Paeds · fetal-neonatal-and-perinatal
Neonatal resuscitation and post-resuscitation stabilisation
Also known as Newborn resuscitation · Delivery-room resuscitation · Neonatal life support · NRP algorithm · Post-resuscitation stabilisation of the newborn
Fellowship guide to neonatal resuscitation and post-resuscitation stabilisation: anticipation, the first-minute assessment, positive-pressure ventilation, chest compressions, adrenaline and volume, temperature and glucose control, cord management, and safe referral for therapeutic hypothermia.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A baby is born, blue and limp. The clock has started, the team has seconds, and the decisions you make in the first minute shape the rest of that child's life. Neonatal resuscitation is the structured set of actions used at birth to help a newborn establish normal breathing and circulation when spontaneous transition fails. It is not adult cardiopulmonary resuscitation scaled down — the problem at birth is almost always the lung, not the heart, and the sequence of the algorithm reflects that. [1] [3]
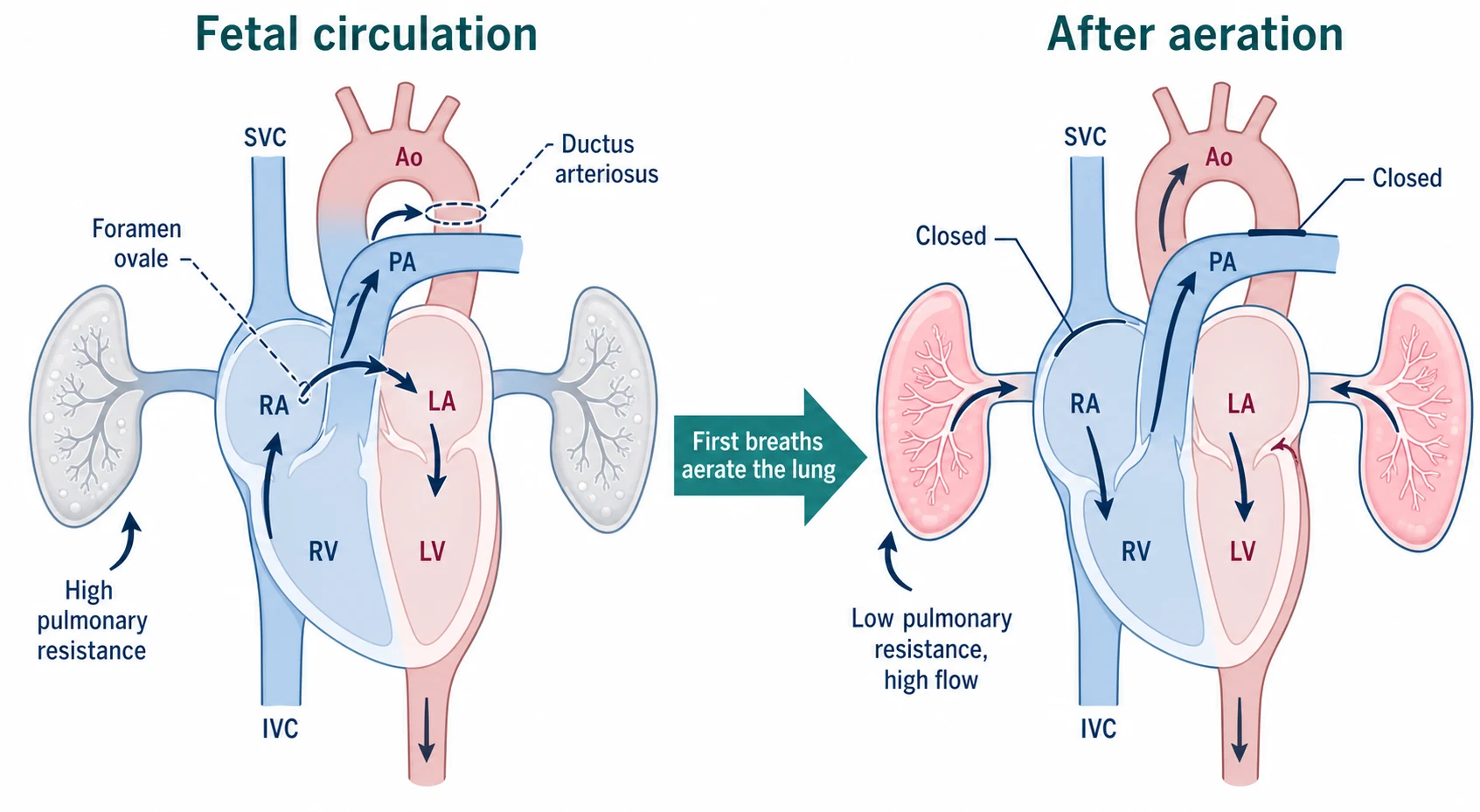
The goal is to support transition — the shift from fetal placental gas exchange to air breathing. In fetal life the lungs are fluid-filled, the pulmonary vessels are tightly constricted, and blood shunts right-to-left through the foramen ovale and ductus arteriosus. The first breaths clear fluid, replace it with air, and drop pulmonary vascular resistance; the shunts then close as systemic resistance rises. When aeration fails, the whole circuit stays fetal, the baby stays hypoxic, and the heart slows. That single mechanism — failed aeration — is why ventilation is the first and most powerful intervention, and why most "resuscitations" are really the work of getting the lung aerated. [2] [4]
The distinction that matters at the bedside is between routine care (warmth, drying, stimulation, and observation), assisted transition (positive-pressure ventilation to establish breathing), and advanced resuscitation (compressions, adrenaline, volume). The algorithm forces you up that ladder only when the heart rate fails to respond, and it brings you back down the moment it does. [1]
Classification
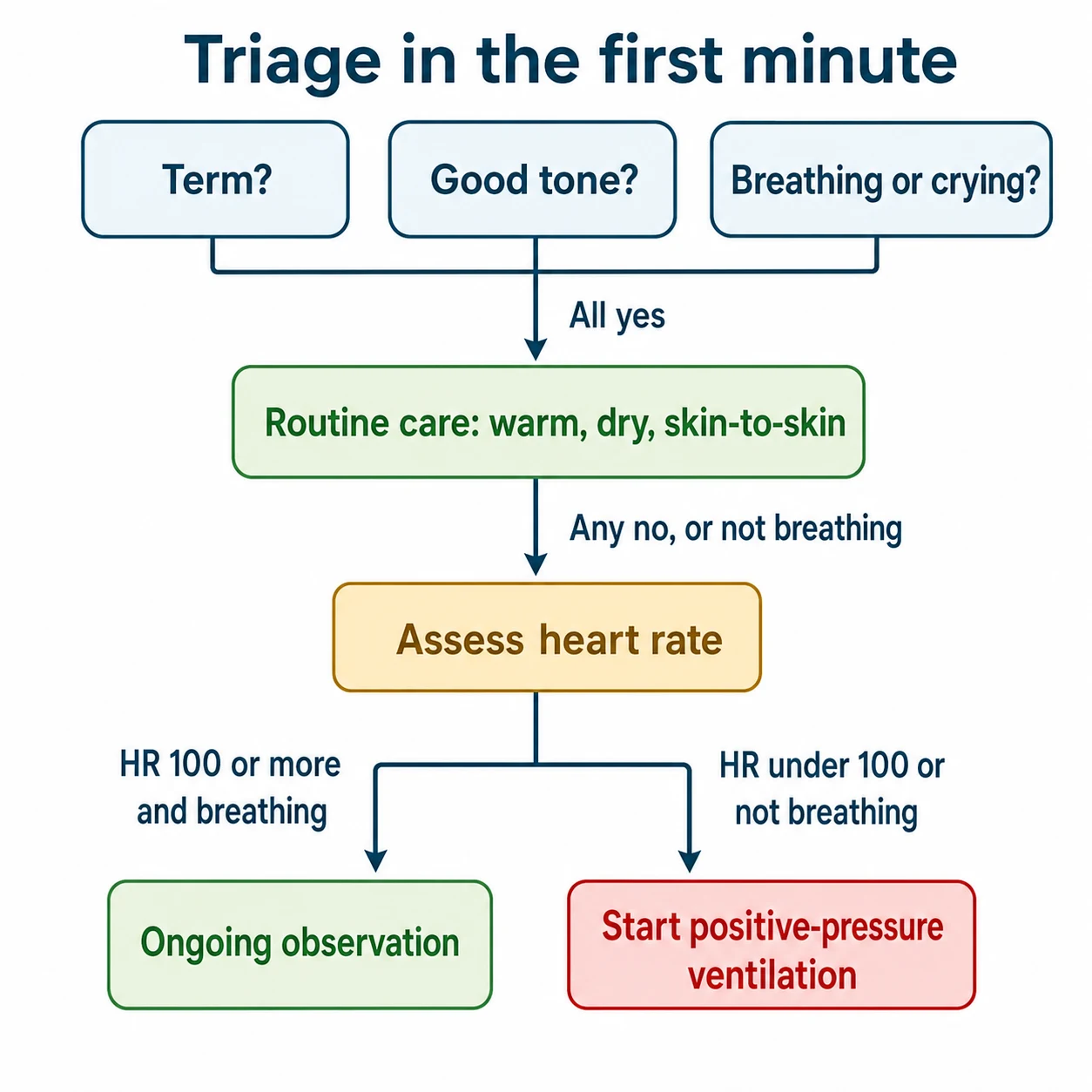
Think of a newborn at birth as being triaged by three questions, asked in the first minute: Is the baby term? Is there good tone? Is the baby breathing or crying? Answer yes to all three and the infant stays with the mother for routine care — warmth, drying, and skin-to-skin. Any "no", or apnoea or gasping, moves the infant onto the resuscitation pathway. This triage is deliberately simple because it has to work under pressure and in any setting. [1] [2]
Once on the pathway, the infant is then classified by the single measurement that drives every escalation: heart rate. A heart rate of 100 beats per minute or above with effective breathing means observe and support. A heart rate under 100, or ongoing apnoea or gasping, means start positive-pressure ventilation. A heart rate under 60 beats per minute despite effective ventilation means add chest compressions and raise the inspired oxygen, then adrenaline. Holding that heart-rate ladder in your head is holding the algorithm. [1]
