Paeds · fetal-neonatal-and-perinatal
Perinatal infection screening and prevention
Also known as Group B Streptococcus (GBS) screening · Intrapartum antibiotic prophylaxis · Mother-to-child transmission (MTCT) · Congenital infection prevention · TORCH screening · Vertical transmission prevention
Fellowship guide to preventing mother-to-child infection: the universal antenatal screen (HIV, hepatitis B, syphilis, rubella), Group B Streptococcus screening and intrapartum prophylaxis, hepatitis B and HIV neonatal prophylaxis, and the assessment of the exposed or unwell neonate.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the handover at a busy birth. A term infant has just arrived and the midwife mentions the mother is "GBS positive, two doses of penicillin given". Before you examine the baby, you have already started preventing disease. That handover — a screen result turned into an intervention — is the whole of this topic. [3]
A perinatal infection is any infection transmitted from the mother to the fetus or newborn around the time of birth — through the placenta, up the genital tract, across the birth canal, or in breast milk. The catalogue is long, from Group B Streptococcus to cytomegalovirus to syphilis, but the paediatric question is always the same: was the mother screened, was the result acted on, and what does the baby need now? [1] [3]
Two ideas run through everything that follows. First, vertical transmission is usually preventable, and the interventions that prevent it — maternal treatment, intrapartum antibiotics, neonatal prophylaxis and immunisation — are cheap, old and effective. [6] [9] Second, the screen is only useful if it changes management. A positive GBS swab changes nothing for the mother at the booking visit; it only matters once labour begins. So the discipline of perinatal infection care is not running tests but closing the loop from result to action, for every mother, every time. [3]
Classification
Sort the organisms two ways — by how they reach the baby, and by how you screen for them. [3]
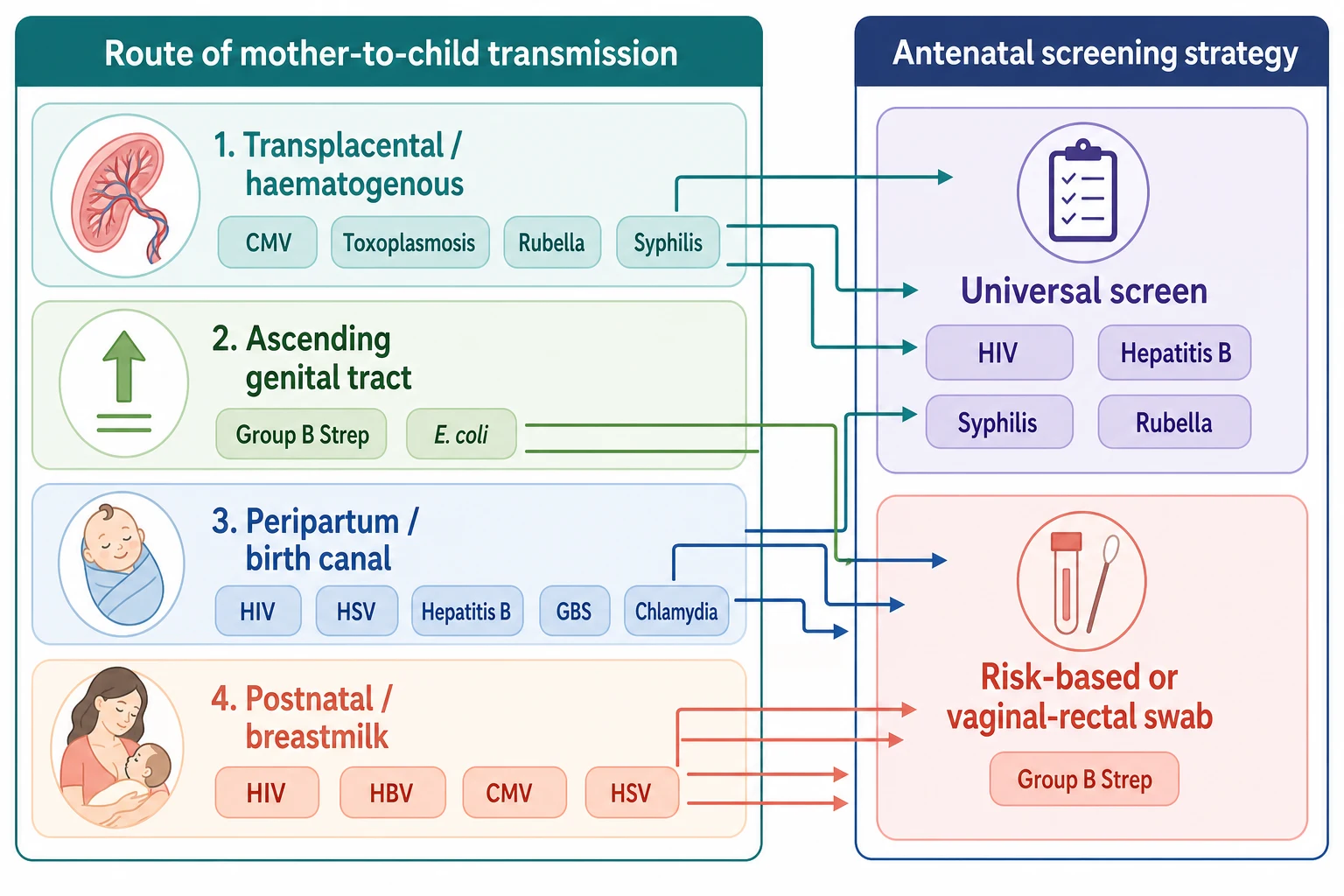
By route of transmission, the picture maps onto four pathways. Transplacental (haematogenous) organisms cross the placenta at any gestation — these are the classic TORCH infections, cytomegalovirus, toxoplasmosis, rubella, and syphilis. Ascending organisms climb from the vagina through the cervix into the uterus, especially after rupture of the membranes — Group B Streptococcus and Escherichia coli. Peripartum organisms infect the baby as it passes through the birth canal in contact with blood and secretions — HIV, herpes simplex virus, hepatitis B, GBS, chlamydia and gonorrhoea. Postnatal organisms are acquired through breastfeeding or close contact — HIV, hepatitis B, CMV and HSV. [1] [14]
