Paeds · fetal-neonatal-and-perinatal
Persistent pulmonary hypertension of the newborn
Also known as Persistent pulmonary hypertension of the newborn
Fellowship guide to persistent pulmonary hypertension of the newborn.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A term infant born after meconium-stained liquor grunts, tachypnoeas, and turns blue within the first hour of life despite supplemental oxygen. This is the classic presentation of persistent pulmonary hypertension of the newborn (PPHN), one of the most time-critical diagnoses in neonatology. [1]
PPHN arises when the pulmonary vascular resistance fails to fall normally after birth. Blood continues to bypass the lungs through fetal channels — the foramen ovale, ductus arteriosus, and intrapulmonary shunts — producing profound, often refractory hypoxaemia. The condition carries a mortality of 4–33% and survivors face substantial neurodevelopmental risks. [1]
Epidemiology & Risk Factors
PPHN affects approximately 1.9 per 1000 live births and occurs almost exclusively in term and late-preterm infants (≥34 weeks). Boys are affected slightly more often than girls. [1]
The strongest prenatal risk factors are Caesarean delivery without labour, maternal diabetes, and late-preterm birth. Postnatal triggers include perinatal asphyxia, meconium aspiration syndrome, neonatal sepsis, and pneumonia. Pulmonary hypoplasia from congenital diaphragmatic hernia or prolonged oligohydramnios produces a particularly severe phenotype. [1]
Maternal SSRI use in late pregnancy drew intense attention after the landmark 2006 NEJM study showed an approximate doubling of PPHN risk. The absolute risk remains small (number needed to harm ≈250), and stopping antidepressants risks maternal relapse. The consensus is to continue SSRIs when clinically indicated and heighten surveillance at delivery. [2]
Pathophysiology
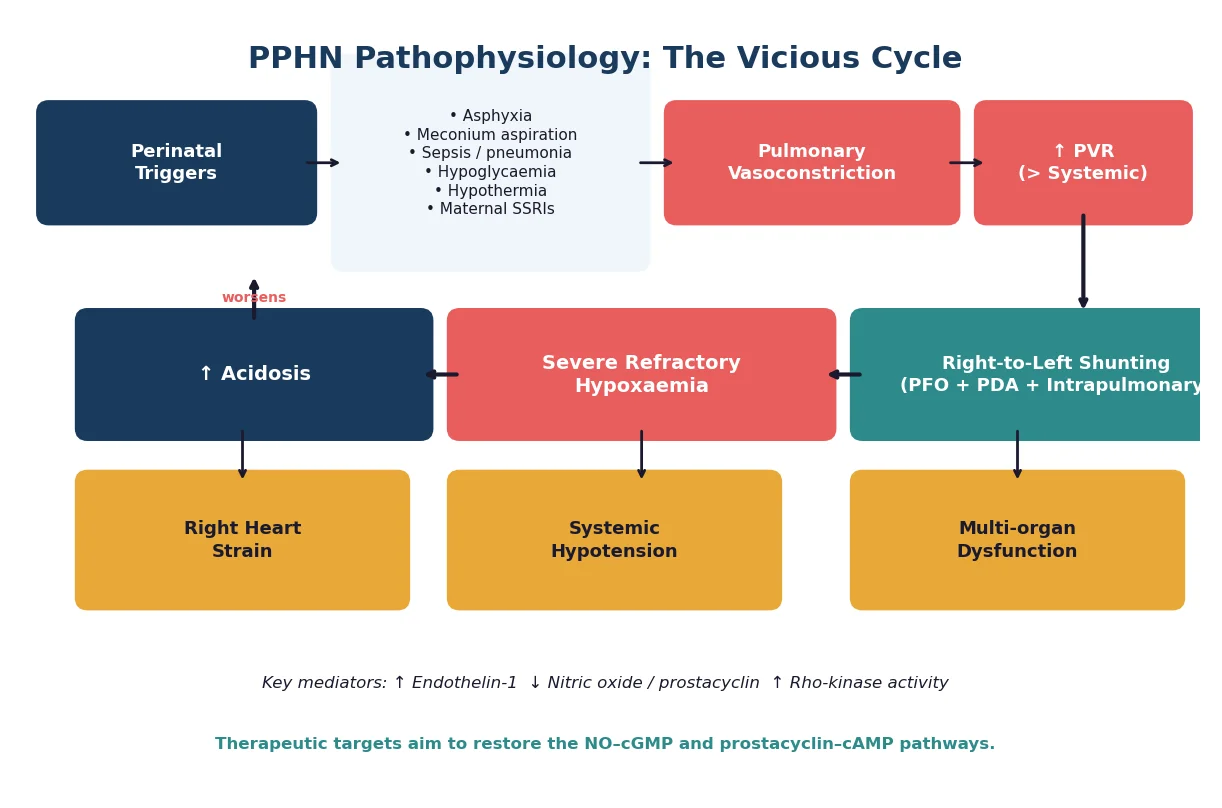
In utero, the pulmonary vascular resistance is high — the placenta, not the lungs, provides gas exchange. At birth, three events drop pulmonary blood flow tenfold: umbilical cord clamping, lung liquid clearance, and a surge in alveolar oxygen tension. Endothelial nitric oxide synthase and prostacyclin release mediate this dramatic vasodilation. [6]
PPHN occurs when this vasodilation fails. Vasoconstrictors (endothelin-1, Rho-kinase) dominate, while vasodilators (nitric oxide, prostacyclin) are deficient or their downstream pathways are blunted. Smooth muscle thickening in small pulmonary arteries further narrows the vascular lumen. [6]
The consequence is a vicious cycle. High PVR drives blood through fetal shunts, bypassing the lungs. The resulting hypoxaemia produces acidosis, which constricts the pulmonary vasculature even further. Systemic hypotension compounds the problem — if systemic vascular resistance falls below PVR, the right-to-left shunt worsens. [1]
Classification
