Paeds · fetal-neonatal-and-perinatal
Neonatal seizures and encephalopathy
Also known as Neonatal seizures and encephalopathy · Neonatal seizures · Neonatal encephalopathy · Hypoxic-ischaemic encephalopathy with seizures
Fellowship guide to neonatal seizures and encephalopathy: recognition, EEG-based classification, the excitotoxic cascade, the aetiological differential, the antiseizure-medication ladder and therapeutic hypothermia.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A neonatal seizure is the clinical or electrographic expression of abnormal, excessive neuronal discharge in the immature brain occurring within the first 28 days of life. Unlike seizures in older children, the great majority are provoked — they are an acute symptom of an underlying brain insult, not a manifestation of epilepsy — which is why the decisive clinical task is not to stop the movements but to find and treat the cause. [5]
Neonatal encephalopathy is the broader term for a disturbance of neurological function in the newborn: altered consciousness, abnormal tone, depressed or absent reflexes, autonomic dysfunction, feeding difficulty, and (often) seizures. Hypoxic-ischaemic encephalopathy (HIE) is the commonest cause of neonatal encephalopathy and the commonest provocation for neonatal seizures, so the two are deeply linked — an encephalopathic infant must be observed for seizures, and a seizing infant must be assessed for encephalopathy and its cause. [5] [10]
Classification
Neonatal seizures are best classified on two axes at once: by the relationship between the clinical event and the EEG, and by the underlying aetiology. The EEG-clinical axis matters because most seizures in the NICU have no visible clinical correlate, and the aetiology axis matters because the cause — not the seizure itself — drives treatment and prognosis. [5] [8]
By EEG-clinical correlation there are three categories. An electroclinical seizure has both a clinical sign and a simultaneous EEG ictal change — this is the textbook seizure, but it is the minority in the NICU. An electrographic-only (subclinical) seizure has an EEG ictal pattern but no outward clinical sign — this is the commonest type, and the reason continuous EEG is essential. A clinical-only (nonelectrographic) event is a motor or behavioural phenomenon with no EEG correlate — this is usually non-seizure motor behaviour (jitteriness, myoclonus) and should not be treated with escalating antiseizure drugs. [5] [8]
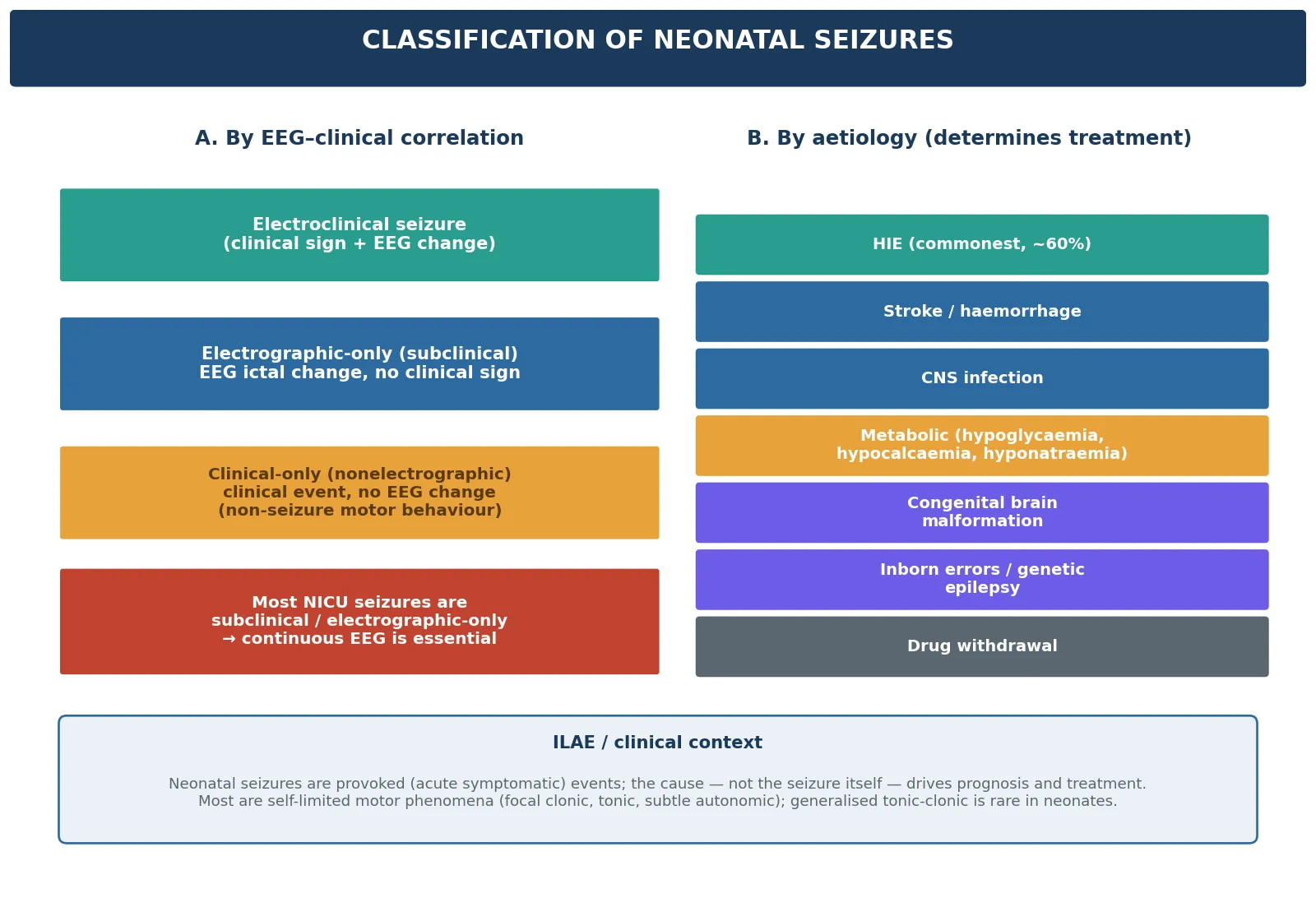
Clinically, neonatal seizures are described by their semiology. Focal clonic (repetitive, rhythmic jerking of a limb or face) and focal tonic (sustained posturing) are the most reliably epileptic. Myoclonic, subtle (orofacial-buccal, ocular, cycling or swimming movements) and autonomic (apnoea, tachycardia, desaturation, blood pressure swings) are harder to identify clinically. Generalised tonic-clonic seizures are rare in neonates — the immature brain cannot synchronise a hemisphere-wide discharge — and a reported "generalised tonic-clonic" in a newborn should prompt the question of whether the event was a seizure at all. [5]
Epidemiology & Risk Factors
Neonatal seizures occur in roughly 1 to 3 per 1000 live births in term infants and far more frequently in preterm infants, in whom incidence may reach 1 in 10 to 1 in 20 of very-low-birthweight admissions. The epidemiology is dominated by gestation and by the perinatal context: seizures are more common, more often subclinical, and carry a worse outcome in the preterm brain. [5]