By screening strategy, the field divides cleanly in two. Four infections are screened universally because they are common, serious and actionable: HIV, hepatitis B, syphilis and rubella, performed at the booking antenatal visit. [11] GBS is the exception — screened by a vaginal-rectal swab late in pregnancy (universal in some countries) or managed by a risk-based approach (others). [3] The remaining infections, such as CMV, toxoplasmosis, HSV and parvovirus, are not screened for universally because there is no cheap, accurate, actionable test in the well mother; they are investigated only when a clinical trigger appears.
Epidemiology & Risk Factors
Group B Streptococcus colonises the gastrointestinal and genital tracts of roughly one in five pregnant women worldwide, and it remains the leading bacterial cause of early-onset neonatal sepsis in high-income settings. [2] Before intrapartum antibiotic prophylaxis, the burden was large and the mortality real; the introduction of screening and prophylaxis cut early-onset GBS disease dramatically, and Stoll's more recent data show that as GBS fell, Gram-negative organisms such as E. coli rose to share the early-onset sepsis burden, especially in preterm infants. [1] [5]
The other heavy hitters carry their own epidemiology. Untreated maternal syphilis ends in serious adverse outcomes — stillbirth, neonatal death, prematurity or congenital syphilis — in well over half of pregnancies, which is why universal antenatal screening and treatment is one of the most cost-effective interventions in all of medicine. [10] Cytomegalovirus is the commonest congenital infection in the developed world, and although most infected newborns are asymptomatic, it is the leading non-genetic cause of sensorineural hearing loss in children. [12]
Risk factors for vertical transmission cluster around three drivers. Maternal load and organism set the baseline risk — a high HIV viral load or an untreated high syphilis titre transmits readily. [6] Timing and breach of barriers raise risk — prolonged rupture of membranes, prematurity, chorioamnionitis and instrumented or traumatic delivery all open a door for ascending and birth-canal organisms. [3] Gaps in care are the most dangerous and the most preventable — late booking, no records, missed screening, and failure to act on a positive result each break a link in the chain. [9]
Pathophysiology
