Paeds · fetal-neonatal-and-perinatal
Parenteral nutrition in neonates
Also known as Neonatal parenteral nutrition · Neonatal PN · Total parenteral nutrition in the newborn · Intravenous nutrition for preterm infants · Parenteral amino acid and lipid therapy in neonates
Fellowship guide to parenteral nutrition in neonates: why the preterm newborn faces a catabolic crisis if starved, the composition and advancement of the PN admixture (amino acids, glucose, lipid), central versus peripheral access, the monitoring schedule, the stepwise transition to enteral feeding, and the complications — catheter sepsis, PN-associated cholestasis (IFALD), metabolic derangement and refeeding — that define safe practice.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a 26-week infant weighing 780 g on day one of life, an umbilical venous catheter in place, the gut too immature to absorb the calories and protein the brain needs to grow. The clinical question is not whether to feed intravenously, but how fast, how much, and how to do it without infecting the line or injuring the liver. [2]
Parenteral nutrition is the intravenous delivery of macronutrients (amino acids, glucose and lipid), micronutrients (electrolytes, trace elements and vitamins) and fluid to an infant whose enteral route is absent, inadequate or unsafe. In neonatology it is most often a transitional bridge that carries the preterm or surgical newborn from the transplacental nutrition of fetal life to full enteral feeding, and only occasionally a long-term therapy for the infant with intestinal failure. [2]
The reason PN exists as a discipline is the newborn's extreme vulnerability to starvation. Most glycogen, fat and protein stores are deposited in the third trimester, so the very preterm infant is born with the smallest reserve at the highest metabolic demand. [7] The fetal accretion rate of 3.5 to 4 g/kg/day of protein is the most anabolic period of human life; failing to match it metabolically produces negative nitrogen balance, albumin fall, glucose instability and a measurable loss of brain and somatic growth that does not fully recover. Early amino acid delivery is therefore not a convenience but a developmental necessity. [4]
So the examiner's first question is always the same: when, how much, and for how long — and how do you protect the baby from the treatment while you give it? That question drives every prescription. [3]
Classification
Begin with the route, then the indication, then the timing, because each axis changes the prescription and the risk. [2]
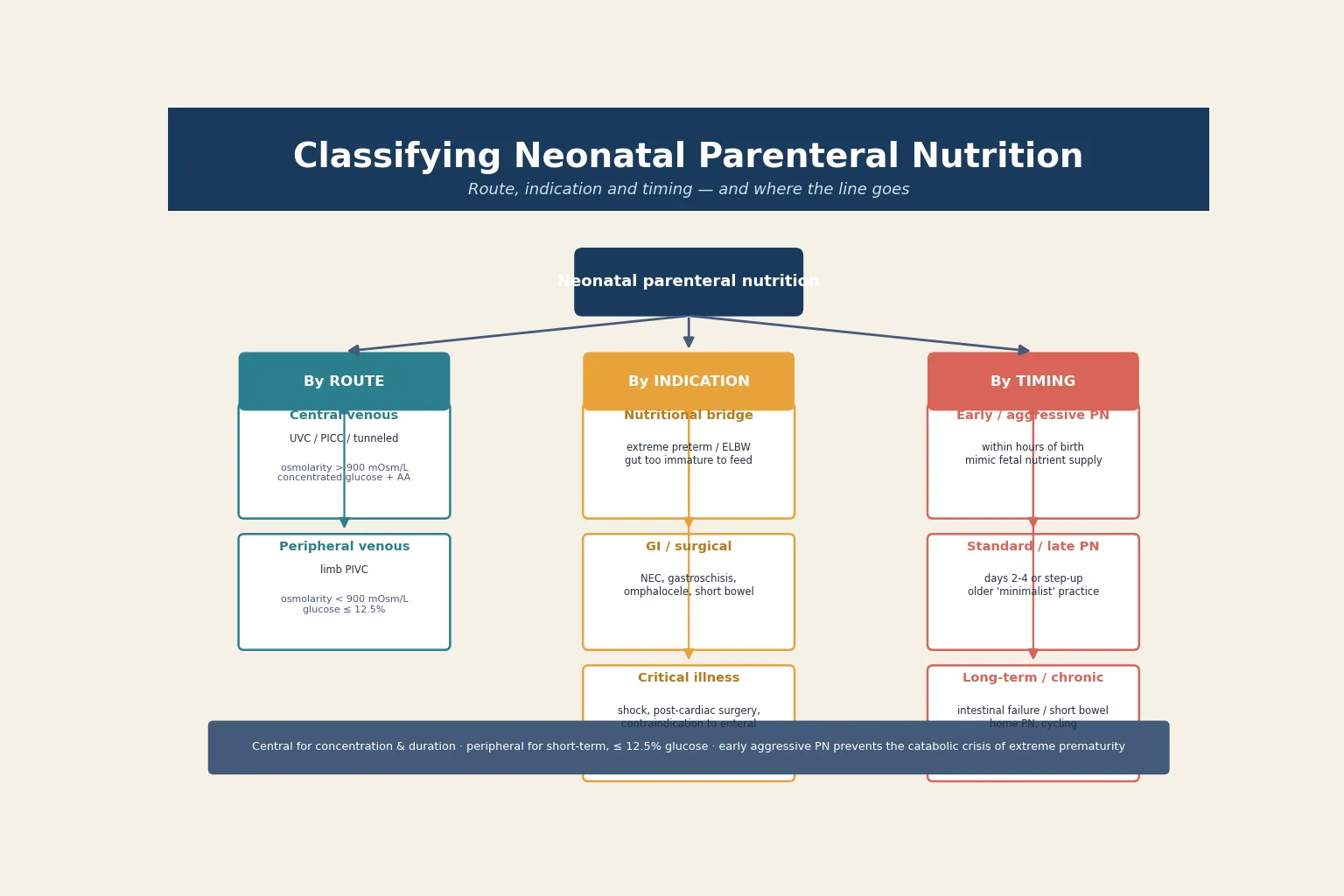
By route, PN is central or peripheral. Central nutrition — via an umbilical venous catheter, peripherally inserted central catheter (PICC) or tunneled line — tolerates the high osmolarity (above 900 mOsm/L) of concentrated glucose and amino acids and is the standard for any infant needing PN beyond a day. Peripheral nutrition, through a limb cannula, is reserved for short-term use and must stay below roughly 900 mOsm/L with glucose no stronger than 12.5%, which limits the energy and protein that can be delivered. [2]
