Paeds · fetal-neonatal-and-perinatal
Neonatal stroke and intracranial haemorrhage
Also known as Neonatal stroke and intracranial haemorrhage · Perinatal arterial ischaemic stroke · Neonatal intraventricular haemorrhage · Neonatal haemorrhagic stroke · Cerebral sinovenous thrombosis in the neonate
Fellowship guide to neonatal stroke and intracranial haemorrhage: perinatal arterial ischaemic stroke, cerebral sinovenous thrombosis, germinal matrix-IVH and neonatal haemorrhagic stroke, their pathophysiology, MRI-based diagnosis, Papile grading, PHVD management and neurodevelopmental prognosis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A neonate who presents with a focal seizure, hand-preference, or unexplained encephalopathy may have sustained a cerebrovascular injury around the time of birth. The 2007 NICHD-NINDS workshop defined perinatal stroke as a group of cerebrovascular events occurring between 20 weeks of fetal life and 28 days postnatal, and it distinguished several distinct entities that share a narrow time window but differ in mechanism, vessel involvement, and outcome. [1]
Perinatal arterial ischaemic stroke (PAIS) is a focal arterial infarction of the brain confirmed by neuroimaging, occurring in the perinatal period and producing a focal neurological deficit or seizures. Cerebral sinovenous thrombosis (CSVT) is thrombosis of the cerebral venous sinuses or deep veins. Neonatal haemorrhagic stroke is a non-traumatic, intracranial haemorrhage — subdural, subarachnoid, parenchymal or intraventricular — that produces acute neurological dysfunction. [1] [2]
In the preterm infant, the dominant cerebrovascular lesion is germinal matrix-intraventricular haemorrhage (GMH-IVH), originating in the fragile capillary bed of the subependymal germinal matrix, with potential extension into the ventricle and the periventricular white matter. This entity, graded by the Papile system, carries its own pathophysiology and its own principal complication — post-haemorrhagic ventricular dilation (PHVD). [4] [5]
Classification
Neonatal cerebrovascular injury is classified along two axes: the vessel involved (arterial versus venous) and the tissue effect (ischaemia versus haemorrhage). This framework matters because each entity has a different aetiology, imaging signature, management pathway, and prognostic implication. [1]
The ischaemic group includes perinatal arterial ischaemic stroke — a focal arterial territory infarction, most commonly involving the left middle cerebral artery — and cerebral sinovenous thrombosis, which may produce venous infarction with or without haemorrhagic conversion. The haemorrhagic group includes germinal matrix-intraventricular haemorrhage (predominantly preterm), extra-axial bleeds (subdural and subarachnoid, often related to birth trauma or coagulopathy in term infants), and parenchymal or cerebellar haemorrhage. [1] [4]
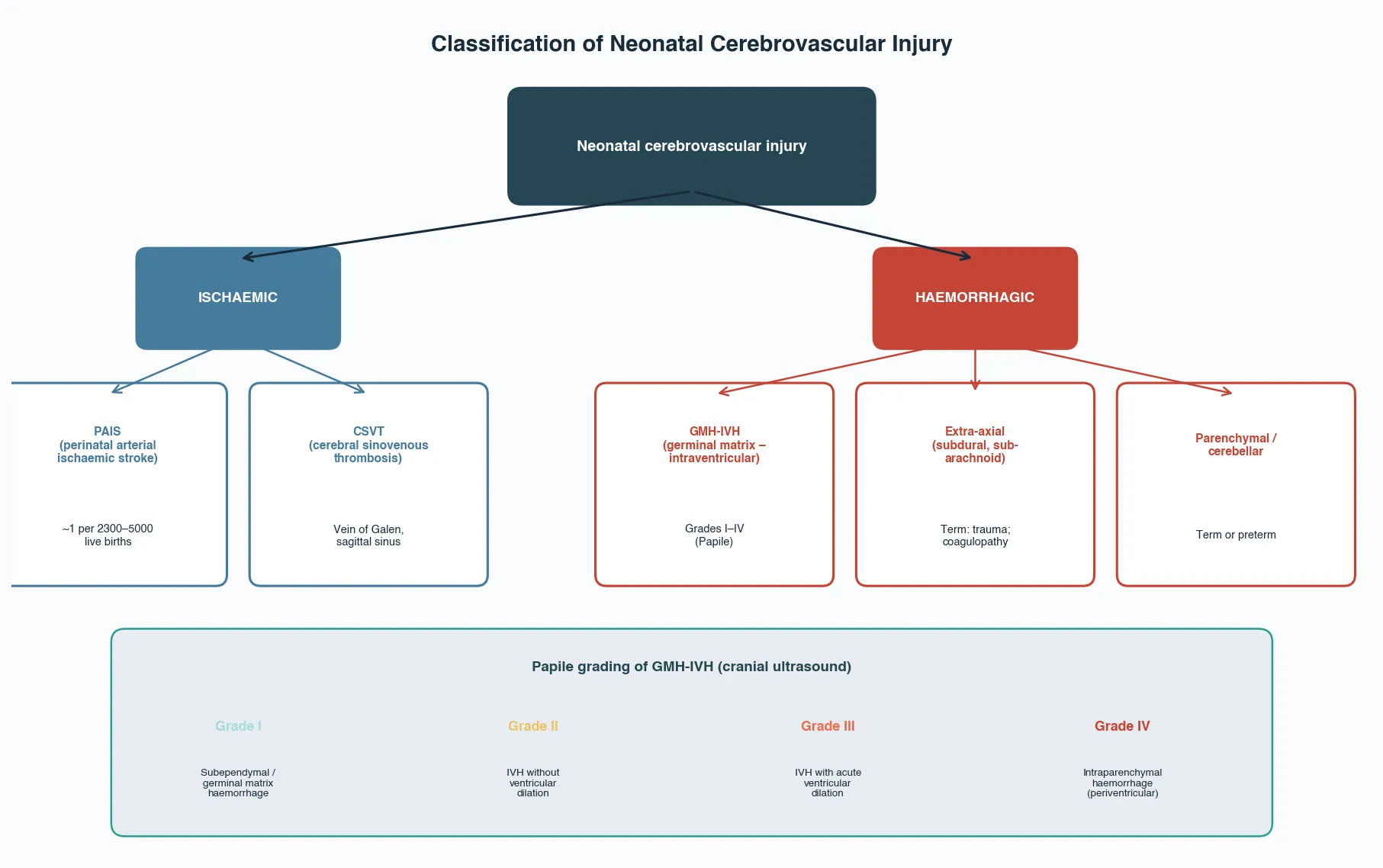
Germinal matrix-IVH is graded using the Papile system, which is applied on cranial ultrasound. Grade I is a subependymal germinal matrix haemorrhage confined to the caudothalamic groove. Grade II is intraventricular haemorrhage without ventricular dilation. Grade III is intraventricular haemorrhage with acute ventricular dilation. Grade IV — now understood as a periventricular haemorrhagic infarction from venous obstruction rather than simple extension — is parenchymal haemorrhage adjacent to the ventricle. [4] [5]
[4]Epidemiology & Risk Factors
