Paeds · fetal-neonatal-and-perinatal
Patent ductus arteriosus in preterm infants
Also known as Patent ductus arteriosus · Haemodynamically significant PDA · hsPDA · Preterm ductus arteriosus
Fellowship guide to patent ductus arteriosus in preterm infants: why the preterm ductus fails to close, what makes it haemodynamically significant, the bedside and echocardiographic assessment, the modern expectant-first management ladder with ibuprofen, indomethacin and paracetamol, the ligation causality-or-bias debate, and the evidence behind treating the infant rather than the echo.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 26-week infant, three days old, ventilated for respiratory distress syndrome, is weaning nicely. Over the next 48 hours the team notice bounding pulses, a widened pulse pressure, and a creeping oxygen and ventilator requirement. The echocardiogram shows a 2 mm duct with left-to-right flow and diastolic flow reversal in the descending aorta. This is the classic presentation of a patent ductus arteriosus (PDA) becoming haemodynamically significant, and the decisions made here are some of the most contested in modern neonatology. [13] [7]
The ductus arteriosus is the fetal vessel connecting the main pulmonary artery to the descending aorta. In utero it shunts the right ventricular output away from the high-resistance lungs and toward the placenta. After birth it is meant to close — first functionally, by smooth muscle contraction within hours, then anatomically, by intimal proliferation over two to three weeks, leaving the ligamentum arteriosum. A PDA in the preterm context is persistent patency beyond this expected window. It is not a congenital malformation in the usual sense; it is the predictable consequence of an immature ductal wall meeting the postnatal circulation. [7] [14]
The distinction that governs all management is between a PDA that is merely present and one that is haemodynamically significant — a substantial left-to-right shunt producing measurable pulmonary over-circulation and systemic hypoperfusion. Most preterm ducts stay open for a while and most close on their own; only a minority cause the end-organ compromise that justifies treatment. Holding the question "is this duct significant?" at the centre of every assessment is the single most important habit for this topic, because the evidence base of the last decade has remorselessly dismantled the older reflex of closing every duct. [1] [11]
The modern story of the preterm PDA is a story of restraint winning over intervention. Three decades of trials — from prophylactic indomethacin to early ibuprofen to the BeNeDuct trial of expectant management — have shown that routine closure does not improve survival without bronchopulmonary dysplasia, does not improve long-term neurodevelopment, and carries real harms. The fellowship candidate who can articulate why practice shifted, and name the trials, will answer this topic well. [1] [6] [11]
Epidemiology & Risk Factors
The incidence of a PDA is inversely proportional to gestational age. Roughly 55–65% of infants born under 28 weeks have a patent ductus at four to seven days, falling to around 20–30% at 28–31 weeks and below 5% in term infants. The extreme preterm is the patient of interest: the more immature the ductal smooth muscle, the more likely it is to stay open. [7] [14]
Risk factors cluster around two themes — immaturity and the sick preterm lung. The dominant risks are decreasing gestational age and birth weight, respiratory distress syndrome (surfactant deficiency), and the absence of antenatal corticosteroids. Additional contributors include fluid overload in the first days of life, perinatal asphyxia, neonatal sepsis, and male sex. Each of these either weakens the ductal wall's contractile response or keeps pulmonary vascular pressure high, sustaining flow through the duct. [14] [13]
Not every open duct stays open. Chorne and colleagues showed that the factors predicting persistent patency — even during indomethacin treatment — are extreme immaturity, a larger initial duct size, and the need for higher ventilator support. Knowing who is likely to fail spontaneous (and pharmacological) closure helps target the infants who may eventually need intervention, while reinforcing that the majority will not. [14]