By indication, three groups dominate neonatal practice. The nutritional bridge covers the extreme preterm whose gut is too immature to meet metabolic demand. The gastrointestinal and surgical group covers necrotising enterocolitis, gastroschisis, omphalocele, atresias and short bowel syndrome, where the enteral route is absent or unsafe. The critical-illness group covers shock, post-cardiac surgery, or any state where feeding is contraindicated. [1]
By timing, PN is early (aggressive), standard or long-term. Early aggressive PN begins within hours of birth to mimic fetal nutrient supply; standard or late PN is the older minimalist practice of stepping up over days; long-term PN supports intestinal failure and may move to home cycling. The timing axis is where the PEPaNIC controversy lives, and the candidate must hold the two truths together: early PN protects the preterm, but late PN helps the critically ill older child. [1]
Epidemiology & Risk Factors
Almost every extremely preterm infant receives PN at some point in the first weeks of life, because the gut simply cannot absorb enough before 30 to 32 weeks to match metabolic demand. The sicker and more premature the infant, the longer and more intense the PN course, and the higher the exposure to its complications. [2]
The infants at the greatest need are also those at the greatest risk. Very and extremely preterm infants (below 32 weeks) have the smallest nutrient reserve, the most immature gut, and the longest dependency on PN. Growth-restricted infants add the double burden of depleted intrauterine stores. Surgical infants — gastroschisis, atresia, necrotising enterocolitis with resection — move onto a long PN pathway where the length of remaining bowel, the presence of the ileocaecal valve, and the colon determine whether intestinal failure is temporary or lifelong. [2]
Two complications dominate the epidemiology and define the safety case. Catheter-related bloodstream infection is roughly proportional to line days and breaks in the line, and it carries a measurable mortality in the ELBW infant. Parenteral nutrition-associated cholestasis, now called intestinal failure-associated liver disease (IFALD), rises with the duration of PN, the dose of soybean lipid, the absence of enteral feeding, and the degree of prematurity — affecting a significant minority of infants on PN beyond a few weeks. [10]
Social determinants shape access and outcome. Late or absent antenatal care raises the rate of extreme preterm birth; remoteness delays the establishment of central access and metabolic monitoring; and the cost and logistics of long-term home PN fall hardest on disadvantaged families, who need a coordinated, funded, multidisciplinary pathway. [10]
Pathophysiology
To understand why PN is started so early, follow the nutrient deficit. To understand why it is so carefully titrated, follow the harm it can do. The neonate sits between a catabolic cliff and a metabolic injury, and PN must thread the gap. [7]
