Paeds · fetal-neonatal-and-perinatal
Retinopathy of prematurity
Also known as Retinopathy of prematurity · ROP · Retrolental fibroplasia
Fellowship guide to retinopathy of prematurity: classification by ICROP-3, screening, the two-phase pathogenesis, and Type 1 treatment.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Retinopathy of prematurity (ROP) is a disorder of the developing retinal blood vessels in which the immature, incompletely vascularised retina grows abnormal new vessels that can scar, contract, and detach. It is the leading cause of preventable childhood blindness in high-income countries, and it is entirely a disease of prematurity: the more immature the infant, the greater the risk [7].
The crucial clinical point is that ROP is silent at the bedside. An infant can be growing, weaning from oxygen, and outwardly well while sight-threatening disease develops silently in the periphery of the retina. For this reason, ROP is not a diagnosis made from symptoms or vital signs. It is found only by scheduled retinal examination of infants who are at risk by virtue of gestational age and birth weight, and the entire purpose of a screening programme is to detect and treat the disease before it reaches the point of irreversible retinal detachment [6].
Classification is governed worldwide by the International Classification of Retinopathy of Prematurity, now in its third edition (ICROP-3), which standardises how every eye is described by three axes — zone, stage, and the presence of plus disease [1].
Classification
ROP is classified along three axes, and an examiner will expect you to describe an eye in exactly this order: which zone, what stage, and whether plus disease is present. Each axis answers a different question. Zone tells you how posterior and dangerous the disease is. Stage tells you how severe the local vascular change is. Plus disease tells you how active and progressive the disease is right now [1].
The retina is divided into three concentric zones centred on the optic disc, not the fovea. Zone I is the smallest and most posterior circle, with a radius twice the distance from the optic disc to the fovea. Zone II extends from the edge of Zone I out to the nasal ora serrata. Zone III is the remaining temporal crescent. Because normal vessels reach the nasal ora first (around 36 weeks postmenstrual age) and the temporal ora last (around 40 weeks), the temporal periphery is the last region to vascularise and the most common site of disease [1].
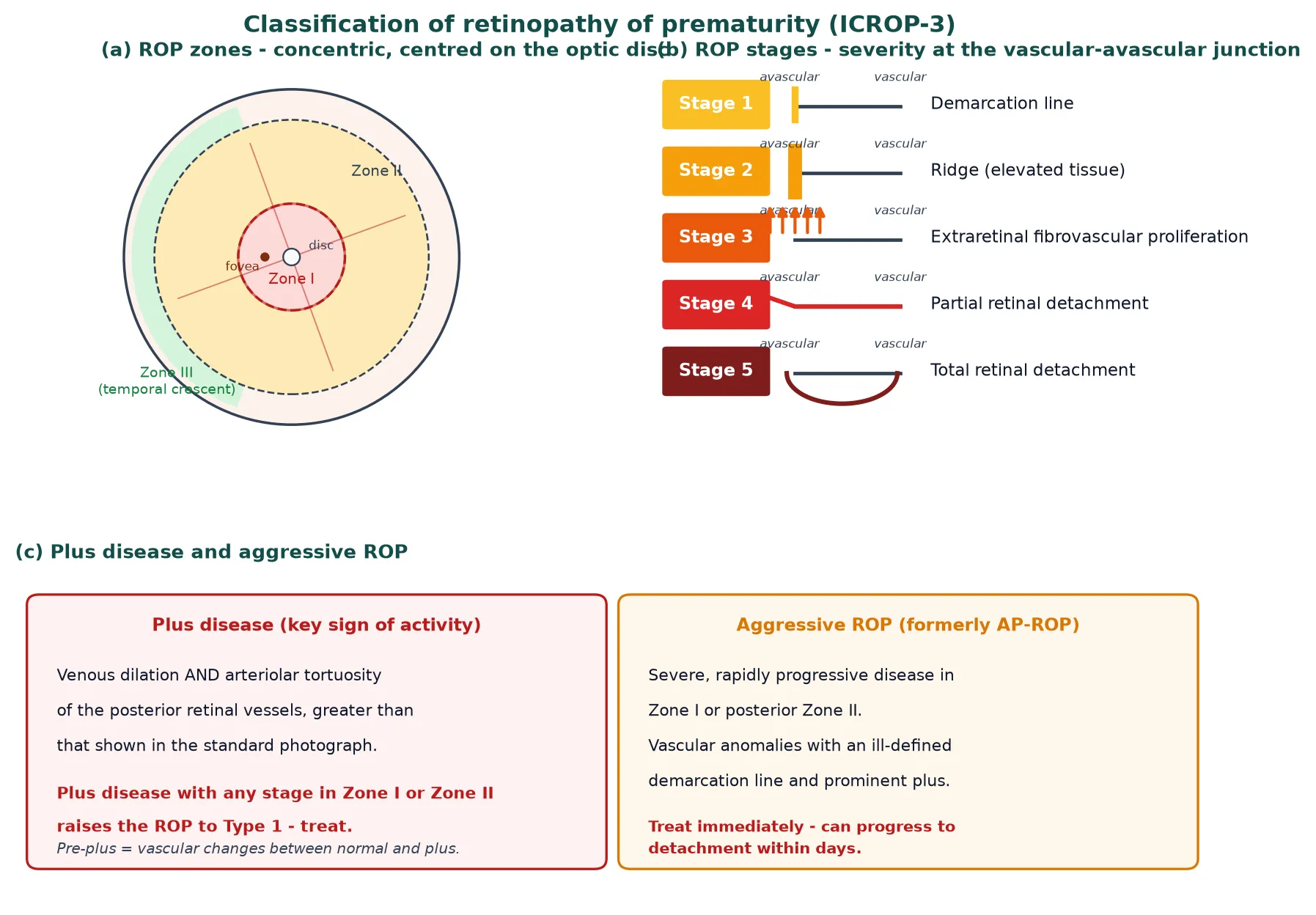