The temporal trend matters for the examiner. As survival of the most extreme gestations has improved, the raw number of preterm infants with a PDA has risen, even as treatment rates have fallen. The apparent paradox — more ducts, less treatment — is the direct product of the expectant-first evidence base, and it is the trend a candidate must be able to explain. [11] [12]
Pathophysiology
Two forces hold the fetal ductus open: low oxygen tension and high circulating prostaglandins, chiefly prostaglandin E2 from the placenta. The ductal smooth muscle relaxes in response to both. After birth, the cord is clamped and the placenta is gone; oxygen tension rises and prostaglandin levels fall. The ductal wall is now free to contract. [7] [13]
Functional closure is an oxygen-driven, calcium-mediated event. Rising oxygen tension closes oxygen-sensitive potassium channels on the ductal smooth muscle cell, the membrane depolarises, calcium enters, and the smooth muscle contracts. The parallel fall in prostaglandins removes the dominant relaxing influence. Within hours the lumen narrows, and over two to three weeks intimal proliferation and medial necrosis complete the anatomical closure that becomes the ligamentum arteriosum. [7]
The preterm ductus fails at this for three compounding reasons. Its smooth muscle is immature, with a thinner medial layer and a weaker contractile response to oxygen. It remains abnormally sensitive to the relaxing prostaglandins, which fall only slowly in the preterm because the immature kidney and lung clear them poorly. And its intimal cushions are underdeveloped, so the substrate for anatomical closure is deficient. The same gestational age that predicts surfactant deficiency predicts ductal patency. [7] [14]

Once the duct stays open, the direction and magnitude of the shunt are governed by the balance of systemic and pulmonary vascular resistance. In the first day or two the pulmonary vascular resistance is still high and the shunt is small or bidirectional. As the resistance falls over days three to seven, the shunt becomes progressively left-to-right. Blood is now pumped from the aorta back into the pulmonary circulation in both systole and diastole — the basis of the continuous murmur and the diastolic steal. [13]
The haemodynamic consequences flow directly from that shunt. Pulmonary over-circulation floods the lungs, raising the oxygen and ventilator requirement, causing pulmonary oedema and occasionally pulmonary haemorrhage, and contributing to bronchopulmonary dysplasia. Systemic hypoperfusion is the mirror image: diastolic flow is stolen into the lungs, so the diastolic blood pressure falls, the kidneys, gut and brain are underperfused, and the infant develops oliguria, a rising creatinine, feed intolerance or frank necrotising enterocolitis, and is at risk of intraventricular haemorrhage. The widened pulse pressure and bounding pulses are the physical signs of this large stroke volume entering a low-resistance pulmonary bed. [13] [10]
Classification
The classification that matters clinically separates a PDA that is merely present from one that is haemodynamically significant (hsPDA). A small or closing duct with no end-organ effect is an incidental finding; a duct with a large left-to-right shunt causing pulmonary over-circulation and systemic steal is hsPDA. This single distinction drives the entire management ladder, and a candidate who conflates the two will answer badly. [13] [7]
Significance is graded by echocardiography, using a constellation of measures rather than any single number. A duct diameter above 1.5 mm suggests a large shunt. A left atrial-to-aortic root ratio (LA:Ao) above 1.5 marks left heart volume overload. Diastolic flow reversal in the descending aorta or the coeliac axis is the direct echocardiographic fingerprint of the systemic steal. A growing or pulsatile ductal flow pattern and an increased left ventricular output complete the picture. Significance is a judgement from the whole echo, not a single threshold. [13] [12]
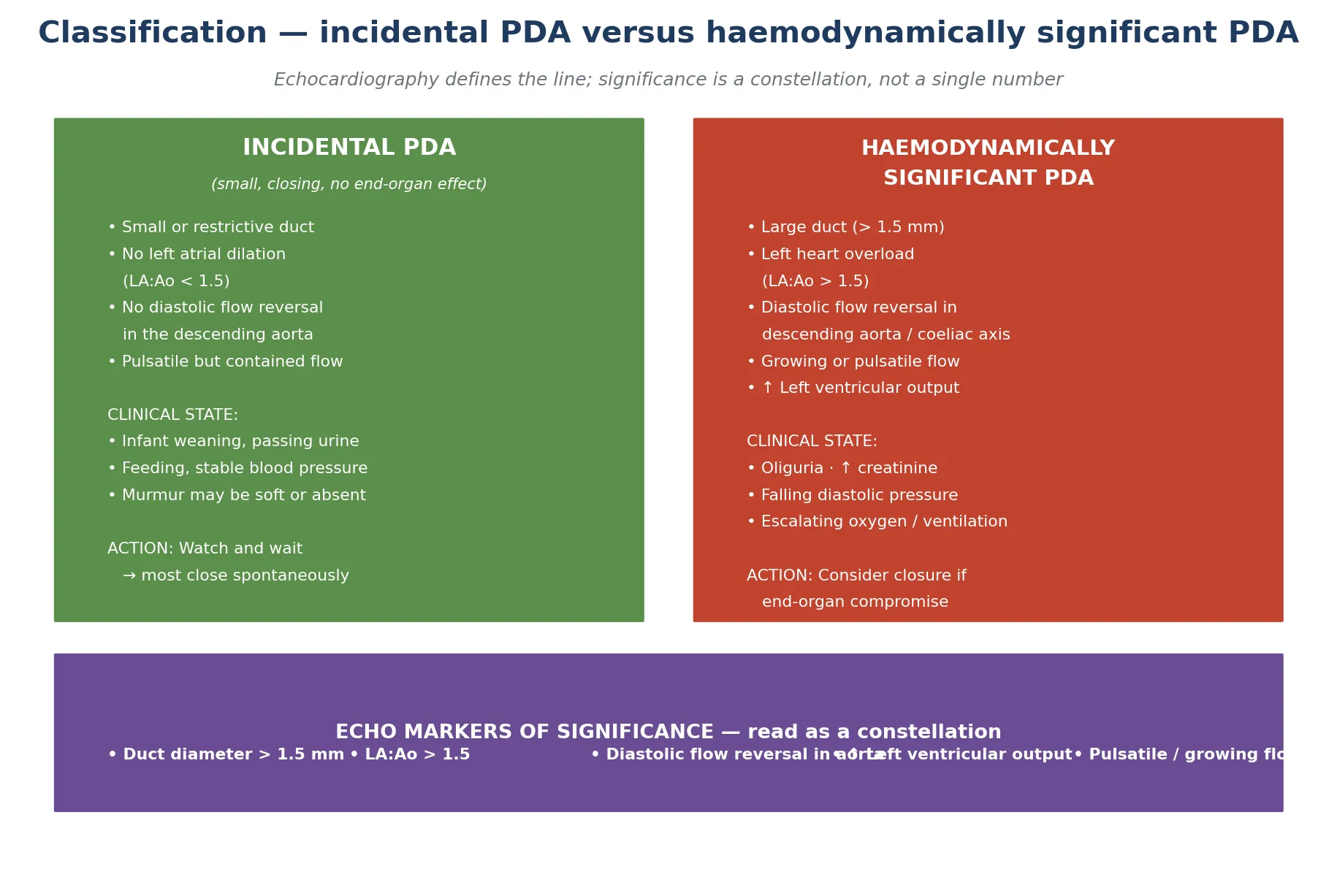
The clinical and echocardiographic pictures should agree, and discordance is informative. A loud murmur with a small, restrictive duct on echo is not haemodynamically significant; a quiet chest with a large duct, left heart dilation and aortic flow reversal most certainly is. The lesson the examiners draw from this agreement is that the stethoscope under-calls significance and the echo over-calls size — the treating team must integrate the echo with the bedside end-organ assessment before deciding. [13]
