Paeds · fetal-neonatal-and-perinatal
Poor feeding and feeding intolerance in the neonate
Also known as Neonatal feeding intolerance · Poor feeding in the newborn · Neonatal necrotising enterocolitis · Bilious vomiting in the neonate · Gastric residuals in the preterm infant
Fellowship guide to poor feeding and feeding intolerance in the neonate: why these are alarm signals not diagnoses, the surgical-versus-medical split, the Bell staging of necrotising enterocolitis, the bedside and radiographic assessment, and the stepwise management from feed cessation and resuscitation through safe re-advancement of enteral feeds.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a ten-day-old infant born at 27 weeks who has been tolerating small trophic feeds of expressed breast milk. The nurse tells you the residual before the last feed was larger than the feed itself, the abdomen looks fuller, and the infant has had three apnoeic spells. Before you reach for a prokinetic or dismiss this as "just a preterm being slow", hold two ideas separate: is this a normal, immature gut learning to coordinate, or is this the gut signalling trouble — and how will you tell? [3]
Poor feeding in the neonate means an infant who will not wake to feed, has a weak or disorganised suck, or whose intake is falling. Feeding intolerance means the gut is failing to move feeds forward — shown by gastric residuals, vomiting, abdominal distension, or blood in the stool. Neither is a diagnosis: each is a pattern that demands a cause. The neonate has almost no reserve and a narrow window between "looks well" and "collapses", so the discipline is to find the cause early, before the pattern becomes a crisis. [2]
The reason these signals matter so much is the gut's unique role at birth. In fetal life the placenta delivers nutrition parenterally; at birth the gut must abruptly take over, digesting and absorbing milk while its motility, mucosal barrier, microbiome and digestive enzymes mature. The preterm gut does all of this with an immature barrier and an abnormal colonising flora, which is exactly why prematurity is the dominant risk factor for necrotising enterocolitis (NEC) — the inflammatory, potentially necrotising bowel injury that is the can't-miss cause of feeding intolerance. [3]
So the examiner's first question is always: is this a gut that will settle with time and support, or one that is heading for NEC, obstruction or collapse? That single distinction drives the neonatal plan. [1]
Classification
Begin with the danger, then localise. The first split is surgical from medical, because a surgical obstruction (often with bilious vomiting) is an emergency that demands contrast imaging and a surgeon, while a medical cause needs resuscitation and investigation. [2]
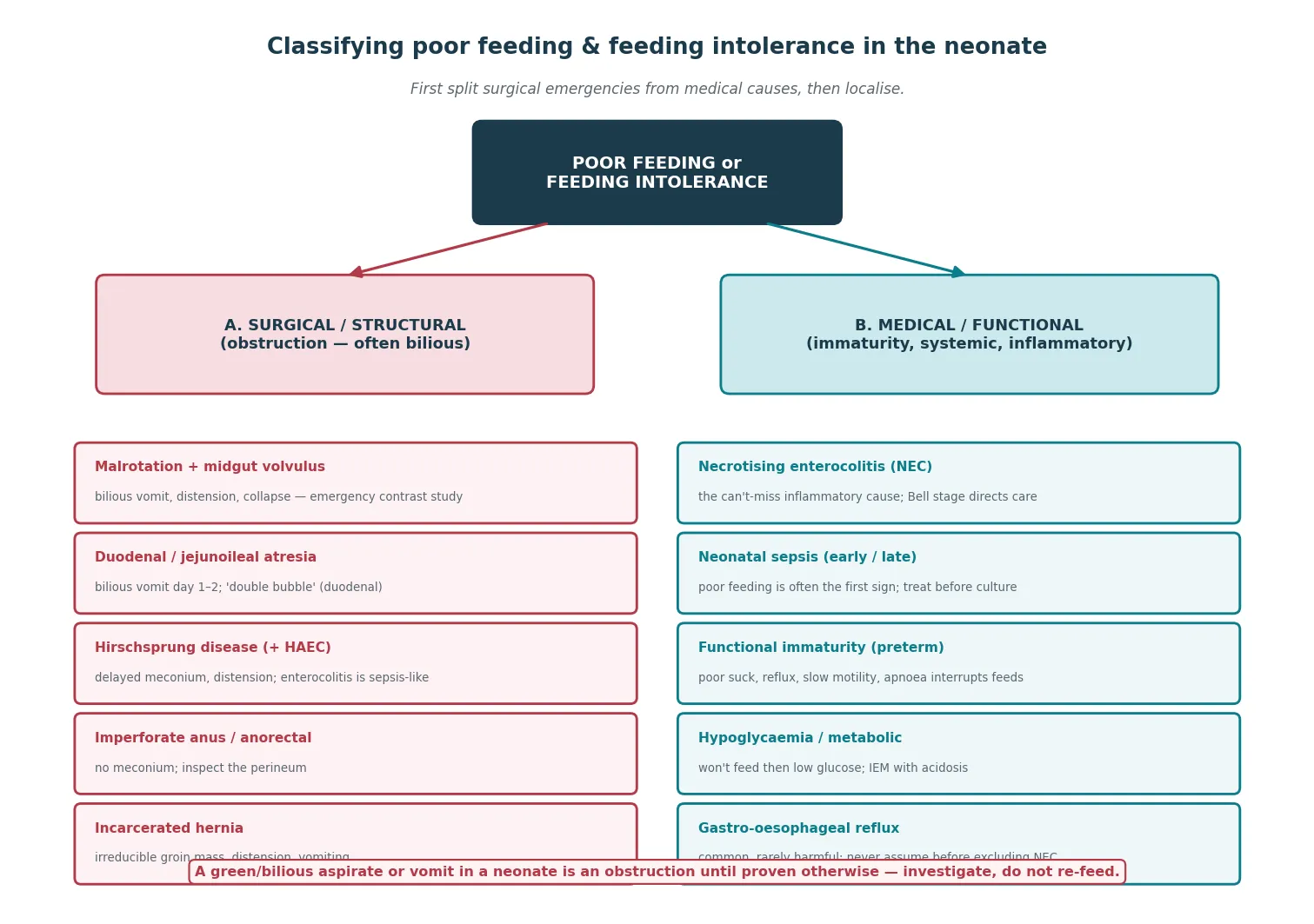
On the surgical and structural side, the obstruction may be high or low. A high obstruction presents with early, often bilious vomiting: malrotation with midgut volvulus (the emergency), duodenal atresia (classically with the double-bubble and, often, trisomy 21), and jejunoileal atresia. A low obstruction presents with distension and failure to pass meconium: Hirschsprung disease (which may present as Hirschsprung-associated enterocolitis, a sepsis-like emergency), anorectal malformation (diagnose by inspecting the perineum), meconium plug, and, rarely in the neonate, an incarcerated inguinal hernia. [3]
On the medical and functional side, NEC is the inflammatory cause and the one you cannot miss. Neonatal sepsis (early or late) presents with poor feeding as often the first sign, and must be treated before the culture returns. [4] Functional immaturity of the preterm gut produces the common, benign pattern of small residuals, reflux, slow motility and apnoea interrupting feeds in an otherwise well infant. Hypoglycaemia and the metabolic disorders cause poor feeding directly, sometimes with acidosis or hyperammonaemia. Gastro-oesophageal reflux is common and usually physiological, but it is also a trap: labelling a neonate as "reflux" before excluding NEC or obstruction costs lives. [3]
NEC itself is classified by the modified Bell staging criteria — the framework that turns the clinical and radiographic picture into a stage that directs management (see Pathophysiology and Management for the full table). [1]
Epidemiology & Risk Factors
