Paeds · fetal-neonatal-and-perinatal
Respiratory distress syndrome of prematurity
Also known as Hyaline membrane disease · Surfactant deficiency disease · Neonatal respiratory distress syndrome · RDS of prematurity
Fellowship guide to respiratory distress syndrome of prematurity: surfactant deficiency as the central mechanism, the gestational-age incidence ladder, clinical and radiographic features, the differential from transient tachypnoea and sepsis, and the full management bundle of antenatal corticosteroids, early nasal CPAP, surfactant replacement, oxygen targeting, mechanical ventilation and caffeine.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 27-week infant is grunting and retracting in the first hour of life, the inspired oxygen creeping upward. That is the opening scene of respiratory distress syndrome of prematurity, the prototypical lung disease of the preterm newborn, and one of the defining problems of neonatology. It is caused primarily by deficiency of pulmonary surfactant, the phospholipid-rich mixture secreted by the type II pneumocyte that lines alveoli and lowers surface tension at the air-liquid interface. Without enough of it, alveoli collapse at end-expiration, the lung becomes stiff and poorly aerated, and the infant works hard and fails to oxygenate. [1] [3]
The names carry the history. "Hyaline membrane disease" describes the eosinophilic alveolar lining seen at autopsy in the era before surfactant therapy. "Surfactant deficiency disease" names the mechanism. The modern term, respiratory distress syndrome of prematurity, keeps the mechanism central while signalling that the syndrome is graded, modifiable, and largely preventable. [3]
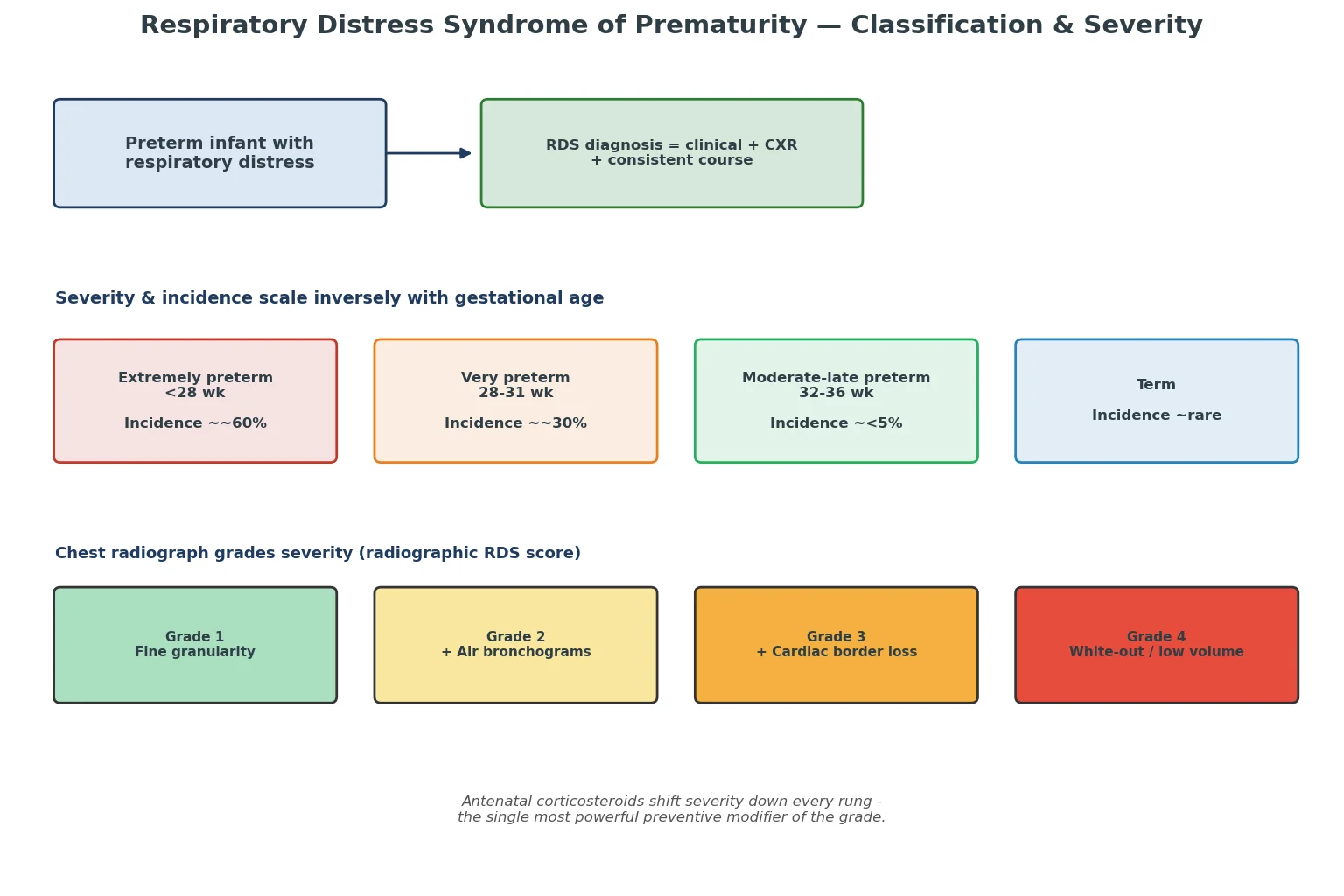
Two facts shape every decision. First, severity and incidence scale inversely with gestational age: the smaller and earlier the infant, the more likely and the worse the disease. Second, antenatal corticosteroids given to the mother are the single most powerful modifier, reducing both incidence and severity. Hold those two together and you have the strategic frame for the whole topic. [1] [4]
Classification
RDS is best classified along two axes that you read together at the bedside. The first is gestational age and incidence, which sets prior probability before the infant takes a breath. The second is severity, judged from the inspired oxygen requirement, the level of respiratory support needed, and the chest radiograph. [1]
The radiograph carries a four-point severity ladder. Grade 1 shows fine granular opacities, grade 2 adds prominent air bronchograms, grade 3 loses the cardiac and diaphragmatic borders, and grade 4 shows a near-total white-out with small low-volume lungs and a bell-shaped thorax. The grade tracks the FiO2 requirement and the likelihood of needing surfactant and ventilation. [3]
