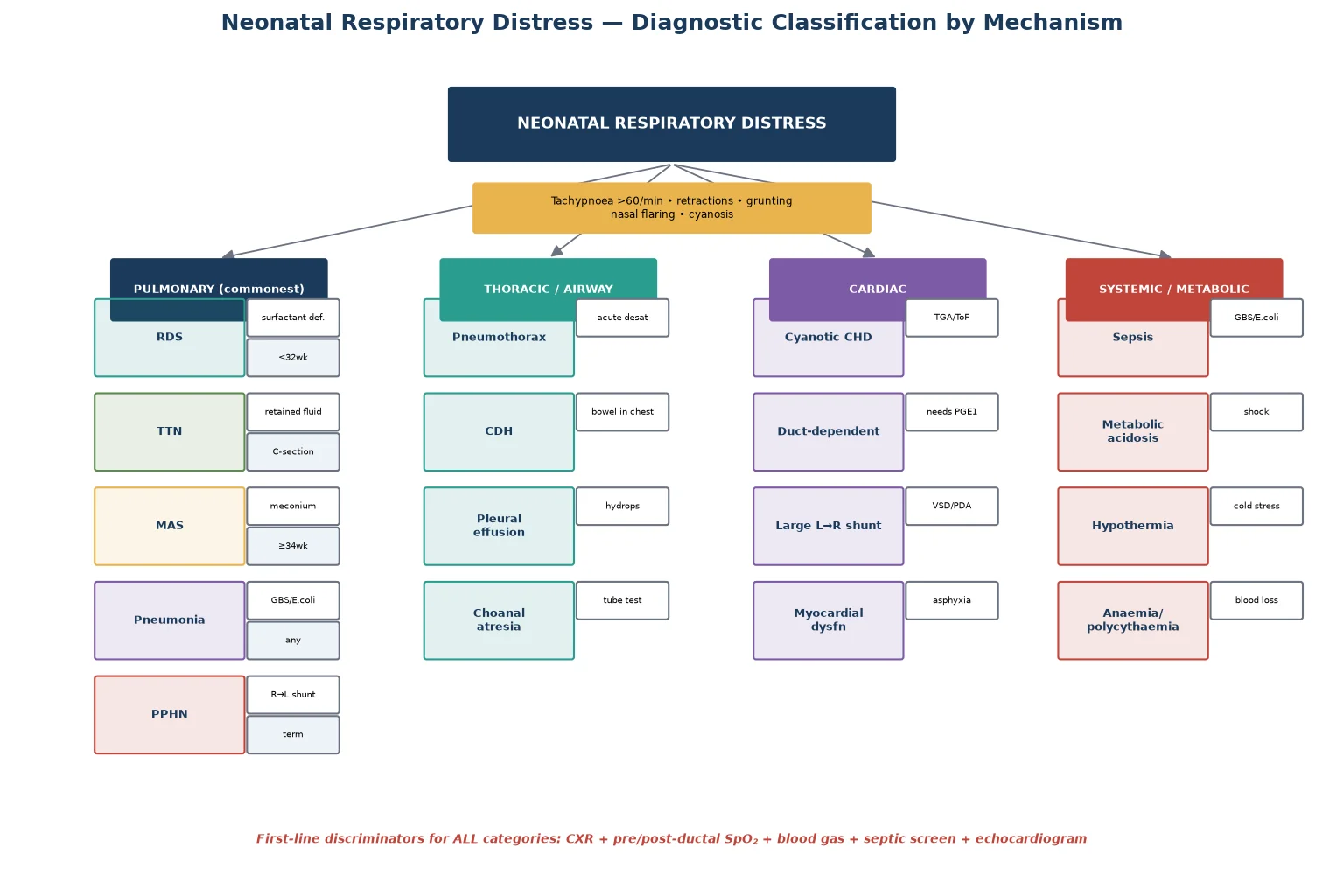
Neonatal respiratory distress is best classified by anatomical mechanism, because each category maps to a signature chest X-ray pattern, a target investigation, and a specific first-line therapy. The four broad mechanistic families are pulmonary (the commonest), extrapulmonary thoracic or airway, cardiac, and systemic or metabolic. [1] [5]
Clinical Presentation
The clinical presentation is a constellation of signs that, taken together, quantify the severity of work of breathing and the degree of gas-exchange failure. Tachypnoea (rate above 60 per minute sustained over several counts) is usually the first sign; expiratory grunting follows as the infant attempts to maintain alveolar recruitment. Subcostal and intercostal recession, suprasternal indrawing, and nasal flaring reflect the increased elastic and resistive load on a poorly compliant lung. [5]
Cyanosis, initially peri-oral then central, signals hypoxaemia; pallor and mottling suggest poor perfusion or evolving acidosis. Apnoea — especially in the preterm infant — is an ominous sign of respiratory muscle fatigue and impending failure, not a benign event. The temporal evolution is informative: RDS worsens over the first 24 to 48 hours, TTN peaks in the first day and resolves over 72 hours, and sepsis may declare itself with a smouldering but progressive course. A differential cyanosis (pink pre-ductal, blue post-ductal, or vice versa) or failure to reach target saturations in supplementary oxygen should immediately raise PPHN or congenital heart disease. [5] [6]
Differential Diagnosis
The differential diagnosis spans the four mechanistic families. Within the pulmonary group, RDS, TTN, MAS, neonatal pneumonia, and pulmonary haemorrhage are the principal contenders; PPHN may complicate any of them. Thoracic and airway causes include pneumothorax (which can complicate any parenchymal disease or positive-pressure ventilation and presents with sudden asymmetrical breath sounds and a shift in the cardiac impulse), congenital diaphragmatic hernia (bowel loops in the chest on one side with mediastinal shift, often diagnosed antenatally but occasionally a postnatal surprise), pleural effusion, and upper-airway obstruction such as choanal atresia. [5]
Cardiac causes — cyanotic congenital heart disease (transposition, tetralogy, total anomalous pulmonary venous return), duct-dependent lesions that collapse as the ductus closes, and large left-to-right shunts — are the most easily missed because the chest X-ray may be deceptively normal and the infant may not have a murmur. Systemic causes include early-onset sepsis (GBS, Escherichia coli), metabolic acidosis from shock or inborn errors, hypothermia, and severe anaemia or polycythaemia. The discriminating investigations — chest X-ray, blood gas, pre/post-ductal oximetry, septic screen and echocardiogram — resolve this list within the first hour. [5] [6]
Clinical & Bedside Assessment
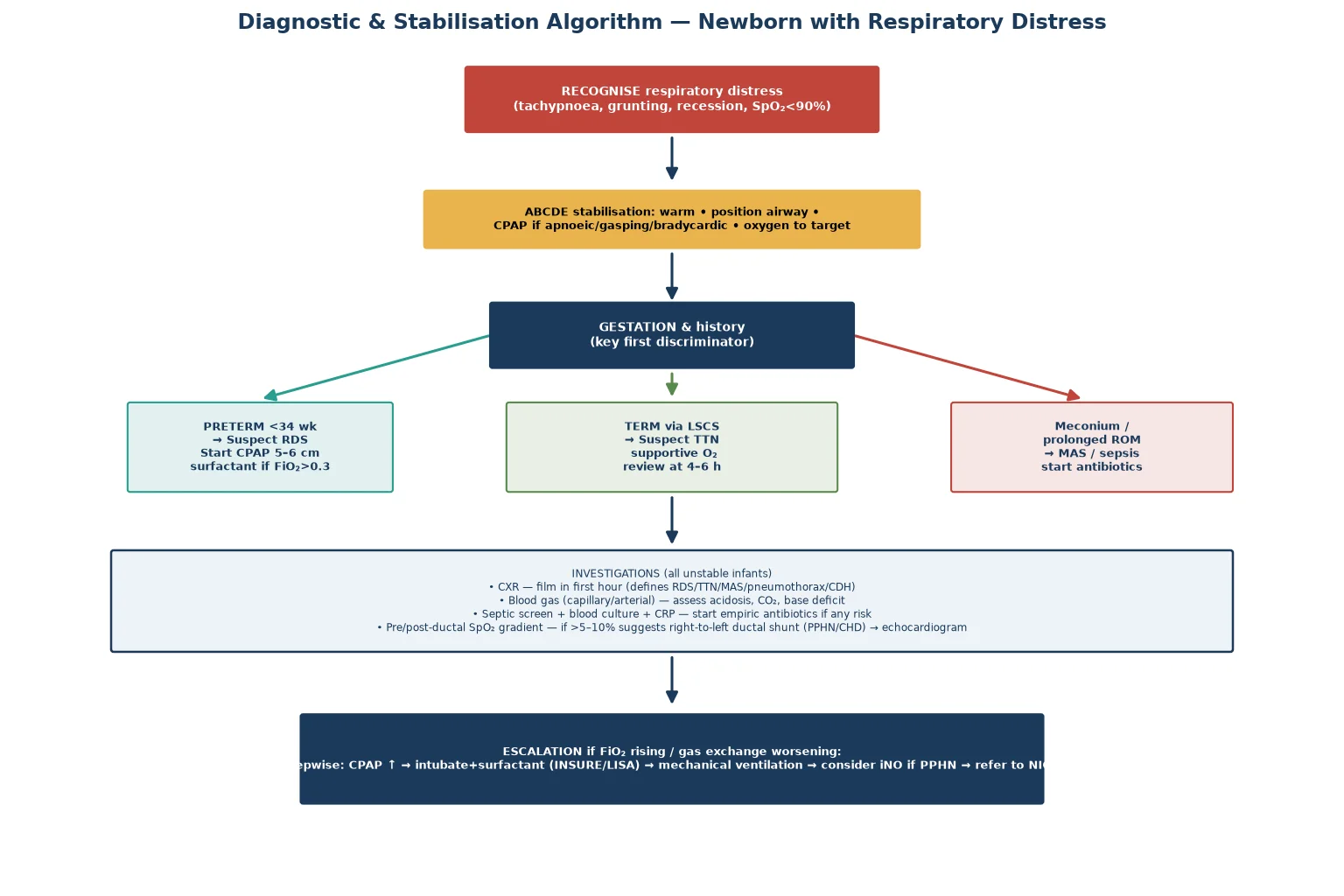