The catabolic crisis of prematurity is the core physiology. Glycogen, fat and protein are deposited mainly in the third trimester, so the very preterm infant is born with the smallest reserve at the moment of the highest demand. The fetal brain is growing and the body accreting 3.5 to 4 g/kg/day of protein, which is the most anabolic period of life. [7] When the enteral route cannot deliver, withholding nutrition flips that anabolic state into negative nitrogen balance within hours: plasma amino acids fall, protein synthesis lags, glucose becomes unstable, and brain and somatic growth are lost in a window that does not fully recover. This is the rationale for early amino acid delivery directly after birth. [7]
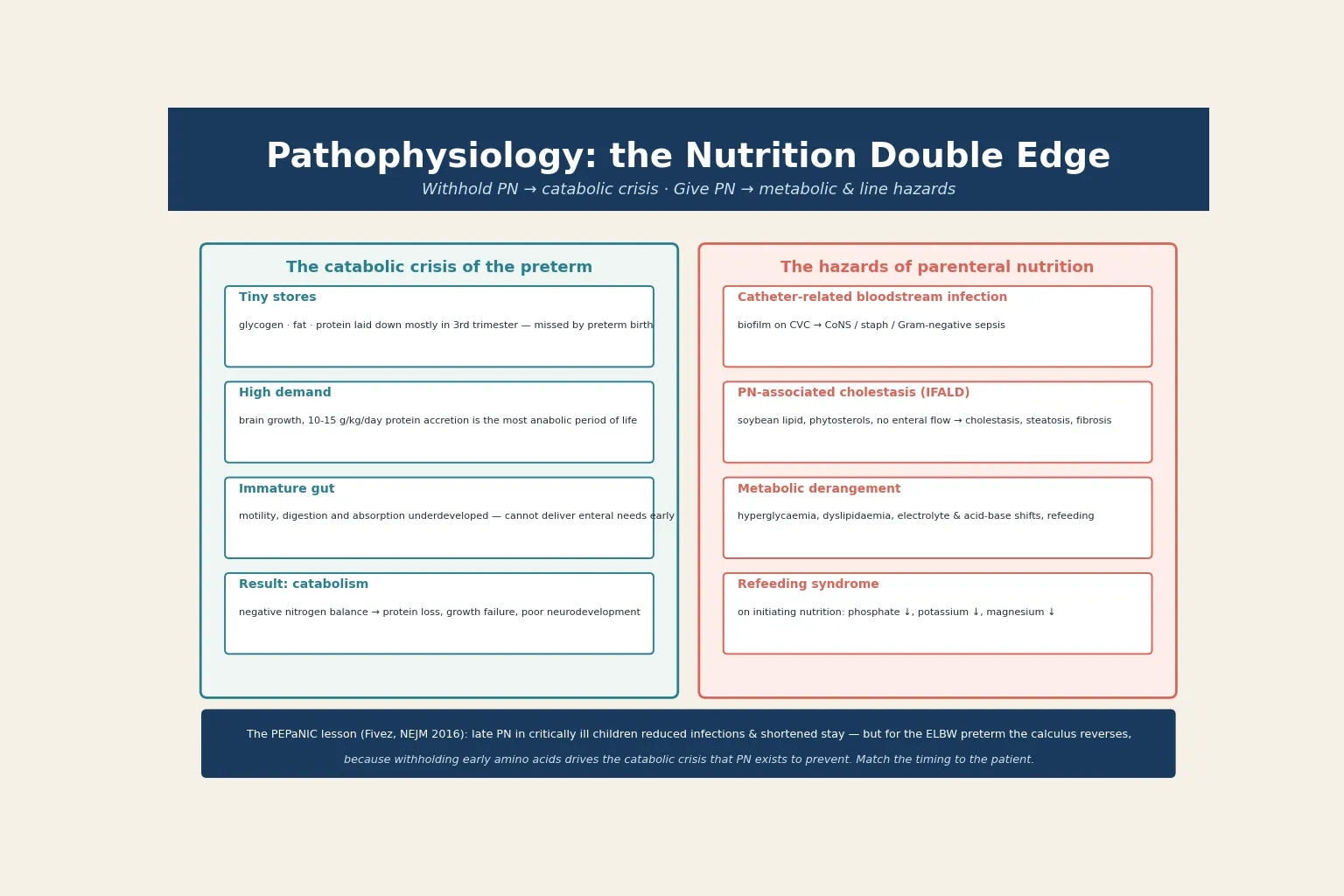
Against this stands the harm that PN itself inflicts, and it is the pathophysiology the candidate must master to prescribe safely. The central catheter is a foreign body in the bloodstream; biofilm forms on it, and a break in the line for medication or sampling seeds organisms — coagulase-negative staphylococci most often, but also staphylococci, Gram-negatives and Candida — producing catheter-related bloodstream infection. [10] The liver injury of IFALD follows a different mechanism: excess soybean lipid and its phytosterols, combined with the absence of enteral bile flow and gut trophic signalling, impair biliary secretion and produce cholestasis, steatosis and, in prolonged cases, fibrosis and portal hypertension. [10]
The metabolic hazards are immediate. Glucose infusion that outruns the infant's insulin response produces hyperglycaemia, osmotic diuresis and dehydration; lipid that exceeds clearance raises triglycerides and risks fat overload and pancreatitis. [5] Refeeding syndrome, long recognised in malnourished adults, also occurs in the depleted neonate: initiating or escalating nutrition drives intracellular phosphate, potassium and magnesium uptake and depletes their serum levels, sometimes with arrhythmia, respiratory failure and encephalopathy. [3]
Clinical Presentation
The neonate on PN does not present with PN itself — they present with the prematurity, the surgery, or the critical illness that made PN necessary. What the candidate must recognise is the presentation of complication: the infant on PN who deteriorates is, until proven otherwise, an infant with line sepsis, metabolic derangement, cholestasis or refeeding. [10]
Line sepsis declares itself as the classic septic picture in an infant with a central line in situ: temperature instability, apnoea or bradycardia, increasing respiratory support, feeding intolerance, lethargy, and a rising or falling white cell count with a high or band-predominant differential. Any unexplained deterioration in a baby with a central catheter is line sepsis until cultures prove otherwise, and a pause to think is a pause that kills — take cultures and treat. [10]
Metabolic derangement is often silent and found only on surveillance. Hyperglycaemia produces an osmotic diuresis (weight loss despite fluid, glycosuria) and, if severe, intraventricular haemorrhage risk from hyperosmolality. Hypoglycaemia produces the neuroglycopenic signs — jitteriness, apnoea, seizures. Lipid intolerance shows as a milky (lipaemic) plasma sample or a rising triglyceride. [5] Refeeding syndrome presents as the unexplained fall in phosphate, potassium or magnesium on a baby whose nutrition has just been started or escalated, sometimes with respiratory distress, irritability or cardiac arrhythmia. [3]