Perinatal arterial ischaemic stroke occurs in approximately 1 per 2300 to 1 per 5000 live births, making it one of the most common focal causes of neonatal seizures and the leading identified cause of hemiplegic cerebral palsy in term infants. Neonatal haemorrhagic stroke is less common, with a population incidence estimated at roughly 1 in 9500 live births for pure haemorrhagic stroke and 1 in 6300 including haemorrhagic infarction. [1] [2]
Germinal matrix-IVH is overwhelmingly a disease of prematurity. Among very-low-birthweight infants (under 1500 g) the incidence reaches 20 to 25 percent in most series, with the highest rates in the most immature infants. The germinal matrix involutes after 32 weeks, which is why GMH-IVH is rare in term infants. [4]
For PAIS, risk factors cluster around the peripartum period: instrumental or emergency delivery, prolonged second stage, cord abnormalities (nuchal cord, true knot), maternal thrombophilia, chorioamnionitis, birth asphyxia, polycythaemia, and dehydration. However, in many infants no single cause is found — PAIS is often multifactorial, with a complex interplay of maternal, placental, intrapartum, and neonatal prothrombotic conditions. [1] [3]
For neonatal haemorrhagic stroke, risk factors include birth trauma (vacuum, forceps, difficult delivery), coagulation disorders (vitamin K deficiency, haemophilia, thrombocytopenia), and vascular malformations. For GMH-IVH, the risks are those of extreme prematurity itself: the fragile germinal matrix vasculature, pressure-passive cerebral circulation, fluctuating blood pressure, respiratory distress, pneumothorax, and acidosis. [2] [4]
Pathophysiology
The ischaemic and haemorrhagic entities share a developing brain but differ fundamentally in mechanism. PAIS results from arterial occlusion — most often an embolus or thrombus in a major cerebral artery, frequently the left middle cerebral artery. The resulting focal infarct triggers an excitotoxic cascade identical in principle to that of hypoxic-ischaemic injury: ATP depletion, ion pump failure, glutamate-mediated calcium influx, and apoptotic or necrotic neuronal death. [1]
The immature brain has a dual vulnerability here. On one hand, the developing white matter has a rich population of pre-myelinating oligodendrocytes that are exquisitely sensitive to oxidative and excitotoxic injury. On the other, the capacity for plasticity — the un-injured hemisphere acquiring functions of the damaged one — is greater in the neonate than at any other age, which is the neurobiological basis for the sometimes-surprising functional recovery. [3]
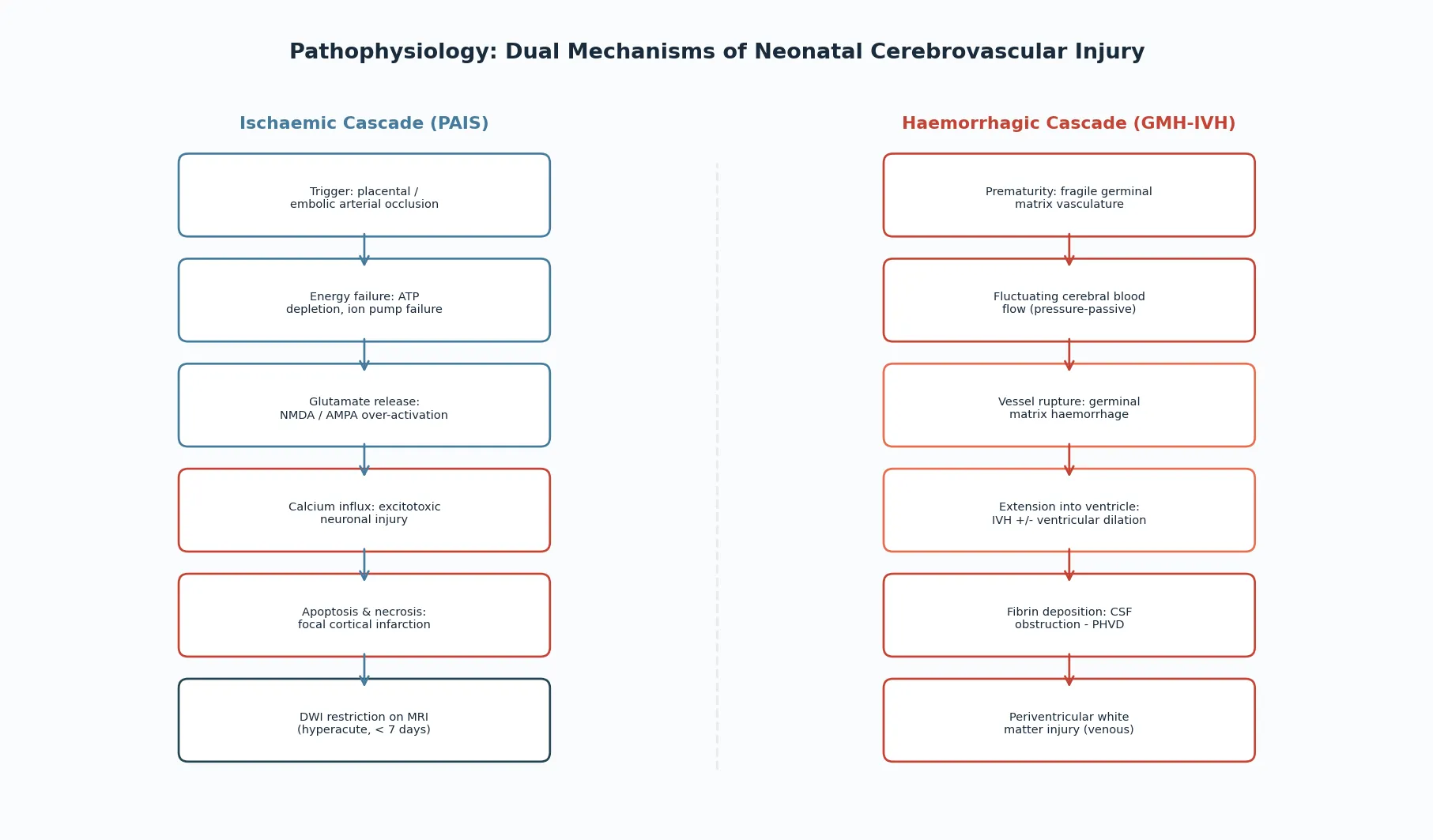
GMH-IVH arises from the germinal matrix, a highly vascularised, gelatinous tissue in the subependymal region that is the site of neuronal and glial precursor migration. The capillaries of the germinal matrix are structurally immature — they lack the autoregulatory capacity of mature cerebral vessels, making the preterm cerebral circulation pressure-passive. Fluctuations in cerebral blood flow from respiratory distress, blood pressure swings, or hypoxia-ischaemia can rupture these fragile vessels. The haemorrhage may remain in the germinal matrix (grade I), extend into the ventricle (grade II–III), or produce a periventricular haemorrhagic infarction through compression of the terminal veins (grade IV). [4]