PPHN is classified by the underlying vascular mechanism rather than by severity score alone. Three mechanisms are recognised, though they overlap frequently in clinical practice. [1]
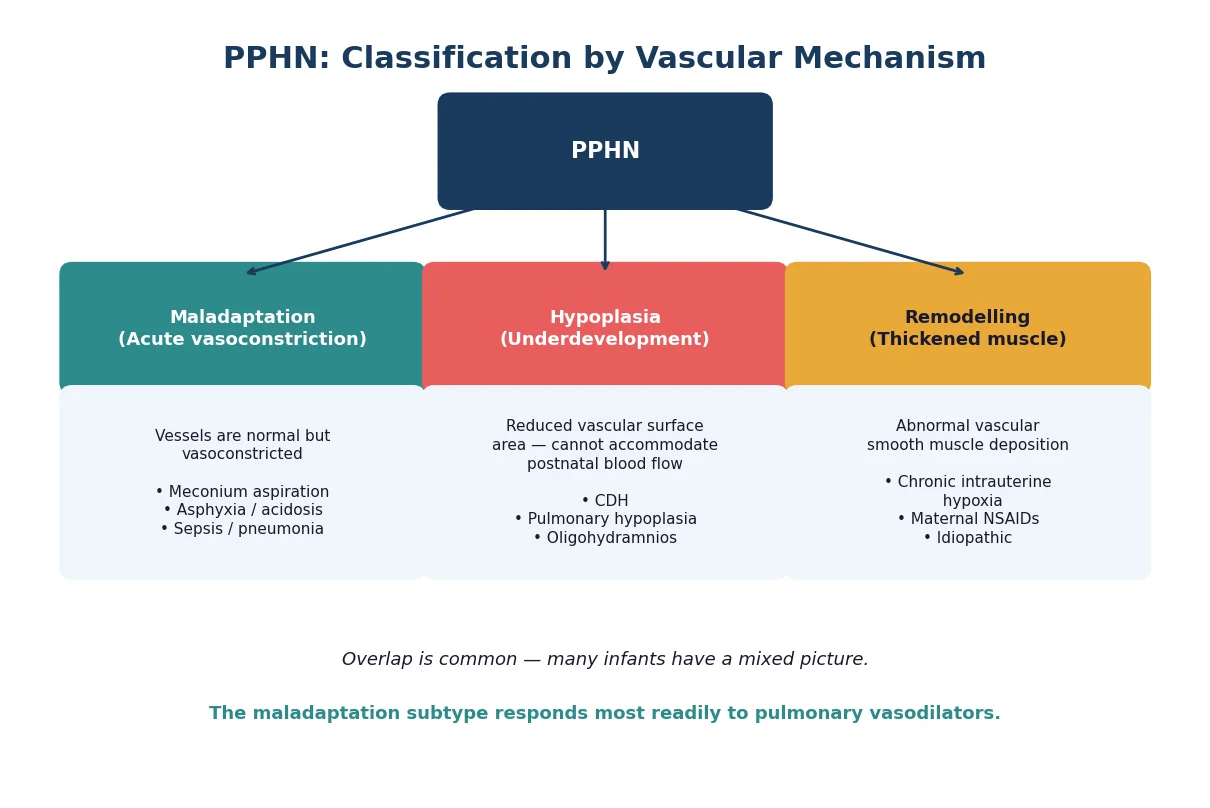
The maladaptation subtype — acute, reversible vasoconstriction in structurally normal vessels — responds most readily to pulmonary vasodilators. Hypoplasia (reduced vascular bed in CDH or oligohydramnios) is harder to reverse because the vascular surface area itself is insufficient. Remodelling (abnormal smooth muscle deposition from chronic intrauterine hypoxia) may partially respond but often requires prolonged therapy. [6]
Clinical Presentation
A term or late-preterm infant develops respiratory distress and cyanosis within the first 12–24 hours after birth. The oxygen requirement climbs rapidly and often fails to respond to supplemental oxygen in a pattern that distinguishes PPHN from simple lung disease. [1]
Auscultation reveals a loud, single second heart sound (prominent P₂) reflecting high pulmonary artery pressure. A tricuspid or mitral regurgitation murmur may be audible. Hepatomegaly suggests right heart strain. Infants with severe disease develop systemic hypotension, poor peripheral perfusion, and oliguria from the resulting multi-organ dysfunction. [7]
Differential Diagnosis
Cyanotic congenital heart disease is the most urgent differential — transposition of the great arteries, total anomalous pulmonary venous return, and truncus arteriosus can mimic PPHN and must be excluded by echocardiography before committing to iNO therapy. Starting iNO in a duct-dependent cardiac lesion can precipitate collapse by reducing PVR and stealing systemic output. [4]
Primary lung disorders are common co-pathologies. Respiratory distress syndrome, meconium aspiration, congenital pneumonia, and congenital diaphragmatic hernia can all coexist with PPHN and worsen the hypoxaemia. The chest X-ray helps distinguish a parenchymal process from idiopathic PPHN, where the lung fields appear normal or oligemic. [1]
Sepsis triggers inflammatory pulmonary vasoconstriction and is both a cause and a mimic. Polycythaemia and methaemoglobinaemia are rarer but important considerations when the cyanosis is disproportionate to the respiratory effort. [1]
Clinical & Bedside Assessment
Begin with simultaneous pre-ductal and post-ductal pulse oximetry. A right-hand probe sits pre-ductal (before the ductus takeoff); any lower-limb probe sits post-ductal. Re-measure after 100% FiO₂ for 10 minutes — a minimal rise in SpO₂ or PaO₂ points toward PPHN or cyanotic CHD rather than primary lung disease. [1]
Examine for signs of right heart strain. A tricuspid regurgitation murmur, hepatomegaly, and a gallop rhythm suggest pulmonary hypertension is causing backward failure. Assess blood pressure in all four limbs — differential pressures suggest coarctation or interrupted aortic arch, which changes the differential entirely. [7]