Three levels of newborn care at birth
- Term, good tone, breathing or crying
- Warm, dry, skin-to-skin
- Observe breathing and colour
- Apnoea, gasping, or heart rate under 100
- Positive-pressure ventilation is the core act
- Most respond within 30 to 60 seconds
- Heart rate under 60 despite effective ventilation
- Add compressions, then adrenaline, then volume
- About 1% of newborns reach this level
Epidemiology & Risk Factors
The reassuring headline is that the overwhelming majority of newborns need no intervention. The harder truth is that the small minority who do are concentrated wherever risk can be anticipated — which is why anticipation is the first act of resuscitation. You prepare differently for a 26-week preterm, a fresh stillbirth with absent heart tones, or a term infant born through thick meconium, and you must have the right team and equipment in place before delivery. [1]
Risk concentrates along three axes. Antenatal factors include pre-eclampsia, diabetes, intrauterine growth restriction, oligohydramnios, reduced fetal movements, and known congenital anomaly. Intrapartum factors include fetal distress, emergency caesarean, instrumental delivery, cord prolapse, shoulder dystocia, abruption, chorioamnionitis, and meconium-stained liquor. Neonatal factors — chiefly prematurity and low birthweight — change both the likelihood and the technique: the preterm lung is hard to aerate and easily damaged by pressure and oxygen. [2] [4]
Setting changes everything. A tertiary centre with a neonatal team, a blender, and a radiant warmer can deliver the full algorithm; a rural hospital or an out-of-hospital birth may have only warmth, a bag, and air, and must know when to call for retrieval. Globally, intrapartum-related events remain a leading cause of neonatal mortality in low-resource settings, which is why basic warming, drying, and air-ventilation skills matter everywhere. [2]
Pathophysiology
To understand the algorithm you have to understand what it is trying to reverse. In the fetus the lungs are filled with fluid, the pulmonary arterioles are clamped shut, and the placenta does the work of gas exchange. Blood bypasses the lungs through two fetal channels: the foramen ovale, which shunts right atrial blood to the left atrium, and the ductus arteriosus, which shunts pulmonary artery blood to the aorta. [2] [4]
At birth three things must happen together. The first breaths and reabsorption of lung fluid replace fluid with air, which lowers pulmonary vascular resistance and pulls blood into the lungs. The rise in left atrial pressure and fall in right-sided pressure close the foramen ovale, and the rise in blood oxygen constricts then closes the ductus arteriosus. Systemic vascular resistance climbs as the cord is clamped and placental flow falls away. The circulation has now converted, in minutes, from a parallel right-to-left shunt to a normal adult-type series circuit. [2]