The white matter injury that accompanies severe IVH is not merely a mass effect. Blood breakdown products are toxic to oligodendrocyte precursors, and the venous congestion caused by a parenchymal haematoma produces a venous infarction that destroys the periventricular white matter tracts. This periventricular injury — not the intraventricular blood itself — is the principal driver of the motor and cognitive outcome in grade III–IV IVH. [5]
Clinical Presentation
The clinical presentation of neonatal stroke and intracranial haemorrhage depends on the lesion type, the gestational age, and the timing of the event. A term infant with PAIS most often presents with focal seizures — typically focal clonic movements of one limb or one side of the face — in the first 24 to 72 hours of life. Some infants show hand-preference, focal tone asymmetry, or an abnormal Moro response on one side. [1] [3]
A less common but important presentation is the infant who appears well in the nursery and presents weeks later with early hand-preference or developmental asymmetry — the so-called "late-presenting" or "presumed perinatal stroke," where the infarct occurred perinatally but was not recognised acutely. These infants come to attention through surveillance for asymmetric motor development, and their imaging shows a chronic, encephalomalacic territory infarct. [1]
Preterm infants with GMH-IVH may be asymptomatic if the haemorrhage is small (grades I–II) and detected only on routine screening cranial ultrasound. Larger haemorrhages produce a sudden clinical deterioration — apnoea, pallor, hypotension, metabolic acidosis, a fall in haematocrit, and seizures — sometimes described as a catastrophic deterioration with a bulging fontanelle. [4]
Neonatal haemorrhagic stroke in a term infant presents variably: seizures, encephalopathy, irritability, poor feeding, or a bulging fontanelle. The subdural and subarachnoid bleeds associated with birth trauma may be clinically silent or may produce a self-limited seizure that resolves. A large parenchymal or posterior fossa haemorrhage may present with rapid neurological deterioration and signs of raised intracranial pressure. [2]
Differential Diagnosis
The differential diagnosis of acute neurological deterioration in a neonate is broad, and stroke and haemorrhage sit within it alongside several other serious conditions. The first question is whether the event is a seizure at all, and the second is what caused it. The cause-specific treatments differ, which is why the differential drives the investigation plan. [1]
Hypoxic-ischaemic encephalopathy is the principal mimic of PAIS in a term infant: both can produce encephalopathy and seizures, and both can coexist. HIE typically produces a more diffuse, global injury pattern with a consistent perinatal asphyxia history, while PAIS produces a focal, territory-based lesion. The distinction matters for prognosis and for the cooling decision — cooling is for moderate-to-severe HIE, not for isolated stroke. [1] [3]
[1] [2]Metabolic causes — particularly hypoglycaemia, which can produce a characteristic posterior parieto-occipital injury pattern — must be excluded because they are rapidly reversible and produce an identical clinical picture of seizures and encephalopathy. Central nervous system infection (bacterial meningitis, HSV encephalitis) can produce both seizures and haemorrhage, and structural malformations (vascular malformations, focal cortical dysplasia) may present with focal seizures. [1]
Clinical & Bedside Assessment
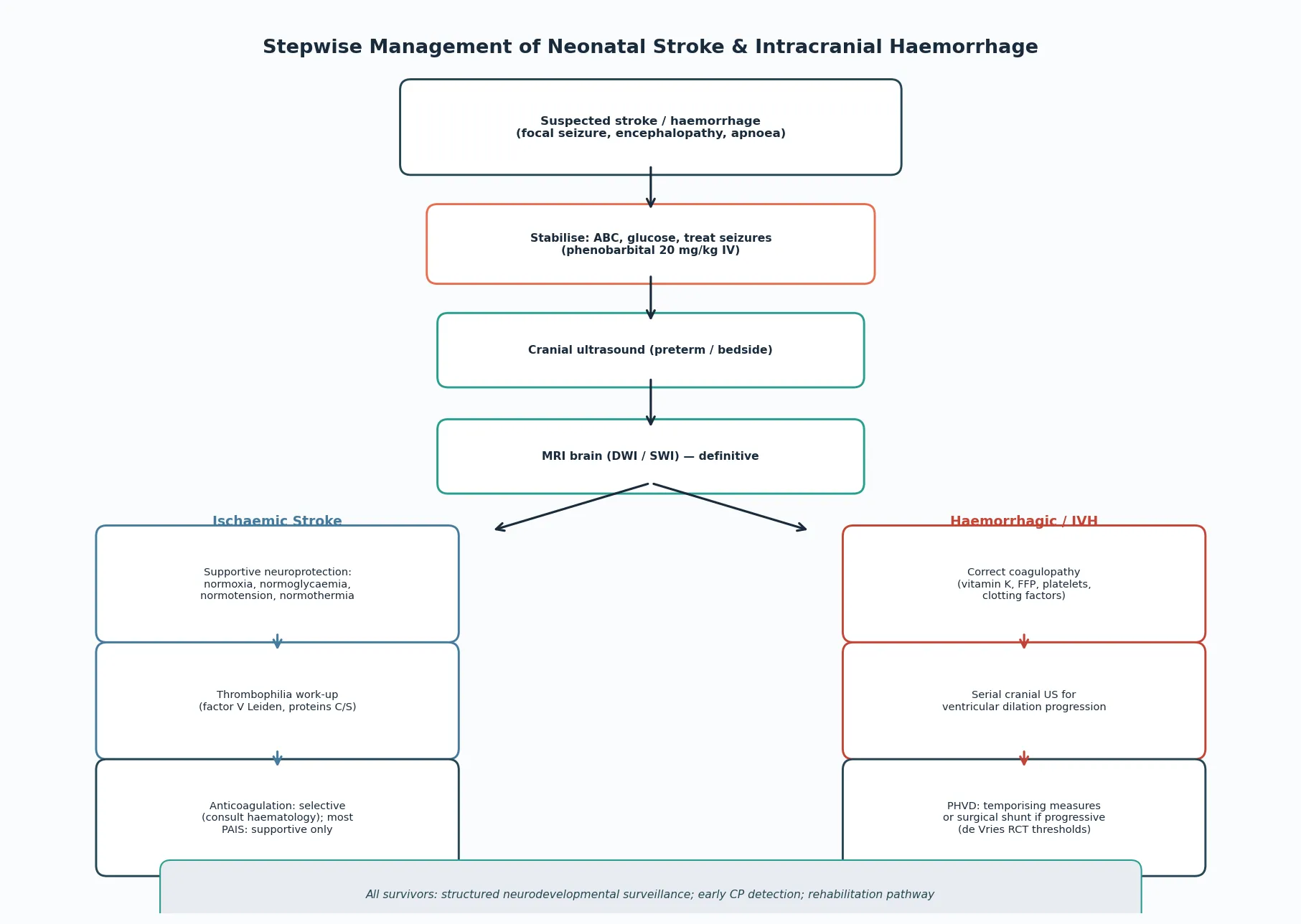