Poor feeding and feeding intolerance are among the commonest concerns in any neonatal unit, but the danger concentrates in the preterm infant. NEC, the worst outcome, affects roughly 5 to 10 percent of very-low-birth-weight infants and carries a mortality of 20 to 30 percent — which is why a feeding concern in a preterm infant is never routine. [3]
The dominant risk factor for NEC is prematurity. The more immature the gut, the thinner the mucosal barrier, the weaker the tight junctions, the less mature the immune and motility functions, and the more abnormal the colonising microbiome. NEC is rare in term infants and rare once the gut matures, so a term infant with NEC should prompt a search for another gut insult — hypoxia, sepsis, hypotension, congenital heart disease, or polycythaemia. [3]
The route and type of feeding powerfully modulate NEC risk. Formula feeding substantially increases NEC risk compared with human milk, because mother's own milk delivers immunoglobulins, lactoferrin, growth factors and human milk oligosaccharides that shape a protective microbiome and mature the barrier. Donor breast milk retains much of this protection. [7] Standardised feeding protocols — written, unit-wide rules for advancement — are themselves protective, because they reduce the variability that precedes NEC. [5]
Other risk factors stack on prematurity: gut ischaemia or hypoxia (the gut is the shock organ), episodes of hypotension or low perfusion, sepsis, anaemia and rapid transfusion, indomethacin or ibuprofen treatment for a patent ductus, and indwelling central lines. For the term and late-preterm infant with poor feeding, the risk profile shifts toward sepsis, hypoglycaemia, hypothermia, perinatal asphyxia, structural obstruction, and the metabolic and endocrine disorders. [4]
Pathophysiology
To understand why feeding intolerance can tip into NEC so quickly, follow the gut barrier. The story is an immature intestine meeting an abnormal world, and it explains why a well preterm can deteriorate over hours. [3]
The modern model is a three-hit pathogenesis. First, the premature gut has a thin mucosal barrier, weak tight junctions, immature digestive capacity, and an underdeveloped immune response. Second, dysbiosis — colonisation by an abnormal microbiome, with fewer protective anaerobes — takes hold, especially when formula (which lacks human milk oligosaccharides) is the substrate. Third, an ischaemic or inflammatory insult — hypoxia, low flow, sepsis, or the substrate itself — triggers an exaggerated Toll-like receptor 4 (TLR4) inflammatory response that the immature gut cannot contain. [3]
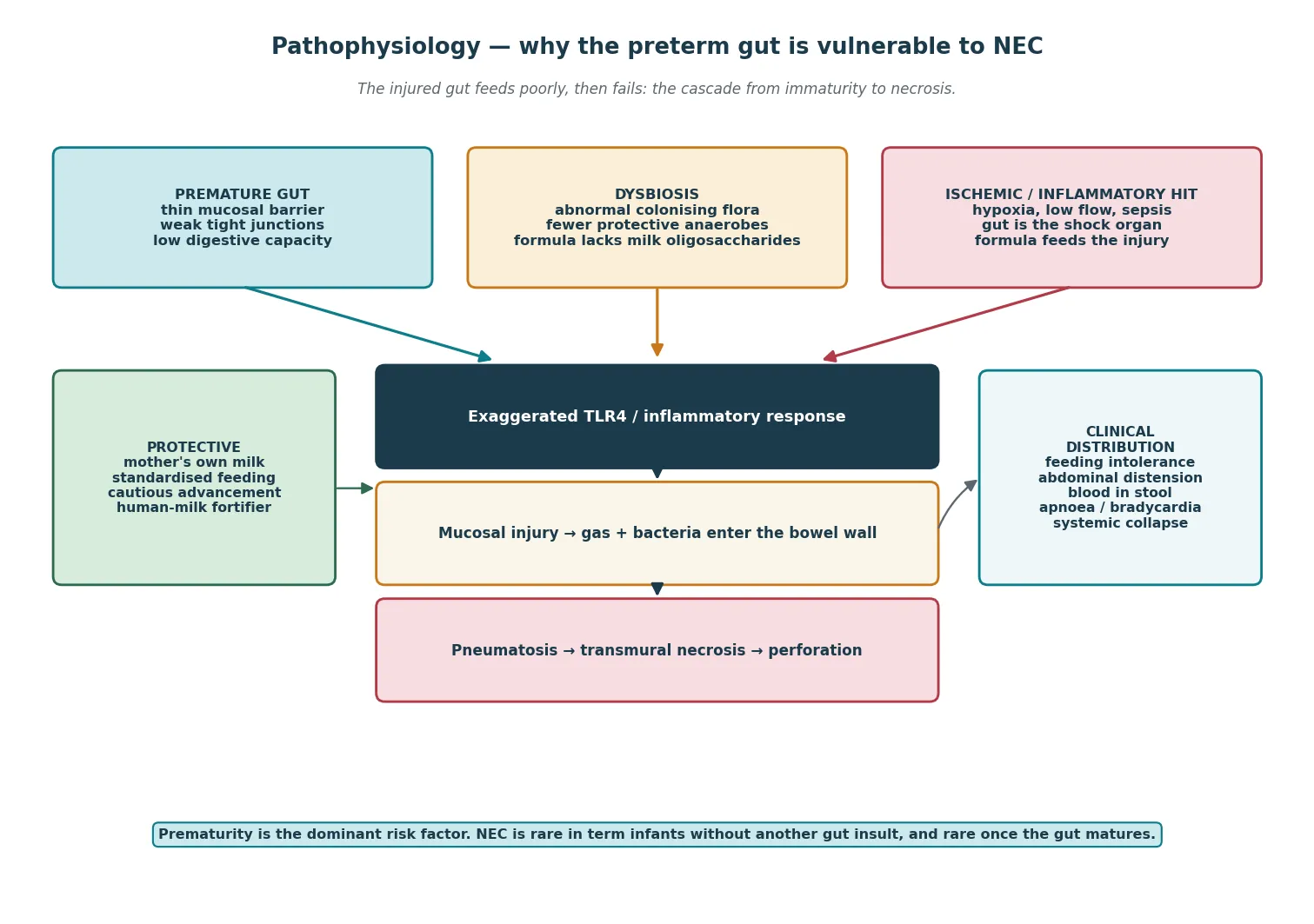
Once inflammation takes hold, the cascade runs fast. The injured mucosa breaks down, gas-forming bacteria and luminal gas enter the bowel wall to produce pneumatosis intestinalis (the radiographic hallmark), and if the injury progresses the wall becomes necrotic, may perforate, and releases bacteria and toxin into the peritoneum and the bloodstream — producing the systemic collapse, acidosis, thrombocytopenia and disseminated intravascular coagulation of advanced NEC. Portal venous gas signals severe disease because gas has entered the portal venous system through the injured mucosa. [3]
Standing against this is the protective effect of human milk. Mother's own milk delivers secretory immunoglobulin A, lactoferrin, growth factors (epidermal growth factor, insulin-like growth factor), and human milk oligosaccharides that feed a protective microbiome and accelerate barrier maturation. This is the biological basis for the evidence that human milk — mother's own first, then donor — reduces NEC. [7]
Why functional immaturity causes harmless intolerance in the well preterm is the same physiology in a milder key. Lower oesophageal sphincter tone is low, gastric emptying is slow, intestinal motility is discoordinated, and apnoea of prematurity interrupts the feed cycle. The result is the common pattern of small residuals, mild reflux, and slow advancement — all benign in an infant who is systemically well, feeding forward, and growing. [5]
Clinical Presentation
The neonate with feeding intolerance shows the gut failing, and the first signs are often systemic rather than abdominal — which is why a feeding concern is never ignored. The problem is that the early signs are non-specific, so the discipline is to look deliberately for the dangerous ones. [2]