To understand why each organism needs a different intervention, follow the four pathways from mother to baby and the barriers in between. [1]
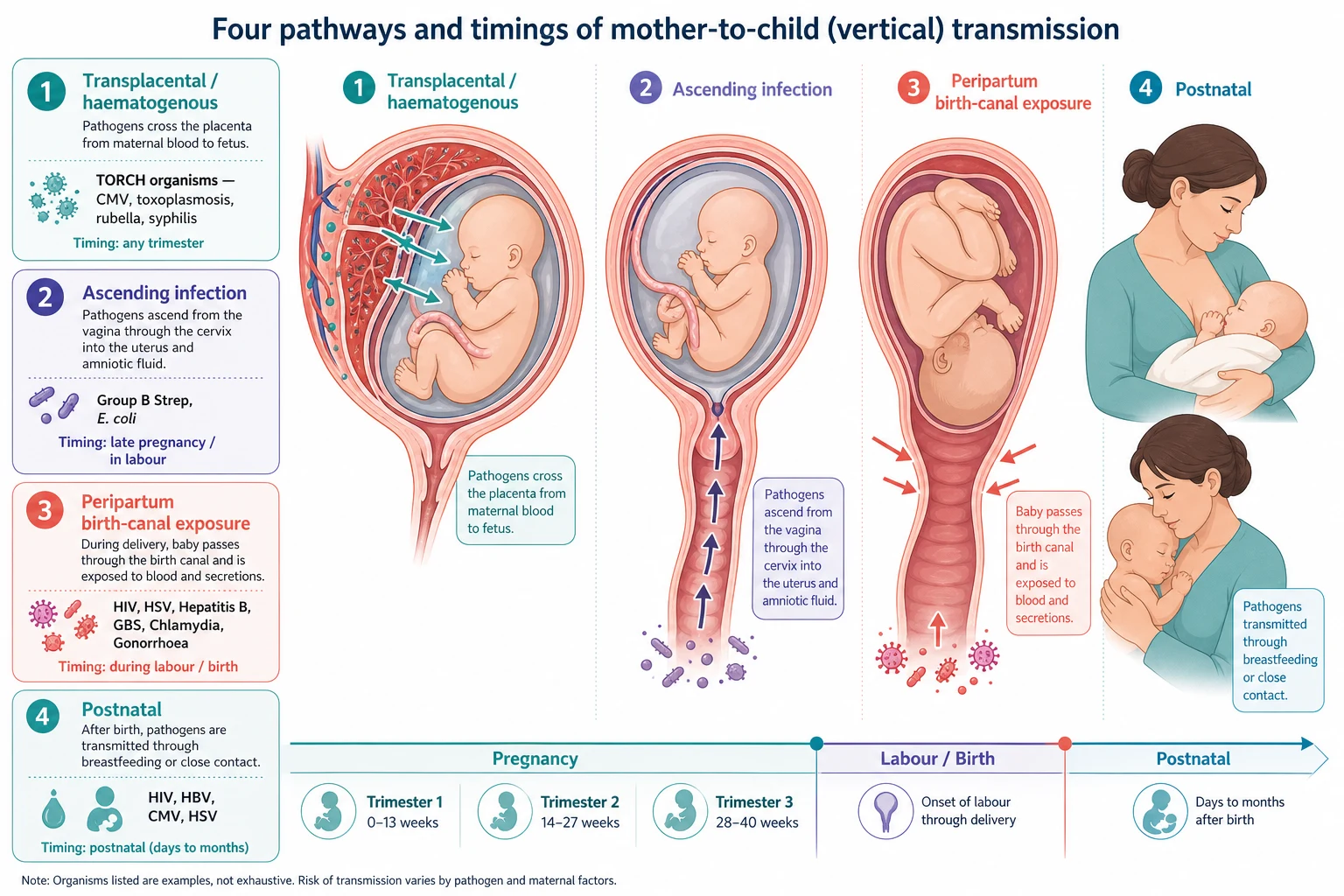
The placenta is the first barrier, and it is a good one against most bacteria — but the TORCH organisms have evolved to cross it, so they can infect the fetus directly through the bloodstream at any trimester. [12] This is why congenital CMV, toxoplasmosis, rubella and syphilis can damage the fetus long before labour, producing the classic stigmata of microcephaly, hepatosplenomegaly, chorioretinitis, sensorineural hearing loss and growth restriction. [12] [15]
The amniotic membranes are the second barrier, and once they rupture, bacteria from the lower genital tract can ascend. The longer the rupture, the higher the risk — prolonged rupture of membranes is a key driver of ascending GBS and E. coli infection, and clinical chorioamnionitis (maternal fever with fetal tachycardia) marks established intrauterine infection. [3]
The birth canal is the third barrier, and peripartum exposure is the moment of highest risk for several organisms. The baby swallows and is bathed in maternal blood and secretions; HIV, HSV, hepatitis B, GBS, chlamydia and gonorrhoea are all acquired here. This is precisely why intrapartum interventions work — maternal antiretroviral therapy suppresses the viral load before the baby is exposed, intrapartum penicillin lowers the GBS inoculum, and planning delivery around a primary HSV lesion avoids the most dangerous contact. [6] [14]
Finally, breast milk carries HIV, CMV, hepatitis B and HSV postnatally. For HIV this shapes the infant feeding decision and the role of extended infant prophylaxis, while for CMV it is mostly a concern for the very preterm or immunocompromised infant of a CMV-positive mother. [8] [12]
Clinical Presentation
Most of this topic is silent. The screened and treated mother has no symptoms, and the well newborn needs no examination finding to justify prevention — the result drives the action. The clinical presentations appear when the chain has broken, and they declare themselves in two patterns. [3]
The first pattern is early-onset neonatal sepsis, overwhelmingly a GBS and E. coli story within the first 72 hours of life. The baby shows respiratory distress, grunting, tachypnoea or apnoea, temperature instability, poor feeding and lethargy; in the worst cases there is septic shock, pneumonia and pulmonary hypertension. [1] [5] A GBS-colonised mother who did not receive adequate intrapartum antibiotics is the classic setup, and prematurity amplifies the risk.