Bedside assessment follows the same two-layer structure as any neonatal neurological emergency: immediate stabilisation, then a focused neurological examination that refines the cause. Maintain the airway, give oxygen, ventilate if apnoeic, secure intravenous access, and check the blood glucose immediately. The first-line antiseizure medication — phenobarbital 20 mg/kg intravenously — is given while the cause is sought, not after. [1]
The focused neurological examination assesses consciousness level, tone (axial and appendicular), the primitive reflexes, cranial nerves, and the anterior fontanelle. A bulging fontanelle suggests raised intracranial pressure from a haemorrhage or progressive ventricular dilation. A focal neurological deficit — asymmetric tone, a hand-preference, an absent or asymmetric Moro — points toward a focal lesion such as PAIS. [1] [4]
The focused history captures the elements that reweight the differential: the perinatal course and any asphyxia, the gestational age and birthweight, the delivery mode (instrumental versus spontaneous), cord blood gases and Apgar scores, maternal thrombophilia, a family history of thrombosis or coagulopathy, and the presence of birth trauma. For the preterm infant, the history focuses on haemodynamic stability, respiratory status, and risk factors for GMH-IVH. [1] [3]
Investigations
Neuroimaging is the definitive investigation for all neonatal cerebrovascular lesions, but the modality depends on the suspected entity and the infant's stability. Cranial ultrasound is the first-line and screening tool for the preterm infant: it is portable, does not require transport, and reliably detects intraventricular haemorrhage and ventricular size. It is performed routinely in very-low-birthweight infants on days 3 to 7 of life, and repeated serially to monitor for extension and post-haemorrhagic ventricular dilation. [4] [6]
MRI is the diagnostic gold standard for PAIS, CSVT, and neonatal haemorrhagic stroke. Diffusion-weighted imaging (DWI) detects acute ischaemic injury within hours, showing restricted diffusion in the affected arterial territory. Susceptibility-weighted imaging (SWI) detects haemorrhage and venous thrombosis. MR venography confirms or excludes CSVT. In stable infants, MRI is obtained as soon as feasible; in unstable infants, cranial ultrasound is performed first and MRI is deferred until retrieval or stabilisation. [1] [3]
[1]The laboratory work-up runs in parallel with imaging. A coagulation screen — prothrombin time, activated partial thromboplastin time, fibrinogen, and platelet count — is essential, because both ischaemic and haemorrhagic stroke may reflect an underlying coagulopathy. A thrombophilia screen — factor V Leiden, prothrombin gene mutation, proteins C and S, antithrombin, lipoprotein(a) — is considered in selected cases, particularly PAIS with a family history or recurrent events. A full blood count, C-reactive protein, blood culture, and, when indicated, a lumbar puncture exclude infection. [1] [3]
Management — Resuscitation
Resuscitation of the neonate with a suspected stroke or haemorrhage follows the ABCDE framework with a neurological focus. Maintain the airway in a neutral position, give oxygen and ventilate if the infant is apnoeic, secure intravenous access, and check the blood glucose at once. Hypoglycaemia is both a mimic and a cause of neonatal seizures and must be corrected immediately with 10% dextrose 2 mL/kg intravenously. [1]