When aeration fails, none of this happens. The lung stays fluid-filled, pulmonary resistance stays high, the shunts stay open, and blood keeps bypassing the lungs. The baby stays hypoxic and hypercapnic, and the newborn heart — which is exquisitely sensitive to hypoxia — slows. This is why restoring ventilation almost always restores the heart rate: you are not rescuing a failing heart, you are re-opening the circuit the heart was waiting for. Compressions and adrenaline come later precisely because they are rarely needed once the lung is aerated. [1] [3]
The preterm lung adds two extra hazards. Its surfactant deficiency makes it stiff and prone to collapse, so a few centimetres of water pressure can be the difference between no aeration and lung over-distension and air leak. Its immature antioxidant defences make it vulnerable to oxygen toxicity, which is why resuscitation of the preterm starts in low oxygen rather than 100%. [1] [8]
Cold stress compounds all of this. A cold newborn raises its metabolic rate and oxygen consumption to generate heat, worsens metabolic acidosis, and impairs surfactant function. This is the physiological basis for the relentless focus on warmth — temperature control is not comfort care, it is resuscitation. [2]
Clinical Presentation
A newborn failing to transition shows it in three places: tone, breathing, and heart rate. Poor tone is a global sign of distress and is one of the earliest things you see as you receive the baby — a floppy, limp infant is not transitioning. Breathing may be absent (apnoea), inadequate (gasping), or simply not vigorous enough to clear fluid. Heart rate is the number that drives the algorithm, and it is the one you must get right. [1]
Assess heart rate fast and accurately. Auscultation over the precordium with a stethoscope is the quickest bedside method; palpation of the umbilical cord base is less reliable and tends to underestimate. When the rate is low or you cannot be sure, apply three-lead electrocardiography within the first minute — the AHA and ERC both now recommend ECG for rapid, accurate heart-rate assessment during resuscitation, because decisions to compress and to give adrenaline hang on this number. [1] [2]
Effective ventilation announces itself in two ways: a gentle rise of the chest with each breath, and a rising heart rate and colour within 30 to 60 seconds. If you see neither, ventilation is not working and you must run the corrective steps before escalating — the commonest reason a baby "needs compressions" is that ventilation was never effective in the first place. [1] [10]
Some presentations point away from simple failed aeration toward a specific diagnosis that needs a specific act. Pallor, poor perfusion and a history of blood loss suggest hypovolaemia and the need for volume. Asymmetric breath sounds or sudden deterioration on a ventilated preterm suggest a pneumothorax. A scaphoid abdomen and respiratory distress suggest a diaphragmatic hernia. Cyanosis that does not improve with oxygen may be a duct-dependent congenital heart lesion. After resuscitation, persistent tachypnoea, grunting, abnormal tone or seizures signal ongoing instability and the need for neonatal unit admission. [2] [4]
Differential Diagnosis