IFALD declares itself more slowly: a conjugated bilirubin that creeps upward, pale stools, hepatomegaly, and a rising alkaline phosphatase and gamma-glutamyl transferase over weeks of PN. It is the complication the candidate must catch early, because early modification of the lipid regimen and enteral advancement can reverse it, whereas late IFALD can progress to irreversible liver failure. [8] [10]
Differential Diagnosis
When an infant on PN deteriorates, the differential is the set of PN complications and the diseases they mimic. The disciplined approach is to assess the line, the glucose, the lipid, the liver and the electrolytes in parallel, not to anchor on any one. [10]
A new fever or respiratory deterioration in a baby with a central catheter is catheter-related bloodstream infection until blood cultures prove otherwise, but the same picture can be necrotising enterocolitis, pneumonia, or a metabolic decompensation — so cultures (peripheral and through the line), a blood gas, glucose, lactate, a CRP and an abdominal X-ray run together. [10]
Rising conjugated bilirubin on PN is IFALD in the first instance, but the candidate must exclude biliary atresia (pale stools, dark urine, the timing), a TORCH infection, an alpha-1-antitrypsin deficiency, a galactosaemia, and a bile-duct obstruction from a stone or a choledochal cyst. The duration and pattern of PN, the lipid dose, and the presence or absence of enteral feeding usually point to IFALD, but the metabolic and infective screen is mandatory before attributing the cholestasis to PN alone. [8]
Refractory metabolic acidosis or a rising ammonia in a catabolic infant on PN is the classic way an inborn error of metabolism declares itself — the stress of catabolism unmasks the enzyme defect, and PN is the trigger, not the cause. Send ammonia, lactate, amino acids, acylcarnitines and urine organic acids, and involve the metabolic service before the child decompensates. [3]
Clinical & Bedside Assessment
Begin with a focused history and examination that frames the nutritional need and the complication risk: gestation and birthweight centile (the reserve), the reason PN was started (prematurity, surgery, critical illness), the postnatal age and day of PN (the duration), the enteral feeding status and tolerance, the line type and site, and any prior infection, hyperglycaemia or cholestasis. [2]
Accurate daily weights are the single most important bedside observation, because weight trend is the ultimate judge of whether the nutrition prescription is working. Plot weight, length and head circumference on a gestation- and sex-specific chart (a Fenton chart for the preterm), and trend the centiles: a flat or falling head-growth velocity means the prescription is failing the brain, however elegant the biochemistry looks. [3]
Examine for the complications at every review. Inspect every central line site for redness, swelling or discharge; feel for hepatomegaly (the early sign of IFALD); assess tone, perfusion and anterior fontanelle (dehydration from osmotic diuresis); and watch the abdomen for distension or tenderness that might signal NEC or feed intolerance. [10] The infant on PN is a system, and the bedside examination reads each system in turn.