The systemic signs are the gut's distress and often precede the abdominal signs: temperature instability (hypo- or hyperthermia), apnoea and bradycardia, lethargy or irritability, glucose instability, and poor perfusion. These are the signs of early NEC or sepsis, and they are the reason poor feeding is treated as a potential emergency, not a nuisance. [4]
The gastrointestinal signs are the localising features. Look for gastric residuals that are increasing, large, or changing in character; abdominal distension; vomiting — and crucially, whether it is bilious (green) or non-bilious; blood in the stool (frank blood, or a positive occult test); and abdominal wall changes — erythema, induration, oedema, or a shiny, discoloured abdominal wall that signals transmural disease. A palpable abdominal mass or a loop of bowel that feels fixed and tender is a surgical sign. [1]
The bilious versus non-bilious split is the single most useful bedside discriminator and is worth committing to. Bilious (green) vomit or aspirate means the obstruction is below the ampulla of Vater and is a surgical emergency until proven otherwise — think malrotation with volvulus, duodenal or jejunoileal atresia, Hirschsprung disease, or annular pancreas. Non-bilious vomit points above the ampulla (pyloric stenosis, though classically a later presentation) or to a systemic or functional cause. [3]
A neonate with malrotation and midgut volvulus is the can't-miss emergency hiding inside bilious vomiting: a previously well infant with bilious vomit, rapid progression to distension, collapse and shock, and a radiograph that may look deceptively normal early. This is a surgical emergency where minutes of bowel matter — do not wait for the perfect study. [3]
Differential Diagnosis
The differential turns on one question: is the gut obstructed, inflamed, systemically upset, or just immature? The answer comes from the clinical pattern, the abdominal examination, and the radiograph — but the list of causes must be held in mind so none is missed. [2]
When the picture is an obstruction with bilious vomiting, exclude malrotation with midgut volvulus first (the emergency), then duodenal atresia, jejunoileal atresia, Hirschsprung disease (with or without enterocolitis), anorectal malformation, meconium plug or meconium ileus (think cystic fibrosis), and an incarcerated inguinal hernia. A careful perineal inspection and a rectal examination or tube pass may immediately reveal the answer. [3]
When the picture is inflammatory or systemic without obstruction, the headline is NEC. Distinguish NEC from spontaneous intestinal perforation (SIP), which presents as an isolated free air without pneumatosis in the first days of life, classically after indomethacin or steroid exposure and in the extremely preterm — SIP is a different disease with a different surgical approach. Neonatal sepsis with ileus mimics NEC and often coexists; treat both. [4]
Do not forget the metabolic and endocrine causes of poor feeding. Inborn errors of metabolism present with poor feeding, vomiting, and lethargy, often with metabolic acidosis, hyperammonaemia, or hypoglycaemia. Congenital adrenal hyperplasia causes poor feeding, vomiting, and salt-wasting with hyperkalaemia. Hypoglycaemia itself causes poor feeding and neuroglycopenic signs, and a poorly feeding neonate rapidly becomes a hypoglycaemic one. [3]
The dangerous trap is labelling the infant as "reflux". Gastro-oesophageal reflux is common and usually physiological in the neonate, and over-diagnosis hides NEC, obstruction, sepsis and metabolic disease. Reserve the diagnosis for an infant in whom the dangerous causes have been excluded and the pattern fits — and never reach for acid suppression or feed thickener as a first move. [3]
Clinical & Bedside Assessment
Begin with a focused history that frames the feeding risk. Establish the gestation and birthweight, the route and type of feeding (mother's own milk, donor milk, formula, nasogastric vs oral), the age at onset, the pattern of meconium passage, and the maternal and perinatal factors (prolonged rupture of membranes, chorioamnionitis, asphyxia, maternal infections). A 27-week preterm on advancing formula feeds is a very different patient from a term, well, breastfed infant on day two. [5]
Examine the abdomen systematically and deliberately. Inspect for distension, symmetry, abdominal wall colour (erythema, induration, shininess, discolouration), and the hernial orifices. Palpate gently for tenderness, guarding, palpable loops (are they fixed or changing?), masses, and a fullness in the right iliac fossa; check the hernial orifices and inspect the perineum for an anus. Auscultate — though bowel sounds are a poor discriminator, their absence with distension suggests ileus or peritonitis. [1]