Severity also maps onto the support needed. Mild RDS is managed on nasal CPAP alone. Moderate RDS meets the surfactant threshold and may need brief ventilation. Severe RDS requires sustained mechanical ventilation and carries the highest risk of bronchopulmonary dysplasia. Reading severity from the radiograph and the FiO2 together is what tells you where on the management ladder the infant now sits. [1] [2]
Epidemiology & Risk Factors
The headline epidemiology is the gestational-age incidence ladder. Roughly 60 percent of infants born under 28 weeks develop RDS, about 30 percent at 28 to 31 weeks, fewer than 5 percent at 32 to 36 weeks, and the disease is rare at term — when a term infant looks like this, think transient tachypnoea, sepsis, meconium aspiration or a duct-dependent cardiac lesion first. [1]
What raises and what lowers the risk of RDS
- Lower gestational age (the dominant factor)
- Male sex
- Caesarean without labour
- Perinatal asphyxia and acidosis
- Maternal diabetes (hyperinsulinaemia antagonises cortisol)
- Second twin, family history
- Antenatal corticosteroids (24–34 weeks)
- Female sex
- Chronic intrauterine stress: pre-eclampsia, IUGR
- Labour before caesarean
- Tertiary in-hospital delivery
Maternal diabetes is worth a sentence of its own because the mechanism is examinable. Fetal hyperinsulinaemia antagonises the cortisol-driven surge that normally matures the type II pneumocyte and switches on surfactant synthesis, so the infant of a diabetic mother may behave like a more premature lung than the dates suggest. Chronic intrauterine stress does the opposite — pre-eclampsia and growth restriction mildly accelerate maturation, which is why a small-for-gestational-age preterm can sometimes surprise you with a milder course. [1]
Setting matters at the population level. Inborn delivery in a tertiary centre, with antenatal steroids given and a neonatal team present, consistently reduces the severity of RDS and its complications compared with outborn delivery, which is why regionalised perinatal care is itself an intervention. [1]
Pathophysiology
The whole disease turns on one molecule-class doing one job. Pulmonary surfactant is secreted by type II pneumocytes and spreads as a monolayer at the alveolar air-liquid interface, where it lowers surface tension most at end-expiration. By the Laplace relationship, this keeps small alveoli from collapsing into large ones and holds the lung open at a low, stable pressure. Surfactant begins to appear around 24 weeks and rises sharply toward term, which is exactly the gestational window where RDS becomes common. [3]
When surfactant is deficient, the mechanics unravel. Surface tension rises, alveoli collapse at end-expiration, functional residual capacity falls, and lung compliance drops. Each breath costs far more work, and the lung spends most of its cycle under-aerated. The result is a low-volume, stiff lung that is the radiographic and physiological signature of RDS. [3]
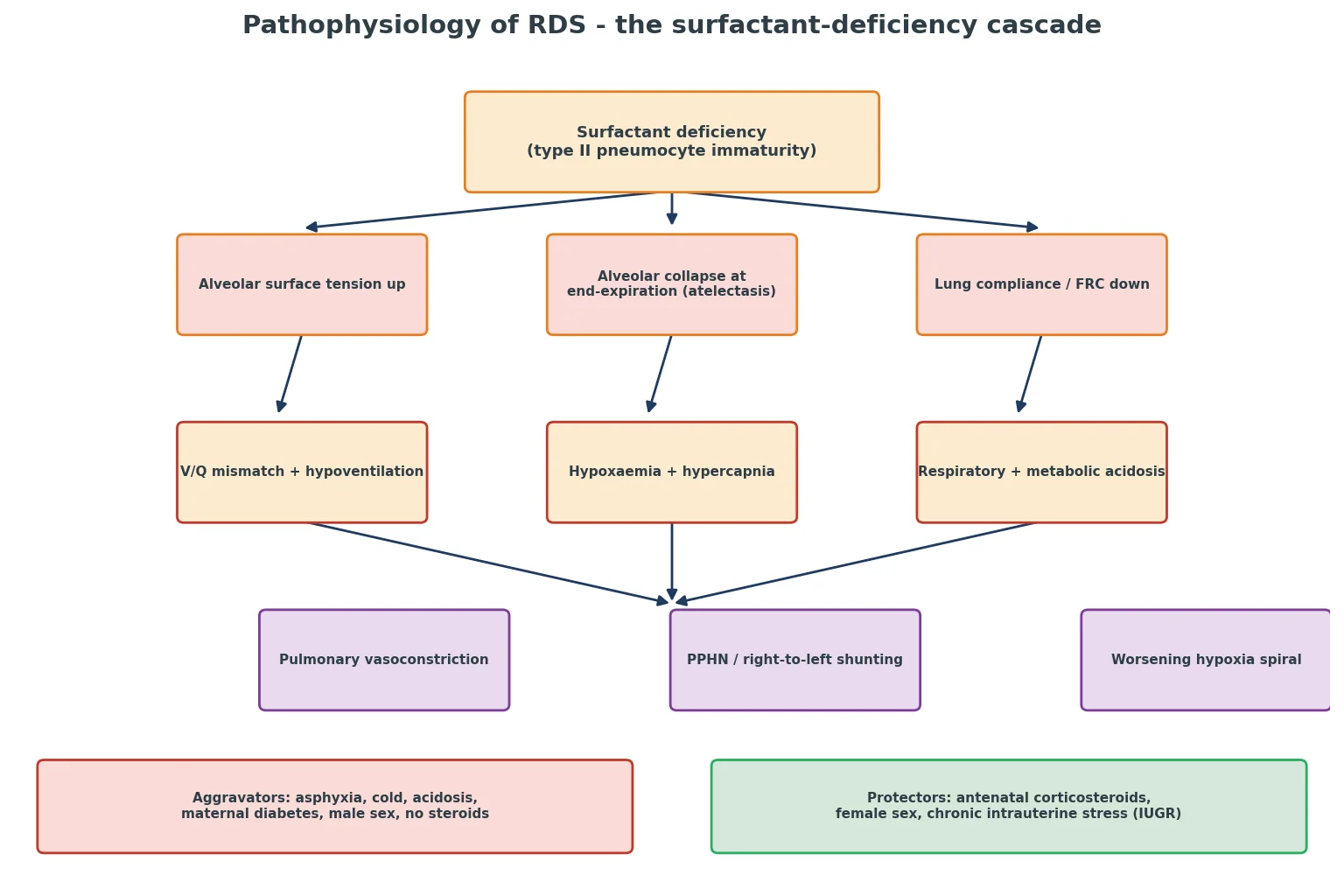