Seizures are treated with phenobarbital 20 mg/kg intravenously as first-line, with continuous EEG where available because most neonatal seizures are subclinical. The neuroprotective principle is to maintain adequate cerebral perfusion and oxygenation: correct hypoxia, hypotension, hypoglycaemia, and hyperthermia, because each of these extends the area of secondary injury. Neuroimaging is obtained in parallel, not sequentially — the MRI is arranged while the infant is stabilised, not after seizures are controlled. [1] [3]
Immediate management of suspected neonatal stroke or haemorrhage
Airway, breathing, oxygen; ventilate if apnoeic
Check blood glucose — treat hypoglycaemia with 10% dextrose 2 mL/kg IV
Secure IV access; send coagulation, FBC, glucose, cultures
Give phenobarbital 20 mg/kg IV for seizures; start continuous EEG
Obtain cranial ultrasound (preterm) or arrange MRI (term, once stable)
Maintain normoxia, normotension, normothermia, normoglycaemia
Involve neonatology and paediatric neurology early; retrieve if needed
Management — Definitive & Stepwise
Definitive management differs by entity but shares a common principle: protect the injured brain from secondary insults, treat the specific cause, and prevent complications. For PAIS the management is primarily supportive — there is no neonatal equivalent of adult thrombolysis or thrombectomy. The goal is to optimise cerebral perfusion by maintaining normoxia, normoglycaemia, normotension, and normothermia, and to treat seizures to an electrographic endpoint. [1] [3]
Anticoagulation in neonatal PAIS is selective and contentious. The decision depends on whether a prothrombotic condition, a venous thrombosis (CSVT), or a cardiac source of embolism is identified, and it requires haematology consultation. Most isolated PAIS cases are managed supportively, because the risk of haemorrhagic transformation and the lack of evidence for benefit outweigh the theoretical advantage of anticoagulation. [1]
For GMH-IVH, management aims to prevent extension and to manage the complication of post-haemorrhagic ventricular dilation. The supportive measures — gentle handling, avoiding rapid fluid or volume changes, maintaining haemodynamic stability, and avoiding fluctuations in pCO2 — are applied to all preterm infants at risk. Serial cranial ultrasound monitors for extension and for the development of PHVD. [4] [5]
Post-haemorrhagic ventricular dilation is managed in a stepwise fashion. The de Vries 2019 randomised controlled trial established treatment thresholds based on the Levene ventricular index and the anterior horn width, demonstrating that intervention at a defined threshold — rather than waiting for severe dilation — reduces the need for shunt surgery. Temporising measures include serial lumbar punctures, ventricular access devices with CSF drainage, or ventriculosubgaleal shunts. If PHVD progresses despite temporising measures, a permanent ventriculoperitoneal shunt is placed. [6]
[6]In Australia, New Zealand and the United Kingdom, the management of neonatal stroke is guided by the RCPCH stroke guideline and the Australian clinical consensus guideline for subacute rehabilitation (Greenham 2021). For PAIS, supportive neuroprotection is the standard of care, and anticoagulation is reserved for confirmed prothrombotic conditions or CSVT under haematology guidance. For GMH-IVH and PHVD, the de Vries 2019 RCT thresholds for intervention are increasingly adopted in tertiary neonatal units, and all very-low-birthweight infants receive routine cranial ultrasound screening. [1] [6] [8]