Synthesise a one-line summary. A good example: "A 7-day-old 26-week, 780 g infant on day seven of central PN with a stable glucose, a triglyceride of 1.8 mmol/L, no enteral feeds yet, and a line site that is clean — at risk of IFALD with ongoing PN; advance trophic enteral feeds and protect the line." That sentence carries the nutritional state, the complications being watched, and the next move. [2]
Investigations
PN is monitored by a defined daily and weekly schedule, because the prescription changes every day and its complications are silent until they are not. [3]
Daily monitoring during advancement covers glucose (each shift initially, then pre-feed and as needed), weight, and the metabolic panel — sodium, potassium, chloride, bicarbonate, urea, creatinine, calcium, phosphate, magnesium — because electrolytes move as the prescription and the infant change. Triglycerides are checked when lipid is advanced and then periodically, with a triglyceride above 2.5 to 3.0 mmol/L signalling intolerance and the need to slow or reduce the lipid. [5] Liver function — conjugated bilirubin, alkaline phosphatase, gamma-glutamyl transferase, albumin — is trended from the second week onward to catch IFALD early. [10]
Standard ESPGHAN daily targets for the growing neonate
Weekly monitoring adds a full liver function set, a bone profile, and where the course is long, a trace-element and vitamin level. [6] A line-drawn culture pair (peripheral and through the catheter) is the investigation of suspected line sepsis and must never be delayed for antibiotics. Imaging is sparing: an abdominal film for suspected NEC, an ultrasound for line-tip position, and a liver ultrasound or biopsy only when the cholestasis is atypical or prolonged. [10]
Know what to avoid. Do not advance the prescription without a weight and a metabolic panel — blind advancement causes harm. Do not sample routinely through the central line, because every break is a sepsis risk. And do not chase a single abnormal value in isolation — read glucose, lipids, electrolytes, weight and liver function together as the nutritional state of the infant. [3]
What to check each day on the PN ward round
Management — Resuscitation
Most neonates starting PN do not need resuscitation — they need a thoughtful prescription. The exception is the infant who deteriorates on PN, where the resuscitation priority is to treat sepsis, correct metabolic derangement and protect the line as a single bundle. [10]
A febrile or unstable infant with a central catheter in situ is treated as line sepsis without waiting for culture results: take cultures, start broad-spectrum antibiotics that cover coagulase-negative staphylococci and Gram-negatives, and remove or lock the line if the instability is severe or persistent. [10] A metabolic derangement is corrected at the same time — glucose up or down to normal, electrolytes replaced, and a blood gas and ammonia sent if the picture is unclear or the acidosis is refractory.
The specific resuscitation scenarios to rehearse are three. Severe hyperglycaemia with osmotic diuresis is treated by reducing the glucose infusion rate and, in refractory cases, a carefully titrated insulin infusion — never a bolus. [3] Refeeding syndrome is prevented and treated by correcting phosphate, potassium and magnesium before and during the initiation of nutrition, and by advancing the prescription slowly in the depleted infant. [3] A suspected IFALD escalation triggers a lipid review (reduce soybean lipid, consider a fish-oil or mixed-oil emulsion), the protection of any enteral feeding, and the involvement of the hepatology and nutrition service. [8]
The resuscitation errors are predictable: attributing deterioration to the underlying prematurity when the line is the source; under-treating a hyperammonaemic or acidaemic infant as "just septic"; and removing a central line without a replacement plan that leaves the infant without nutrition access. Treat the line as a likely source, read the metabolic panel, and have a replacement plan before removing access. [10]
Management — Definitive & Stepwise
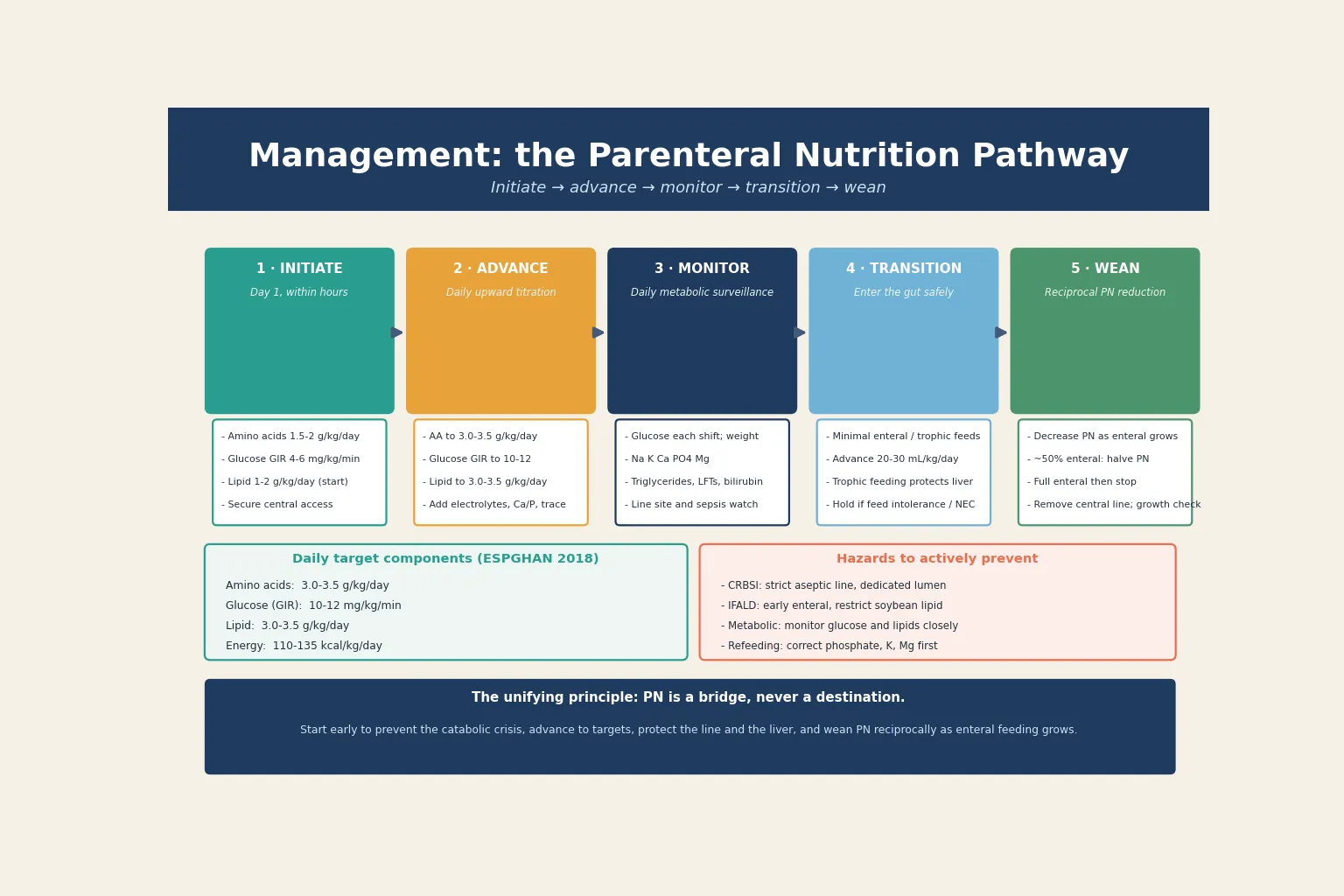
Once stable, definitive care is a sequence you can rehearse: initiate early, advance to targets, monitor daily, protect the line and liver, transition to enteral, and wean PN reciprocally until it stops. [2]
- Initiate early and aggressively in the preterm. Begin amino acids at 1.5 to 2 g/kg/day and a glucose infusion rate of 4 to 6 mg/kg/min within the first hours of life, and start lipid at 1 to 2 g/kg/day, because the catabolic crisis of the very preterm is prevented only by mimicking transplacental nutrient delivery. [7] [4]