Complete the physical examination with an assessment of perfusion, capillary refill time, and the central-to-peripheral temperature gap to evaluate systemic cardiac output. A broad pulse pressure suggests a ductus arteriosus runoff, while a narrow pulse pressure signals impaired cardiac output. [7]
Investigations
An echocardiogram is the single most important investigation. It estimates pulmonary artery pressure from tricuspid regurgitation velocity and septal position, visualises shunting across the foramen ovale and ductus, assesses right and left ventricular function, and — critically — rules out structural congenital heart disease. No infant should receive iNO without a confirming echocardiogram. [4]
Blood gas analysis quantifies the degree of hypoxaemia and acidosis. Send simultaneous pre-ductal and post-ductal samples. Calculate the Oxygenation Index (OI = mean airway pressure × FiO₂ × 100 ÷ PaO₂) on every gas — it grades severity and guides escalation. An OI above 25 warrants discussion with an ECMO centre. [3]
The chest X-ray in idiopathic PPHN shows normal or decreased pulmonary vascular markings with a normal-sized heart. In secondary PPHN, it reveals the underlying cause — patchy infiltrates in meconium aspiration, a bowel loop in the chest in CDH, or diffuse haziness in pneumonia. [1]
A septic screen (blood culture, CRP, inflammatory markers) is mandatory because sepsis is both a cause and a complication. Check blood glucose, ionised calcium, and lactate — abnormalities in any of these worsen pulmonary vasoconstriction and must be corrected. [1]
Management — Resuscitation
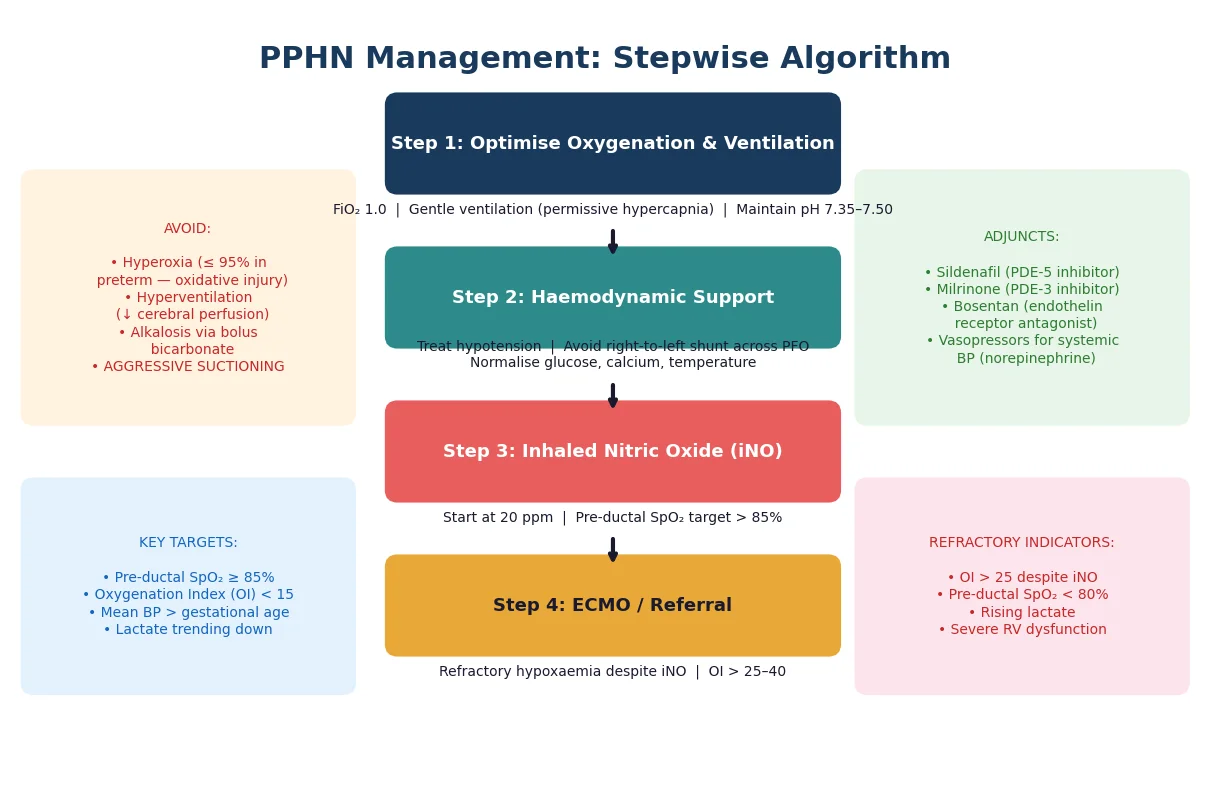
Stabilise the airway and establish adequate ventilation. Use FiO₂ titrated to the pre-ductal SpO₂ target (≥85%) and apply gentle ventilation with permissive hypercapnia, targeting pH 7.35–7.50. Aggressive hyperventilation to induce alkalosis is outdated — it causes cerebral vasoconstriction and barotrauma. [5]
Correct every metabolic derangement. Treat hypoglycaemia, hypocalcemia, and hypothermia aggressively. Acidosis is a potent pulmonary vasoconstrictor; maintaining a mildly alkalotic pH within the 7.35–7.50 range helps keep PVR low. [1]
Systemic hypotension is dangerous because it drops systemic vascular resistance below PVR and widens the right-to-left shunt. Give volume cautiously and use inotropes or vasopressors to maintain a mean blood pressure above the infant's gestational age in weeks. [7]
Resuscitation sequence
Assess airway, breathing, circulation in delivery room
Apply pre- and post-ductal SpO₂ probes immediately
Establish IV access and draw blood gas, glucose, calcium, cultures
Start gentle ventilation targeting pH 7.35–7.50
Correct hypoglycaemia, hypocalcaemia, hypothermia
Support systemic BP with inotropes or vasopressors
Management — Definitive & Stepwise
After initial stabilisation, therapy proceeds in a stepwise fashion. The goal at each stage is to lower PVR while maintaining systemic blood pressure, thereby reducing right-to-left shunting and improving oxygenation. [1]