The five stages describe what is happening at the junction between vascularised and avascular retina. Stage 1 is a thin demarcation line. Stage 2 is a raised ridge of tissue. Stage 3 adds extraretinal fibrovascular proliferation growing from the ridge into the vitreous. Stage 4 is partial retinal detachment, split into 4A (extrafoveal) and 4B (involving the fovea). Stage 5 is total retinal detachment, taking on the classic funnel shape [1].
Plus disease is the single most important feature for decision-making. It is defined as venous dilation and arteriolar tortuosity of the posterior retinal vessels that is greater than or equal to the vascular change shown in the standard published photograph, assessed at least two disc diameters from the optic disc. Pre-plus disease describes vascular abnormalities that are more than normal but less than full plus disease. The presence of plus disease signals an actively progressing process and, with the appropriate zone and stage, is what pushes an eye over the treatment threshold [2].
The 2005 ICROP revision formalised aggressive posterior ROP, and ICROP-3 renamed it simply aggressive ROP, because such disease is not always confined to the posterior retina. Aggressive ROP is a severe, rapidly progressing vasoproliferative process in Zone I or posterior Zone II with an ill-defined demarcation line, shunts, and prominent plus disease that can advance to retinal detachment within days. It demands immediate treatment [1].
Epidemiology & Risk Factors
The risk of ROP is set almost entirely by how premature and how small the infant is. Among extremely preterm infants (under 28 weeks) roughly two-thirds develop some ROP, and population data from the Neonatal Research Network confirm that retinopathy is one of the most common morbidities of extreme prematurity alongside chronic lung disease and intraventricular haemorrhage [8]. In contrast, ROP is rare in infants born at 32 weeks or more or weighing over 1500 g at birth [6].
The modifiable risk factors revolve around oxygen, growth, and systemic illness. Uncontrolled or fluctuating oxygen exposure is central: both relative hyperoxia in the early weeks and the swings in saturation that follow unstable ventilation amplify the disease process. Poor postnatal growth matters because insulin-like growth factor 1 (IGF-1), which is normally supplied by the placenta and tracks closely with weight gain, is required for retinal vessels to grow. Sepsis, anaemia, and blood transfusion add independent risk, and a deteriorating infant is a higher-risk infant [7].