A temporal classification is also useful. An early PDA declares itself between days three and seven as the pulmonary vascular resistance falls; a persistent PDA is one still open and significant beyond one to two weeks. Persistent patency, especially in the extremely preterm, is the group most associated with prolonged ventilation and bronchopulmonary dysplasia, and the group most likely to provoke a treatment decision. [6] [11]
Haemodynamically significant versus insignificant PDA
- Small or restrictive duct on echo
- No left atrial dilation (LA:Ao below 1.5)
- No diastolic flow reversal in aorta
- Infant weaning, passing urine, feeding
- Watch and wait — most close spontaneously
- Large duct (above 1.5 mm), pulsatile flow
- Left heart overload (LA:Ao above 1.5)
- Diastolic flow reversal in descending aorta
- Oliguria, falling diastolic pressure, rising oxygen need
- Consider pharmacological closure if end-organ compromise
Clinical Presentation
The classical presentation is the preterm infant who was weaning and then stops. Somewhere between day three and seven, as the pulmonary vascular resistance falls, the shunt opens up and the clinical signs emerge. The team notice first that the ventilator and oxygen settings cannot be reduced, then that they have to be increased. [13] [7]
The bedside cardiovascular signs are the fingerprint of a large left-to-right shunt. Feel the pulses — they are bounding, palpable at the wrists and ankles. Watch the precordium — it is hyperdynamic, heaving with each beat. Listen for the murmur — a systolic or continuous machinery murmur at the upper left sternal border, though in the smallest infants it may be absent or soft. Measure the blood pressure — a widened pulse pressure, with a characteristically low diastolic, is the sign that the diastolic steal has begun. [13]
The end-organ signs are often more telling than the murmur, and they precede it. Pulmonary over-circulation shows as a creeping oxygen requirement, pulmonary oedema on the radiograph, rising carbon dioxide, and occasionally pulmonary haemorrhage. Systemic hypoperfusion shows as oliguria, a rising creatinine, metabolic acidosis, hypotension (especially the low diastolic), feed intolerance and abdominal distension. Any preterm infant who develops these in the second week has a significant PDA until the echo proves otherwise. [10] [13]
BUMP-WIDE — the haemodynamically significant PDA
Not every presentation is dramatic. Many preterm ducts are first detected on a routine echocardiogram in an infant who is clinically stable, and the question is then whether the duct is significant at all. Equally, a large duct may declare itself abruptly with a pulmonary haemorrhage in an infant who had been weaning — one of the few situations in which a PDA presents as an emergency. The spectrum, from incidental echo finding to pulmonary haemorrhage, is the range the examiner expects you to hold. [7] [13]
Differential Diagnosis
When a ventilated preterm infant deteriorates in the second week, a significant PDA is one diagnosis on a list. The discipline is to hold the differentials in parallel, because a PDA is treated by closure (or patience) while the others are not, and missing sepsis while chasing the duct is a classic error. [13]
The respiratory differentials dominate. Worsening respiratory distress syndrome, evolving bronchopulmonary dysplasia, nosocomial pneumonia, and pulmonary interstitial emphysema all produce a rising oxygen and ventilator requirement and can coexist with a PDA. Late-onset sepsis causes deterioration, hypotension and feed intolerance indistinguishable from the systemic steal of a PDA — and sepsis itself can keep the duct open. [13]
The cardiovascular and neurological differentials must not be forgotten. Intraventricular haemorrhage presents as sudden deterioration, hypotension and acidosis. Sepsis-induced myocardial dysfunction mimics the low-output state. A genuine structural cardiac lesion — coarctation of the aorta (weak femorals, differential blood pressure), or a duct-dependent lesion — must be excluded before any attempt to close the duct, because closing a duct-dependent circulation is catastrophic. [7]
The resolving question is not "is there a PDA?" but "is the PDA causing this deterioration?". The answer comes from integrating the clinical end-organ signs with the echocardiographic markers of significance, while actively ruling out sepsis with blood cultures and inflammatory markers. Only when the duct is significant and the other causes are excluded does treatment become the rational next step. [13] [11]