- Advance to targets over the first days. Titrate amino acids up to 3.0 to 3.5 g/kg/day, the glucose infusion rate to 10 to 12 mg/kg/min, and lipid to 3.0 to 3.5 g/kg/day, adding electrolytes, calcium, phosphate, trace elements and vitamins as the prescription and the infant allow. The ESPGHAN 2018 guidelines set the targets and the safe rate of advance. [4] [5] [6]
- Monitor daily and adjust. Check glucose each shift, weigh daily, run the electrolyte and metabolic panel, and check triglycerides and liver function on the schedule above. Treat the infant and the trend, not a single number. [3]
- Protect the line. A dedicated lumen for PN, a strict no-break policy, an aseptic insertion and dressing protocol, and a low threshold for line review are the bundle that keeps catheter-related bloodstream infection down. [10]
- Protect the liver. Advance enteral feeding as early and as fast as safely possible, restrict the soybean-lipid dose, consider a mixed-oil or fish-oil-containing emulsion for the infant with rising cholestasis, and avoid sepsis (which itself worsens IFALD). [8] [10]
- Transition to enteral and wean PN reciprocally. Start minimal enteral or trophic feeds, advance as tolerated (commonly 20 to 30 mL/kg/day), and reduce PN as enteral volume grows — roughly halving PN when the infant reaches half their enteral target and stopping PN once full enteral feeding (about 120 to 150 mL/kg/day) is established. [2]
- Plan growth and follow-up. The endpoint is not "PN stopped" but an infant growing along their own centile, with the line removed and the family supported. Arrange nutritional, growth and neurodevelopmental surveillance, and for the infant with intestinal failure, coordinate the long-term home-PN and surgical pathway. [2]
The first week of PN in the very preterm
Day 0–1: start amino acids 1.5–2 g/kg/day, glucose GIR 4–6, lipid 1–2 g/kg/day
within hours of birth via central access
Days 1–3: advance amino acids to 3–3.5 g/kg/day, lipid to 3–3.5 g/kg/day
monitor glucose, triglycerides, electrolytes daily
Days 2–7: start minimal enteral / trophic feeds, protect line and liver
advance enteral as gut tolerates
Weeks 1–3: wean PN reciprocally as enteral grows
halve PN at ~50% enteral
Full enteral (≥120–150 mL/kg/day): stop PN, remove line
confirm growth along centile
Specific Subtypes & Scenarios
The very preterm or ELBW infant. The archetype. Start early aggressive PN within hours, advance to ESPGHAN targets, protect the line, and wean as trophic enteral feeds establish. The danger is either withholding (catabolic crisis, growth failure) or over-delivering (hyperglycaemia, lipid intolerance). [7] [4]
The surgical neonate — gastroschisis, atresia, NEC with resection. The enteral route is absent or unsafe, and PN is the nutrition lifeline for weeks. The length and quality of remaining bowel, the ileocaecal valve, and the colon predict whether the child will achieve enteral autonomy or progress to intestinal failure. Coordinate surgery, nutrition and hepatology from the outset. [2]
Intestinal failure and short bowel syndrome. Long-term PN becomes the therapy, not the bridge. The aims are to preserve and adapt the bowel (avoid unnecessary resection, promote adaptation with enteral trophic feeding, manage bacterial overgrowth), protect the liver from IFALD (mixed-oil or fish-oil lipid, advance enteral, avoid sepsis), and move to a home-PN and cycling programme when stable. [8]
The critically ill older infant — the PEPaNIC lesson. In the haemodynamically unstable child in PICU, delaying PN to day 8 reduced infections and shortened stay in the Fivez trial. This applies to the critically ill child, not to the ELBW preterm whose developmental need for early protein accretion overrides the late-PN benefit. Hold both truths: early for the preterm, late for the critically ill older child. [1]
IFALD — the rising conjugated bilirubin. Reduce the soybean-lipid load, switch to a mixed-oil or pure-fish-oil (omega-3) emulsion, advance enteral feeding aggressively, treat line sepsis, and involve hepatology. Fish-oil lipid emulsion can reverse established PN-associated liver injury, but the best strategy is prevention through early enteral feeding and lipid restraint. [8] [10]
Rural and remote setting. Plan central access, a standard PN prescription, daily metabolic monitoring and early retrieval liaison before the infant deteriorates. A preterm infant on PN without metabolic monitoring or line-care expertise is an avoidable crisis — escalate and retrieve early, and use telehealth for the nutrition review in the interim. [10]