A preventable "third epidemic" of ROP is now unfolding in middle-income countries, where improving neonatal survival is outpacing the introduction of monitored oxygen delivery and organised screening. In these settings, larger and more mature infants than in high-income countries are developing severe ROP because oxygen is delivered without pulse-oximetry control and screening programmes are incomplete [7].
Pathophysiology
To understand ROP, picture what is normal first. Retinal blood vessels grow outwards from the optic disc during fetal life, reaching the nasal ora serrata at about 36 weeks postmenstrual age and the temporal ora at about 40 weeks. A preterm infant is born while this vascularisation is still incomplete, leaving a peripheral rim of avascular retina — a metabolically hungry tissue with no blood supply, waiting to be vascularised [7].
The disease then unfolds in a classic two-phase model. In Phase 1, the relative hyperoxia of extrauterine life, together with the loss of placental IGF-1, suppresses vascular endothelial growth factor (VEGF) and IGF-1 signalling. The result is arrested growth and even regression of the developing capillaries, enlarging the avascular retina rather than closing it. In Phase 2, that avascular retina becomes hypoxic as the infant grows and its metabolic demand rises. The hypoxic tissue releases a surge of VEGF; as IGF-1 recovers with postnatal growth, the drive to neovascularisation is unleashed. But the new vessels are abnormal — disorganised, leaky, and prone to forming scars that contract and pull the retina off the back of the eye [7].
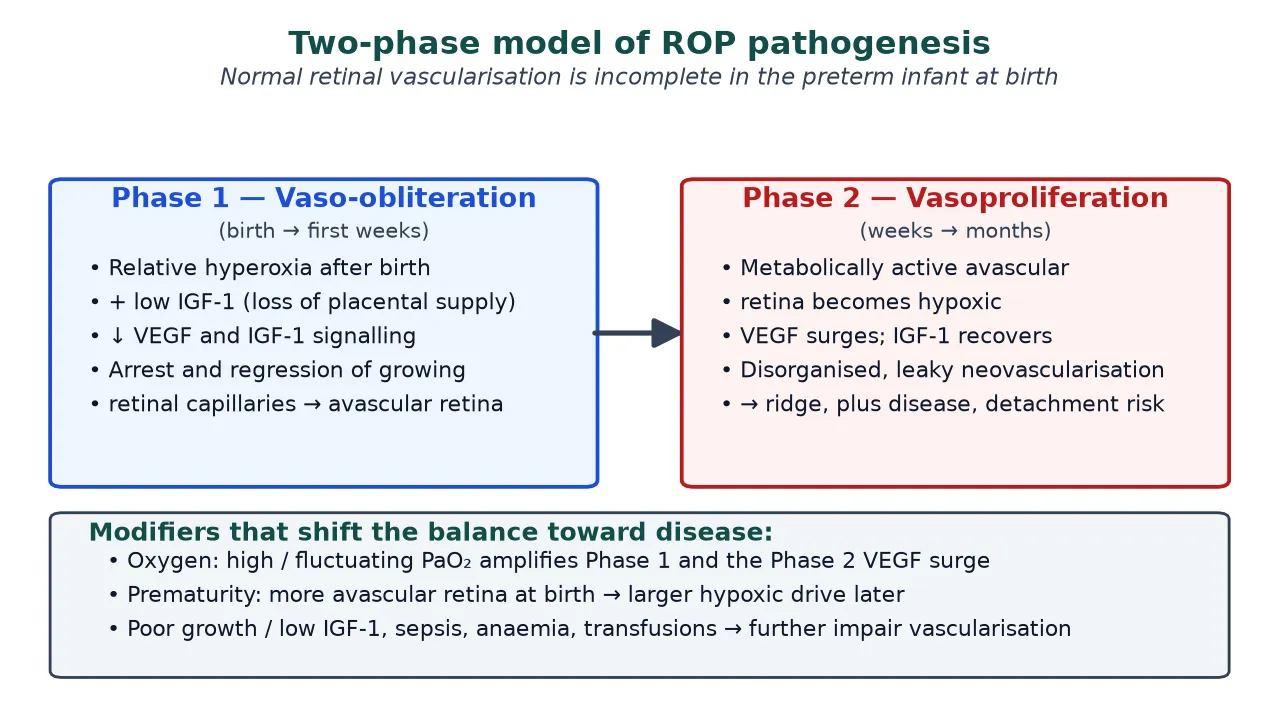
This model explains every risk factor and every treatment. Oxygen swings worsen both phases: too much drives Phase 1 destruction, too little and too late fuels the Phase 2 VEGF surge. Poor growth keeps IGF-1 low and prolongs the window of vulnerability. Laser treatment works by ablating the avascular retina and removing the source of the VEGF surge; anti-VEGF drugs work by directly neutralising that surge [7].