Bedside assessment proceeds in two layers: an immediate ABCDE stabilisation and a targeted history and examination that refines the mechanism. Stabilisation comes first — maintain temperature (warm, dry, stimulate), position the airway, and provide CPAP or positive-pressure ventilation if the infant is apnoeic, gasping, centrally cyanotic, or bradycardic. Oxygen is titrated to target saturations rather than given in fixed high concentration, because hyperoxia is harmful to the preterm retina and adds no benefit once the target is met. [5] [6]
The focused history captures the elements that reweight the differential: gestation and birthweight (RDS versus TTN); mode of onset and whether labour occurred (TTN risk); presence of meconium-stained liquor (MAS); maternal GBS status, prolonged rupture of membranes, and chorioamnionitis (sepsis); maternal diabetes and antenatal steroid receipt (RDS modifier); and any antenatally diagnosed structural anomaly. Examination seeks the signature of each mechanism — asymmetrical breath sounds and tracheal deviation (pneumothorax), scaphoid abdomen with reduced air entry on one side (diaphragmatic hernia), murmurs and pulse discrepancies (congenital heart disease), and the general perfusion and tone that signal systemic illness. [5] [6]
Investigations
Investigations confirm the mechanism and quantify severity. The chest X-ray is the highest-yield single test and should be obtained early in any distressed infant: RDS shows a symmetric ground-glass appearance with air bronchograms and low lung volumes; TTN shows prominent perihilar streaking, fluid in the minor fissure, and mild hyperinflation; MAS shows coarse, patchy infiltrates with hyperinflation and occasionally a pneumothorax; pneumonia shows focal or patchy consolidation; a pneumothorax shows a hyperlucent hemithorax with mediastinal shift; and a diaphragmatic hernia shows bowel loops within the chest with mediastinal shift. [1] [5]
Blood gas analysis (capillary or arterial) assesses the degree of acidosis, the carbon dioxide tension, and the base deficit — a marker of tissue hypoperfusion — and guides escalation. The septic screen (blood culture, C-reactive protein, and if indicated a lumbar puncture and surface swabs) is performed and empiric antibiotics started whenever infection is plausible, because neonatal pneumonia is clinically and radiologically indistinguishable from RDS in the preterm infant. Pre- and post-ductal saturations quantify any right-to-left shunt; a significant gradient, or failure of saturations to improve in high-concentration oxygen, prompts echocardiography to confirm or exclude congenital heart disease and PPHN. A blood glucose excludes hypoglycaemia, and a full blood count evaluates anaemia, polycythaemia, and the neutrophil count for sepsis. [5] [6]
Management — Resuscitation
Resuscitation of the distressed newborn follows the international neonatal resuscitation algorithm. The priorities are warmth, airway, and breathing: dry and warm the infant, position the head in slight extension to open the airway, clear secretions if obstructing (routine suctioning is not recommended for vigorous infants, and for non-vigorous infants born through meconium the priority is ventilation, not intubation and tracheal suctioning), and assess tone, breathing, and heart rate. [5] [6]