Complications & Pitfalls
Short-term, expect line sepsis, hyperglycaemia, hypoglycaemia, lipid intolerance, electrolyte shifts and refeeding; long-term, expect IFALD, metabolic bone disease, line occlusion and, in the most dependent infants, irreversible liver failure needing transplant. These complications are the reason PN is a discipline, not a prescription. [10]
The pitfalls are predictable, and worth naming so you avoid them. Withholding early amino acids in the preterm out of a generic caution about PN — that drives the catabolic crisis PN exists to prevent. [7] Applying the PEPaNIC late-PN lesson to the wrong patient — the ELBW preterm is not the PICU child, and early protein accretion is non-negotiable. [1] Sampling or breaking the line repeatedly — every break is a sepsis opportunity. Chasing a single glucose or lipid value without reading the whole panel and the weight trend. Letting the soybean-lipid dose creep up while enteral feeds stall — the surest path to IFALD. [10] Failing to correct phosphate, potassium and magnesium before initiating nutrition in the depleted infant — refeeding. And removing a central line without a nutrition replacement plan — leaving the infant without access. [3]
Prognosis & Disposition
Outcome is driven by the gestation, the underlying condition, the duration of PN, and the prevention of its complications. For most preterm infants, PN is a successful bridge to full enteral feeding within weeks, and growth and neurodevelopment follow the underlying prematurity rather than the nutrition itself. The risk concentrates in the long-term PN group, where IFALD, recurrent sepsis and intestinal failure determine the course. [2]
The evidence that makes early PN worthwhile is the te Braake programme and the ESPGHAN framework: early amino acid delivery prevents negative nitrogen balance and supports brain growth, and the protein target of 3 to 3.5 g/kg/day is the foundation of neonatal nutrition. [7] [4] For the critically ill older child, the PEPaNIC trial reframes the timing question, reducing infections and length of stay with a late-PN strategy — but it does not apply to the ELBW preterm. [1] For established IFALD, fish-oil lipid emulsion can rescue liver injury and reduce transplant need. [8]
Disposition follows the trajectory. A stable preterm on a standard PN pathway is managed in the neonatal unit with daily monitoring and reciprocal weaning. A surgical or intestinal-failure infant moves onto a long-term, multidisciplinary pathway with surgery, nutrition, hepatology and the home-PN service. A deteriorating infant — line sepsis, refractory metabolic derangement, or advancing IFALD — escalates to the intensive-care and specialist team, and in the rural setting, retrieval is activated early. [10]
Special Populations
Indigenous and socioeconomically disadvantaged families carry a higher burden of preterm birth and late antenatal access, raising both the need for PN and the complexity of follow-up. Provide culturally safe care, address nutrition and housing directly, and ensure the surveillance and home-PN pathway is funded and continuous. [2]
Rural and remote settings must plan central access, a standard PN prescription, daily metabolic monitoring and early retrieval liaison. A preterm infant on PN without monitoring or line expertise is an avoidable crisis — escalate and retrieve early, and support the family with telehealth in the interim. [10]
The very preterm and growth-restricted infant compounds depleted stores with the highest metabolic demand, lowering the threshold for early aggressive PN and the closest monitoring. Protein and energy targets are non-negotiable here, because the brain is growing fastest when the reserve is smallest. [7]
Intestinal-failure and complex surgical infants run on a specialist, technology-dependent pathway — long-term PN, home cycling, hepatology surveillance, and possible bowel-lengthening surgery or transplant — coordinated by a multidisciplinary intestinal-failure team. [8]
Out-of-home-care and migrant-refugee families need deliberate continuity of the nutrition, growth and neurodevelopmental follow-up across moves, so that the prescription and the surveillance are not lost. [2]
Families of infants on long-term PN need clear parent education, support for home PN, and explicit safety-netting on the signs of line sepsis, cholestasis and metabolic decompensation to return for. [10]
Evidence, Guidelines & Regional Differences