Clinical & Bedside Assessment
Begin at the bedside, because the echo is interpreted in the light of the clinical state. The focused cardiovascular examination has four targets. Feel the peripheral pulses for the bounding quality of a large stroke volume. Watch the precordium for the hyperdynamic impulse. Listen for the murmur at the upper left sternal border, accepting that it may be absent. Measure the blood pressure for the widened pulse pressure and the falling diastolic. [13]
Then assess the two end-organ territories the steal attacks. For pulmonary over-circulation, trend the FiO₂ and ventilator settings, examine the chest radiograph for cardiomegaly and pulmonary plethora or oedema, and review the blood gases for a rising carbon dioxide. For systemic hypoperfusion, document the urine output (the most sensitive bedside perfusion marker in a neonate), the creatinine trend, the lactate and acid-base status, and the blood pressure trend, with particular attention to the diastolic. [13] [10]
Examine the abdomen for distension and tenderness — the gut is a target of the steal, and feed intolerance or bloody stools raise the spectre of necrotising enterocolitis. Assess the anterior fontanelle and tone, because fluctuating cerebral blood flow from the steal contributes to intraventricular haemorrhage. A deteriorating preterm with a significant duct should have these end-organ signs charted serially, because the decision to treat is made on trajectory, not a single snapshot. [13]
The echocardiogram is the investigation that defines significance, but it is a functional echo performed and interpreted by the neonatal or cardiology team, read alongside the bedside picture. The candidate's job at the cot-side is to assemble the end-organ case for or against significance, so that when the echo is done its findings can be weighed against a clear clinical question. [12] [13]
Investigations
Echocardiography is the gold standard, and it does two jobs. First, it confirms normal cardiac structure and excludes duct-dependent congenital heart disease — the essential safety check before any attempt at closure. Second, it grades ductal significance through the constellation of measures already described: duct diameter, flow pattern, LA:Ao ratio, left heart size, left ventricular output, and diastolic flow in the descending aorta and coeliac axis. [12] [13]
The chest radiograph supports the haemodynamic case. Cardiomegaly, increased pulmonary vascular markings (pulmonary plethora), and pulmonary oedema are the radiographic signs of a large left-to-right shunt, though they are non-specific and lag the echo. The radiograph also helps rule out pneumonia, air leak and evolving bronchopulmonary dysplasia as alternative explanations for the respiratory deterioration. [13]
In Australia and Aotearoa New Zealand, functional point-of-care echocardiography performed by trained neonatologists is now standard for assessing ductal significance, with cardiology confirmation when structural disease is suspected. In the United Kingdom, BAPM-aligned units similarly integrate neonatologist-led echo with cardiology support. In North America, targeted neonatal echocardiography programmes are widespread but practice varies between units. In low-resource settings without bedside echo, the clinical end-organ assessment carries the decision. [13]
Blood tests frame the end-organ compromise and exclude the mimics. Renal function (urea, creatinine, electrolytes) documents the steal; acid-base captures the metabolic acidosis of hypoperfusion; full blood count and CRP with blood cultures pursue sepsis. Cardiac biomarkers such as BNP or NT-proBNP are emerging research tools that correlate with significance but are not yet standard decision-makers. [13]
The synthesis is the point. No single investigation diagnoses a haemodynamically significant PDA; the diagnosis is the integration of the end-organ clinical signs, the echocardiographic markers, and the exclusion of the mimics. A candidate who orders the echo, the gases, the renal function and the septic screen and then reasons from all of them together answers this topic correctly. [11] [13]
Management — Resuscitation