Specific Subtypes & Scenarios
The term infant with focal seizures on day 2 is the central scenario. The most likely diagnosis is PAIS, and the first task is to obtain an MRI with DWI to confirm the arterial territory infarct, exclude HIE, and evaluate for CSVT. Management is supportive neuroprotection with seizure control. The thrombophilia work-up is selective, and the family is counselled about the risk of hemiplegic cerebral palsy and the role of early developmental surveillance. [1] [3]
The extremely preterm infant with grade III–IV IVH is the high-risk scenario. The immediate task is serial cranial ultrasound to grade the haemorrhage and monitor for extension. The principle is that the periventricular white matter injury — not the intraventricular blood — drives outcome, so management focuses on preventing PHVD and its secondary white matter damage. The de Vries 2019 RCT thresholds guide intervention, and the family is counselled about the high risk of cerebral palsy and cognitive impairment. [4] [6]
Cerebellar haemorrhage in the preterm infant is a scenario that examiners probe. Small cerebellar haemorrhages, increasingly detected with advanced cranial ultrasound and MRI, may be clinically silent or may produce subtle motor and cognitive deficits. Steggerda and colleagues found that perinatal and postnatal factors (prematurity, ventilation, fluctuations in haemodynamics) are associated with these lesions, and that outcome is influenced by the size and location of the haemorrhage. [7]
[1] [6]Cerebral sinovenous thrombosis is the must-not-miss venous entity. It may present with seizures, encephalopathy, or an unexplained intracranial haemorrhage (a haemorrhagic infarct in a non-arterial distribution should raise suspicion). MR venography confirms the diagnosis, and management includes optimisation of hydration and haemodynamics, treatment of seizures, and — in many centres — anticoagulation under haematology guidance, because untreated CSVT can propagate and produce extensive venous infarction. [1]
Complications & Pitfalls
The complications of neonatal stroke and intracranial haemorrhage are neurological and are driven by the size, location, and type of the lesion. The Baak 2023 systematic review and meta-analysis established that the principal early predictors of adverse neurodevelopment after PAIS are the size of the infarct, the involvement of the corticospinal tract, the presence of seizures, and the severity of the neurological examination at presentation. Hemiplegic cerebral palsy develops in roughly 30 to 60 percent of PAIS survivors. [3]
For GMH-IVH, the complications are driven by the grade. Grades I–II generally carry a favourable outcome, while grades III–IV carry a high risk of cerebral palsy, cognitive impairment, and epilepsy. The mechanism of the grade IV injury — venous infarction of the periventricular white matter — explains why the motor outcome is often a spastic diplegia or quadriplegia, because the periventricular white matter carries the corticospinal tracts. Post-haemorrhagic ventricular dilation is itself a complication that amplifies the white matter injury. [4] [5]
Prognosis & Disposition