Clinical Presentation
ROP produces no symptoms and no signs that a clinician can detect at the bedside. There is nothing to find on a standard neonatal examination. The retinal changes — the demarcation line, the ridge, the extraretinal proliferation, the vascular tortuosity of plus disease, and ultimately detachment — are visible only through a dilated pupil with an indirect ophthalmoscope [6].
What the clinician does see is the risk profile, not the disease itself. An infant who fits the screening criteria is presumed to be at risk regardless of how well they look. An infant who is unstable, growing poorly, requiring escalating or fluctuating oxygen, or who has intercurrent sepsis or anaemia is at heightened risk of rapid progression and must not miss scheduled examinations [7].
When ROP is missed or untreated, the late presentation is visual: an eye that has progressed to retinal detachment may show leukocoria (a white pupillary reflex), strabismus, nystagmus, or simply no visual behaviour. By this stage the outcome is often irreversible, which is why the entire screening programme exists to intervene before detachment occurs [1].
Differential Diagnosis
The diagnosis of ROP in a preterm infant is rarely in doubt once the retina is examined, but the differential matters when an abnormal retinal vascular pattern or leukocoria is found in a larger or term infant, where ROP should not be the default. The key distinction is whether the infant meets the classic risk profile and whether the findings are bilateral and confined to the avascular periphery [1].
| Condition | Key distinguishing features | Diagnostic clue |
|---|---|---|
| Familial exudative vitreoretinopathy (FEVR) | Term infant, family history, peripheral avascular retina | Autosomal dominant, no prematurity |
| Persistent fetal vasculature (PFV) | Unilateral, microphthalmia, retrolental mass | Leukocoria from birth |
| Norrie disease | X-linked male infant, grey retrolental mass | Deafness and developmental delay |
| Incontinentia pigmenti | Female infant, skin then dental and ocular signs | Streaked skin lesions |
| Coats disease | Unilateral retinal telangiectasia | Exudative detachment in a boy |
| Congenital cataract | Opacity in the lens, red reflex absent | Seen on direct viewing |
| Retinoblastoma | Leukocoria, calcified retrolental mass | MRI and ophthalmology review |
The most important mimic is familial exudative vitreoretinopathy (FEVR), which produces a peripheral avascular retina and neovascularisation that can look exactly like ROP but occurs in term infants and often has a family history. Recognising FEVR matters because its management and genetic counselling differ from ROP [1].
Clinical & Bedside Assessment
The retinal examination is the bedside assessment, and it must be done properly. Both eyes are dilated with a mydriatic such as tropicamide, and an experienced examiner performs indirect binocular ophthalmoscopy, usually with scleral indentation to view the peripheral retina where ROP lives. For each eye the examiner records the zone, the stage, the extent of disease in clock-hours, and the presence of plus or pre-plus disease [1].
Recognising aggressive ROP is a critical skill, because its appearance is subtle and its course is explosive. The junction between vascularised and avascular retina is ill-defined, the neovascularisation may be flat rather than proliferative, shunts are prominent, and plus disease is marked. This pattern in Zone I or posterior Zone II should trigger treatment without waiting for a higher stage [1].
The systemic assessment runs in parallel with the ocular one. Review the oxygen targeting and stability, the growth trajectory, the haemoglobin, and any active sepsis, because these modifiable factors both raise the risk of progression and influence how urgently the next examination is needed [7].