Positive-pressure ventilation is started if the infant is apnoeic or gasping, if the heart rate is below 100 per minute, or if central cyanosis persists despite free-flow oxygen. The first breaths use an air–oxygen blend in most resuscitations — term infants start in air (21%) and preterm infants in 21–30% — with oxygen titrated upward only if saturations remain below target, because the neonatal transition is gradual and saturations of 70–80% in the first five minutes are normal. CPAP (5–6 cm H₂O) is started early in spontaneously breathing preterm infants with distress, as it splints alveoli, conserves surfactant, and reduces the need for intubation. [3] [5]
Neonatal resuscitation sequence for the distressed infant
Warm, dry, stimulate; position airway; start the clock
Assess tone, breathing, heart rate; start pulse oximetry
If apnoeic/gasping or HR under 100: start positive-pressure ventilation (PPV)
Use air–oxygen blend; titrate oxygen to target saturations by age
If laboured breathing with good tone: start CPAP 5–6 cm H₂O
If HR under 60 after 30 s effective ventilation: add chest compressions and raise oxygen
Reassess HR and breathing every 30–60 s; escalate to intubation if not improving
Management — Definitive & Stepwise
Definitive management is mechanism-specific and stepwise, escalating from the least invasive effective support to the most. For RDS the cornerstones are CPAP, surfactant, and oxygen titration: early nasal CPAP (started in the delivery suite for any preterm infant with distress) reduces intubation rates and bronchopulmonary dysplasia, and exogenous surfactant is given to preterm infants who remain in significant distress or whose FiO₂ requirement exceeds 0.30. [1] [3] The SUPPORT trial established that an initial CPAP strategy in extremely preterm infants is not inferior to prophylactic intubation and surfactant, cementing CPAP-first as the standard and reserving surfactant for infants who fail CPAP. [3]
Surfactant is delivered as a single or two-dose regimen of a natural (animal-derived) preparation, which the Cochrane review confirms is superior to synthetic products for reducing mortality and pneumothorax. [2] [8] Increasingly, surfactant is given by less invasive techniques — the INSURE (intubate–surfactant–extubate) approach or minimally invasive surfactant administration via a thin catheter while the infant breathes on CPAP — which preserve spontaneous breathing and reduce ventilator exposure and bronchopulmonary dysplasia. [4]