When a newborn fails to transition, work through causes by what is most common and most reversible. Inadequate ventilation — from a poor mask seal, an obstructed airway, or insufficient pressure — is the single commonest cause and the first thing to correct. Most "failed resuscitations" are failed ventilation. [1] [10]
Beyond that, hold a short list of alternatives that change management: [1] [4]
What else fails transition, and the tell
- Secretions, blood, meconium, or malposition
- Correct with suction and airway positioning
- Part of the MR SOPA sequence
- Acute blood loss, cord rupture, vasa praevia
- Pallor, poor perfusion, weak pulses
- Treat with 10 mL/kg volume or blood
- Opioids, magnesium sulfate, general anaesthesia
- Respiratory depression with a preserved heart rate
- Ventilate first; naloxone is not a resuscitation drug
- Asymmetric breath sounds on a ventilated preterm
- Sudden deterioration
- Needs needle decompression or chest drain
- Diaphragmatic hernia, choanal atresia, airway malformation
- Antenatally suspected or found on exam
- Tailor the airway and ventilation plan
Duct-dependent congenital heart disease usually declares itself after the first hours as the ductus closes, producing differential or fixed cyanosis unresponsive to oxygen; prostaglandin E1 is the treatment, not more resuscitation. Sepsis and metabolic disease (hypoglycaemia, inborn errors) complicate the post-resuscitation course and must be screened for once the baby is stable. When resuscitation is unexpectedly difficult or prolonged, always ask whether you are treating the wrong problem. [2]
Clinical & Bedside Assessment
The assessment is the algorithm's eyes. In the first 60 seconds, receive the baby under a radiant warmer, start the clock, and assess tone, breathing, and heart rate. Warm, dry, and stimulate — these are not separate from assessment, they are the first intervention, and many infants who look flat simply need to be warmed, dried, and stimulated to breathe. [1]
Confirm the heart rate early and reassess it after every change. Auscultate at the precordium, and when the rate is low or uncertain move to ECG. Watch for chest rise as the live readout of effective ventilation, and check bilateral air entry. When ventilation is not producing chest rise, run the corrective sequence before escalating. [1]
MR SOPA — the ventilation-corrective ladder
Confirm a correctly placed endotracheal tube with bilateral chest movement, equal air entry, and a rising heart rate; colourimetric CO2 detection adds objective confirmation. If you cannot intubate within a reasonable attempt and the heart rate is not rising, place a laryngeal mask airway as a rescue — it is effective for ventilation when mask ventilation or intubation fails. [1] [2]
Run the resuscitation as a team. Allocate roles before delivery — leader, airway, assessor, timer, scribe — and use call-out and closed-loop confirmation ("Heart rate 50" / "Copy, starting compressions"). A timekeeper calling the minute keeps the algorithm honest. Debrief after every significant resuscitation, and document the sequence, times, interventions and responses — this is both medico-legal record and the data for quality improvement. [10]
Investigations