The second pattern is the stigmata of congenital infection, the footprint of an organism that crossed the placenta. Look for petechiae and a "blueberry muffin" rash, hepatosplenomegaly, jaundice, thrombocytopenia, chorioretinitis, sensorineural hearing loss, microcephaly, intracranial calcifications and growth restriction. [12] These findings point to the TORCH group rather than to GBS, and they widen the differential from "is this sepsis?" to "which congenital infection is this?". [15]
A few organisms have distinctive presentations worth knowing cold. Neonatal HSV presents at one to three weeks with skin vesicles, or catastrophically with encephalopathy or fulminant hepatitis and sepsis-like illness; the maternal history is often a primary genital lesion near delivery. [14] Congenital syphilis can present with stillbirth or hydrops, or at a few weeks with rash, snuffles, hepatosplenomegaly and bony changes. [10] Symptomatic congenital CMV brings thrombocytopenia, petechiae, hepatosplenomegaly and sensorineural hearing loss, and is the one congenital infection with proven antiviral therapy. [13]
Differential Diagnosis
The differential turns on a single triage question: is this early-onset bacterial sepsis, a congenital infection, or something else? [5]
Early-onset sepsis is the urgent, common and treatable default for any unwell neonate in the first 72 hours. GBS and E. coli lead, and the decision is empirical — start antibiotics within the hour and investigate to confirm, rather than wait for a culture. [1] [5] Chorioamnionitis, prolonged rupture of membranes, prematurity and maternal GBS colonisation without prophylaxis all push toward this diagnosis.
When the picture is stigmata rather than sepsis — petechiae, organomegaly, chorioretinitis, hearing loss, microcephaly, growth restriction — think the TORCH differential and test accordingly: CMV PCR in urine and saliva, toxoplasma and rubella serology, syphilis serology, and HSV PCR if vesicles or encephalopathy are present. [12] [15] Always remember that congenital infection also causes growth restriction and can mimic placental insufficiency, so a small-for-gestational-age infant with stigmata deserves a congenital infection workup, not reassurance. [12]
Beware the mimics. Respiratory distress in a term infant can be transient tachypnoea of the newborn, respiratory distress syndrome, or meconium aspiration — but in an at-risk infant you must treat sepsis as the assumption until proven otherwise. [5] And remember that a normal maternal screen at booking is only a snapshot: a mother with a new HSV primary lesion at term, or a fresh syphilis exposure, can still transmit even with clean booking results. [10] [14]
Clinical & Bedside Assessment
Begin with the maternal record, not the baby. For any neonate with infection exposure or illness, work through three questions in order: what was the mother screened for, what were the results, and what was done about each? [3] Document the booking screen (HIV, hepatitis B, syphilis, rubella), the GBS status and how it was determined, the timing and adequacy of any intrapartum antibiotics, the duration of rupture of membranes, any intrapartum fever or chorioamnionitis, and any maternal lesions or new symptoms. [3] [9]
Examine the baby with two lenses at once. The sepsis lens looks for respiratory distress, grunting, tachypnoea (a sustained respiratory rate above 60), apnoea, temperature instability, poor perfusion, lethargy and poor feeding — any of which in an at-risk infant justifies investigation and empiric treatment. [1] The congenital infection lens looks for growth restriction, microcephaly, rash and petechiae, hepatosplenomegaly, jaundice, cataracts and chorioretinitis, and an abnormal neurological or hearing finding. [12]
Assess function and trend it. A single normal observation at one hour means little; the value is in the trajectory over the first day. Use a structured observation tool and a documented plan that names who escalates and when, so a baby drifting toward sepsis is caught early rather than late. [3]
Finally, synthesise. A clean one-line summary sounds like: "A term male born after 18 hours of ruptured membranes to a GBS-positive mother who received one dose of penicillin, now grunting and tachypnoeic at four hours — probable early-onset GBS sepsis; start septic workup and empiric antibiotics." That sentence tells the team the risk, the likelihood, and the first move. [1] [3]
Investigations
Investigation is targeted, not blanket. The well, at-risk infant whose mother received adequate prophylaxis needs far less than the symptomatic infant or the baby of a mother with no records. [3]
The limited evaluation of the well GBS-at-risk infant — the baby whose mother had inadequate intrapartum antibiotics but who looks and behaves well — is a blood culture and a full blood count with differential at 24 to 48 hours, without routine lumbar puncture or empiric antibiotics. [3] The full septic screen of the symptomatic infant adds a lumbar puncture (cell count, protein, glucose, culture and HSV PCR if indicated), C-reactive protein, chest radiograph, and electrolytes and blood gas as the clinical picture demands. [5] Start empiric intravenous antibiotics first, then refine.
