Paeds · fetal-neonatal-and-perinatal
Routine care of the healthy newborn
Also known as Newborn care · Postnatal care of the newborn · Neonatal routine care · Well newborn care · Baby check · Essential newborn care
Fellowship guide to routine care of the healthy term newborn: golden-hour immediate care, feeding establishment, vitamin K and hepatitis B prophylaxis, cord and skin care, jaundice and hypoglycaemia monitoring, safe sleep counselling, discharge readiness and follow-up, with regional guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A healthy term newborn looks well at birth but is not finished adapting. The placenta has been the lungs, liver, thermostat and metabolic engine for nine months. At clamping of the cord, all of that work transfers to the newborn in a matter of minutes. Routine care exists because that transition is predictable but not guaranteed — small failures in warmth, feeding, glucose or bilirubin handling can silently become emergencies in the first days of life. [9] [1]
This topic covers everything that happens to a well baby between cord clamping and safe discharge home. It does not cover neonatal resuscitation (which assumes the baby is not transitioning well), intensive care, or the newborn screening programmes themselves (bloodspot, hearing, CCHD pulse oximetry) — those have their own dedicated topics. It does cover how those screens fit into the routine care timeline and what to do when they are incomplete at discharge. [11]
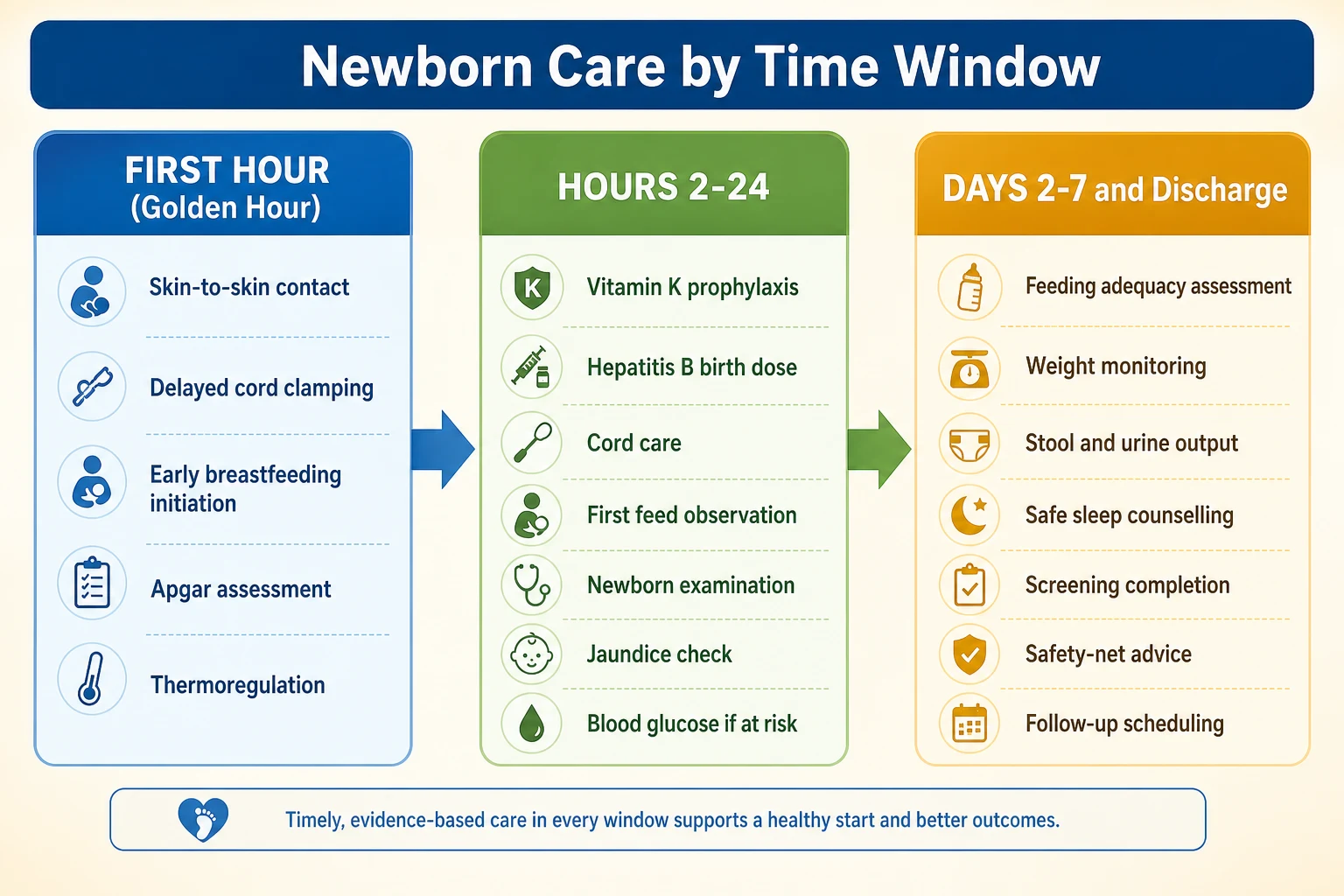
The framework most services use is the golden hour leading into time-based care phases. The first hour is for skin-to-skin, warmth, delayed cord clamping, and early breastfeeding. Hours 2 to 24 are for the newborn examination, vitamin K, hepatitis B vaccine, cord care, feeding observation, and risk-tailored monitoring. Days 2 to 7 are for confirming feeding adequacy, weight trajectory, jaundice safety, safe sleep counselling, and discharge readiness. [9] [14]
Classification
Think about the healthy newborn's care in time windows, because the risks and the tasks change at each stage. What you worry about in the first hour (warmth, transition, cord clamping) is different from what you worry about at 48 hours (feeding adequacy, weight loss, jaundice). [9] [19]
The golden hour is the first 60 minutes after birth. Its evidence-based elements are immediate and sustained skin-to-skin contact on the maternal chest, delayed cord clamping when the newborn is vigorous, early initiation of breastfeeding within the first hour, and attention to thermoregulation by keeping the baby warm, dry, and covered. This period also includes the Apgar assessment at 1 and 5 minutes, though Apgar is a transition score, not a care plan. [9] [11]