The gastric residual deserves a disciplined read. Aspirate and measure it before each feed in the preterm on a protocol, and judge its volume, colour, and character. A residual that is large relative to the feed, increasing over successive checks, bilious, or changing from milk to bilious or blood-stained is a red flag. Volume alone is a poor predictor — the trend and the character matter more than the number, which is why the routine practice of aspiration is increasingly questioned. [10]
Check the systemic observations for the involvement that turns a feeding problem into an emergency: temperature, heart rate, respiratory rate, oxygen saturation, capillary refill and perfusion, and the frequency of apnoea and bradycardia. Hypothermia, tachycardia, poor perfusion, or a rising apnoea burden in a feeding-intolerant neonate is NEC or sepsis until proven otherwise. [4]
Synthesise a one-line summary. A good example: "A ten-day-old 27-week preterm on advancing expressed breast milk feeds, with increasing gastric residuals, a fuller abdomen, and new apnoea — suspected early necrotising enterocolitis; make nil by mouth, aspirate, resuscitate, image." That sentence carries the category, the severity, and the first move. [1]
The abdominal exam in suspected NEC or obstruction
Investigations
Investigation has two jobs: to confirm or exclude NEC, and to find or exclude a surgical obstruction. The backbone is the plain abdominal radiograph, read alongside the bedside panel and, when needed, a contrast study. [2]
The abdominal radiograph is the single most important investigation in suspected NEC. Look for pneumatosis intestinalis (gas in the bowel wall — the hallmark), portal venous gas (severe disease), a persistently dilated loop that does not change between films (a sign of impending necrosis or perforation), ascites, and free intra-abdominal gas (perforation). A left-lateral-decubitus or cross-table-lateral view detects small amounts of free air that an anteroposterior film misses. Pneumatosis alone, with compatible systemic signs, defines definite NEC. [3]
The laboratory panel supports the diagnosis and grades the severity. Send a full blood examination (watch the platelet count — thrombocytopenia is a marker of severe disease — and the haematocrit for a fall suggesting intra-abdominal bleeding), a C-reactive protein (a rising trend supports inflammation), a blood gas (metabolic acidosis signals advanced disease), glucose and electrolytes, and blood cultures. Send a stool culture and check for blood. Cross-match, coagulation and a platelet count prepare the infant who may need surgery. [1]
When the picture is bilious vomiting without NEC, request an upper gastrointestinal contrast study to confirm or exclude malrotation: the duodenojejunal flexure lies abnormally to the right of the spine, and a volvulus produces a "corkscrew" or "beak" appearance. This is an emergency study — do not delay resuscitation or surgical referral for it. A contrast enema may identify a microcolon (distal atresia) or Hirschsprung disease (a transition zone), but it is not the first study in an unwell neonate. [3]
Know what to avoid. Do not continue feeds while investigating suspected NEC or obstruction. Do not delay antibiotics while awaiting culture. Do not settle on a diagnosis of reflux without excluding the dangerous causes. And do not treat a single number — a gastric residual, a CRP, a radiograph — without the clinical context; NEC is a clinical, radiographic and laboratory synthesis. [2]
Management — Resuscitation
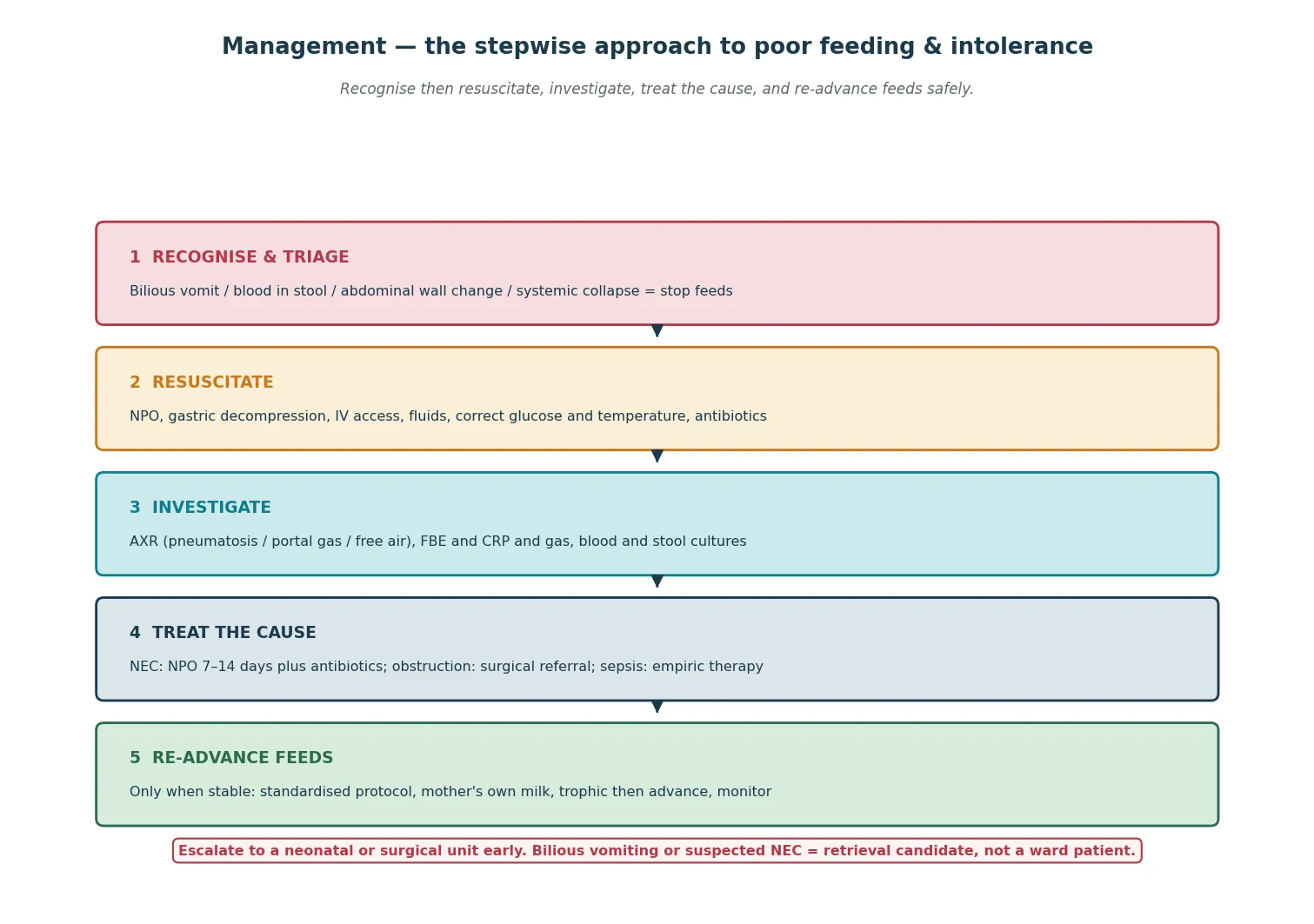
The immediate move when feeding intolerance, suspected NEC, or bilious vomiting is recognised is to stop feeds and decompress the gut — then resuscitate the infant and investigate. The danger is continuing feeds through a dangerous sign. [2]
The resuscitation bundle is: make the infant nil by mouth (NPO), pass a large-bore orogastric or nasogastric tube on free drainage to decompress the stomach and bowel, establish intravenous access, give fluid resuscitation for shock (10 mL/kg boluses of isotonic crystalloid, titrated to perfusion), correct glucose and temperature, and start broad-spectrum empiric antibiotics covering the common Gram-positive and Gram-negative enteric organisms. [1]