For suspected congenital infection, send the targeted panel. CMV is best detected by PCR on urine or saliva collected within the first three weeks; toxoplasmosis and rubella are serological; syphilis uses a treponemal test plus a non-treponemal titre; and HSV is PCR on surface swabs and cerebrospinal fluid. [12] [15] Hearing assessment (automated auditory brainstem response) is part of the congenital infection workup because CMV is the leading cause of sensorineural hearing loss. [12]
Know what to avoid. Do not culture or image a well baby purely to reassure yourself. Do not delay empiric antibiotics waiting for a full septic screen in a sick neonate. And never assume that a normal full blood count excludes sepsis — a single early count can be normal in a genuinely septic infant, so trend the picture clinically. [5]
Screen the mother for these four
Management — Resuscitation
Most babies in this topic are not resuscitated — they are protected before they ever become unwell. But when a baby does present with early-onset sepsis, the first hour is decisive, and resuscitation follows the standard neonatal life support algorithm while you begin empiric treatment in parallel. [5]
Stabilise airway, breathing and circulation; give supplemental oxygen and respiratory support for respiratory failure; establish intravenous access; and treat hypotension and poor perfusion with fluid boluses and inotropes as needed. The septic neonate can decompensate from pulmonary hypertension and shock, so escalate early to the neonatal team and plan retrieval in a rural setting before the baby is in extremis. [1] [5]
The two resuscitation moves specific to infection are empiric antibiotics and antiviral coverage. Start intravenous benzylpenicillin plus gentamicin (or ampicillin plus gentamicin) immediately after taking cultures for suspected early-onset sepsis, covering GBS and E. coli. [1] [3] Add intravenous aciclovir urgently if HSV is plausible — vesicles, encephalopathy, fulminant hepatitis, or a maternal primary HSV lesion — because delayed antiviral therapy costs lives and brains. [14]
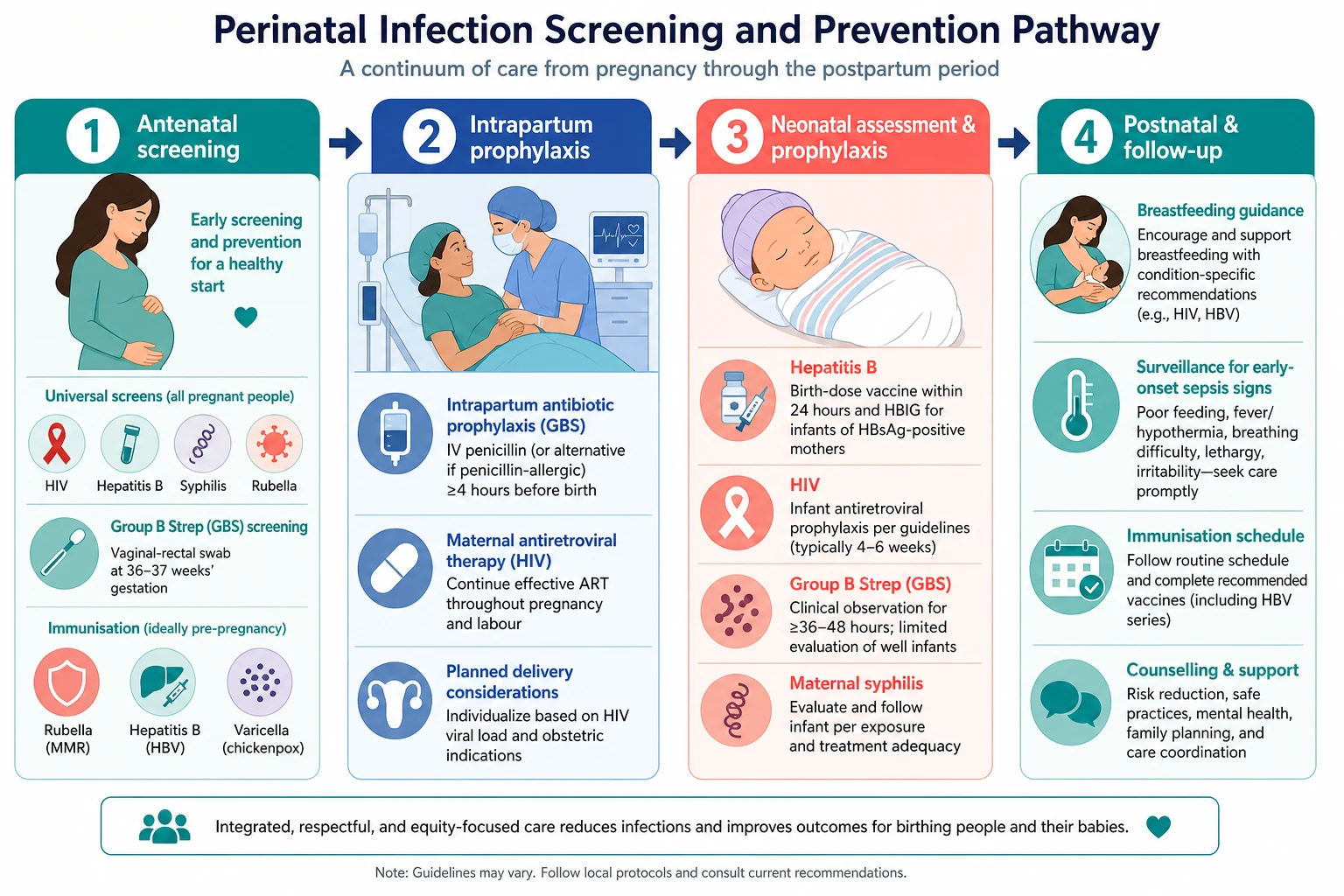
For prevention at resuscitation, two invisible acts matter most. Give the hepatitis B birth-dose vaccine (and HBIG for an HBsAg-positive mother) within 12 hours of birth to any exposed or unvaccinated-status infant. [9] And start infant antiretroviral prophylaxis for the HIV-exposed neonate as soon as possible after birth, with the regimen chosen by the HIV team on the basis of maternal viral load. [6] [7]
Management — Definitive & Stepwise
Once the baby is stable, definitive perinatal infection care is best organised organism by organism. For each, know the screen, the maternal intervention, and what the newborn needs. [3]
Group B Streptococcus is prevented by intrapartum antibiotic prophylaxis. Screen at 36 to 37 weeks by vaginal-rectal swab (or use a risk-based approach), and give intrapartum intravenous benzylpenicillin in labour to colonised or at-risk mothers. [3] The Cochrane review confirms that intrapartum antibiotics for known colonisation reduce early-onset GBS disease, though the evidence base for the universal screening strategy itself is more limited. [4]
Intravenous benzylpenicillin
Dose
initial 2.4 g (3 million units), then 1.2 g every 4 hours until delivery
For the HIV-exposed infant, prevention is a package that begins in pregnancy: maternal combination antiretroviral therapy to suppress the viral load, consideration of mode and timing of delivery, infant antiretroviral prophylaxis from birth, and an infant feeding plan. [6] The legacy of PACTG 076 — zidovudine during pregnancy, labour and to the neonate — was the first proof that vertical transmission could be slashed, and modern combination therapy now brings transmission below one to two percent. [6] When maternal viral load is not suppressed, the CHER trial's lesson that early treatment of the infant saves lives underpins more intensive neonatal prophylaxis. [7] [8]
For hepatitis B, prevention hinges on the birth dose. Give hepatitis B vaccine to every newborn, and add hepatitis B immunoglobulin (HBIG) within 12 hours to infants of HBsAg-positive mothers (and to infants whose mother's status is unknown, pending testing). [9] This combination prevents the great majority of perinatal HBV transmission and the chronic carriage that would otherwise follow. [9]