The immediate priority is to optimise the conditions that allow the duct to close and the infant to tolerate the shunt, not to reach for the drug cupboard. Correct hypoxia and acidosis, both of which relax the ductal smooth muscle and keep it open. Treat anaemia to preserve oxygen delivery. Review the ventilation — permissive hypercapnia and volume-targeted, lung-protective settings reduce the shear stress that worsens pulmonary over-circulation. [13] [11]
Fluid management is the first deliberate intervention. Avoid fluid overload in the first days of life, because excess circulating volume enlarges the shunt; modest fluid restriction is reasonable once significance is established, though the evidence for restriction alone closing a duct is weak. Review the total fluid intake and the sodium balance before considering anything more invasive. [13]
The haemodynamically significant duct with systemic steal may need circulatory support while the closure decision is made. Treat hypotension, recognising that the duct is stealing diastolic flow — a vasoconstrictor such as dopamine or noradrenaline may be more effective than volume, and volume boluses rarely help and may worsen the shunt. Maintain gut perfusion by reducing or pausing feeds when the steal is substantial, to lower the risk of necrotising enterocolitis. [13] [10]
The resuscitative phase is also the conservative-management phase, and for many infants it is the only phase they need. The explicit framing of the modern approach is that expectant, supportive care is the default, and that the burden of proof sits with the decision to add pharmacological or surgical closure. Holding this framing — and explaining it to the parents — is the resuscitative mindset the examiner rewards. [1] [11]
Management — Definitive & Stepwise
The stepwise ladder runs from expectant management through pharmacological closure to surgical or transcatheter ligation, and the evidence base now weights the first rung far more heavily than the third. [11] [12]
Step one is expectant management. Most preterm ducts close spontaneously — more than half, even in extremely low birth weight infants, with a contemporary permissive approach. The supportive measures above are continued, the end-organ signs are watched, and the echo is repeated if the clinical picture changes. The BeNeDuct trial showed that early ibuprofen did not improve the composite of death or bronchopulmonary dysplasia compared with expectant management, and the PDA-TOLERATE trial showed that treating a moderate-to-large duct at one week did not either. Expectant management is not inaction; it is an evidence-based strategy. [1] [6] [11]
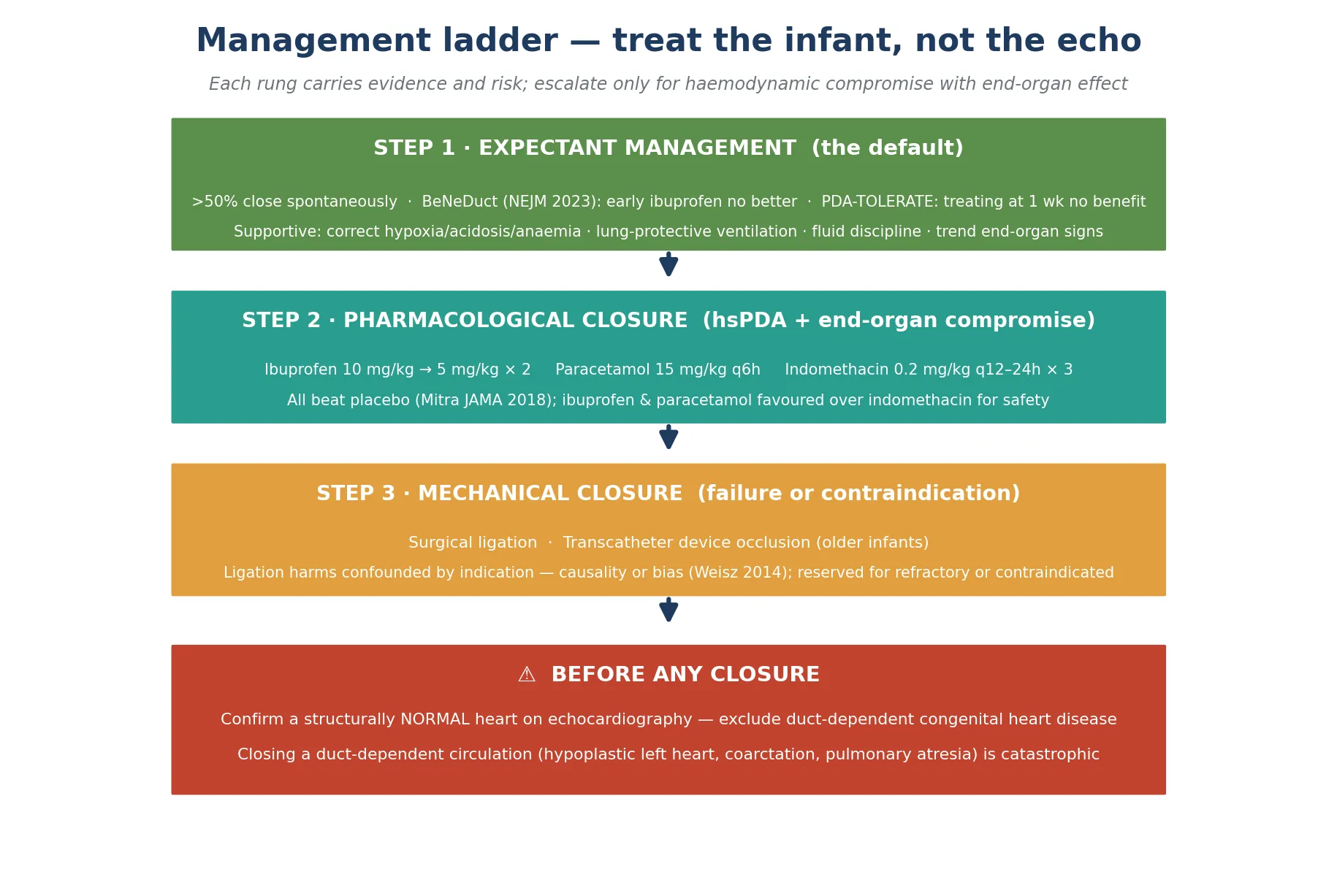
Step two is pharmacological closure, reserved for the duct that is haemodynamically significant and causing end-organ compromise not responding to supportive care. The cyclo-oxygenase inhibitors — ibuprofen and indomethacin — close the duct by suppressing the prostaglandins that keep it relaxed; paracetamol (acetaminophen) closes it by a less fully understood mechanism, probably involving prostaglandin pathways in the ductal wall itself. [2] [3] [4]
Pharmacological closure of the preterm PDA
The network meta-analysis by Mitra and colleagues established that ibuprofen, indomethacin and paracetamol are all more effective than placebo for closure, with ibuprofen and paracetamol generally favoured over indomethacin because of fewer renal and gastrointestinal adverse effects. Paracetamol in particular has emerged as an effective agent with a more favourable renal profile, making it attractive when cyclo-oxygenase inhibitors are contraindicated. The choice is individualised to the infant's renal and hepatic function and feeding status. [2] [4] [8]
Step three is mechanical closure — surgical ligation or, for older and larger infants, transcatheter device occlusion. Ligation is reserved for the duct that fails a course or two of pharmacotherapy, or when pharmacotherapy is contraindicated (renal failure, necrotising enterocolitis, active bleeding). The crucial caveat, articulated by Weisz and McNamara, is that the well-documented association of ligation with bronchopulmonary dysplasia, intraventricular haemorrhage and neurodevelopmental impairment is heavily confounded by indication — sicker infants with larger ducts get ligated, so the harms may reflect the illness, not the operation. Causality, not just association, is the test. [10] [13]
BeNeDuct (NEJM 2023) and PDA-TOLERATE (J Pediatr 2019)
Randomised trials of early ibuprofen versus expectant management (BeNeDuct) and treatment of a moderate-large PDA at 1 week versus continued expectant care (PDA-TOLERATE) in preterm infants.