Escalate to a higher level of care when any of these is present: bilious vomiting (until obstruction excluded), systemic collapse (shock, persistent acidosis, apnoea requiring ventilation), suspected NEC on radiograph (pneumatosis, portal gas), perforation (free air), abdominal wall change with systemic signs, or a neonate with a dangerous underlying cause (metabolic acidosis, hyperammonaemia). Involve the neonatal team early and, in the rural setting, activate retrieval before deterioration. [3]
For the bilious-vomiting neonate, the resuscitation includes an emergency surgical referral alongside the contrast study — malrotation with volvulus is a minutes-matter emergency, and the cost of waiting is the loss of the midgut. Resuscitate, give antibiotics and fluid, confirm with contrast if the infant is stable enough, and do not delay the surgical referral for the study. [3]
The resuscitation errors to avoid are predictable: continuing feeds through bilious vomiting; attributing an increasing or bilious residual to immaturity; delaying antibiotics while awaiting culture; under-treating shock; and treating the radiograph or the number rather than the infant. Stop feeds, decompress, resuscitate, and treat the cause. [2]
Management — Definitive & Stepwise
Once stable, definitive care is a sequence: treat the cause, sustain the infant while the gut rests, and re-advance feeds safely when the gut has recovered. [1]
For suspected NEC (Bell stage I), make the infant NPO, decompress, resuscitate, start broad-spectrum antibiotics, and investigate; the NPO duration is typically 3 to 7 days if the picture settles and NEC is excluded, escalating if confirmed. For definite NEC (Bell stage II) — pneumatosis on radiograph — the NPO period is 7 to 10 days with continued antibiotics and monitoring for surgical deterioration. For advanced NEC (Bell stage III) with perforation, portal gas, or persistent acidosis, the NPO period extends to 14 days or more, and surgical intervention is indicated. [1]
The antibiotic regimen covers the common enteric organisms: a broad-spectrum combination such as a penicillin (ampicillin or piperacillin-tazobactam) with an aminoglycoside (gentamicin) and, in severe disease or perforation, metronidazole for anaerobic cover and possibly a third-generation cephalosporin or carbapenem — guided by local unit policy and resistance patterns. The exact regimen and duration are unit-specific; verify against the local protocol. [2]
Surgical intervention is indicated for perforation (free air), a fixed and dilated loop that does not change over serial films, clinical deterioration despite maximal medical therapy, or a positive paracentesis. In the very-low-birth-weight infant with isolated perforation, a primary peritoneal drain is often first-line; in proven NEC with necrosis, a laparotomy with resection of necrotic bowel and stoma formation is the operation. The decision is made jointly by the neonatal and surgical teams. [1]
[1]When the gut has recovered, re-advance feeds safely. Use a standardised feeding protocol: start with minimal enteral (trophic) feeds of mother's own milk, advance slowly (commonly 15 to 30 mL/kg/day in the stable very-low-birth-weight infant), use a single feed type, and check tolerance before each advancement. Mother's own milk is first-line; donor milk is second-line. Re-introduce feeds cautiously after NEC, watching for recurrence. [5]
Plan discharge once the infant is on full enteral feeds of appropriate volume and energy, gaining weight, feeding competently by mouth or a sustainable tube plan, thermally stable, and with confident parents who know the signs to return for. Plan follow-up for growth, neurodevelopment (especially after NEC), and surgical review where a stoma or resection is in place. [3]
The first hour of dangerous intolerance
Recognise a red flag (bilious vomit, blood in stool, wall change, collapse, rising/bilious residual)
Stop feeds — do not re-feed
Make NPO, pass a gastric tube on free drainage, establish IV access
Decompress the gut
Resuscitate: fluids for shock, correct glucose and temperature, start broad-spectrum antibiotics
Treat the systemic insult
Send the abdominal radiograph (include a lateral decubitus) and the laboratory panel
Confirm or exclude NEC and perforation
Escalate: involve neonatal and surgical teams; activate retrieval early in the rural setting
Bilious vomiting or suspected NEC is a retrieval candidate