The newborn's status can also be classified by feeding pathway (exclusive breastfeeding, expressed breast milk, formula supplementation, or mixed feeding) and by risk category for complications. The AAP defines specific at-risk groups for hypoglycaemia screening: infants of diabetic mothers, late-preterm infants, large-for-gestational-age and small-for-gestational-age infants, and those with perinatal stress such as asphyxia, hypothermia or sepsis. These categories change how aggressively you monitor glucose and feeding. [1] [2]
Golden Hour
0 to 60 min
- Skin-to-skin contact
- Delayed cord clamping if vigorous
- Early breastfeeding initiation
- Thermoregulation
- Apgar assessment
First Day
1 to 24 hours
- Vitamin K prophylaxis
- Hepatitis B birth dose
- Complete newborn examination
- Cord and skin care
- Glucose check if at risk
- Jaundice risk assessment
Discharge Phase
Days 2 to 7
- Feeding adequacy confirmed
- Weight loss within limits
- Jaundice safe or treated
- Safe sleep counselled
- Follow-up booked 48 to 72 h
- Safety-net understood
Epidemiology & Risk Factors
Most newborns are healthy and adapt without intervention. That is precisely why the minority who do not are dangerous — the well-looking majority creates a false sense of security. The risk factors that change routine care cluster into infant, maternal and social categories. [19] [21]
Late-preterm infants (34 to 36+6 weeks gestation) are the highest-volume at-risk group on a postnatal ward. They have less subcutaneous fat, less glycogen reserve, immature feeding coordination, slower gut maturation and a higher risk of both hypoglycaemia and significant hyperbilirubinemia. They are not candidates for very early discharge and need closer monitoring than their "almost term" appearance suggests. [1] [2]
Infants of diabetic mothers carry double risk: hypoglycaemia from fetal hyperinsulinaemia and feeding difficulty from macrosomia or prematurity. Other infant risk factors for hypoglycaemia include being large or small for gestational age, and perinatal stress from birth asphyxia, hypothermia or sepsis. These are the groups where proactive glucose screening and feeding support pay off. [1]
Maternal factors that change the plan include diabetes (pre-existing or gestational), medications affecting lactation or neonatal adaptation, hepatitis B surface antigen positivity (which triggers HBIG plus vaccine), and mode of delivery. Caesarean delivery can delay breastfeeding initiation and complicate rooming-in. [17] [18]
Social factors are not soft risk factors — they are the most common reason a newborn is lost to follow-up. Language barriers, first-time parenthood, mental health concerns, housing instability, transport difficulties and prior negative healthcare experiences all predict failed early follow-up. The plan must match the family's actual capacity to return, not the service's default assumption. [19]
Pathophysiology