Hypoxic-ischaemic encephalopathy is the single commonest cause, accounting for around half to two-thirds of neonatal seizures in most series, followed by cerebral infarction (arterial or sinovenous stroke), intracranial haemorrhage (intraventricular, subdural, subarachnoid), central nervous system infection, and metabolic derangements. [5] [10]
Key risk factors stratify by mechanism. For HIE the determinants are perinatal asphyxia (cord prolapse, placental abruption, uterine rupture, tight nuchal cord), low Apgar scores, cord blood acidosis (pH under 7.0 or base deficit of 12 mmol/L or more), and the need for resuscitation. For stroke the risks include maternal thrombophilia, chorioamnionitis, instrumental delivery and polycythaemia. For infection the risks are prolonged rupture of membranes, maternal group B streptococcal colonisation, chorioamnionitis, and maternal HSV. Metabolic causes cluster in infants of diabetic mothers (hypoglycaemia), preterm infants (hypocalcaemia, hyponatraemia), and those with inborn errors. [5] [10]
Pathophysiology
The unifying pathophysiology of HIE-related neonatal seizures is the excitotoxic cascade. Perinatal hypoxia-ischaemia depletes cellular ATP, which disables the sodium-potassium pump and the membrane reuptake mechanisms; neurones depolarise, release glutamate, and over-stimulate NMDA and AMPA receptors. The result is a massive influx of calcium and sodium into the cell, which both generates the hyperexcitability we recognise as a seizure and activates downstream injury pathways (mitochondrial calcium overload, oxidative stress, apoptosis and necrosis). [5]
The cascade has a temporal structure that is the whole rationale for therapeutic hypothermia. After the primary hypoxic-ischaemic insult there is a partial recovery — the latent phase, lasting roughly 6 to 48 hours — followed by a secondary energy failure in which mitochondrial dysfunction, excitotoxicity and inflammation drive a wave of secondary neuronal death. This window, between the insult and the secondary cascade, is the therapeutic target: cooling the brain to 33.5 to 34.5 °C within the first 6 hours of life slows metabolism and interrupts the cascade. [1] [3]
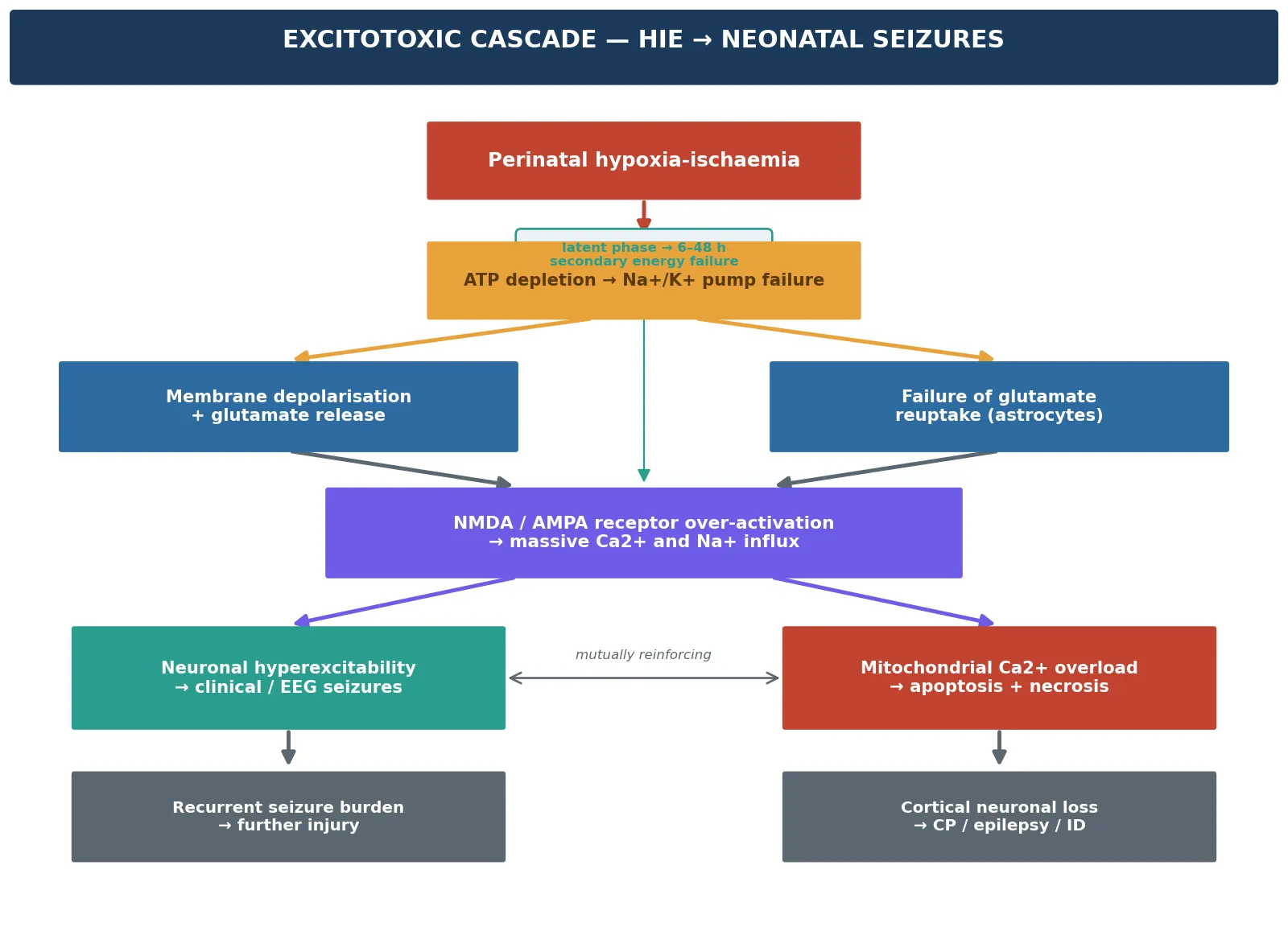
Seizures are not merely a symptom of this injury — they amplify it. Each electrographic seizure consumes energy the injured brain cannot spare, propagates glutamate release, and extends the area of secondary damage. This is why seizure burden (the cumulative electrographic seizure load over time) independently predicts adverse neurodevelopmental outcome, even after controlling for the severity of HIE. The clinical implication is direct: detect and treat seizures to an electrographic endpoint, because subclinical seizures left untreated continue to injure the brain. [9] [10]
Clinical Presentation
The clinical presentation of a neonatal seizure is notoriously difficult to recognise at the bedside, because the immature brain produces focal and fragmentary phenomena rather than the dramatic convulsions of older children. A focal clonic seizure — repetitive, rhythmic jerking of one limb or one side of the face that cannot be stopped by gentle restraint or repositioning — is the most reliably epileptic sign. Focal tonic posturing, myoclonic jerks, and subtle phenomena (eyelid fluttering, oral-buccal movements, cycling or swimming limb movements, apnoea) are harder to identify. [5]