Atelectasis then triggers the gas-exchange collapse. Collapsed alveoli are perfused but not ventilated, so blood shunts right-to-left within the lung, producing hypoxaemia that does not correct with added oxygen alone. Hypoventilation raises the carbon dioxide, and the combined respiratory and metabolic acidosis does two damaging things: it directly inhibits any remaining surfactant function, and it constricts the pulmonary arterioles. If the hypoxia and acidosis persist, pulmonary vascular resistance stays high, the fetal shunts stay open, and the infant tips into persistent pulmonary hypertension of the newborn — a dangerous escalation of what began as a surfactant problem. [1] [3]
This cascade explains why the aggravators are so named. Asphyxia, hypothermia and acidosis all impair surfactant function and push the infant down the spiral, while antenatal corticosteroids act upstream by maturing the type II pneumocyte and switching on surfactant synthesis before birth. Knowing the cascade lets you see why gentle ventilation, warmth, oxygen targeting and surfactant are not a random checklist but a coordinated attack on a single mechanism. [3] [4]
Clinical Presentation
The infant with RDS shows the disease in the first minutes to hours of life, and the signs are the signs of a stiff, under-aerated lung worked hard. Tachypnoea above 60 breaths per minute is the floor. Expiratory grunting is the infant generating auto-positive end-expiratory pressure by exhaling against a partially closed glottis, splinting alveoli open against the collapsing tendency — a physiologically meaningful sign, not a curiosity. Subcostal and intercostal retractions and nasal flaring reflect the increased work of breathing, and central cyanosis appears as hypoxaemia deepens. [1] [3]
The time course is characteristic. The distress usually appears within minutes to hours, worsens over the first 24 to 48 hours as the small surfactant reserve is consumed, and then improves after around 72 hours as endogenous surfactant production rises — unless an intervention, most often surfactant, accelerates the turnaround. A preterm infant whose oxygen requirement is climbing through the first hours is following the classical curve, and the climbing FiO2 is the trigger to act. [1]
Extremely preterm infants present more abruptly and often need support from the delivery room, because their surfactant deficit is near-total. Some present with apnoea and fatigue rather than dramatic retractions, because the immature respiratory centre and weak muscles simply give up before the work of breathing becomes visibly dramatic. Recognising fatigue as a sign of failure — not improvement — is essential. [1]
Some features should make you question the diagnosis or look for a complication. A sudden deterioration with asymmetrical breath sounds in a ventilated infant means a pneumothorax until proven otherwise. Pink frothy secretions suggest a pulmonary haemorrhage. Differential cyanosis or cyanosis unresponsive to oxygen points to duct-dependent congenital heart disease. A scaphoid abdomen suggests a diaphragmatic hernia. Each of these changes the single most important next step. [1]