Specific Subtypes & Scenarios
Suspected NEC (Bell stage I). The preterm infant with new feeding intolerance, a fuller abdomen, and systemic signs but no pneumatosis yet. Manage with NPO, decompression, resuscitation, antibiotics, and close observation; the picture often clarifies over 48 to 72 hours, settling or progressing to definite NEC. [1]
Definite NEC (Bell stage II). The radiograph shows pneumatosis intestinalis, with or without portal venous gas. Manage with NPO for 7 to 10 days, continued antibiotics, and serial monitoring for surgical signs (fixed loop, perforation, deterioration). Most infants recover with medical management; a minority progress. [1]
Advanced NEC and perforation (Bell stage III). Shock, persistent metabolic acidosis, thrombocytopenia, portal gas, or free air signal advanced disease. Intensive medical management plus urgent surgical intervention — peritoneal drain for isolated perforation in the very small, laparotomy with resection and stoma for necrotic bowel. These infants carry high mortality and long-term morbidity. [1]
Neonate with bilious vomiting. The surgical-obstruction pathway. Resuscitate, give antibiotics and fluid, refer urgently to surgery, and confirm with an upper GI contrast study (for malrotation) or the appropriate study for the suspected level of obstruction. Malrotation with volvulus is the can't-miss emergency — the cost of delay is the loss of the midgut. [3]
Spontaneous intestinal perforation. An isolated free air without pneumatosis in an extremely preterm infant in the first days of life, classically after indomethacin or steroid exposure. It is a different disease from NEC — less systemic inflammation, often managed with a peritoneal drain, and a shorter antibiotic course. [3]
Stable growing preterm (no NEC). Feed on a standardised protocol: trophic feeds of mother's own milk, gradual advancement, fortification when tolerance and growth demand it, and a disciplined approach to the gastric residual (trend and character over volume). Weight-gain targets guide adequacy. [5]
Late-preterm and term infant with poor feeding. The danger profile shifts: exclude sepsis, hypoglycaemia, structural obstruction, and metabolic disease. Support feeding (supplementary expressed milk, lactation support), monitor glucose, and keep the infant warm; a low threshold for transitional care or NICU when feeding is not establishing. [4]
Complications & Pitfalls
Short-term, expect perforation and peritonitis, shock, metabolic acidosis, thrombocytopenia and disseminated intravascular coagulation, and the acute surgical event. Long-term, NEC survivors carry a heavy burden: short-bowel syndrome and intestinal failure after extensive resection (dependence on parenteral nutrition, central-line sepsis, cholestasis), intestinal strictures weeks to months after the acute episode, and neurodevelopmental impairment that is more frequent and more severe after surgical NEC than after medical NEC. [3]
The pitfalls are predictable, and worth naming so you avoid them. Labelling the infant as "reflux" before excluding NEC, obstruction, sepsis and metabolic disease — the classic and dangerous shortcut. Continuing feeds through bilious vomiting or a rising residual — a feed should never go in when the gut is signalling danger. Over-reliance on the gastric-residual volume alone — the trend and the character matter more than the number. [10] Delaying antibiotics or surgical referral while awaiting confirmation. And treating the radiograph rather than the infant — a well infant with a borderline radiograph is different from a collapsing one. [1]
A second tier of traps deserves attention. Missing Hirschsprung-associated enterocolitis — a neonate with delayed meconium, distension, and sepsis-like collapse has enterocolitis until proven otherwise. Missing spontaneous intestinal perforation as a distinct entity from NEC, which changes the surgical and antibiotic plan. And the complications of prolonged NPO and parenteral nutrition — line sepsis, cholestasis, and mucosal atrophy — which is why the gut is rested for as long as it needs but no longer. [3]
Prognosis & Disposition
Outcome is driven by the gestational age, the Bell stage at recognition, the presence of perforation, the rapidity of deterioration, and the need for surgery — not by any single sign or number. Medical NEC (Bell stage I to II without surgery) generally has a good outcome; surgical NEC, especially with extensive resection, carries high mortality (20 to 30 percent overall, higher with perforation) and a heavy long-term morbidity. [3]