The cardinal distinction the examiner rewards is seizure versus jitteriness. Jitteriness is a tremor: fast, rhythmic, stimulus-sensitive, abolished by holding the affected limb flexed, and not accompanied by ocular or autonomic phenomena. A seizure is slower, not stimulus-sensitive, persists despite restraint, and is often accompanied by eye deviation, apnoea or autonomic change. Confusing the two is the commonest bedside error — jitteriness is over-treated with antiseizure drugs and true seizures are missed. [5]
The presentation of encephalopathy itself is graded by the Sarnat score, which combines mental state, muscle tone, reflexes and autonomic function. Sarnat stage 1 (mild) shows hyperexcitability and mild hypotonia with preserved reflexes; stage 2 (moderate) shows lethargy, hypotonia, and depressed reflexes with seizures common; stage 3 (severe) shows stupor or coma, flaccid tone, and absent reflexes. The Sarnat stage at presentation is one of the criteria for cooling eligibility (moderate, stage 2, and severe, stage 3). [1] [5]
Differential Diagnosis
The differential of abnormal movements in a neonate splits into two questions. First, is the movement a seizure at all? Second, if it is, what is the cause? Answering the first prevents over-treatment of non-epileptic motor phenomena; answering the second is the whole point, because each cause has a different, specific treatment. [5]
Non-seizure motor phenomena include jitteriness (the commonest mimic), benign neonatal sleep myoclonus (brief myoclonic jerks confined to sleep, stopping on waking), hyperekplexia (startle-induced hypertonia), opisthotonus (cerebral or metabolic), Sandifer syndrome (oesophageal reflux-related posturing), and drug-induced dyskinesia. These share the feature of having no EEG correlate, and the response is reassurance or treatment of the underlying condition, not antiseizure drugs. [5]
Within the metabolic causes, hypoglycaemia (glucose under 2.6 mmol/L) is the fastest to find and the fastest to reverse; hypocalcaemia (ionised calcium under 1.0 mmol/L), hypomagnesaemia, and hyponatraemia are next. Inborn errors of metabolism (ammonia, lactate, amino acids) and pyridoxine- or pyridoxal-phosphate-dependent seizures present with refractory seizures that respond to specific cofactors. Genetic epilepsies — benign familial neonatal seizures (KCNQ2/3) and self-limited neonatal seizures — present with a positive family history and a well-looking infant between events. [5]
Clinical & Bedside Assessment
Bedside assessment proceeds in two layers: an immediate ABC stabilisation and a focused neurological examination that refines the cause. Stabilisation comes first — maintain the airway, give oxygen and ventilate if apnoeic, secure intravenous access, and check the blood glucose at once, because hypoglycaemia is the fastest reversible provocation. The focused neurological examination then quantifies the encephalopathy. [5]
The neurological examination assesses consciousness (alert, lethargic, stupor, coma), tone (axial and appendicular, hypotonia or hypertonia), the primitive reflexes (Moro, grasp, suck, galant), cranial nerves, the anterior fontanelle (bulging suggests raised intracranial pressure or haemorrhage), and the head circumference. A formal Sarnat stage is assigned to grade encephalopathy severity, because moderate (stage 2) and severe (stage 3) HIE are the cooling-eligible groups. [1] [5]