Differential Diagnosis
When a newborn is in respiratory distress, RDS is the leading diagnosis in a preterm infant but never the only possibility, and several mimics change management entirely. Work through the differential by gestational age, onset, radiograph and response to oxygen. [1]
RDS and its mimics — the tell that separates them
- Preterm, surfactant-deficient lung
- Worsens over 24–48 h, FiO2 climbing
- Low-volume granular CXR with air bronchograms
- Responds to surfactant
- Usually term or late-preterm, often after caesarean without labour
- Resolves over 24–72 h
- Streaky perihilar infiltrates, fluid in fissures
- Self-limiting
- Any gestation; maternal risk factors
- May mimic RDS exactly
- Assume and treat empirically until excluded
- Patchy or nodular CXR
- Term or post-term, meconium-stained liquor
- Coarse infiltrates, hyperinflation
- Often with PPHN
- Cyanosis unresponsive to oxygen
- Pre- and post-ductal saturation difference
- Treat with prostaglandin E1
Two rules govern the differential. First, neonatal sepsis can mimic RDS precisely, so a septic screen and empirical antibiotics are part of the workup whenever RDS is the diagnosis, not an alternative to it. Second, any cyanosis that fails to correct with oxygen, or a pre- to post-ductal saturation gap, demands echocardiography and consideration of prostaglandin E1 — missing a duct-dependent lesion is catastrophic. [1]
Clinical & Bedside Assessment
The bedside assessment reads the respiratory system directly. Document the respiratory rate, the work of breathing through retractions and nasal flaring, the presence and quality of grunting, the symmetry and adequacy of air entry, and the colour and perfusion. A structured score such as the Silverman-Andersen or Downes retraction score lets you track severity over time rather than relying on impression. [1]
The inspired oxygen requirement is the most dynamic single measure. A preterm on nasal CPAP whose FiO2 climbs past 0.30 has met the threshold for surfactant in the 2022 European guideline, and the trend matters as much as the number — a steadily rising FiO2 is the infant telling you the surfactant reserve is exhausted. [1]
When an infant is intubated, confirm tube position before giving surfactant down it — bilateral air entry, symmetrical chest rise, and carbon dioxide detection — because surfactant delivered to a malpositioned tube, to one lung, or to the oesophagus does harm and no good. After any dose, watch for the complications of positive pressure: a sudden deterioration means a pneumothorax, and blood-tinged froth means a pulmonary haemorrhage. [1] [2]
Investigations
The chest radiograph is the defining investigation, and its classic triad is low lung volumes, fine granular opacities, and air bronchograms, often with a bell-shaped thorax. The granular pattern reflects widespread alveolar collapse interspersed with aerated bronchi, and the low volume reflects the loss of functional residual capacity. A normal or over-inflated film in a distressed newborn argues strongly against uncomplicated RDS. [1] [3]