Prognosis is determined by the lesion type, size, and location, and by the effectiveness of secondary brain protection — not by the number of clinical seizures. For PAIS, the Baak 2023 meta-analysis quantified the outcome: roughly 30 to 60 percent of survivors develop hemiplegic cerebral palsy, with cognitive impairment, epilepsy, and behavioural difficulties in a substantial subset. The predictors of worse outcome are a larger infarct, corticospinal tract involvement, bilateral lesions, and early severe neurological signs. [3]
For GMH-IVH, the Papile grade is the principal prognostic variable. Grades I–II carry a generally favourable prognosis — most infants do well, though there is a slightly increased risk of milder neurodevelopmental problems. Grades III–IV carry a high risk of major neurodevelopmental impairment: cerebral palsy, cognitive impairment, visual impairment, and epilepsy. The presence and severity of PHVD and of periventricular white matter injury independently predict outcome beyond the grade itself. [4] [5]
Disposition follows severity. Any infant with an acute stroke or significant haemorrhage is admitted to a neonatal intensive care unit; infants requiring MRI or specialist neurology input are managed in (or retrieved to) a tertiary centre. After discharge, all survivors enter a structured neurodevelopmental surveillance programme — the Australian clinical consensus guideline (Greenham 2021) outlines the subacute rehabilitation pathway — because early detection of cerebral palsy and cognitive impairment enables early intervention. [3] [8]
Special Populations
The extremely preterm infant is the highest-risk population. The germinal matrix is most vascular and most fragile below 28 weeks, the cerebral circulation is most pressure-passive, and the comorbidities of extreme prematurity (respiratory distress, haemodynamic instability, acidosis) amplify the risk of GMH-IVH. The threshold for routine cranial ultrasound screening is lowest here, and the threshold for PHVD monitoring is lowest for the highest grades. [4]
The infant with a confirmed prothrombotic condition requires coordinated management with haematology. Anticoagulation decisions are individualised — the risk of recurrence is weighed against the risk of haemorrhagic transformation, and management is under specialist guidance. The family is counselled about the implications for future pregnancies and siblings. [1] [3]
The infant with presumed perinatal stroke — presenting weeks to months after birth with early hand-preference — enters the same developmental surveillance pathway, but the counselling shifts from acute management to early intervention, because the lesion is already chronic. Early detection of hemiplegic cerebral palsy, constraint-induced movement therapy, and multidisciplinary rehabilitation improve functional outcomes. [3] [8]
Evidence, Guidelines & Regional Differences
The evidence base for neonatal stroke has matured over the past two decades but remains observational for many management decisions. The 2007 NICHD-NINDS workshop (Raju) established the definitional and classification framework for perinatal stroke that still underpins clinical practice and research. The Cole 2017 population-based case-control study quantified the epidemiology of neonatal haemorrhagic stroke, establishing an incidence of roughly 1 in 9500 live births and identifying risk factors including birth trauma and coagulopathy. [1] [2]