In the heat of resuscitation, only a handful of measures earn their place: heart rate by ECG, oxygen saturation by pulse oximetry, temperature, and glucose. Everything else is deferred until the baby is stable, because no test should delay time-critical ventilation or compressions. [1] [2]
Pulse oximetry uses a pre-ductal probe on the right wrist to judge how well the lungs are oxygenating, and it is interpreted against a minute-by-minute target nomogram, not against the adult 100%. A post-ductal probe can be added to screen for differential cyanosis when duct-dependent cardiac disease is suspected. [1]
After the baby is stable, blood gas and lactate quantify the degree of acidosis and guide ongoing care, glucose screens for hypoglycaemia, and a chest radiograph looks for a cause — pneumonia, meconium aspiration, diaphragmatic hernia, or air leak. Septic screens and empiric antibiotics follow when infection is suspected, guided by maternal risk factors. Echocardiography distinguishes structural congenital heart disease from persistent pulmonary hypertension when cyanosis persists despite oxygen. [2] [4]
Management — Resuscitation
Before delivery, prepare and check the equipment: a preheated radiant warmer, warm dry towels and a hat, a clock, a stethoscope, suction, an appropriately sized mask, a T-piece or self-inflating bag with a pressure gauge and blender, air and oxygen sources, a pulse oximeter and ECG leads, laryngoscope and correctly sized endotracheal tubes, a CO2 detector, a laryngeal mask airway, adrenaline, and volume. For a high-risk delivery, have two skilled people present and the umbilical catheterisation kit ready. [1]
The first 60 seconds are warmth, drying, stimulation, and assessment. Receive the baby, start the clock, dry and remove wet towels, stimulate by rubbing the back or flicking the soles of the feet, and assess tone, breathing and heart rate. Most term babies who needed only this will be breathing by a minute. [1]
If the baby is apnoeic or gasping, or the heart rate is under 100, start positive-pressure ventilation — this is the pivotal act. Ventilate at 40 to 60 breaths per minute using the lowest pressure that gives gentle chest rise. For a term infant begin in air (21% oxygen); for a preterm infant under about 35 weeks begin in 21 to 30% oxygen, titrated against the saturation nomogram. Add PEEP for the preterm to support the stiff lung. [1] [8]
Positive-pressure ventilation
Dose
40–60 breaths per minute; lowest pressure giving gentle chest rise (about 20–25 cm H2O in most term infants; preterm often needs PEEP 5 cm H2O)
If the heart rate does not rise, run MR SOPA before escalating — most "non-responders" have a fixable ventilation problem. If, after 30 seconds of effective ventilation, the heart rate is still under 60, add chest compressions coordinated with ventilation in a 3:1 ratio (three compressions to one breath, about 120 events per minute), using the two-thumb encircling technique over the lower third of the sternum, compressing one-third of the anteroposterior depth, and raise the inspired oxygen toward 100%. Reassess the heart rate every 60 seconds. [1]
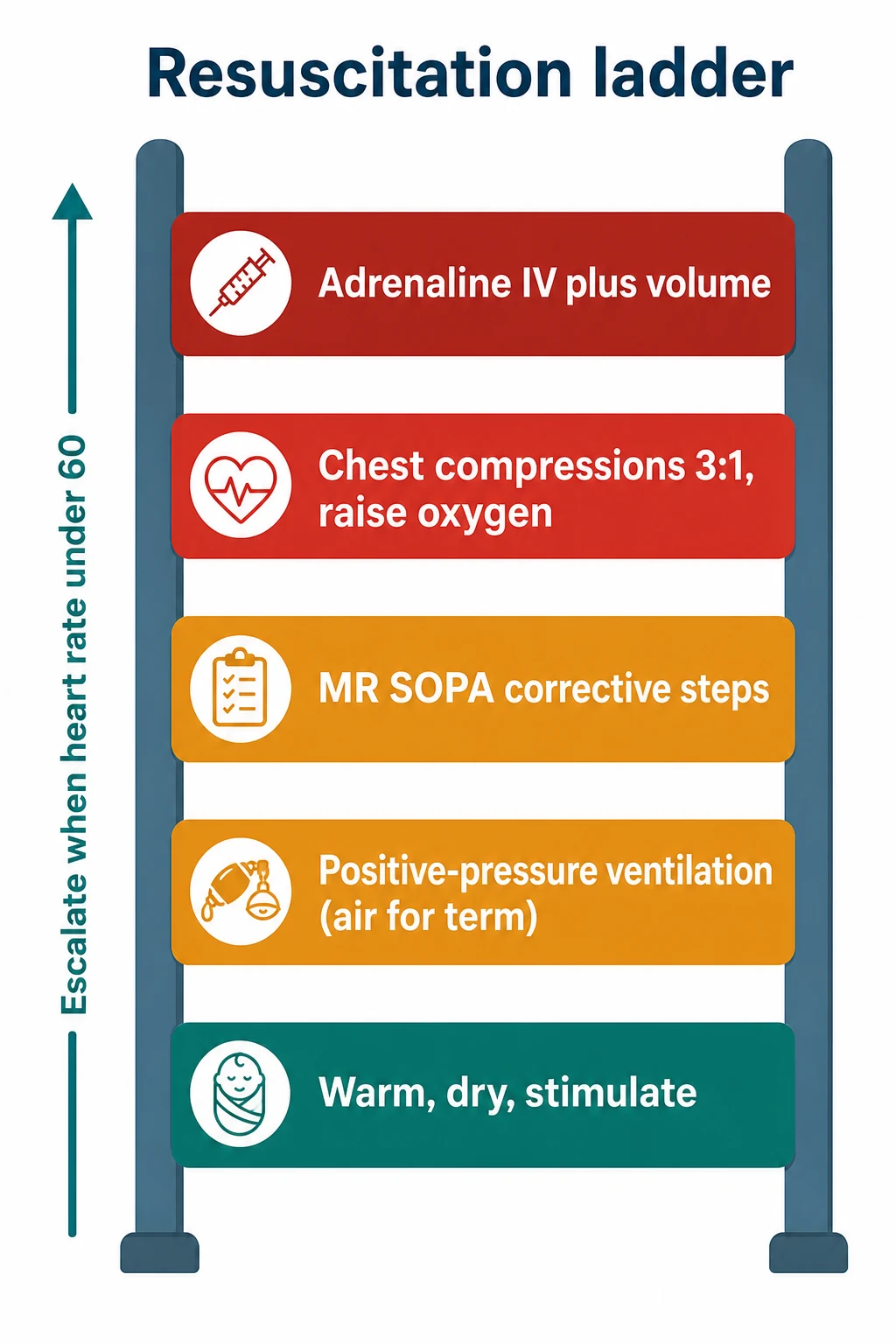
The escalation ladder