For syphilis, treat the mother in pregnancy with intramuscular benzathine penicillin, which prevents almost all congenital syphilis if given adequately and early enough before delivery. [10] The untreated or partially treated mother risks stillbirth and congenital syphilis, so confirm the maternal treatment was appropriate, the dose complete, and the interval to delivery adequate — and evaluate the infant accordingly. [10]
For HSV, the decisive act is usually obstetric: a caesarean before membrane rupture for a mother with a primary genital lesion or prodrome near delivery. [14] If neonatal HSV is suspected or confirmed, treat with high-dose intravenous aciclovir; prevention rests on recognising the maternal lesion and avoiding contact at the most dangerous moment. [14]
For congenital CMV, there is no antenatal screen, but a symptomatic infant benefits from treatment — the Kimberlin trial showed that six months of oral valganciclovir improves audiologic and neurodevelopmental outcomes in symptomatic congenital CMV disease. [13] Toxoplasmosis in pregnancy is managed with spiramycin or combination pyrimethamine and sulfadiazine, with the Mandelbrot trial informing the choice and timing of therapy. [15]
Perinatal infection numbers for viva recall
Specific Subtypes & Scenarios
The GBS-at-risk term infant whose mother had inadequate prophylaxis. If the baby is well, perform a limited evaluation (blood culture and full blood count at 24 to 48 hours) and observe; if unwell, perform a full septic screen and start empiric benzylpenicillin and gentamicin. The decision is clinical and the threshold to treat is low. [3]
The HIV-exposed neonate. Start infant antiretroviral prophylaxis as soon as possible after birth, choose the regimen with the HIV team based on maternal viral load and resistance history, plan early virological testing (HIV PCR), and agree an infant feeding plan that is safe and supported. [6] [7] The CHER and HPTN 046 trials frame why early infant therapy and extended prophylaxis matter. [7] [8]
The hepatitis B exposed infant (HBsAg-positive mother). Give hepatitis B vaccine plus HBIG within 12 hours, complete the vaccine series, and arrange serological follow-up after the series to confirm protection rather than chronic carriage. [9]
Maternal syphilis — treated or uncertain. Confirm the maternal treatment was adequate, the appropriate benzathine penicillin regimen, and that enough time elapsed before delivery. Investigate and treat the infant on the basis of maternal treatment adequacy and infant clinical and serological findings. [10]
Neonatal HSV. Any vesicular lesion, unexplained encephalopathy, or fulminant sepsis-like hepatitis in the first three weeks demands urgent intravenous aciclovir and PCR confirmation. Maternal history of a primary genital lesion near delivery is the strongest risk factor. [14]
The mother with no antenatal records. Treat as unknown risk, not low risk. Test for HIV and hepatitis B urgently, treat the infant as potentially exposed until results return, and screen for syphilis. Default to action over reassurance. [3] [9]
Preterm prolonged rupture of membranes and chorioamnionitis. These raise the risk of ascending GBS and E. coli infection substantially; the preterm infant is doubly vulnerable, so maintain a low threshold for evaluation and empiric antibiotics. [5]
Complications & Pitfalls
Short-term complications are the acute emergencies — early-onset sepsis with shock and pulmonary hypertension, neonatal HSV encephalitis, fulminant hepatitis, and the pneumonia and respiratory failure of GBS. [1] [14] Long-term complications are the chronic legacies of congenital infection — sensorineural hearing loss and neurodevelopmental impairment from CMV, congenital defects from rubella, stillbirth and bony or neurosyphilis from untreated syphilis, and chronic hepatitis and hepatocellular carcinoma from perinatally acquired hepatitis B. [9] [12]
The common pitfalls are predictable, and worth naming so you avoid them. Treating a normal maternal booking screen as a permanent guarantee — a clean result at twelve weeks does not protect against a new HSV or syphilis exposure at term. [10] [14] Reassuring yourself with a single normal full blood count in an at-risk infant, when only the clinical trend over hours tells the truth. [5] Forgetting the birth dose of hepatitis B vaccine because the baby looked well, missing the one cheap intervention that prevents lifelong carriage. [9] Assuming "no records" means "low risk" rather than "unknown risk" — the default must be to screen and to protect. [3] And fragmenting care across the maternity-to-paediatric handover, so a positive screen result never reaches the person who can act on it. [3] [9]