The focused history captures the elements that reweight the aetiological differential: the perinatal course and any asphyxia event; cord blood gases and Apgar scores; maternal infection, prolonged rupture of membranes, and HSV status; maternal diabetes; delivery mode and trauma; a family history of seizures, metabolic disease or consanguinity; and any antenatally diagnosed anomaly. Each of these points toward one cause and away from another, and directs the first-hour investigation bundle. [5]
Investigations
Investigations confirm the diagnosis, quantify the seizure burden, and find the cause. Continuous video-EEG is the gold standard for seizure detection and for guiding treatment to an electrographic endpoint, because most NICU seizures are subclinical. The American Clinical Neurophysiology Society guideline recommends continuous EEG for any infant with a suspected seizure or at high risk (HIE being cooled, on extracorporeal support, with intracranial haemorrhage), continued for at least 24 hours after the last electrographic seizure. [8]
Where continuous conventional EEG is not immediately available, amplitude-integrated EEG (aEEG) is a reasonable bedside screening tool: it tracks background activity and flags suspected seizures, though it misses some focal and low-amplitude events. The aEEG background pattern also carries prognostic weight — a flat or suppressed background that fails to recover after HIE predicts adverse outcome and post-neonatal epilepsy. [9]
The metabolic and infective work-up runs in parallel with EEG. The immediate bedside tests are blood glucose, then calcium (ionised), magnesium, sodium, blood gas and lactate. The broader panel adds ammonia, liver function, and full blood count. A septic screen — blood culture, C-reactive protein, and a lumbar puncture (cell count, protein, glucose, culture, and HSV PCR) — is performed whenever infection is plausible. Imaging is directed by the suspected cause: cranial ultrasound for intraventricular haemorrhage and major structural lesions; MRI for stroke, the HIE injury pattern (basal ganglia, thalamic, watershed infarction), and malformations. [5] [8]
Management — Resuscitation
Resuscitation of the seizing neonate follows the ABCDE framework with two neonatal-specific priorities: the airway and breathing first, and the blood glucose immediately. Maintain the airway in a neutral position, give oxygen and ventilate if the infant is apnoeic or gasping, secure intravenous or intraosseous access, and check the capillary or heel-prick glucose without delay. [5]
If the glucose is low (under 2.6 mmol/L), give a bolus of 10% dextrose 2 mL/kg intravenously and start a maintenance dextrose infusion. If the infant is encephalopathic with perinatal asphyxia, assess Sarnat stage at once and activate the cooling pathway if stage 2 or 3 — the 6-hour window closes whether or not the seizures are controlled. The first-line antiseizure medication is given while the cause is sought, not after. [1] [5]
Immediate management of the suspected neonatal seizure
Airway, breathing, oxygen; ventilate if apnoeic
Check blood glucose at once — treat hypoglycaemia with 10% dextrose 2 mL/kg IV
Secure IV access; send glucose, Ca2+, Mg2+, Na+, blood gas, cultures
Give first-line antiseizure medication: phenobarbital 20 mg/kg IV
Start continuous video-EEG to confirm and guide treatment