Key finding
Neither routine early ibuprofen nor treatment at one week reduced death or bronchopulmonary dysplasia compared with expectant management. The trials anchored the modern expectant-first paradigm.
The synthesis the examiner wants is the explicit shift from "close every duct" to "treat the infant with a significant duct causing end-organ compromise, and only then". Each rung of the ladder — expectant care, pharmacotherapy, ligation — carries evidence and risk, and the skill is matching the rung to the infant's haemodynamic state rather than to the echo report. [1] [11] [13]
Specific Subtypes & Scenarios
The extremely preterm infant (under 26 weeks) is the archetype. The patency rate is highest, the ductal wall most immature, and the risk of bronchopulmonary dysplasia greatest. Paradoxically this is the group for whom the expectant-first evidence is strongest, because their fragile kidneys and guts are least tolerant of cyclo-oxygenase inhibitors. The approach is prolonged supportive care, serial end-organ assessment, and treatment only for clear haemodynamic compromise. [11] [13]
The PDA with pulmonary haemorrhage is one of the few true emergencies. A large left-to-right shunt overloads the pulmonary capillary bed until it bleeds. The response is to lower the pulmonary blood flow — reduce the shunt by pharmacological closure, optimise the ventilation and coagulation, and support the circulation. This is a clear indication for active treatment rather than patience. [13]
The PDA with necrotising enterocolitis or renal dysfunction illustrates the tension between the steal and the treatment. The steal underperfuses the gut and kidney, arguing for closure; yet the cyclo-oxygenase inhibitors themselves reduce renal and mesenteric blood flow and are relatively contraindicated in established necrotising enterocolitis and oliguria. Paracetamol is the rational choice when a COX inhibitor is unsafe, and surgical ligation is considered when pharmacotherapy is impossible or failing. [4] [13]
Prophylactic indomethacin for the extreme preterm is a distinct scenario with its own evidence. The Fowlie Cochrane review established that prophylactic indomethacin reduces early severe intraventricular haemorrhage and ductal patency, but it does not improve survival without bronchopulmonary dysplasia or long-term neurodevelopment. It is therefore used selectively in units with high intraventricular haemorrhage rates rather than as a blanket strategy. [5] [12]
The refractory PDA — still large and significant after one or two courses of pharmacotherapy — forces the ligation-versus-patience decision. The modern lean is toward continued expectant management and conservative support, reserving ligation for the infant who cannot be weaned from the ventilator and in whom the duct is the clear limiting factor, always tempering the decision by the causality-or-bias caveat. [10] [13]
The term or late-preterm infant with a persistent PDA is a different entity — a true congenital duct rather than a failure of preterm closure. These infants are referred to paediatric cardiology for transcatheter device closure, typically beyond the neonatal period, and are not managed with cyclo-oxygenase inhibitors. Recognising the distinction prevents the error of treating a congenital duct with neonatal protocols. [7]
Complications & Pitfalls
The complications arise from two sources — the untreated significant shunt and the treatment itself. From the shunt: prolonged ventilation, bronchopulmonary dysplasia, pulmonary haemorrhage, necrotising enterocolitis, renal dysfunction, intraventricular haemorrhage and, in the extreme, death. From the treatment: the renal and gastrointestinal toxicity of the cyclo-oxygenase inhibitors, intestinal perforation, the operative risks of ligation (pneumothorax, phrenic or recurrent laryngeal nerve injury, bleeding, post-ligation cardiac syndrome), and the harm of treating a duct that would have closed on its own. [13] [10]
The classic pitfall is treating the echo, not the infant. Closing a large but clinically silent duct exposes the infant to drug and operative risk for a shunt that was causing no end-organ harm and would likely have closed spontaneously. The expectant-first evidence exists precisely to prevent this error, and the candidate who reaches for pharmacotherapy on the strength of the duct diameter alone answers badly. [1] [11]
The mirror-image pitfall is missing sepsis or duct-dependent heart disease while attributing deterioration to the duct. Late-onset sepsis mimics the systemic steal exactly, and treating a septic infant with a cyclo-oxygenase inhibitor deepens the renal and gut injury. Closing a duct-dependent circulation — hypoplastic left heart, critical coarctation, pulmonary atresia — is catastrophic, which is why a structurally normal heart must be confirmed on echo before any closure attempt. [7] [13]
A subtler pitfall is over-attributing the harms of ligation. The observational association of ligation with adverse outcomes is heavily confounded by the fact that the sickest infants are the ones ligated. Reading that association as causation leads either to reflex avoidance of a needed ligation or to defensive practice. The disciplined answer, after Weisz and McNamara, is to weigh ligation on its haemodynamic merits while acknowledging that the long-term risk reflects both the operation and the illness it was treating. [10]
Finally, the fluid pitfall: generous fluid intake in the first days enlarges the shunt and sustains patency, and aggressive volume boluses to treat the steal-driven hypotension worsen the over-circulation. Disciplined fluid management is both a preventive and a therapeutic measure, and the candidate who frames it as part of the management ladder answers completely. [13] [11]