In practice, treatment often starts before the radiograph. A preterm infant in increasing distress on CPAP may begin surfactant on clinical grounds, with the film confirming the diagnosis and excluding a pneumothorax, diaphragmatic hernia or alternative pathology shortly after. Delaying surfactant for a radiograph in a deteriorating infant is a common and avoidable error. [1]
Blood gases track the physiological derangement and the response to treatment. The classical pattern is a respiratory acidosis with raised carbon dioxide and a metabolic acidosis reflecting poor perfusion and tissue hypoxia, alongside hypoxaemia. Capillary gases are useful for trending; arterial samples are reserved for severe disease. A persistent metabolic acidosis or rising lactate is a warning that gas exchange and perfusion are failing. [1]
Continuous pre-ductal pulse oximetry is mandatory, with targets set by the gestational-age-specific oxygen strategy. A septic screen and blood cultures are sent and empirical antibiotics started while infection is excluded, because sepsis and RDS are clinically indistinguishable at presentation. Echocardiography is indicated when cyanosis is slow to resolve, to assess pulmonary hypertension and ductal shunting and to exclude structural congenital heart disease. [1]
Management — Resuscitation
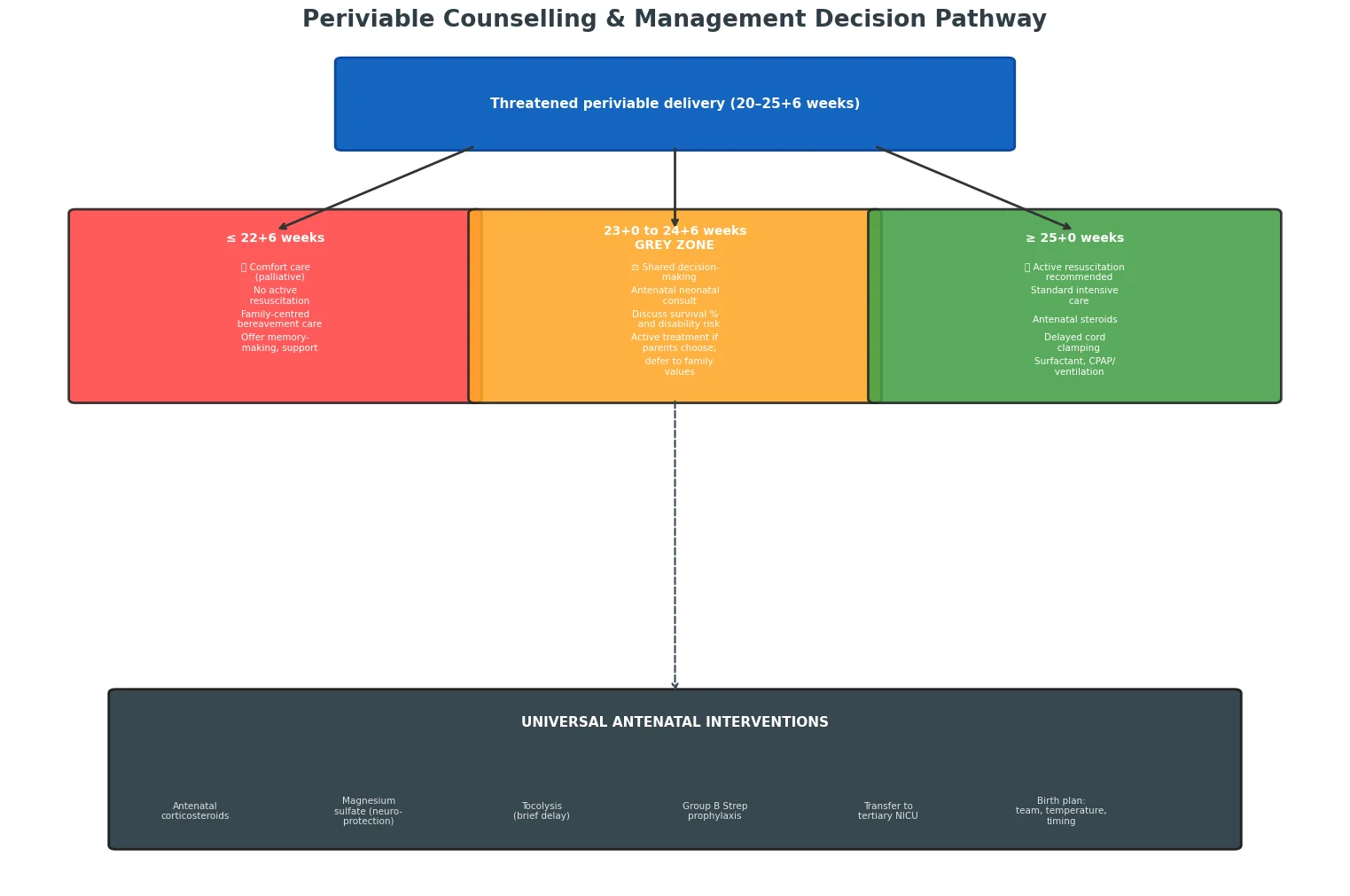
Prevention is the first and most effective treatment. Antenatal corticosteroids — betamethasone or dexamethasone — given to the mother at 24 to 34 weeks' gestation when preterm birth is threatened accelerate fetal lung maturation, reduce the incidence and severity of RDS, and lower neonatal death and intraventricular haemorrhage. The greatest benefit is when delivery occurs 24 hours to 7 days after the course. Roberts and Dalziel's Cochrane review established this as one of the most effective interventions in all of perinatal medicine. [1] [4]
In the delivery suite the principles are warmth, gentleness and early lung recruitment. Receive the preterm infant under a radiant warmer, place in a plastic bag and on a thermal mattress without drying for the most immature, and aim for a temperature of 36.5 to 37.5 degrees from the first minute. Start respiratory support early and gently: for the spontaneously breathing preterm, begin nasal CPAP at 5 to 7 cm of water in the delivery suite rather than routinely intubating. Start in low oxygen — 21 to 30 percent for the preterm — titrated against the gestational-age saturation nomogram. [1]
In Australia and New Zealand, follow the 2022 European Consensus Guideline as adopted by the ANZNN, with delivery planned in a tertiary centre wherever possible, antenatal corticosteroids given before 34 weeks, early CPAP, surfactant at a FiO2 threshold of 0.30, and saturation targets of 91 to 95 percent beyond the first minutes. Retrieval is coordinated through the regional neonatal retrieval network.