Assess Sarnat stage; activate cooling for moderate–severe HIE within 6 h
Lumbar puncture and cranial imaging once stable; aciclovir if HSV plausible
Management — Definitive & Stepwise
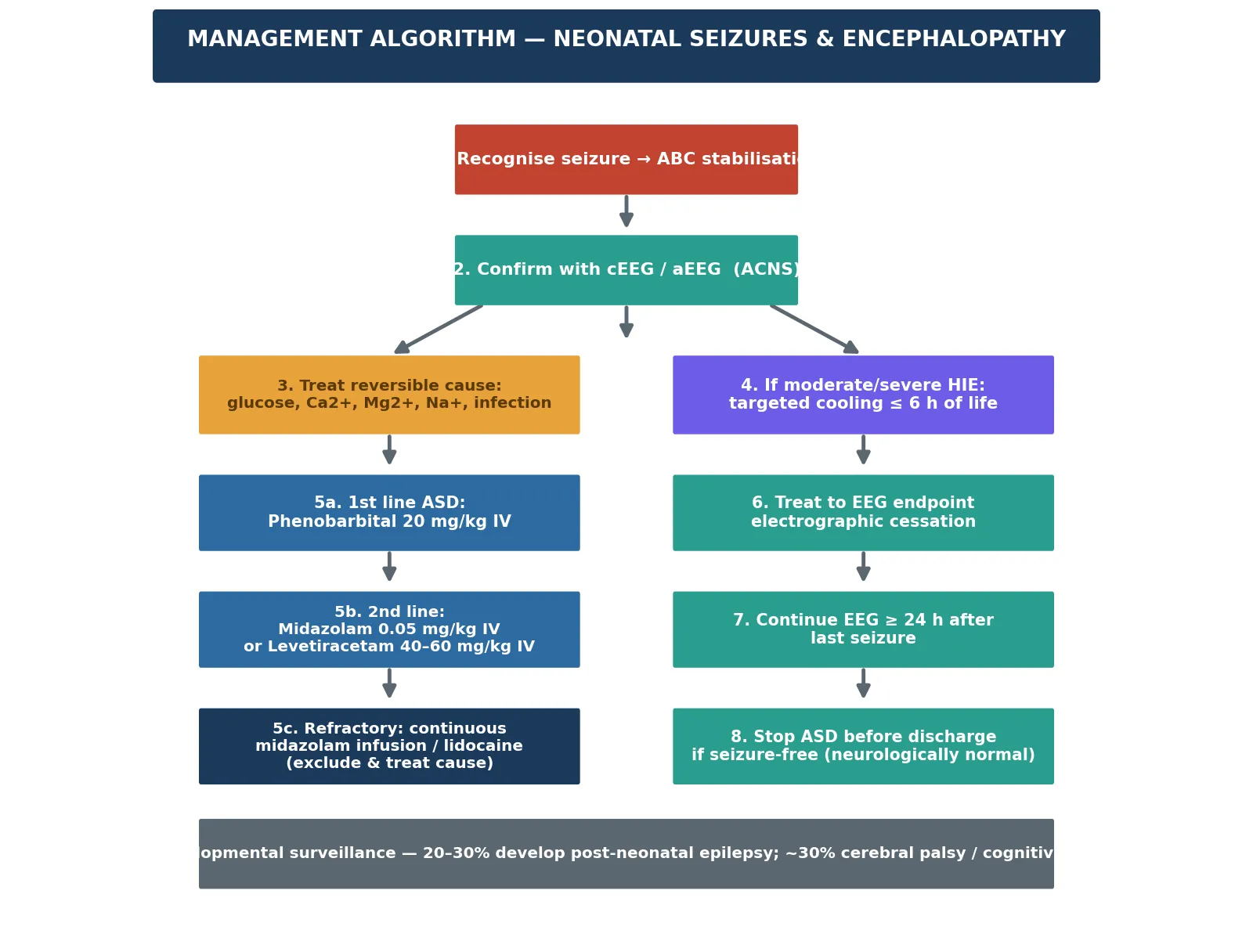
Definitive management is layered: treat the cause, give neuroprotection for HIE, and apply the antiseizure-medication ladder to an EEG endpoint. The cause-specific treatments — dextrose for hypoglycaemia, calcium or magnesium for electrolyte derangement, antibiotics and aciclovir for infection — are given as soon as the abnormality is identified, because they are more effective than any antiseizure drug when the seizure is metabolically driven. [5]
The antiseazure-medication ladder begins with phenobarbital 20 mg/kg intravenously over 10 to 20 minutes as the first-line agent, the traditional and most widely used choice. The Painter 1999 NEJM trial established that phenobarbital and phenytoin have similar (and modest) efficacy — each achieving complete electroclinical cessation in only about 45 to 50 percent of infants — which is why the modern ladder escalates rather than relies on a single drug. [4] [5]
If seizures persist after the loading dose, the second-line options are a second phenobarbital bolus (to a total of 40 mg/kg), intravenous midazolam 0.05 mg/kg, or levetiracetam 40 to 60 mg/kg intravenously. The Sharpe 2020 randomised trial found phenobarbital superior to levetiracetam (Sharpe 2020 failed non-inferiority; LEV inferior for electrographic cessation) as a first-line agent for short-term electrographic seizure reduction, and levetiracetam is increasingly used because of its favourable safety profile — but phenobarbital remains the consensus first choice in the 2023 ILAE Task Force recommendations, reflecting equipoise rather than certainty. [5] [6] [7]
[1]For refractory seizures, a continuous midazolam infusion or, in some centres, a lidocaine infusion is used, while the search for a treatable cause continues — especially a metabolic or structural lesion, since a refractory seizure in a neonate often signals an identifiable and treatable provocation. The 2023 Abiramalatha Cochrane review highlights the genuine uncertainty: no single agent has been proven superior, and the evidence base for the ladder is weaker than clinical practice implies. [5] [6]
In Australia, New Zealand and the United Kingdom, therapeutic hypothermia is the standard of care for term (at least 36 weeks) infants with moderate (Sarnat 2) or severe (Sarnat 3) HIE, started within 6 hours of life at a target of 33.5 to 34.5 °C for 72 hours. Eligibility typically requires a combination of cord or early blood gas acidosis (pH under 7.0 or base deficit at least 12 mmol/L) or an Apgar history of perinatal asphyxia, plus encephalopathy and/or an abnormal aEEG. Cooling is maintained during retrieval, and rewarming is slow (0.5 °C per hour). [1] [2] [3]
The duration of antiseizure medication is deliberately short in most infants. In the neurologically normal infant with a clear provoked cause (for example, hypoglycaemia or a single brief HIE-related seizure), the antiseizure drug is stopped before discharge, because prolonged prophylaxis does not prevent post-neonatal epilepsy and may worsen the neurodevelopmental outcome. Infants with ongoing neurological abnormality, an abnormal MRI, or a confirmed epilepsy syndrome are maintained on therapy and followed in a neurology clinic. [5]
Specific Subtypes & Scenarios