The foundational ESPGHAN 2005 guidelines (Koletzko) established the framework for paediatric parenteral nutrition, and the 2018 ESPGHAN/ESPEN/ESPR/CSPEN update refined it into the component guideline series — energy (Joosten), amino acids (van Goudoever), lipids (Lapillonne) and iron and trace minerals (Domellöf) — that now set the daily targets and advancement rates used worldwide. [2] [3] [4] [5] [6]
The timing controversy is the PEPaNIC trial (Fivez, NEJM 2016), a landmark multicentre study showing that late PN in critically ill children reduced new infections and shortened PICU stay. [1] It reframed practice in the PICU population, but it must not be over-generalised to the ELBW preterm, whose early protein need is supported by the te Braake early-amino-acid data and the Cochrane review of early versus late amino acids in preterm infants (Trivedi 2024). [7] [9]
The IFALD evidence is the Puder fish-oil study (Annals of Surgery 2009) showing that an omega-3 lipid emulsion improved outcomes in parenteral nutrition-associated liver injury, and the ESPGHAN position paper on intravenous lipid emulsions and hepatotoxicity (Hojsak 2016) that reviewed the lipid- and liver-risk evidence. [8] [10]
Two live controversies: the timing of PN in the critically ill neonate — early aggressive PN for the preterm versus the PEPaNIC late-PN lesson, reconciled by matching the timing to the patient's developmental state; and the optimal lipid emulsion — pure soybean, mixed-oil, or fish-oil-containing — to deliver energy and essential fatty acids while protecting the liver from IFALD. [1] [5]
Exam Pearls
- Neonatal PN is a bridge, not a destination — start early in the preterm to prevent the catabolic crisis, advance to targets, protect the line and liver, and wean reciprocally as enteral feeding grows. [2]
- The preterm carries the smallest reserve at the highest demand — protein accretion runs at 3.5 to 4 g/kg/day, so early amino acids are a developmental necessity, not a convenience. [7]
- The ESPGHAN daily targets: amino acids 3 to 3.5 g/kg/day, glucose GIR 10 to 12 mg/kg/min, lipid 3 to 3.5 g/kg/day, energy about 90 to 120 kcal/kg/day on exclusive parenteral nutrition (total energy targets rise toward 110 to 135 kcal/kg/day as enteral feeds advance) — start at half and advance. [4] [5]
- Route is dictated by osmolarity — central (above 900 mOsm/L) via UVC, PICC or tunneled line; peripheral below 900 mOsm/L with glucose no stronger than 12.5%. [2]
- The PEPaNIC trial (Fivez, NEJM 2016) showed late PN reduced infections and stay in critically ill children — but it does not apply to the ELBW preterm. [1]
- A rising conjugated bilirubin on PN is IFALD until excluded — reduce soybean lipid, advance enteral, consider fish-oil emulsion, treat sepsis. [8]
- The four complications to name: catheter-related bloodstream infection, IFALD, metabolic derangement (glucose and lipid), and refeeding syndrome. [10]
- Refeeding: falling phosphate, potassium or magnesium on starting or escalating nutrition — correct electrolytes before and during initiation. [3]
- The line is sepsis until proven otherwise in any deteriorating infant on PN — take cultures and treat, do not wait. [10]
References
- [1]Fivez T Early versus Late Parenteral Nutrition in Critically Ill Children. New England Journal of Medicine, 2016.PMID 26975590
- [2]Koletzko B Guidelines on Paediatric Parenteral Nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), supported by the European Society of Paediatric Research (ESPR). Journal of Pediatric Gastroenterology and Nutrition, 2005.PMID 16254497
- [3]Joosten K ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Energy. Clinical Nutrition, 2018.PMID 30078715
- [4]van Goudoever JB ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Amino acids. Clinical Nutrition, 2018.PMID 30100107
- [5]Lapillonne A ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Lipids. Clinical Nutrition, 2018.PMID 30143306
- [6]Domellöf M ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Iron and trace minerals. Clinical Nutrition, 2018.PMID 30078716
- [7]te Braake FW Amino acid administration to premature infants directly after birth. Journal of Pediatrics, 2005.PMID 16227030
- [8]Puder M Parenteral fish oil improves outcomes in patients with parenteral nutrition-associated liver injury. Annals of Surgery, 2009.PMID 19661785
- [9]Trivedi A Early versus late administration of amino acids in preterm infants receiving parenteral nutrition. Cochrane Database of Systematic Reviews, 2024.PMID 38275196
- [10]Hojsak I ESPGHAN Committee on Nutrition Position Paper: Intravenous Lipid Emulsions and Risk of Hepatotoxicity in Infants and Children — a Systematic Review. Journal of Pediatric Gastroenterology and Nutrition, 2016.PMID 26825766