[1]Oxygen targeting is set by the NeOProM trials, which compared lower (85 to 89 percent) with higher (91 to 95 percent) saturation targets in extremely preterm infants. The higher target reduced mortality; the lower target reduced severe retinopathy but increased death. The synthesis is clear: target 91 to 95 percent beyond the first minutes, accepting that the very first minutes after birth normally run lower before climbing. Both sustained hypoxia and sustained hyperoxia are harmful. [5] [6]
Management — Definitive & Stepwise
The definitive management is a stepwise ladder, and the skill is escalating only when the step below fails and de-escalating the moment it succeeds. The ladder runs from antenatal corticosteroids and delivery-suite warmth, through early nasal CPAP, to surfactant, to mechanical ventilation, to caffeine and extubation. [1]
Early nasal CPAP with selective surfactant is now first-line. The COIN trial and the early-CPAP arm of the SUPPORT trial (Finer) showed that starting CPAP, rather than routinely intubating every preterm, reduces the need for mechanical ventilation and surfactant without worsening outcome. CPAP splints the lung open, restores functional residual capacity, and buys time for endogenous surfactant production — and for many moderately preterm infants it is all that is needed. [7] [12]
Poractant alfa (porcine surfactant)
Dose
200 mg/kg initial dose (2.5 mL/kg of the 80 mg/mL preparation), with up to two further doses of 100 mg/kg if needed
Surfactant replacement is given once the FiO2 climbs past 0.30 on CPAP. Poractant alfa is dosed at an initial 200 mg per kilogram, with beractant and calfactant as alternatives at their own doses. The technique has evolved: rather than intubating every infant who needs surfactant, the LISA and MIST approaches deliver surfactant through a thin catheter while the infant stays on CPAP, reducing mechanical ventilation and bronchopulmonary dysplasia. The older INSURE technique — intubate, give surfactant, rapidly extubate — remains a reasonable option. The Verder trials established that early surfactant with rapid extubation beats prolonged ventilation. [1] [2] [10]
The respiratory support ladder for RDS
Prevent: antenatal corticosteroids 24–34 weeks + tertiary in-hospital delivery
Delivery suite: warmth 36.5–37.5°C, early nasal CPAP 5–7 cm H2O, low starting oxygen
Surfactant at FiO2 > 0.30 on CPAP — prefer LISA/MIST; otherwise INSURE
Mechanical ventilation if CPAP fails or recurrent apnoea or severe acidosis — lowest effective settings
Caffeine citrate 20 mg/kg load then 5–10 mg/kg daily — for apnoea and to aid extubation
De-escalate: wean FiO2 and pressure as gas exchange improves; extubate to CPAP early
Mechanical ventilation is reserved for infants who fail CPAP and surfactant — those with recurrent apnoea, persistent severe acidosis, or relentless oxygen requirements. Use the lowest effective settings: volume-targeted ventilation is preferred for its tighter control of tidal volume and lower risk of volutrauma, and the goal is always to extubate back to CPAP as soon as the lung recovers. Caffeine citrate is loaded at 20 mg per kilogram then maintained at 5 to 10 mg per kilogram daily; the CAP trial showed it reduces apnoea, shortens the duration of ventilation and oxygen, and improves survival without neurodevelopmental disability. High-risk infants under 1.25 kg now receive it routinely from the first days. [1] [8]
Supportive care completes the bundle: maintain the temperature at 36.5 to 37.5 degrees, manage fluids and nutrition carefully to avoid both dehydration and patent ductus arteriosus, keep the glucose normal, and prevent hypotension and anaemia. The success of RDS management is built as much on these mundane supports as on surfactant and ventilation. [1]
Specific Subtypes & Scenarios
The extremely preterm infant under 28 weeks is the patient who consumes most neonatal skill. Surfactant deficiency is near-universal, the course is abrupt, and the risks of bronchopulmonary dysplasia, intraventricular haemorrhage, retinopathy of prematurity and patent ductus arteriosus are highest. The strategy is antenatal steroids wherever possible, delivery in a tertiary centre, early CPAP, a low threshold for surfactant, low starting oxygen, and caffeine from the first days. [1] [5]
The infant of a diabetic mother may have surfactant maturation delayed by hyperinsulinaemia, so a later-gestation infant can behave like an earlier one. Add the predictable risks of hypoglycaemia, polycythaemia and congenital anomaly, and the respiratory assessment is only one part of a wider screen. The late-preterm infant 34 to 36 weeks with distress is more often transient tachypnoea than RDS, but surfactant deficiency still occurs, especially after caesarean without labour and in the diabetic infant, so the differential must be actively worked. [1]
Perinatal asphyxia worsens surfactant function and acidifies the lung, compounding RDS and complicating decisions about therapeutic hypothermia when the gestation qualifies. The infant failing CPAP needs a focused workup for the reversible causes: a pneumothorax, sepsis, a haemodynamically significant ductus, and persistent pulmonary hypertension each change management and each are missed without looking. [1]