[1]The term infant with HIE is the central scenario, because it is the commonest and the one where the clock matters most. Once moderate or severe HIE is recognised and cooling is started within 6 hours, seizures are detected and treated to an EEG endpoint with phenobarbital first-line, escalating as needed. The TOBY and NICHD trials established that cooling reduces death and major disability, and the Jacobs 2013 Cochrane meta-analysis confirmed the pooled benefit — so the question in this scenario is never whether to cool an eligible infant, but how fast. [1] [2] [3]
The preterm infant with seizures and intraventricular haemorrhage is a different problem. The preterm brain's vulnerability is the germinal matrix and the periventricular white matter, not the cortex; seizures are more often subclinical, antiseizure-drug pharmacokinetics are altered by immature hepatic metabolism and a large volume of distribution, and the differential includes metabolic derangements and sepsis as much as haemorrhage. The principle is the same — find and treat the cause, confirm with EEG, treat to an endpoint — but the threshold for imaging and metabolic screening is lower and the drug doses are adjusted for weight and gestation. [5]
The infant with suspected metabolic disease is the refractory-seizure scenario that examiners probe. Seizures that do not respond to the first-line ladder demand a re-screen for a metabolic cause: re-check glucose, ionised calcium, magnesium, sodium, ammonia, lactate and blood gas. A trial of pyridoxine (vitamin B6) or pyridoxal-phosphate is considered in refractory cases, and inborn errors of metabolism (amino acids, organic acids, urea cycle) are excluded. The lesson is that a refractory neonatal seizure is often a missed cause, not a drug failure. [5]
Complications & Pitfalls
The complications of neonatal seizures are neurological, and they are driven by seizure burden and by the underlying cause. Post-neonatal epilepsy develops in roughly 20 to 30 percent of infants after HIE-related seizures; cerebral palsy, cognitive impairment and learning difficulties occur in a similar proportion, concentrated in infants with severe HIE, a high seizure burden, or an abnormal MRI pattern. The Basti 2020 and Nyman 2022 studies quantify this: higher seizure burden and a poor aEEG background recovery each independently predict worse outcome. [9] [10]
The complications of therapeutic hypothermia are predictable and managed proactively: sinus bradycardia (common, benign, not an indication to rewarm), thrombocytopenia and coagulopathy (monitor and correct), pulmonary hypertension (screen with pre/post-ductal saturations), and subcutaneous fat necrosis (a self-limiting calcinosis that can cause late hypercalcaemia in the weeks after cooling). Rewarming must be slow — 0.5 °C per hour — to avoid seizures and hypotension. [1] [3]
Prognosis & Disposition
Prognosis is determined by the underlying cause, the seizure burden, and the speed of effective neuroprotection — not by the number of clinical seizures. HIE-related seizures carry the heaviest burden: even with cooling, roughly a quarter to a third of infants with moderate-to-severe HIE develop cerebral palsy, cognitive impairment or epilepsy, and cooling reduces this risk by an absolute difference of around 10 to 15 percent in death or major disability. [1] [2] [3]