The Baak 2023 systematic review and meta-analysis synthesised the early predictors of neurodevelopment after PAIS, establishing that infarct size, corticospinal tract involvement, and early neurological severity are the most consistent prognostic factors across cohorts. The Wagenaar 2025 study reported 2-year safety and neurodevelopmental data for intranasal mesenchymal stromal cells after PAIS — a novel therapeutic direction that remains experimental but represents the shift toward regenerative neuroprotection. [3] [9]
For GMH-IVH, Ballabh's 2010 review established the mechanism of disease, and the 2021 Ballabh and de Vries review in Nature Reviews Neurology synthesised the mechanisms of white matter injury in IVH — the venous infarction paradigm for grade IV and the toxicity of blood breakdown products to oligodendrocyte precursors. The de Vries 2019 randomised controlled trial provided the evidence base for intervention thresholds in post-haemorrhagic ventricular dilation. [4] [5] [6]
Across ANZ, the UK and North America, cranial ultrasound is the standard screening tool for GMH-IVH in very-low-birthweight infants, with MRI as the diagnostic standard for PAIS. The de Vries 2019 RCT thresholds for PHVD intervention are increasingly adopted in tertiary neonatal units across these regions. The Australian clinical consensus guideline (Greenham 2021) provides the rehabilitation pathway for childhood stroke survivors. There is no consensus on routine anticoagulation for isolated PAIS; practice varies by centre and is guided by haematology consultation and the identification of a prothrombotic condition. [1] [6] [8]
Exam Pearls
Causes and risk factors — 'STROKE BABE'
References
- [1]Raju TN; Nelson KB; Ferriero D; Lynch JK Ischemic perinatal stroke: summary of a workshop sponsored by the National Institute of Child Health and Human Development and the National Institute of Neurological Disorders and Stroke. Pediatrics, 2007.PMID 17766535
- [2]Cole L; Dewey D; Letourneau N; Kaplan BJ; Chaput K; Gallagher C; Husein M; Mackie M; Mohammed N; Yager JY; et al Clinical Characteristics, Risk Factors, and Outcomes Associated With Neonatal Hemorrhagic Stroke: A Population-Based Case-Control Study. JAMA Pediatr, 2017.PMID 28114647
- [3]Baak LM; van der Aa NE; Verhagen AAE; Dudink J; Groenendaal F Early predictors of neurodevelopment after perinatal arterial ischemic stroke: a systematic review and meta-analysis. Pediatr Res, 2023.PMID 36575364
- [4]Ballabh P Intraventricular hemorrhage in premature infants: mechanism of disease. Pediatr Res, 2010.PMID 19816235
- [5]Ballabh P; de Vries LS White matter injury in infants with intraventricular haemorrhage: mechanisms and therapies. Nat Rev Neurol, 2021.PMID 33504979
- [6]de Vries LS; Groenendaal F; Liem KD; Heep A; Brouwer MJ; 't Hooft L; van Haastert IC; de Kort GA; Wilbrandus BH; Benders MJ; et al Treatment thresholds for intervention in posthaemorrhagic ventricular dilation: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed, 2019.PMID 29440132
- [7]Steggerda SJ; De Bruïne FT; van den Berg-Huysmans AA; Rijken M; Leijser LM; Walther FJ; van Wezel-Meijler G Small cerebellar hemorrhage in preterm infants: perinatal and postnatal factors and outcome. Cerebellum, 2013.PMID 23653170
- [8]Greenham M; Knight S; Rodda J; Scheinberg A; Anderson V; Mackay MT Australian clinical consensus guideline for the subacute rehabilitation of childhood stroke. Int J Stroke, 2021.PMID 32691701
- [9]Wagenaar N; Baak LM; van der Aa NE; Groenendaal F; Dudink J Perinatal Arterial Stroke Treated With Stromal Cells Intranasally: 2-Year Safety and Neurodevelopment. Stroke, 2025.PMID 40654084