When surfactant is given down an endotracheal tube, give it slowly in fractional boluses, reposition between aliquots, and watch for tube obstruction and desaturation, because too-rapid instillation into a poorly positioned tube causes acute deterioration. In a non-tertiary setting, stabilise with warmth, air-oxygen blended CPAP, glucose and empirical antibiotics, and transfer early with the regional neonatal retrieval service, surfactant given before transfer if the threshold is met. [1] [2]
Complications & Pitfalls
The acute complications of RDS and its treatment are the air-leak syndromes, pulmonary haemorrhage, and intraventricular haemorrhage. A pneumothorax presents as sudden deterioration with asymmetrical breath sounds in a ventilated infant and needs immediate needle decompression or a chest drain. Pulmonary interstitial emphysema reflects barotrauma and predicts bronchopulmonary dysplasia. Pulmonary haemorrhage presents with pink frothy secretions and a sudden fall in lung compliance, treated with increased positive end-expiratory pressure and cautious ventilation. [1] [11]
Bronchopulmonary dysplasia is the chronic lung disease that complicates prolonged ventilation and oxygen in the preterm, defined by the persistence of oxygen requirement or respiratory support at 36 weeks' postmenstrual age. Jobe and Bancalari set out its definition and its inflammatory, injury-and-repair pathogenesis. Prevention is the whole strategy upstream: antenatal steroids, gentle ventilation, early surfactant, caffeine, avoiding hyperoxia and volutrauma, and minimising infection. Once established, BPD means prolonged oxygen, diuretic and steroid trials, and long-term respiratory and neurodevelopmental follow-up. [1] [11]
Oxygen itself is a double-edged treatment. Too little causes hypoxic injury and death; too much drives retinopathy of prematurity and oxidative lung injury. The NeOProM synthesis — that 91 to 95 percent beats both lower and higher targets — is the evidence base for the relentless discipline of saturation targeting in the preterm. The patent ductus arteriosus adds a common complication in the smallest infants, with left-to-right shunting complicating lung mechanics and often needing medical or surgical closure. [5] [11]
The common pitfalls are practical. Giving surfactant down a malpositioned tube, failing to wean the ventilator after the dose, accepting prolonged hypoxia in the first minutes, or running saturations at 100 percent beyond transition — each is avoidable and each is examinable. Document the FiO2 trend, the surfactant dose and time, and the ventilator settings at every step. [1]
Prognosis & Disposition
Outcome in RDS is driven by gestational age, birthweight, antenatal steroid exposure, the severity at presentation, and the complications that follow. In the surfactant-and-CPAP era, survival of even extremely preterm infants with RDS has improved dramatically, though the smallest and earliest still carry the highest risks of bronchopulmonary dysplasia, neurodevelopmental impairment and rehospitalisation. [1] [11]
Uncomplicated RDS typically resolves over the first week, with surfactant often producing dramatic improvement within minutes to hours. The FiO2 and support are weaned as the lung recovers, and the infant is moved from ventilation to CPAP, then to low-flow oxygen or air, then to feeding and discharge planning. Infants who develop bronchopulmonary dysplasia travel a longer path, with prolonged oxygen dependency, growth challenges and specialist follow-up. [1]
The first week and the months that follow
Every preterm graduate of RDS needs structured follow-up: growth monitoring, neurodevelopmental assessment, audiology, and ophthalmology surveillance for retinopathy of prematurity, with the schedule set by gestational age and disease severity. An infant who deteriorates or cannot be stabilised locally is retrieved to a higher-level centre with the regional neonatal team, ventilation and temperature maintained throughout. [1] [5]
Special Populations
The extremely preterm infant under 28 weeks is the population where RDS is universal, where every intervention matters, and where the long-term outcomes are decided. The strategy is built around antenatal steroids, tertiary delivery, early CPAP, early surfactant, low oxygen, caffeine and the prevention of bronchopulmonary dysplasia, with the family engaged and counselled from before birth. [1]
The infant of a diabetic mother carries delayed surfactant maturation alongside hypoglycaemia, polycythaemia and a higher rate of congenital anomaly, so the respiratory assessment sits within a wider metabolic and structural screen. The growth-restricted preterm may have slightly accelerated lung maturation from chronic intrauterine stress but faces the separate risks of asphyxia, hypoglycaemia and hypothermia that small-for-gestational-age infants carry. [1]
In multiple births, the second twin and monochorionic complications such as twin-to-twin transfusion change both the risk and the planning, and two resuscitation teams may be needed. In the outborn or non-tertiary setting, the irreducible core is warmth, blended CPAP, glucose, empirical antibiotics and early retrieval, with surfactant given before transfer if the threshold is met — because the damage done by hypothermia, hyperoxia and delayed surfactant in transit is preventable. [1]