Metabolic and infective causes carry a variable prognosis — excellent when the derangement is corrected quickly (hypoglycaemia, hypocalcaemia), guarded when the injury is established (severe HSV encephalitis). Genetic self-limited epilepsies (benign familial neonatal seizures) carry a favourable prognosis, with seizures remitting and development usually normal, though a slightly higher risk of later epilepsy. [5]
Disposition follows severity. Any actively seizing or encephalopathic infant is admitted to a neonatal intensive care unit; infants undergoing cooling are managed in (or retrieved to) a tertiary NICU with continuous EEG and neurology support. After discharge, all infants with HIE-related seizures, a high seizure burden, or an abnormal MRI enter a structured neurodevelopmental surveillance programme, because early detection of cerebral palsy and epilepsy enables early intervention. [9] [10]
Special Populations
The extremely preterm infant is a high-risk group: seizures are more often subclinical, the brain's vulnerability is the germinal matrix and periventricular white matter rather than the cortex, and antiseizure-drug pharmacokinetics are altered by immature hepatic metabolism and a large volume of distribution. The principle — find the cause, confirm with EEG, treat to an endpoint — is unchanged, but doses are weight- and gestation-adjusted, and the threshold for cranial ultrasound and metabolic screening is lower. [5]
The infant with a suspected inborn error of metabolism presents the refractory-seizure problem. Ammonia, lactate, amino acids and organic acids are checked; a trial of pyridoxine or pyridoxal-phosphate is considered when seizures are refractory; and specific dietary and cofactor treatments (glucose, arginine, pyridoxine, biotin) are given once the lesion is identified. The key is that a refractory neonatal seizure is often a missed metabolic cause, not a drug ladder to climb. [5]
The infant with congenital heart disease faces perioperative seizures from hypoxic-ischaemic injury, thromboembolic stroke, or the effects of cardiopulmonary bypass; the approach is the same, with the added complexity that the cardiac lesion constrains fluid and drug choices. Late-preterm and rural or remote infants raise retrieval considerations: cooling must be initiated and maintained during transport to a tertiary centre, because the 6-hour window does not pause for geography. [1] [5]
Evidence, Guidelines & Regional Differences
The evidence base for neonatal seizures and encephalopathy is mature on neuroprotection and weaker on the choice of antiseizure drug. The landmark cooling trials — TOBY (Azzopardi 2009), the NICHD whole-body hypothermia trial (Shankaran 2005), and the Jacobs 2013 Cochrane meta-analysis — established that cooling term infants with moderate-to-severe HIE within 6 hours of life at 33.5 to 34.5 °C for 72 hours reduces death and major disability, and cooling is now the global standard of care. [1] [2] [3]
The antiseizure-medication evidence is more equivocal. The Painter 1999 NEJM trial found phenobarbital and phenytoin each achieved complete cessation in only about 45 to 50 percent of infants — a humbling result that underpins the modern escalating ladder. The Sharpe 2020 randomised trial found phenobarbital superior to levetiracetam (Sharpe 2020 failed non-inferiority; LEV inferior for electrographic cessation) as first-line therapy for short-term electrographic seizure reduction, and the 2023 Abiramalatha Cochrane review found no single agent proven superior, so the 2023 ILAE Task Force consensus recommends phenobarbital as the traditional first choice while acknowledging genuine equipoise. [4] [5] [6] [7]