The long-term outlook after NEC is dominated by two problems. Short-bowel syndrome follows extensive resection: the infant is dependent on parenteral nutrition, faces repeated central-line infections and cholestasis, and needs a specialist intestinal-failure service for the slow, sometimes years-long process of intestinal adaptation. Neurodevelopmental impairment — cognitive, motor, and behavioural — is significantly more common after surgical NEC, which is why survivors need structured neurodevelopmental follow-up. [3]
Disposition follows the risk. A stable growing preterm on a feeding protocol stays in the nursery or special care with protocol-driven advancement. Suspected NEC goes to NICU for observation and medical management. Definite or advanced NEC, bilious vomiting, perforation, or systemic collapse goes to NICU with the neonatal and surgical teams involved and, in the rural setting, retrieval activated early. [1]
Plan discharge once the infant is on full enteral feeds, gaining weight, feeding competently, thermally stable, and with confident, safety-netted parents. Plan follow-up for growth, neurodevelopment (especially after NEC), surgical review where a stoma or resection is in place, and the intestinal-failure pathway for short-bowel survivors. [3]
Special Populations
Extremely preterm and very-low-birth-weight infants are the highest-risk group for NEC. Their feeding strategy is built around the protective evidence: mother's own milk first, donor milk second, trophic feeds, cautious standardised advancement, human-milk-based fortification, and the selective use of probiotics where unit policy supports it. Every decision balances the drive to grow against the risk of NEC. [6]
Late-preterm infants compound prematurity, feeding immaturity, hypoglycaemia, jaundice, and temperature instability. Provide dedicated feeding support (supplementary expressed milk, lactation support), monitor glucose and temperature, and keep a low threshold for transitional care or NICU when feeding is not establishing. [4]
Indigenous and socioeconomically disadvantaged families carry a higher burden of prematurity and its complications, and may face real barriers to breastfeeding support, donor-milk access, and follow-up. Provide culturally safe, continuous care; address nutrition and lactation support directly; and ensure the surveillance and follow-up loop does not drop. [5]
Rural and remote settings must plan early feeding support, recognise bilious vomiting and the NEC red flags, and activate retrieval before deterioration. A neonate with suspected NEC or bilious vomiting born away from neonatal and surgical support is an avoidable crisis — escalate and retrieve early, and support the family with telehealth in the interim. [3]
Infants after gastrointestinal surgery or with complex congenital disease run on specialist feeding protocols — stoma management, re-feeding, fortification, and multidisciplinary follow-up by neonatology, surgery, dietetics, and the intestinal-failure service. [1]
Families of infants with prolonged or complicated feeding courses need clear parent education, lactation and feeding support, and explicit safety-netting on the signs to return for — poor feeding, vomiting, abdominal distension, blood in stool, and any change in colour or activity. [3]
Evidence, Guidelines & Regional Differences
The evidence base for NEC prevention is strong on human milk. The Cochrane review by Quigley and Embleton (2019) found that feeding preterm or low-birth-weight infants formula rather than donor breast milk increases the risk of NEC — which is the foundation of the "mother's own milk first, donor milk second" hierarchy. [7]
The evidence on feed advancement is reassuring. The Cochrane review by Oddie and Young (2021) found that slow advancement of enteral feed volumes does not reduce NEC compared with faster advancement — suggesting that cautious protocols protect through standardisation and human milk rather than through a magic rate, and that delaying nutrition to avoid NEC is not supported. [8]
The evidence on probiotics is more contested. The Cochrane review by Sharif and Meader (2023) found that probiotics probably reduce NEC and mortality in very preterm or very-low-birth-weight infants, but implementation is debated because of safety concerns (probiotic bacteraemia in the extremely preterm), variable product quality, and divergent regulatory and unit policy across regions. [6]