Prognosis & Disposition
The single most important prognostic fact is that most preterm ducts close spontaneously. With a contemporary expectant approach, more than half of even extremely low birth weight infants achieve closure without pharmacotherapy or surgery, and many of the remainder close after a single course of a cyclo-oxygenase inhibitor or paracetamol. Patience is usually rewarded. [1] [11]
The haemodynamically significant duct that persists beyond one to two weeks, especially in the extremely preterm, is associated with prolonged ventilation, bronchopulmonary dysplasia, a longer hospital stay and, in some studies, worse short-term neurodevelopmental outcomes. The unresolved question — whether the persistent duct causes these outcomes or merely marks the sickest infants — is the heart of the controversy, and the trials have not shown that closing the duct reliably prevents them. [6] [11] [12]
For the duct that remains open at discharge, the prognosis is still favourable. Most close within the first year, and surgical or transcatheter closure is deferred until the infant is larger, unless the shunt is imposing a haemodynamic burden. Transcatheter device occlusion is the standard approach for the duct that persists beyond infancy, performed by paediatric cardiology. [7] [13]
Disposition is to a tertiary neonatal unit with neonatologist-led functional echocardiography and cardiology support. Infants needing ligation require surgical availability, and those with prolonged significant ducts need coordinated follow-up of respiratory, renal and neurodevelopmental outcomes. The expectation the examiner wants is that most infants are managed conservatively in a tertiary NICU and discharged with a closing or closed duct and a follow-up plan. [13]
Special Populations
The extremely preterm infant (under 26 weeks) is the population at the centre of this topic. The patency rate is highest, the ductal smooth muscle most immature, the kidneys and gut most fragile, and the risk of bronchopulmonary dysplasia greatest. This is the group for whom the expectant-first evidence is strongest and for whom the harms of treatment weigh heaviest, demanding the most judicious weighing of each rung of the ladder. [11] [13]
The infant with renal dysfunction reframes the drug choice. Cyclo-oxygenase inhibitors reduce renal blood flow and worsen oliguria and the creatinine, so paracetamol is the preferred agent when closure is necessary. The renal steal of the significant duct itself must be distinguished from drug-induced injury, because both can coexist and both raise the creatinine. [4] [13]
The infant with necrotising enterocolitis or gut ischaemia is the population in whom cyclo-oxygenase inhibitors are relatively contraindicated, because they reduce mesenteric perfusion and are linked to intestinal perforation. Paracetamol may be safer, and surgical ligation is considered when pharmacotherapy is unsafe or has failed. The decision is made jointly with the surgical team. [13] [10]
The infant with a duct-dependent circulation is the population in whom closure must not occur. Hypoplastic left heart syndrome, critical coarctation, interrupted aortic arch, and pulmonary atresia with a duct-dependent supply all rely on the duct. Prostaglandin E1 is given to keep it open, and the duct is maintained until definitive cardiac surgery. Confusing a duct-dependent lesion with a preterm PDA and treating with a cyclo-oxygenase inhibitor is a catastrophic, avoidable error — the structurally normal heart must be confirmed first. [7]
In the low-resource setting, where functional echocardiography and the full pharmacological armamentarium may be unavailable, the clinical end-organ assessment carries the decision. Ibuprofen (including the oral preparation) is accessible and effective, and the expectant-first principle is if anything more important, because the capacity to rescue from treatment-related complications is limited. The emphasis is on supportive care, fluid discipline, and clear criteria for referral to a higher-level centre. [13]
Evidence, Guidelines & Regional Differences
The defining feature of the modern evidence base is the failure of routine closure to improve long-term outcomes, despite reliable ductal closure rates. The BeNeDuct trial randomised preterm infants to early ibuprofen or expectant management and found no difference in death or bronchopulmonary dysplasia. The PDA-TOLERATE trial treated moderate-to-large ducts at one week and likewise found no benefit. The Cochrane review of early treatment versus expectant management confirms the picture. [1] [6] [11]
The pharmacological evidence, by contrast, is clear on efficacy. The network meta-analysis of Mitra and colleagues showed that ibuprofen, indomethacin and paracetamol each increase closure compared with placebo, with ibuprofen and paracetamol favoured over indomethacin for safety. The Cochrane reviews of ibuprofen and paracetamol corroborate this. The drugs work; what the trials question is whether using them routinely changes the outcomes that matter. [2] [3] [4]
Prophylactic indomethacin sits in its own evidence compartment. The Fowlie Cochrane review established that it reduces early severe intraventricular haemorrhage and ductal patency, but it does not improve survival without bronchopulmonary dysplasia or long-term neurodevelopment. The Mitra overview of Cochrane reviews places the whole PDA intervention field in context, and the Liebowitz secondary analyses of PDA-TOLERATE add that the comparative effectiveness of the drugs is modest and that equipoise in the real world is poor — infants treated outside trials were sicker. [5] [8] [9] [12]