Step one optimises lung inflation and FiO₂ with adequate PEEP, avoiding atelectasis and overdistension. Step two maintains haemodynamic stability with blood pressure, glucose, calcium, and temperature targets. Step three introduces inhaled nitric oxide at 20 ppm for moderate-to-severe disease. Step four adds adjunctive vasodilators — sildenafil or milrinone — for refractory cases. Step five refers for ECMO if the OI remains above 25–40 despite maximal therapy. [1]
Inhaled nitric oxide is the first-line selective pulmonary vasodilator. It relaxes vascular smooth muscle via the cyclic GMP pathway and, because it is delivered directly to ventilated alveoli, improves ventilation–perfusion matching without causing systemic hypotension. The Cochrane review confirms that iNO improves oxygenation and reduces ECMO use by approximately 40% in term and near-term infants. Start at 20 ppm and titrate down as the infant improves. [5]
When iNO alone is insufficient, adjunctive vasodilators enter the picture. Sildenafil inhibits phosphodiesterase-5, prolonging the nitric oxide effect; milrinone inhibits phosphodiesterase-3, providing both pulmonary vasodilation and inotropic support. A 2024 network meta-analysis found iNO most effective overall, but sildenafil and milrinone provide incremental benefit when iNO fails. [8]
Extracorporeal membrane oxygenation is the final rescue therapy for refractory PPHN. Veno-arterial ECMO is preferred when haemodynamic instability accompanies the hypoxaemia. Early referral to an ECMO-capable centre is essential — the decision should be made before the infant is in extremis. [3]
Specific Subtypes & Scenarios
Idiopathic PPHN presents as isolated pulmonary vascular dysfunction with a normal chest X-ray and no identifiable parenchymal trigger. These infants have pure maladaptation and typically respond well to iNO. [1]
PPHN with meconium aspiration syndrome involves a triad of airway obstruction, chemical pneumonitis, and inflammation-driven vasoconstriction. Surfactant may help by reducing alveolar injury and improving lung compliance. Oxygenation often improves more slowly than in idiopathic disease. [1]
PPHN with congenital diaphragmatic hernia represents the most challenging subtype. The ipsilateral lung is hypoplastic, the contralateral lung is underdeveloped, and the pulmonary vasculature is structurally abnormal. These infants frequently require early ECMO and prolonged ventilation. Avoiding barotrauma is paramount because the reduced lung surface area amplifies the effect of volutrauma. [1]
Alveolar capillary dysplasia with misalignment of pulmonary veins is a rare, fatal cause of refractory PPHN. It should be suspected when PPHN is unresponsive to all therapies including ECMO, and lung biopsy confirms the diagnosis. Genetic testing for FOXF1 mutations supports the diagnosis. [6]
Complications & Pitfalls
Chronic lung disease affects a subset of survivors, particularly those with meconium aspiration or CDH. The risk is highest with prolonged high-pressure ventilation and oxygen exposure. [1]