Warm, dry, stimulate; assess tone, breathing and heart rate (first 60 seconds)
Start positive-pressure ventilation if apnoeic, gasping, or heart rate under 100 (air for term)
Apply MR SOPA corrective steps if chest is not rising or heart rate not improving
Add chest compressions 3:1 and raise oxygen if heart rate under 60 despite effective ventilation
Give intravenous adrenaline (and consider volume) if heart rate remains under 60
Reassess every 60 seconds; de-escalate as the heart rate recovers
Management — Definitive & Stepwise
Adrenaline is given when the heart rate remains under 60 despite effective ventilation with coordinated compressions. Give 0.01 to 0.03 mg per kilogram (that is 0.1 to 0.3 mL per kilogram of the 1:10,000 concentration) by the intravenous route, ideally through an umbilical venous catheter, and repeat every three to five minutes. The endotracheal route is no longer recommended as a reliable alternative because absorption is variable — if it is used as a stopgap while intravenous access is obtained, the dose is higher (0.05 to 0.1 mg per kilogram), but intravenous is the standard. [1] [4]
Adrenaline (epinephrine) 1:10,000
Dose
0.01–0.03 mg/kg (= 0.1–0.3 mL/kg of the 1:10,000 solution) intravenously; repeat every 3–5 minutes
Volume expansion is reserved for suspected hypovolaemia — acute blood loss, pallor, poor perfusion, or a weak pulse after effective ventilation. Give 10 mL per kilogram of an isotonic crystalloid (normal saline or Ringer's lactate) or O-negative blood, slowly over 5 to 10 minutes and even more slowly in the preterm, because rapid boluses can cause intraventricular haemorrhage. Do not give volume routinely to an asphyxiated infant who is not hypovolaemic. [1]
Temperature is a treatment, not comfort. Aim for 36.5 to 37.5 degrees Celsius from the moment of birth. Use a radiant warmer, warm towels, a hat, and plastic wrap and an exothermic thermal mattress for infants under about 32 weeks. Avoid both hypothermia and hyperthermia — the latter is associated with worsened brain injury. Admission temperature is one of the strongest predictors of outcome and should be audited on every resuscitation. [1] [2]
Glucose must be checked and maintained, because hypoglycaemia compounds brain injury after asphyxia. Check a blood glucose once the infant is stable and treat with enteral feeds or intravenous dextrose as needed. [1]
Therapeutic hypothermia is the one intervention proven to improve outcome after moderate or severe hypoxic-ischaemic encephalopathy. The Azzopardi TOBY trial established that cooling to 33.5 degrees for 72 hours reduces death and disability in term and near-term infants. Refer any infant of 36 weeks gestation or more with moderate or severe encephalopathy to a cooling centre within six hours of birth — the clock starts at birth, not at the decision. Do not start uncontrolled cooling locally; maintain normothermia and transfer. [9]
In Australia and New Zealand, refer to your regional neonatal retrieval service and follow the ANZNN cooling-network criteria for gestational age, encephalopathy grade and aEEG. Maintain normothermia in transit; the cooling centre initiates and controls therapeutic hypothermia.