Regional practice has converged on the expectant-first paradigm but with local texture. In Australia and Aotearoa New Zealand, neonatal networks favour expectant management with neonatologist-led functional echocardiography, treating only the haemodynamically significant duct with end-organ effects. In the United Kingdom, BAPM guidance supports the same conservative-first approach with regional cardiology support. In North America, practice is more variable but has shifted firmly toward conservatism, led in Canada by the group producing much of the contemporary Cochrane evidence. In Europe, paracetamol is increasingly first-line. [13] [11]
The live controversy the examiner will probe is whether a subset of preterm infants — perhaps those with the largest shunts and clearest end-organ compromise — does benefit from closure, and how to identify them. The honest answer is that the trials, powered on composite outcomes, have not resolved this, and that the current standard is targeted treatment of the infant with a significant duct causing measurable harm, with the evidence and its limits explained openly to the family. [11] [13]
Exam Pearls
State the one-liner mechanism: the preterm ductus fails to close because its immature smooth muscle contracts weakly to oxygen and stays sensitive to the relaxing prostaglandins, and it becomes significant when the falling pulmonary vascular resistance opens a large left-to-right shunt. Most close spontaneously; treat the haemodynamically significant duct causing end-organ compromise, not the echo. [7] [13]
State the bedside triad: bounding pulses, hyperdynamic precordium, widened pulse pressure — with the machinery murmur at the upper left sternal edge as a softer, inconstant fourth. The renal and diastolic signs of the steal precede the murmur. [13]
State the echo markers of significance: duct diameter above 1.5 mm, left atrial-to-aortic root ratio above 1.5, and diastolic flow reversal in the descending aorta. Significance is a constellation, not a single number, and it must agree with the clinical end-organ picture. [12] [13]
State the drug doses: ibuprofen 10 mg/kg then 5 mg/kg at 24 and 48 hours; paracetamol 15 mg/kg every six hours; indomethacin 0.2 mg/kg every 12 to 24 hours for three doses. Paracetamol is favoured when renal function is impaired; cyclo-oxygenase inhibitors are avoided in necrotising enterocolitis and oliguria. [2] [3] [4]
State the evidence: BeNeDuct and PDA-TOLERATE showed no benefit of routine early closure; prophylactic indomethacin reduces intraventricular haemorrhage but not death, bronchopulmonary dysplasia or neurodevelopment; ligation harm is confounded by indication (causality or bias). The closing trap is treating the echo; the opening trap is missing a duct-dependent circulation. [1] [5] [10] [11]
References
- [1]Hundscheid T, Onland W, Kooi EMW, et al Expectant Management or Early Ibuprofen for Patent Ductus Arteriosus. N Engl J Med, 2023.PMID 36477458
- [2]Mitra S, Florez ID, Tamayo ME, et al Association of Placebo, Indomethacin, Ibuprofen, and Acetaminophen With Closure of Hemodynamically Significant Patent Ductus Arteriosus in Preterm Infants: A Systematic Review and Meta-analysis. JAMA, 2018.PMID 29584842
- [3]Ohlsson A, Walia R, Shah SS Ibuprofen for the treatment of patent ductus arteriosus in preterm or low birth weight (or both) infants. Cochrane Database Syst Rev, 2020.PMID 32045960
- [4]Jasani B, Mitra S, Shah PS Paracetamol (acetaminophen) for patent ductus arteriosus in preterm or low birth weight infants. Cochrane Database Syst Rev, 2022.PMID 36519620
- [5]Fowlie PW, Davis PG, McGuire W Prophylactic intravenous indomethacin for preventing mortality and morbidity in preterm infants. Cochrane Database Syst Rev, 2010.PMID 20614421
- [6]Clyman RI, Liebowitz M, Kaempf J, et al PDA-TOLERATE Trial: An Exploratory Randomized Controlled Trial of Treatment of Moderate-to-Large Patent Ductus Arteriosus at 1 Week of Age. J Pediatr, 2019.PMID 30340932
- [7]Benitz WE, Committee on Fetus and Newborn, American Academy of Pediatrics Patent Ductus Arteriosus in Preterm Infants. Pediatrics, 2016.PMID 26672023
- [8]Liebowitz M, Kaempf J, Erdeve O, et al Comparative effectiveness of drugs used to constrict the patent ductus arteriosus: a secondary analysis of the PDA-TOLERATE trial. J Perinatol, 2019.PMID 30850756
- [9]Liebowitz M, Katheria A, Sauberan J, et al Lack of Equipoise in the PDA-TOLERATE Trial: A Comparison of Eligible Infants Enrolled in the Trial and Those Treated Outside the Trial. J Pediatr, 2019.PMID 31255386
- [10]Weisz DE, McNamara PJ Patent ductus arteriosus ligation and adverse outcomes: causality or bias? J Clin Neonatol, 2014.PMID 25024972
- [11]Mitra S, Scrivens A, Fiander M, et al Early treatment versus expectant management of hemodynamically significant patent ductus arteriosus for preterm infants. Cochrane Database Syst Rev, 2025.PMID 40548426
- [12]Mitra S, de Boode WP, Weisz DE, et al Interventions for patent ductus arteriosus (PDA) in preterm infants: an overview of Cochrane Systematic Reviews. Cochrane Database Syst Rev, 2023.PMID 37039501
- [13]Mitra S, Weisz D, Jain A, et al Management of the patent ductus arteriosus in preterm infants. Paediatr Child Health, 2022.PMID 35273674
- [14]Chorne N, Jegatheesan P, Lin E, et al Risk factors for persistent ductus arteriosus patency during indomethacin treatment. J Pediatr, 2007.PMID 18035143