Neurodevelopmental impairment is the most feared long-term complication. Both severe hypoxaemia and the need for ECMO contribute to the risk of cognitive delay, cerebral palsy, and sensorineural hearing loss. Every PPHN survivor needs scheduled neurodevelopmental and audiology follow-up. [1]
PPHN pitfalls mnemonic
Intracranial haemorrhage is a recognised risk of ECMO, both from anticoagulation and from the haemodynamic fluctuations of cannulation. Methaemoglobinaemia can develop with high-dose or prolonged iNO; monitor methaemoglobin levels regularly. [3]
Prognosis & Disposition
Mortality ranges from 4% in mild, iNO-responsive cases to 33% in severe disease requiring ECMO. The underlying cause strongly influences outcome — idiopathic PPHN carries the best prognosis, while CDH-associated PPHN has the worst. [3]
Survivors require comprehensive outpatient follow-up. Neurodevelopmental assessment at 6, 12, and 24 months is standard. Audiology testing is mandatory before discharge and at 6 months, because PPHN survivors have a significantly elevated risk of progressive sensorineural hearing loss. [4]
Discharge criteria include stable oxygenation on room air or minimal home oxygen, established oral feeding, consistent weight gain, and parental competence in any required home therapies. Care coordination with the medical home ensures surveillance does not lapse. [4]
Special Populations
Late-preterm infants (34–36 weeks) face a double jeopardy: higher PPHN incidence than term infants, and greater vulnerability to hypoxaemic injury due to immature cerebral autoregulation. The threshold for iNO and escalation should be lower than in term infants. [1]
Outborn infants need prompt recognition and urgent retrieval. Every non-tertiary centre should know the nearest facility with iNO and ECMO capability. Stabilisation before transport — adequate ventilation, vascular access, corrected metabolic derangements — is as important as speed of transfer. [1]
Infants with CDH require delivery at a tertiary centre when diagnosed antenatally. Immediate postnatal management includes gentle ventilation, nasogastric decompression, and early surgical planning. The pulmonary hypoplasia dictates the clinical course more than the hernia itself. [1]
Evidence, Guidelines & Regional Differences
The American Heart Association and American Thoracic Society published joint guidelines for paediatric pulmonary hypertension in 2015, providing the current consensus framework for PPHN diagnosis and management. These guidelines establish iNO as first-line therapy for moderate-to-severe PPHN and define escalation pathways. [4]
The Cochrane review of nitric oxide for respiratory failure in near-term and term infants confirms that iNO improves oxygenation and reduces the combined outcome of death or need for ECMO. The benefit is clearest in infants with an OI above 15. [5]
Christou et al., 2000 — iNO and ECMO
Observational cohort