[1]Specific Subtypes & Scenarios
The extremely preterm infant (under 28 weeks) needs a planned team, a plastic bag and thermal mattress applied without drying, gentle ventilation with PEEP and low oxygen (start 21 to 30%), a low threshold for early surfactant, and a policy on cord management settled before delivery. Every extra minute hypothermic worsens outcome, so the thermoregulation choreography is rehearsed in advance. [1] [6]
The non-vigorous infant born through meconium-stained liquor is no longer routinely intubated and suctioned — the 2015 change removed routine tracheal suction for non-vigorous infants because it delayed ventilation without benefit. Resuscitate per the standard algorithm: if not breathing, start positive-pressure ventilation. [1] [4]
Suspected congenital diaphragmatic hernia or airway anomaly is anticipated antenatally and met by a team ready to intubate and ventilate gently, avoiding the mask if possible, with a nasogastric tube to decompress the stomach. A baby who cannot be ventilated by mask should move quickly to intubation or a laryngeal mask airway. [2]
The infant of a diabetic mother is resuscitated as usual but watched for early hypoglycaemia, which is predictable and must be screened and treated. Maternal opioid exposure within four hours of birth may depress respiration; the answer is effective ventilation, not naloxone, which is no longer part of routine resuscitation. [1]
Acute blood loss at birth — vasa praevia, cord rupture, or twin-to-twin transfusion — presents with pallor and poor perfusion rather than cyanosis, and needs volume, often O-negative blood, alongside ventilation. Out-of-hospital or ward births demand the same first 60 seconds with whatever equipment exists: warmth, drying, stimulation, and air ventilation by mask are the irreducible core, with early call for retrieval. [2]
Complications & Pitfalls
The biggest pitfall is treating the wrong problem. Escalating to compressions and adrenaline before ventilation is effective is the classic error — most non-responding newborns simply need better ventilation, fixed by MR SOPA. The heart rate that does not rise is far more often a mask-seal or airway problem than a heart problem. [1] [10]
Oxygen harm cuts both ways. Too little oxygen in an infant who genuinely needs it worsens hypoxic injury; too much oxygen, especially in the preterm, causes oxidative injury and retinopathy, and the NeOProM trials set the evidence for targeting saturations rather than maximising them. Volutrauma and air leak come from excessive ventilatory pressure, prevented by using the lowest pressure that gives gentle chest rise and by adding PEEP judiciously in the preterm. [1] [8]
Adrenaline errors are dose errors: the wrong concentration (1:1,000 instead of 1:10,000), the wrong route, or a decimal slip in the mL-per-kilogram calculation. The defence is to know that the resuscitation dose is 0.1 to 0.3 mL per kilogram of 1:10,000, to draw it up in advance for high-risk deliveries, and to give it intravenously. Hypothermia and hyperthermia after resuscitation both worsen brain injury — hold the narrow normothermic band and refer for controlled cooling rather than over- or under-shooting. [1]
Team failures — unclear leadership, role overlap, no timekeeper, no closed-loop communication — are as dangerous as any clinical mistake and are why pre-delivery role allocation and post-event debrief matter. [10]
Prognosis & Disposition
Outcome after neonatal resuscitation is driven by how long and how severely the infant was asphyxiated, by gestational age, and by how quickly effective ventilation restored the circulation. An infant who recovers within a minute or two, stays normothermic and normoglycaemic, and shows no encephalopathy can often stay with or near the mother with observation. An infant who needed advanced resuscitation, who is preterm, or who develops signs of encephalopathy is admitted to the neonatal unit. [1] [9]
The single most important prognostic fork is whether moderate or severe hypoxic-ischaemic encephalopathy develops in an infant of 36 weeks or more. If it does, therapeutic hypothermia within six hours reduces death and disability, and the window is unforgiving. Surveillance after resuscitation watches for seizures, encephalopathy, feeding difficulty and glucose instability, with neurodevelopmental follow-up for any infant who needed significant resuscitation. [9]
A deteriorating infant who cannot be stabilised locally is retrieved to a higher-level centre by a neonatal retrieval team, with normothermia and ventilation maintained in transit. The family is informed honestly and early about what happened and what the outlook is, and offered follow-up. [2]
First ten minutes and the hours that follow
Special Populations
The extremely preterm infant (under 28 weeks) is the population that consumes most neonatal resuscitation skill and where technique matters most: a rehearsed team, immediate thermal protection in a plastic bag without drying, low starting oxygen titrated to the saturation nomogram, gentle ventilation with PEEP and the lowest effective pressure, early surfactant, and a planned cord-management decision. Cord management in this group is contentious — deferred cord clamping is supported for stable preterm infants, but intact cord milking is not recommended under 28 weeks after Katheria's trial showed an excess of severe intraventricular haemorrhage. [1] [6] [7]