Investigations
There is no blood test, imaging test, or monitoring device that diagnoses ROP. The investigation is the serial retinal examination, performed on a schedule determined by gestational age and the findings of previous examinations. Wide-field retinal photography with devices such as the RetCam supplements the examination by creating a permanent, reviewable image of the peripheral retina [6].
Screening pathway
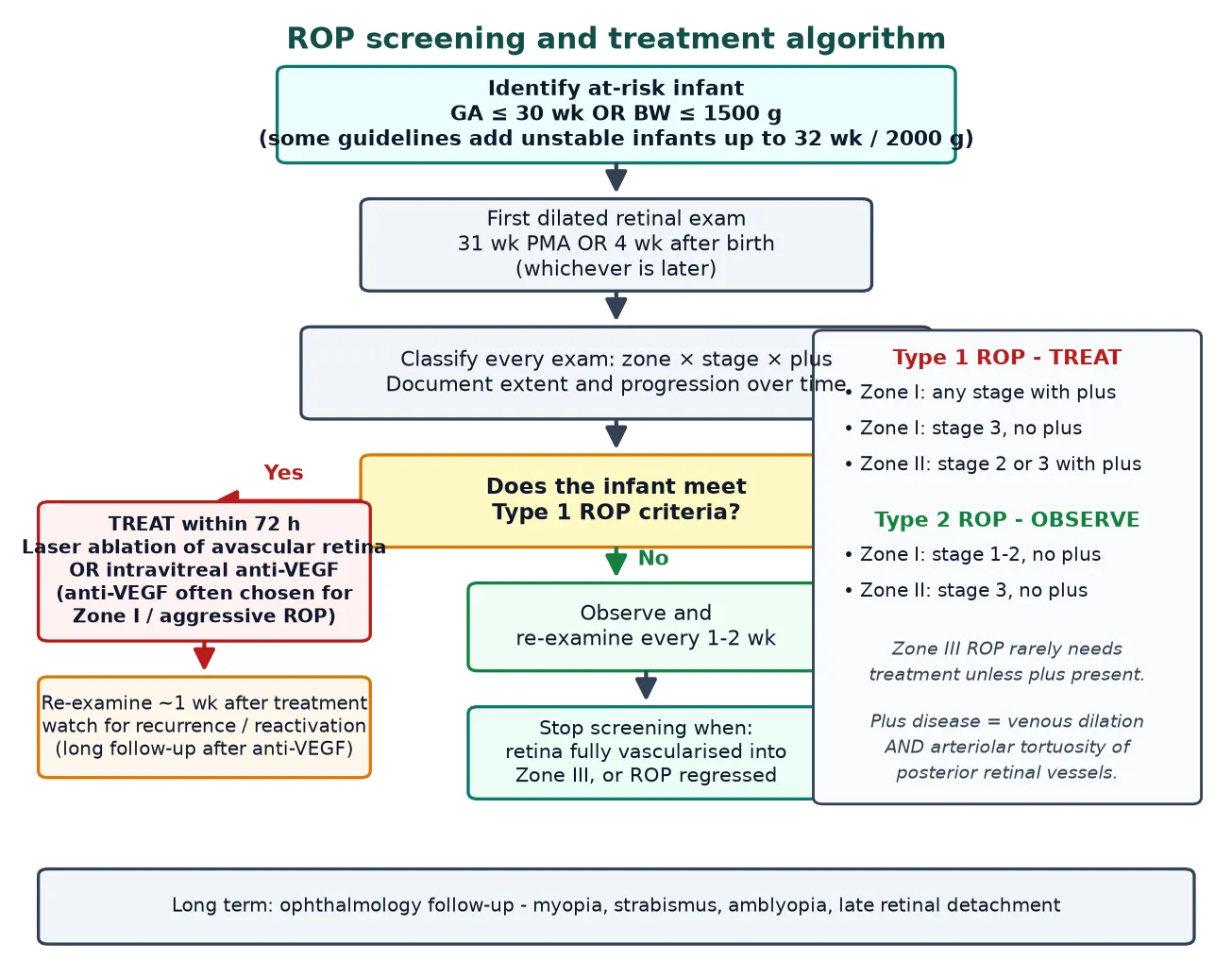
Identify eligibility: GA of 30 weeks or less OR birth weight of 1500 g or less
Arrange first examination at 31 weeks PMA or 4 weeks of age, whichever is later
Dilate and examine both eyes by indirect ophthalmoscopy
Classify each eye by zone, stage, extent, and plus disease
Set the interval to the next examination (1 to 2 weeks for active disease)
Stop screening once vascularised into Zone III or ROP has regressed
Telemedicine has become an important adjunct, particularly where ophthalmologists are scarce. The e-ROP study validated a remote reading system in which trained imagers capture wide-field photographs that are graded off-site, demonstrating that telemedicine can reliably identify referral-warranted ROP and extend screening to regions without on-site ophthalmology [10].