Population: Term infants with PPHN
Key finding
Inhaled nitric oxide reduced the need for ECMO by approximately 40%, establishing iNO as the first-line pulmonary vasodilator.
A 2024 network meta-analysis compared iNO, sildenafil, bosentan, and milrinone head-to-head across randomised trials. Inhaled nitric oxide ranked highest for improving oxygenation, while sildenafil and milrinone offered meaningful benefit as adjunctive or rescue therapy. The analysis supports iNO as first-line, with escalation to combination therapy for refractory cases. [8]
In the ANZ context, iNO is available in all tertiary NICUs and many level-2 special care nurseries via retrieval services. ECMO is centralised in a small number of paediatric cardiac centres; early referral is essential given transport distances. Antenatal corticosteroids and avoiding unnecessary elective Caesarean delivery before 39 weeks remain the primary prevention strategies. [4]
Exam Pearls
The pre–post ductal gradient is the single most testable bedside finding. If asked to perform one investigation on a cyanotic newborn, request an echocardiogram — it simultaneously confirms PPHN, quantifies severity, and excludes structural heart disease. [4]
When asked about management escalation, frame your answer as a stepwise pathway: optimise ventilation, correct metabolic derangements, support systemic blood pressure, start iNO, add adjunctive vasodilators, and refer for ECMO. Naming the oxygenation index thresholds demonstrates mastery. [3]
Remember that iNO is contraindicated in duct-dependent congenital heart disease — reducing PVR can steal systemic output through the ductus. Always confirm the cardiac anatomy first. [4]
References
- [1]Singh Y Pathophysiology and Management of Persistent Pulmonary Hypertension of the Newborn Clin Perinatol, 2021.PMID 34353582
- [2]Chambers CD Selective serotonin-reuptake inhibitors and risk of persistent pulmonary hypertension of the newborn N Engl J Med, 2006.PMID 16467545
- [3]Christou H Inhaled nitric oxide reduces the need for extracorporeal membrane oxygenation in infants with persistent pulmonary hypertension of the newborn Crit Care Med, 2000.PMID 11098980
- [4]Abman SH Pediatric Pulmonary Hypertension: Guidelines From the American Heart Association and American Thoracic Society Circulation, 2015.PMID 26534956
- [5]Finer NN Nitric oxide for respiratory failure in infants born at or near term Cochrane Database Syst Rev, 2006.PMID 17054129
- [6]Martinho S Persistent Pulmonary Hypertension of the Newborn: Pathophysiological Mechanisms and Novel Therapeutic Approaches Front Pediatr, 2020.PMID 32850518
- [7]Siefkes HM Management of systemic hypotension in term infants with persistent pulmonary hypertension of the newborn: an illustrated review Arch Dis Child Fetal Neonatal Ed, 2021.PMID 33478959
- [8]Fei Q Comparison of Different Treatments of Persistent Pulmonary Hypertension of the Newborn: A Systematic Review and Network Meta-Analysis Crit Care Med, 2024.PMID 38363176