Prognosis & Disposition
Outcome depends on the organism, the timeliness of prevention, and the gestational age of the infant — and for most screened and treated infants it is excellent. A well GBS-at-risk infant whose mother received adequate prophylaxis can stay with mother with observation. A symptomatic infant with early-onset sepsis goes to NICU for empiric antibiotics and support, and the mortality and morbidity rise with prematurity, shock and delay in treatment. [1] [5]
For the congenital infections, prognosis is organism-specific. With adequate treatment, symptomatic congenital CMV has improved audiologic and developmental outcomes, though some sensorineural hearing loss and neurodevelopmental impairment persist. [13] Untreated syphilis carries a heavy burden of stillbirth and congenital disease that adequate maternal treatment almost abolishes. [10] The HIV-exposed infant, with modern prevention, is overwhelmingly likely to be uninfected, with a normal outlook — one of the great successes of preventive medicine. [6] [7]
Disposition follows the risk. A well term infant with adequate maternal prophylaxis stays with mother with monitoring; an unwell or high-risk infant goes to a transitional or NICU environment; and every at-risk infant leaves hospital with a documented plan for immunisation completion, hearing testing where indicated, and clear safety-net advice for the family. [3]
Special Populations
Migrant, refugee and asylum-seeking families may have had fragmented or no antenatal care and carry a higher burden of undiagnosed HIV, hepatitis B and syphilis. Treat unknown status as a reason to test and to protect the infant, use interpreters, and ensure results and follow-up are not lost in transition. [9] [10]
Indigenous and socioeconomically disadvantaged families carry higher rates of STIs, GBS disease and late presentation in many settings. Provide culturally safe, accessible antenatal and postnatal care, address the social drivers of late screening, and ensure the prevention loop closes for every mother. [2] [10]
Rural and remote settings must plan antenatal transfer to a service with screening and neonatal capability before delivery wherever possible; an unwell septic neonate born far from support is an avoidable crisis, so plan early and retrieve early. [1]
Immunocompromised and very preterm infants are uniquely vulnerable — a CMV-positive unit of breast milk, a GBS inoculum, or an HSV exposure that a term infant would shrug off can devastate a 26-week neonate. Tailor feeding, prophylaxis and surveillance to the added risk. [5] [12]
Families with no or incomplete immunisation records need catch-up planning — the rubella-negative mother should be vaccinated postnatally, and the infant's hepatitis B and routine schedule must be confirmed and completed. [9] [11]
Evidence, Guidelines & Regional Differences
The foundational evidence frames every organism. Schrag's population data documented the load of GBS disease in the era of intrapartum prophylaxis; [1] Russell's worldwide systematic review quantified maternal GBS colonisation at around one in five women and the serotype distribution that shapes vaccine design; [2] and Stoll's recent surveillance captured the rise of E. coli as a counterweight to GBS in early-onset sepsis, especially among preterm infants. [5] The Ohlsson Cochrane review supports intrapartum antibiotics for known maternal GBS colonisation, while remaining honest about the limits of the evidence for the screening strategy itself. [4]
For HIV, PACTG 076 (Connor 1994) was the turning point — the first proof that antiretroviral therapy cuts mother-to-child transmission; [6] the CHER trial (Violari 2008) showed that early treatment of infected infants saves lives; [7] and HPTN 046 (Coovadia 2012) demonstrated that extended infant nevirapine prevents breastfeeding transmission. [8] For hepatitis B, the ACIP recommendations (Schillie 2018) codify the birth-dose strategy; [9] for syphilis, Gomez's systematic review quantified the grim outcomes of untreated maternal infection; [10] for CMV, Kenneson and Cannon defined the epidemiology [12] and Kimberlin proved valganciclovir helps symptomatic infants. [13] Corey's review remains the definitive HSV reference. [14]