Weight-gain-based risk algorithms use serial postnatal weight as a surrogate for IGF-1 to predict which infants will develop severe ROP. Models such as WINROP, the CHOP-ROP model, and the G-ROP model can stratify risk and, in some settings, safely reduce the number of examinations in low-risk infants, although they supplement rather than replace ophthalmoscopic screening [7].
Management — Resuscitation
The first management step is prevention, and it begins on day one of life. The goal is to protect the developing retinal vessels from the oxygen injury that drives Phase 1 while avoiding the hypoxia that fuels Phase 2. Large trials of saturation targeting converged on a recommended range of 91 to 95 percent for preterm infants, because lower targets increased mortality without a worthwhile reduction in severe ROP [9].
Supplemental oxygen targeting
Loading dose
Target SpO2 91 to 95 percent
Maintenance dose
Avoid large or rapid swings in saturation
Systemic optimisation runs alongside oxygen control. Good postnatal growth restores IGF-1 and supports normal vascularisation, while prompt treatment of anaemia and sepsis removes independent drivers of progression. Unnecessary blood transfusions and erratic oxygen swings should be minimised [7].
Once an examination identifies Type 1 ROP, the time-critical action is to arrange treatment within 72 hours. Aggressive ROP may need treatment even sooner, within 24 to 48 hours, because of its capacity to reach detachment within days [4].
Management — Definitive & Stepwise
Definitive treatment has two main options: laser photocoagulation of the avascular retina and intravitreal injection of a vascular endothelial growth factor antagonist. Both work by removing the drive to neovascularisation — laser physically ablates the VEGF-producing avascular retina, while anti-VEGF neutralises the molecule directly. The choice depends on the zone, the systemic state of the infant, and the reliability of follow-up [4].
Laser photocoagulation
Laser ablation of the avascular peripheral retina is the established standard treatment and is highly effective at halting progression. By destroying the tissue that produces the VEGF surge, it removes the stimulus for further neovascularisation. Its drawbacks are local: laser burns large areas of peripheral retina, producing long-term myopia, constriction of the visual field, and reduced contrast sensitivity [4].
Intravitreal anti-VEGF therapy
Intravitreal anti-VEGF injection is particularly valuable for Zone I and posterior Zone II disease, where the area needing laser would be large and visually destructive. The BEAT-ROP trial showed that a single intravitreal injection of bevacizumab (0.625 mg in 0.025 mL) was superior to conventional laser for Zone I stage 3 disease with plus, with lower rates of recurrence in this high-risk zone [5].
Intravitreal bevacizumab
Loading dose
0.625 mg in 0.025 mL intravitreally
Maintenance dose
Single injection, repeat only for recurrence
Anti-VEGF therapy also spares the peripheral retina and leads to less myopia than laser. Follow-up of BEAT-ROP showed that bevacizumab-treated eyes developed significantly less myopia than laser-treated eyes at follow-up [11]. Against these advantages must be weighed the systemic concern that VEGF has roles beyond the eye, the need for aseptic intraocular injection, and the risk of late reactivation that demands prolonged surveillance [5].
Surgery for retinal detachment
If disease progresses to stage 4 or 5 retinal detachment, management passes to vitreoretinal surgery with scleral buckling or vitrectomy. These procedures carry a guarded prognosis and are a clear marker of failed prevention, which is why the whole system is designed to treat before detachment occurs [3].