The evidence on gastric residuals has shifted the bedside culture. Mihatsch and von Schoenaich (2002) showed that gastric residual volume correlates poorly with feeding tolerance in extremely-low-birth-weight infants, and the survey by Perumbil Pathrose and Spence (2021) documented wide practice variation, arguing for an evidence-based guideline. The trend is away from routine aspiration of large volumes toward trend- and character-based judgement. [10] [9]
The staging system is the foundation of NEC management: the original Bell criteria (Bell and Ternberg 1978) established clinical staging, and the modified Bell criteria (Walsh and Kliegman 1986) added radiographic and clinical detail to direct treatment. [2] [1] The early nutrition framework comes from Ehrenkranz (2007), which set out the evidence for aggressive nutritional management of the very-low-birth-weight infant, balancing growth and NEC risk. [5]
Two live controversies: the role of probiotics — the evidence favours a reduction in NEC, but safety in the extremely preterm, product quality, and regional regulation keep policy divergent; and the significance of the gastric residual — whether to aspirate routinely at all, and how much weight to give the volume, remains in active evolution. [6] [9]
Exam Pearls
- Bilious (green) vomit or aspirate in a neonate is a surgical obstruction until proven otherwise — investigate, do not re-feed. [3]
- Pneumatosis intestinalis is the radiographic hallmark of NEC; portal venous gas and free air signal severe or advanced disease. [1]
- The modified Bell staging (Walsh and Kliegman 1986): suspected (I), definite (II, pneumatosis), advanced (III, shock or perforation). NPO duration and surgery follow the stage. [1]
- Prematurity is the dominant risk factor for NEC; mother's own milk is the dominant protective factor. [3]
- A gastric residual that is bilious, increasing, or changing in character is a red flag — volume alone is a poor predictor. [10]
- Poor feeding is often the first sign of neonatal sepsis — treat before the culture returns. [4]
- Abdominal wall erythema, induration or discolouration with systemic signs is advanced NEC — escalate now. [1]
- Distinguish NEC (pneumatosis, systemic inflammation, NPO 7 to 14 days) from spontaneous intestinal perforation (isolated free air, no pneumatosis, early postnatal, indomethacin or steroid exposure). [3]
- Slow feed advancement does not by itself reduce NEC (Oddie Cochrane 2021) — protection comes from standardisation and human milk, not from starving the infant. [8]
- Mother's own milk first, donor milk second, formula last — formula increases NEC (Quigley Cochrane 2019). [7]
References
- [1]Walsh MC, Kliegman RM Necrotizing enterocolitis: treatment based on staging criteria. Pediatric Clinics of North America, 1986.PMID 3081865
- [2]Bell MJ, Ternberg JL Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Annals of Surgery, 1978.PMID 413500
- [3]Neu J, Walker WA Necrotizing enterocolitis. New England Journal of Medicine, 2011.PMID 21247316
- [4]Fanaroff AA, Korones SB Incidence, presenting features, risk factors and significance of late onset septicemia in very low birth weight infants. The National Institute of Child Health and Human Development Neonatal Research Network. Pediatric Infectious Disease Journal, 1998.PMID 9686724
- [5]Ehrenkranz RA Early, aggressive nutritional management for very-low-birth-weight infants: what is the evidence? Seminars in Perinatology, 2007.PMID 17462488
- [6]Sharif S, Meader N Probiotics to prevent necrotising enterocolitis in very preterm or very low birth weight infants. Cochrane Database of Systematic Reviews, 2023.PMID 37493095
- [7]Quigley M, Embleton ND Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database of Systematic Reviews, 2019.PMID 31322731
- [8]Oddie SJ, Young L Slow advancement of enteral feed volumes to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database of Systematic Reviews, 2021.PMID 34427330
- [9]Perumbil Pathrose S, Spence K A cross-sectional survey of enteral feeding tube placement and gastric residual aspiration practices: need for an evidence-based clinical practice guideline. Advances in Neonatal Care, 2021.PMID 33427751
- [10]Mihatsch WA, von Schoenaich P The significance of gastric residuals in the early enteral feeding advancement of extremely low birth weight infants. Pediatrics, 2002.PMID 11875141