The ACNS 2011 continuous-EEG guideline is the foundation for detection and monitoring: continuous EEG is recommended for any infant with a suspected seizure or at high risk (cooling HIE, ECMO, intracranial haemorrhage), continued for at least 24 hours after the last electrographic seizure, because clinical observation alone misses most NICU seizures. [8]
Across ANZ, the UK, Europe and North America, phenobarbital remains the consensus first-line antiseizure drug for neonatal seizures, with levetiracetam increasingly used as a well-tolerated second-line or alternative first-line agent. Some centres have moved to levetiracetam first-line on the strength of its safety profile and the Sharpe 2020 non-inferiority result; the 2023 ILAE Task Force and the Abiramalatha Cochrane review both acknowledge this equipoise. Local protocol should be followed; the evidence does not mandate a single first agent. [5] [6] [7]
Exam Pearls
Causes of neonatal seizures — 'The fits baby'
References
- [1]Azzopardi DV; Strohm B; Edwards AD; Dyet L; Halliday HL; Juszczak E; Kapellou O; Levene M; Marlow N; Porter E; et al Moderate hypothermia to treat perinatal asphyxial encephalopathy. N Engl J Med, 2009.PMID 19797281
- [2]Shankaran S; Laptook AR; Ehrenkranz RA; Tyson JE; McDonald SA; Donovan EF; Fanaroff AA; Poole WK; Wright LL; Higgins RD; et al Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med, 2005.PMID 16221780
- [3]Jacobs SE; Berg M; Hunt R; Tarnow-Mordi WO; Inder TE; Davis PG Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev, 2013.PMID 23440789
- [4]Painter MJ; Scher MS; Stein AD; Armatti S; Wang J; Alvin JD Phenobarbital compared with phenytoin for the treatment of neonatal seizures. N Engl J Med, 1999.PMID 10441604
- [5]Pressler RM; Abend NS; Auvin S; Boylan G; Cilio MR; Hellström-Westas L; Hsieh DT; Islam MP; Karvelas G; Lakra M; et al Treatment of seizures in the neonate: Guidelines and consensus-based recommendations-Special report from the ILAE Task Force on Neonatal Seizures. Epilepsia, 2023.PMID 37655702
- [6]Abiramalatha T; Thanigainathan S; Ramaswamy VV; Gupta VK, Shephalya R; Mammen A; Sujatha S Anti-seizure medications for neonates with seizures. Cochrane Database Syst Rev, 2023.PMID 37873971
- [7]Sharpe C; Reiner GE; Davis SL; Garcia M; Hardjec K; Ip K; Jiang P; Lai YC; Legido A; Molinaro M; et al Levetiracetam Versus Phenobarbital for Neonatal Seizures: A Randomized Controlled Trial. Pediatrics, 2020.PMID 32385134
- [8]Shellhaas RA; Chang T; Tsuchida T; Scher MS; Riviello JJ; Abend NS; Nguyen S; Wusthoff CJ; Clancy RR The American Clinical Neurophysiology Society's Guideline on Continuous Electroencephalography Monitoring in Neonates. J Clin Neurophysiol, 2011.PMID 22146359
- [9]Nyman J; Mikkonen K; Metsäranta M; Stefanovic V; Wallin-Lundqvist E; Glinianaia SV; Toiviainen-Salo S; Vanhatalo S; Hallberg B; Hellström-Westas L Poor aEEG background recovery after perinatal hypoxic ischemic encephalopathy predicts postneonatal epilepsy by age 4 years. Clin Neurophysiol, 2022.PMID 36183624
- [10]Basti C; Maranella E; Cimini N; Pianetti A; Agostinelli R; Ciavarra C; Dani C Seizure burden and neurodevelopmental outcome in newborns with hypoxic-ischemic encephalopathy treated with therapeutic hypothermia: A single center observational study. Seizure, 2020.PMID 33160202