For TTN, management is supportive: supplemental oxygen titrated to target, minimal handling, and observation, with resolution expected within 24–72 hours; persistent or worsening distress mandates re-evaluation for an alternative diagnosis. For MAS, the priority is airway and ventilation — no routine intubation and suctioning of non-vigorous infants, but prompt ventilation for the depressed infant, with surfactant considered for severe disease because meconium inactivates endogenous surfactant, and inhaled nitric oxide for associated PPHN. Neonatal pneumonia and sepsis require prompt empiric intravenous antibiotics (typically a beta-lactam such as benzylpenicillin or ampicillin with an aminoglycoside), guided by local GBS resistance patterns and stopped if cultures are negative at 36–48 hours. [5] [6]
In Australia, New Zealand and the United Kingdom, empiric cover for early-onset neonatal sepsis is typically benzylpenicillin (or ampicillin) plus gentamicin, reflecting the dominance of group B streptococcus and E. coli; benzylpenicillin 60 mg/kg IV (dose interval by gestation and age) targets GBS, with gentamicin dosed by gestational age and postnatal age. Antibiotics are reviewed at 36–48 hours and stopped if cultures and inflammatory markers are negative, in line with antimicrobial stewardship. [5] [6]
Specific Subtypes & Scenarios
The preterm extreme (under 28 weeks) deserves particular attention. The 2022 European Consensus Guidelines recommend deferred cord clamping for at least 30 seconds (or intact-cord stabilisation) with active warming, early CPAP from the delivery suite, and surfactant by a minimally invasive technique if the FiO₂ requirement exceeds 0.30. [1] Cord milking is contraindicated below 28 weeks: the Katheria 2019 JAMA trial showed an excess of severe intraventricular haemorrhage and the trial was stopped early, so deferred clamping — not milking — is the standard for this group. [7]
The term infant with cyanosis refractory to oxygen is the cardiac-lesion scenario that examiners probe relentlessly. The hyperoxia test (measure post-ductal PaO₂ or saturation in 100% oxygen) was once central but has been superseded by echocardiography; the practical point is that a term infant with respiratory distress, a normal chest X-ray, and no improvement in saturations with oxygen must be assumed to have a duct-dependent lesion until echocardiography proves otherwise, and prostaglandin E1 (alprostadil) should be started at 0.01–0.05 microgram/kg/min while awaiting imaging. [5] [6]
Complications & Pitfalls
The complications of respiratory distress and its treatment fall into pulmonary, neurological, and iatrogenic groups. Pulmonary complications include air leak (pneumothorax, pulmonary interstitial emphysema) from positive-pressure ventilation, pulmonary haemorrhage, and bronchopulmonary dysplasia — the chronic lung disease of prematurity that complicates prolonged ventilation and oxygen exposure. PPHN complicates RDS, MAS, pneumonia, and asphyxia, requiring optimisation of oxygenation, ventilation, and sometimes inhaled nitric oxide. [1] [5]
Neurological complications include intraventricular haemorrhage (linked to prematurity and haemodynamic instability, and the reason cord milking is avoided under 28 weeks) and periventricular leukomalacia. Iatrogenic complications — oxygen toxicity to the retina (retinopathy of prematurity), ventilator-associated lung injury (volutrauma), and nosocomial infection — are minimised by CPAP-first strategies, less invasive surfactant administration, restrictive transfusion, and tight oxygen targeting. [1] [4] [7]