Two live controversies sit beneath the guidelines: whether to screen universally for GBS (the US does, the UK does not, and the Cochrane evidence for screening over risk-based management is incomplete), and the horizon of a maternal GBS vaccine, which could shift prevention upstream from swabs and antibiotics. [2] [4]
Exam Pearls
- The big four universal antenatal screens are HIV, hepatitis B, syphilis, rubella — each has an intervention. GBS is added by swab or by risk. [3] [11]
- GBS is prevented by intrapartum antibiotic prophylaxis; the Cochrane review supports antibiotics for known colonisation, though the evidence for the screening strategy itself is limited. [4]
- Inadequate maternal GBS prophylaxis plus an unwell infant equals empiric benzylpenicillin and gentamicin; a well infant needs a limited evaluation and observation. [3]
- For HIV-exposed infants, prevention is a package — maternal ART, infant prophylaxis, mode of delivery, feeding plan — and brings transmission below 1–2%. [6] [7]
- Every newborn gets hepatitis B vaccine; infants of HBsAg-positive (or unknown-status) mothers get vaccine plus HBIG within 12 hours. [9]
- Untreated maternal syphilis causes stillbirth and congenital syphilis in over half of pregnancies — adequate benzathine penicillin prevents it. [10]
- Neonatal HSV presents at 1–3 weeks with vesicles, encephalopathy or fulminant hepatitis — give IV aciclovir urgently. [14]
- Symptomatic congenital CMV benefits from 6 months of valganciclovir (Kimberlin); CMV is the leading cause of sensorineural hearing loss. [13]
- "No antenatal records" means unknown risk, not low risk — test and protect the infant. [3]
- The chain is screen → intervene → protect → observe; a break at any link is the commonest reason for a preventable perinatal infection. [3] [9]
References
- [1]Schrag SJ Group B streptococcal disease in the era of intrapartum antibiotic prophylaxis. New England Journal of Medicine, 2000.PMID 10620644
- [2]Russell NJ Maternal Colonization With Group B Streptococcus and Serotype Distribution Worldwide: Systematic Review and Meta-analyses. Clinical Infectious Diseases, 2017.PMID 29117327
- [3]Verani JR Prevention of perinatal group B streptococcal disease--revised guidelines from CDC, 2010. MMWR Recommendations and Reports, 2010.PMID 21088663
- [4]Ohlsson A Intrapartum antibiotics for known maternal Group B streptococcal colonization. Cochrane Database of Systematic Reviews, 2014.PMID 24915629
- [5]Stoll BJ Early-Onset Neonatal Sepsis 2015 to 2017, the Rise of Escherichia coli, and the Need for Novel Prevention Strategies. JAMA Pediatrics, 2020.PMID 32364598
- [6]Connor EM Reduction of maternal-infant transmission of human immunodeficiency virus type 1 with zidovudine treatment. Pediatric AIDS Clinical Trials Group Protocol 076 Study Group. New England Journal of Medicine, 1994.PMID 7935654
- [7]Violari A Early antiretroviral therapy and mortality among HIV-infected infants. New England Journal of Medicine, 2008.PMID 19020325
- [8]Coovadia HM Efficacy and safety of an extended nevirapine regimen in infant children of breastfeeding mothers with HIV-1 infection for prevention of postnatal HIV-1 transmission (HPTN 046): a randomised, double-blind, placebo-controlled trial. Lancet, 2012.PMID 22196945
- [9]Schillie S Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recommendations and Reports, 2018.PMID 29939980
- [10]Gomez GB Untreated maternal syphilis and adverse outcomes of pregnancy: a systematic review and meta-analysis. Bulletin of the World Health Organization, 2013.PMID 23476094
- [11]Best JM Rubella. Seminars in Fetal & Neonatal Medicine, 2007.PMID 17337363
- [12]Kenneson A Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Reviews in Medical Virology, 2007.PMID 17579921
- [13]Kimberlin DW Valganciclovir for symptomatic congenital cytomegalovirus disease. New England Journal of Medicine, 2015.PMID 25738669
- [14]Corey L Maternal and neonatal herpes simplex virus infections. New England Journal of Medicine, 2009.PMID 19797284
- [15]Mandelbrot L Prenatal therapy with pyrimethamine + sulfadiazine vs spiramycin to reduce placental transmission of toxoplasmosis: a multicenter, randomized trial. American Journal of Obstetrics and Gynecology, 2018.PMID 29870736