Specific Subtypes & Scenarios
| Scenario | Key features | Management focus |
|---|---|---|
| Zone I disease | Most posterior, highest risk | Low threshold to treat; anti-VEGF often preferred |
| Aggressive ROP | Rapidly progressive, ill-defined junction, prominent plus | Treat immediately within 24 to 48 hours |
| Zone II Type 1 | Stage 2 or 3 with plus | Laser or anti-VEGF within 72 hours |
| Zone III disease | Temporal crescent, low risk | Observe until vascularised; rarely needs treatment |
| Type 2 ROP | Below the treatment threshold | Close observation; treat if it progresses to Type 1 |
| Post anti-VEGF | Late reactivation possible | Prolonged surveillance beyond the usual window |
Zone I disease carries the highest risk because it is the most posterior, so the threshold to treat is lower and anti-VEGF is often preferred over the extensive laser that Zone I would require. Aggressive ROP is the scenario that catches clinicians out: it looks deceptively subtle but can reach detachment within days, so it is treated immediately [1].
Eyes treated with anti-VEGF behave differently from laser-treated eyes and form a distinct follow-up scenario. Because the drug's effect wanes and the VEGF drive can return, late reactivation is possible beyond the usual screening window, so these infants need prolonged, vigilant surveillance [5].
Complications & Pitfalls
The defining complication of untreated ROP is retinal detachment leading to blindness. Even ROP that regresses without surgery is not benign: treated and regressed eyes carry a lifelong increased risk of myopia, strabismus, amblyopia, and late retinal detachment, so all affected infants need long-term ophthalmology follow-up [7].
Each treatment carries its own complications. Laser produces peripheral retinal destruction with consequent myopia and visual-field loss. Intravitreal anti-VEGF carries the small but real risks of intraocular infection, retinal detachment from the injection, the theoretical systemic effects of suppressing VEGF in a developing infant, and late reactivation of disease [5].
The most dangerous pitfalls are programmatic rather than clinical. Missing or delaying a scheduled examination in an eligible infant is the leading preventable cause of poor outcome. Relying on stable saturations or good growth to defer screening, treating after the Type 1 threshold rather than at it, and failing to arrange follow-up after anti-VEGF are all classic errors [6].
Prognosis & Disposition
Most ROP regresses without sequela when it is detected early and treated at the Type 1 threshold. The prognosis worsens steadily with posterior disease (Zone I), with aggressive ROP, and especially once retinal detachment has occurred and surgery is required [7].
Disposition is twofold. In the short term, an infant with active or treated ROP remains under scheduled ophthalmological surveillance until the retina is fully vascularised into Zone III or the ROP has regressed. In the long term, every infant who had ROP — and many who were simply at risk — enters a lifetime of ophthalmology follow-up to detect and manage refractive error, strabismus, amblyopia, and late retinal problems [6].
Special Populations
The extreme-preterm, extremely-low-birth-weight infant is the prototypical ROP patient and carries the highest burden of disease. Growth-restricted infants are a particularly important subgroup because low IGF-1 impairs vascularisation, and they can develop significant ROP even when their gestational age is not the lowest [7].
[7]Indigenous and remotely located infants may face reduced access to screening and treatment, so neonatal networks plan retrieval and telemedicine to maintain screening continuity. Any infant transferred between units — for example, a baby repatriated from a tertiary NICU to a level two nursery — must have explicit handover of their ROP screening schedule so that no examination is lost in the transfer [6].
Evidence, Guidelines & Regional Differences
The evidence base for ROP is built on a sequence of landmark trials that progressively moved treatment earlier and broadened its options. CRYO-ROP, reported in 1988, was the first to prove that treating established threshold disease reduced unfavourable structural outcomes, establishing the principle that ROP treatment prevents blindness [3].
The Early Treatment for Retinopathy of Prematurity (ETROP) trial, reported in 2003, redefined the treatment point. Rather than waiting for threshold disease, it showed that treating earlier — at the Type 1 pre-threshold stage — improved outcomes, and it formalised the Type 1 and Type 2 criteria that still drive decisions today [4].