Prognosis & Disposition
Prognosis is determined by the underlying mechanism, gestation, and the speed of effective intervention. TTN carries an excellent prognosis with full recovery within days and no long-term sequelae. RDS in the modern era — with antenatal steroids, CPAP, and surfactant — has a mortality below 10% in most units for infants above 28 weeks, though extreme prematurity and bronchopulmonary dysplasia remain major challenges. Meconium aspiration has a mortality of up to 5% in severe cases, dominated by PPHN and neurological injury from perinatal asphyxia. Neonatal pneumonia and sepsis outcomes depend on organism and timeliness of antibiotics, with GBS case fatality of 5–10% in term infants and higher in preterm. [1] [5]
Disposition follows severity: mildly distressed term infants with TTN may be managed in a transitional care or special-care setting with monitoring; any infant needing CPAP, supplementary oxygen above a low threshold, or intravenous antibiotics is admitted to the neonatal unit; those requiring intubation, surfactant, inhaled nitric oxide, or prostaglandin E1 are transferred to a neonatal intensive care unit, with retrieval to a tertiary centre if a cardiac lesion or surgical pathology is confirmed. [5] [6]
Special Populations
Infants of diabetic mothers are a high-risk group: fetal hyperinsulinaemia antagonises surfactant maturation, raising the risk of RDS in a term or late-preterm infant, and these infants are also prone to hypoglycaemia, polycythaemia, and hyperviscosity. Late-preterm infants (34–36 weeks) have the highest population rate of respiratory distress because they combine residual surfactant immaturity with an immature liquid-clearance mechanism; they are frequently mismanaged as term infants and represent a large share of neonatal readmissions. [1]
The growth-restricted and asphyxiated infant has compromised respiratory reserve: surfactant may be depleted by stress, the myocardium is dysfunctional, and PPHN is common. Multiple births raise the risk of prematurity and polyhydramnios-related complications. In each of these groups the diagnostic approach is unchanged, but the threshold for CXR, surfactant, and septic screening is lower and the escalation ladder is climbed earlier. [5] [6]
Evidence, Guidelines & Regional Differences
The evidence base and guideline landscape for neonatal respiratory distress are mature and largely concordant internationally. The 2022 European Consensus Guidelines on RDS synthesise surfactant, CPAP, and oxygen-targeting evidence and are the most widely cited reference in neonatal practice; they endorse CPAP-first, minimally invasive surfactant, deferred cord clamping, and blended oxygen titration. [1] The American Heart Association 2020 and European Resuscitation Council 2021 neonatal resuscitation guidelines converge on the same principles: air for term resuscitation, 21–30% for preterm, no routine intubation and suctioning for non-vigorous meconium infants, and early CPAP. [5] [6]