When RDS coexists with hypoxic-ischaemic encephalopathy in an infant of 36 weeks or more, cooling and oxygen targeting must be reconciled, and the lung disease managed within the temperature constraints of therapeutic hypothermia. Family-integrated care, breastfeeding support and parental presence are part of the management of the hospitalised preterm, not an add-on, because the family carries the infant through the long recovery. [1]
Evidence, Guidelines & Regional Differences
The 2022 European Consensus Guideline (Sweet and colleagues) is the current synthesis of practice, setting the recommendations on antenatal corticosteroids, early CPAP, the FiO2-over-0.30 surfactant threshold, oxygen targeting and caffeine. It is the document to cite and the framework to work within. The AAP surfactant clinical report (Polin) sets out the indications, preparations and doses for surfactant replacement. [1] [2]
The oxygen-targeting evidence comes from the SUPPORT, BOOST II and COT trials and the NeOProM prospective meta-analysis (Askie). Together they showed that targeting 91 to 95 percent reduced mortality compared with 85 to 89 percent, while the lower target reduced severe retinopathy at the cost of increased death — a balance resolved firmly in favour of the higher target. [5] [6] [9]
NeOProM (Askie 2018, JAMA)
Population: Extremely preterm infants randomised to lower (85–89%) versus higher (91–95%) oxygen saturation targets
Key finding
Higher target reduced mortality; lower target reduced severe ROP but increased death
Practice change
Target SpO2 91–95% in the preterm beyond the first minutes; both sustained hypoxia and hyperoxia are harmful
The evidence for early CPAP comes from the COIN trial (Morley) and the early-CPAP arm of SUPPORT (Finer), which showed that starting CPAP rather than routinely intubating reduces mechanical ventilation and surfactant without worsening outcome. The Verder trials established early surfactant with rapid extubation, the ancestor of today's LISA and MIST techniques. The CAP trial (Schmidt) established caffeine's role in reducing apnoea and improving survival without disability. [7] [8] [10] [12]
Active controversies remain — the optimal starting oxygen for the preterm, prophylactic versus selective surfactant, volume-targeted versus pressure-limited ventilation, and the role of sustained inflation — but the convergent message across ANZ, UK and North American guidelines is the same: antenatal steroids, early CPAP, surfactant at the right threshold, oxygen at 91 to 95 percent, caffeine, and gentle ventilation. Answer with the current guideline, name the source, and acknowledge where the evidence is still moving. [1] [5]
Exam Pearls
- RDS incidence scales inversely with gestational age: about 60% under 28 weeks, 30% at 28–31 weeks, under 5% at 32–36 weeks, rare at term. [1]
- The classic chest radiograph triad is low lung volumes, fine granular opacities and air bronchograms, often with a bell-shaped thorax. [3]
- Antenatal corticosteroids at 24–34 weeks are the single most effective preventive intervention, reducing RDS, neonatal death and IVH. [4]
- The 2022 European Consensus Guideline sets the surfactant threshold at FiO2 over 0.30 on CPAP. [1]
- Target oxygen saturations of 91–95% beyond the first minutes, informed by the NeOProM meta-analysis. [5]
- Caffeine citrate: load 20 mg/kg, then 5–10 mg/kg daily — the CAP trial showed survival benefit without neurodisability. [8]
- Poractant alfa initial dose is 200 mg/kg (2.5 mL/kg of the 80 mg/mL preparation). [2]
- Expiratory grunting is the infant's auto-PEEP, splinting alveoli open — a physiologically meaningful sign, not a curiosity. [3]
- After surfactant, wean the ventilator promptly — compliance improves within minutes and over-distension risks volutrauma and air leak. [1]
- The COIN and SUPPORT trials established early CPAP over routine intubation; the Verder trials established early surfactant with rapid extubation. [7] [10]
References
- [1]Sweet DG European Consensus Guidelines on the Management of Respiratory Distress Syndrome: 2022 Update. Neonatology, 2023.PMID 36863329
- [2]Polin RA Surfactant replacement therapy for preterm and term neonates with respiratory distress. Pediatrics, 2014.PMID 24379227
- [3]Jobe AH Pulmonary surfactant therapy. N Engl J Med, 1993.PMID 8441430
- [4]Roberts D Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev, 2006.PMID 16856047
- [5]Askie LM Association Between Oxygen Saturation Targeting and Death or Disability in Extremely Preterm Infants in the Neonatal Oxygenation Prospective Meta-analysis Collaboration. JAMA, 2018.PMID 29872859
- [6]Carlo WA Target ranges of oxygen saturation in extremely preterm infants. N Engl J Med, 2010.PMID 20472937
- [7]Morley CJ Nasal CPAP or intubation at birth for very preterm infants. N Engl J Med, 2008.PMID 18272893
- [8]Schmidt B Long-term effects of caffeine therapy for apnea of prematurity. N Engl J Med, 2007.PMID 17989382
- [9]Stenson BJ Oxygen saturation and outcomes in preterm infants. N Engl J Med, 2013.PMID 23642047
- [10]Verder H Surfactant therapy and nasal continuous positive airway pressure for newborns with respiratory distress syndrome. N Engl J Med, 1994.PMID 8090164
- [11]Jobe AH Bronchopulmonary dysplasia. Am J Respir Crit Care Med, 2001.PMID 11401896
- [12]Finer NN Early CPAP versus surfactant in extremely preterm infants. N Engl J Med, 2010.PMID 20472939