BEAT-ROP (2011)
RCT: intravitreal bevacizumab versus laser for stage 3+ ROP
Population: Infants with Zone I or posterior Zone II stage 3+ disease
Key finding
Bevacizumab superior, especially in Zone I disease
Practice change
Established anti-VEGF for posterior disease and raised surveillance for late reactivation
The BEAT-ROP trial in 2011 introduced intravitreal bevacizumab into routine practice, showing superiority over laser for Zone I stage 3 disease with plus disease. Subsequent work confirmed the refractive advantage of anti-VEGF over laser and refined surveillance for its late reactivation [11].
Oxygen targeting was shaped by the SUPPORT, BOOST II, and COT trials, which together showed that lower saturation targets increased mortality without a meaningful reduction in severe ROP, leading to the consensus 91 to 95 percent target [9]. Regional guidelines differ in detail: the AAP, AAO, and AAPOS joint statement governs screening in the United States, the RCPCH and Royal College of Ophthalmologists guide UK practice, and Australian and New Zealand units follow their own national consensus, though all converge on the same risk-based screening principle [6].
The main ongoing controversies concern the optimal anti-VEGF agent and dose, the long-term systemic safety of intravitreal anti-VEGF in developing infants, and the exact role of telemedicine and weight-gain algorithms in reducing examination burden without missing treatable disease [5].
Exam Pearls
Screen every infant with a gestational age of 30 weeks or less or a birth weight of 1500 g or less, and arrange the first examination at 31 weeks postmenstrual age or 4 weeks of age, whichever is later. These thresholds are the most frequently tested facts in ROP [6].
The zones are centred on the optic disc, not the fovea, and Zone I has a radius twice the disc-to-fovea distance. Plus disease is the dominant predictor of progression and the key treatment trigger — more important than stage alone. Normal vascularisation reaches the nasal ora at about 36 weeks and the temporal ora at about 40 weeks [1].
For Zone I disease, anti-VEGF is often preferred over laser, and the BEAT-ROP dose of bevacizumab was 0.625 mg intravitreally. Finally, ICROP-3 renamed aggressive posterior ROP to aggressive ROP, because such disease is not always confined to the posterior retina [5].
ROP DECISION
References
- [1]Chiang MF, Quinn GE, Fielder AR, et al International Classification of Retinopathy of Prematurity, Third Edition Ophthalmology, 2021.PMID 34247850
- [2]International Committee for the Classification of Retinopathy of Prematurity The International Classification of Retinopathy of Prematurity revisited Arch Ophthalmol, 2005.PMID 16009843
- [3]Cryotherapy for Retinopathy of Prematurity Cooperative Group Multicenter trial of cryotherapy for retinopathy of prematurity: preliminary results Pediatrics, 1988.PMID 2895910
- [4]Early Treatment for Retinopathy of Prematurity Cooperative Group Revised indications for the treatment of retinopathy of prematurity: results of the early treatment for retinopathy of prematurity randomized trial Arch Ophthalmol, 2003.PMID 14662586
- [5]Mintz-Hittner HA, Kennedy KA, Chuang AZ; BEAT-ROP Cooperative Group Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity N Engl J Med, 2011.PMID 21323540
- [6]Fierson WM, American Academy of Pediatrics Section on Ophthalmology, et al Screening Examination of Premature Infants for Retinopathy of Prematurity Pediatrics, 2018.PMID 30478242
- [7]Hellstrom A, Smith LEH, Dammann O Retinopathy of prematurity Lancet, 2013.PMID 23782686
- [8]Stoll BJ, Hansen NI, Bell EF, et al Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2012 JAMA, 2015.PMID 26348753
- [9]SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network Early CPAP versus surfactant in extremely preterm infants N Engl J Med, 2010.PMID 20472939
- [10]Quinn GE, Ying GS, Daniel E, et al; e-ROP Cooperative Group Validity of a telemedicine system for the evaluation of acute-phase retinopathy of prematurity JAMA Ophthalmol, 2014.PMID 24970095
- [11]Geloneck MM, Chuang AZ, Clark WL, et al; BEAT-ROP Cooperative Group Refractive outcomes following bevacizumab monotherapy compared with conventional laser treatment: a randomized clinical trial JAMA Ophthalmol, 2014.PMID 25103848