The growth-restricted or asphyxiated term infant may have chronic hypoxia and is at high risk of encephalopathy and hypoglycaemia; resuscitate per algorithm and watch closely for cooling criteria. Anticipated congenital anomalies get a tailored plan decided before delivery — an airway team for a known airway malformation, a diaphragmatic-hernia pathway, a prostaglandin plan for suspected duct-dependent cardiac disease. [2]
In low-resource and out-of-hospital settings, the irreducible core is warmth, drying, stimulation, and air ventilation by mask — these alone save most newborns, and the skill must travel with the clinician. Maternal substance use changes the response: opioid-exposed infants need effective ventilation, not naloxone, and may need ongoing monitoring for withdrawal. Multiple births may need more than one resuscitation team and equipment set, planned in advance. Infants of diabetic mothers are resuscitated as usual but screened for predictable early hypoglycaemia. [1] [2]
Evidence, Guidelines & Regional Differences
The AHA 2020 neonatal resuscitation guideline is the current North American standard, aligned with the NRP 8th edition, and the ERC 2021 newborn resuscitation guideline is the European standard. The two agree on the fundamentals — warmth, the first-minute assessment, ventilation-first, the heart-rate ladder, air for term and low oxygen for preterm, deferred cord clamping, and the abandonment of routine meconium suction. Where they differ is usually in the fine print of ventilation technique and the oxygen ladder, and candidates should know both and name the source. [1] [2]
The ILCOR consensus underpins both, weighing the evidence on each question. On starting oxygen, the evidence supports air for term infants and 21 to 30% for preterm infants under 35 weeks, titrated to the saturation nomogram, informed by the NeOProM trials of oxygen targeting in extremely preterm infants. On cord management, Cochrane reviews support deferred clamping for both term and preterm infants who do not need immediate resuscitation, while Katheria's trial showed intact cord milking should not be used under 28 weeks. [4] [5] [6] [7] [8]
TOBY (Azzopardi 2009, NEJM)
Population: Term and near-term infants with moderate-severe perinatal asphyxial encephalopathy
Key finding
Reduced death and severe neurodevelopmental disability at 18 months
Practice change
Therapeutic hypothermia is the standard of care for eligible infants; refer within the 6-hour window
Controversies and active questions remain: the optimal starting oxygen for the preterm, the role of sustained inflation, the place of intact cord milking between 28 and 34 weeks, the endotracheal adrenaline question, and how best to deliver resuscitation in low-resource settings. Answer with the current guideline, name the source, and acknowledge where the evidence is still moving. [1] [2]
Exam Pearls
- About 10% of newborns need some help; about 1% need advanced resuscitation. [1]
- The three first-minute questions: term, good tone, breathing or crying. [1]
- Ventilation is the core act — inadequate ventilation is the commonest reason a newborn fails to transition. [10]
- PPV: 40 to 60 breaths per minute, air for term, 21 to 30% for preterm under 35 weeks. [1] [8]
- Compressions: heart rate under 60 despite effective ventilation; ratio 3:1; two-thumb technique. [1]
- Adrenaline: 0.01 to 0.03 mg per kilogram IV (0.1 to 0.3 mL per kilogram of 1:10,000). [1]
- Volume: 10 mL per kilogram isotonic crystalloid or O-negative blood for hypovolaemia. [1]
- Target SpO2: 60 to 65% at 1 minute, 80 to 85% at 5 minutes, 85 to 95% at 10 minutes. [1]
- Temperature: 36.5 to 37.5 degrees — both hypothermia and hyperthermia worsen brain injury. [2]
- No routine intubation or suction for non-vigorous meconium infants — resuscitate per algorithm. [1] [4]
- No intact cord milking under 28 weeks — excess severe IVH in Katheria's trial. [7]
- Cooling for moderate-severe HIE at 36+ weeks within 6 hours — the TOBY legacy. [9]
References
- [1]Aziz K Part 5: Neonatal Resuscitation 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Pediatrics, 2021.PMID 33087555
- [2]Madar J European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation, 2021.PMID 33773829
- [3]Wyllie J European Resuscitation Council Guidelines for Resuscitation 2015: Section 7. Resuscitation and support of transition of babies at birth. Resuscitation, 2015.PMID 26477415
- [4]Perlman JM Part 7: Neonatal Resuscitation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation, 2015.PMID 26472855
- [5]McDonald SJ Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database Syst Rev, 2013.PMID 23843134
- [6]Duley L Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst Rev, 2019.PMID 31529790
- [7]Katheria A Association of Umbilical Cord Milking vs Delayed Umbilical Cord Clamping With Death or Severe Intraventricular Hemorrhage Among Preterm Infants. JAMA, 2019.PMID 31742630
- [8]Askie LM Association Between Oxygen Saturation Targeting and Death or Disability in Extremely Preterm Infants in the Neonatal Oxygenation Prospective Meta-analysis Collaboration. JAMA, 2018.PMID 29872859
- [9]Azzopardi DV Moderate hypothermia to treat perinatal asphyxial encephalopathy. N Engl J Med, 2009.PMID 19797281
- [10]Niles DE Incidence and characteristics of positive pressure ventilation delivered to newborns in a US tertiary academic hospital. Resuscitation, 2017.PMID 28411062
- [11]Hoyle ES Quality improvement programme to increase the rate of deferred cord clamping at preterm birth using the Lifestart trolley. Arch Dis Child Fetal Neonatal Ed, 2020.PMID 32350065