The pivotal randomised evidence includes the SUPPORT trial, which established CPAP-first for extremely preterm infants, and the non-invasive surfactant literature that underpins the LISA/INSURE approach. [3] [4] The Cochrane review of animal-derived surfactants confirms their superiority over synthetic products. [8] Regional differences are modest: ANZ and UK practice closely follows these guidelines, with empiric antibiotic conventions reflecting local GBS epidemiology, and a consistent emphasis on deferred cord clamping with the milking contraindication under 28 weeks grounded in the Katheria trial. [7]
The European Consensus Guidelines (widely adopted in ANZ, UK, and Europe) recommend surfactant for preterm infants with RDS whose FiO₂ requirement exceeds 0.30 on CPAP, favouring less invasive administration (LISA/MIST). Some North American centres historically used a higher FiO₂ threshold (over 0.40) or routine prophylactic surfactant in the smallest infants; contemporary practice across regions is converging on CPAP-first with rescue surfactant for CPAP failure. [1] [3]
Exam Pearls
Causes of neonatal respiratory distress — 'Respiratory Distress In Newborn'
References
- [1]Sweet DG; Carnielli VP; Discenza M; Hallman M; Klebermass-Schrehof K; O'Donnell CPF; Plavka R; Resch B; Saugstad OD; Senterre T; et al European Consensus Guidelines on the Management of Respiratory Distress Syndrome: 2022 Update. Neonatology, 2023.PMID 36863329
- [2]Polin RA; Carlo WA; Committee on Fetus and Newborn Surfactant replacement therapy for preterm and term neonates with respiratory distress. Pediatrics, 2014.PMID 24379227
- [3]Finer NN; Carlo WA; Walsh MC; Rich W; Gantz MG; Laptook AR; Yoder BA; Faix RG; Das A; Poole WK; et al Early CPAP versus surfactant in extremely preterm infants. N Engl J Med, 2010.PMID 20472939
- [4]Härtel C; Hartz A; Kribs A; Wieg C; Kuester W; Mehler K; Roll C; Simma S; Wense A; Voss W; et al Association of Administration of Surfactant Using Less Invasive Methods With Outcomes in Extremely Preterm Infants. JAMA Netw Open, 2022.PMID 35943742
- [5]Aziz K; Lee CHC; Escobedo MB; Hoover AV; Kamath-Rayne BD; Kapadia VS; Magid DJ; Niermeyer S; Schmölzer GM; Szyld E; et al Part 5: Neonatal Resuscitation 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Pediatrics, 2021.PMID 33087555
- [6]Madar J; Roehr CC; Ainsworth S; Ersdal H; Morley C; Rabi Y; Szyld E; Wyllie J; Zdelar D European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation, 2021.PMID 33773829
- [7]Katheria A; Reister F; Essers J; Mendler M; Hummler H; Subramaniam A; Carlo WA; Patel S; Rabe H; El-Naggar W; et al Association of Umbilical Cord Milking vs Delayed Umbilical Cord Clamping With Death or Severe Intraventricular Hemorrhage Among Preterm Infants. JAMA, 2019.PMID 31742630
- [8]Singh N; Halliday HL; Stevens TP; Suresh G; Soll R; Roqué JT Comparison of animal-derived surfactants for the prevention and treatment of respiratory distress syndrome in preterm infants. Cochrane Database Syst Rev, 2015.PMID 26690260