The healthy newborn is executing three simultaneous transitions: circulatory, metabolic and thermoregulatory. Understanding these transitions explains why each element of routine care exists. [9] [1]
At birth, the ductus arteriosus begins to close and pulmonary vascular resistance falls as the lungs fill with air. In a healthy newborn this proceeds smoothly. The risk is that some infants with duct-dependent congenital heart disease appear pink and well while the ductus is still open, then collapse as it constricts over hours to days. This is why timing matters — a baby who looks perfect at 6 hours may be different at 30 hours. Routine care includes the structured newborn examination and, in many services, CCHD pulse oximetry screening after the transitional period to catch this window. [9]
Metabolically, the newborn must maintain its own glucose for the first time. The placental supply is cut at birth. Glycogen stores are the bridge, but they are limited, and at-risk infants (preterm, diabetic mother, growth-restricted) deplete them faster. When glucose falls below the operational threshold, the brain is at risk. The AAP clinical report on postnatal glucose homeostasis frames this as a screening-and-feeding problem, not an isolated number problem: treat the infant, not the laboratory value. [1] [2]
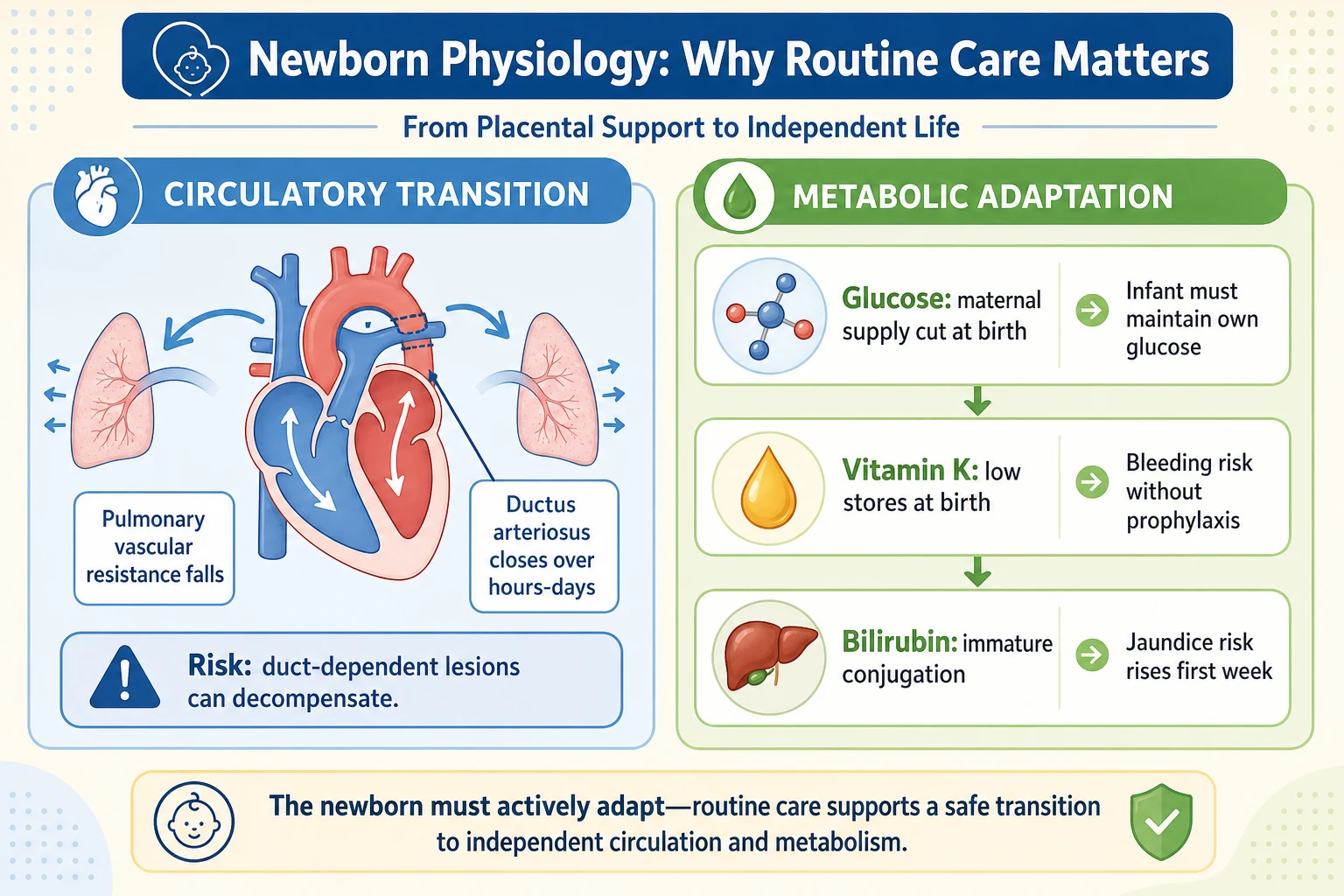
Vitamin K is essential for activation of clotting factors II, VII, IX and X. Newborn stores are low because vitamin K does not cross the placenta well and the gut is not yet colonised by vitamin K-synthesising bacteria. Without prophylaxis, bleeding can present early (first 24 hours, usually in infants of mothers on enzyme-inducing drugs), classically (days 2 to 7), or late (weeks to months, often intracranial and catastrophic). Late VKDB is the preventable disaster that prophylaxis exists to stop. [6] [7] [8]
Bilirubin handling is immature at birth. The liver's glucuronyl transferase activity is low, red cell turnover is high, and gut reabsorption of bilirubin (enterohepatic circulation) is increased before feeding is established. These factors produce physiological jaundice peaking around days 3 to 5. When risk factors push bilirubin above the brain's protective threshold, unconjugated bilirubin crosses into the basal ganglia, causing acute bilirubin encephalopathy and, if untreated, kernicterus. [3]
Thermoregulation is the final transition. Newborns have a large surface-area-to-mass ratio, thin skin, limited subcutaneous fat and cannot shiver effectively. Heat loss occurs through evaporation (wet skin at birth), radiation, convection and conduction. Cold stress raises metabolic demand, consumes glucose and worsens acidosis. Skin-to-skin contact, drying, warm towels and a hat are not mere comfort — they are metabolic protection. [9]
Clinical Presentation
The healthy term newborn on a postnatal ward looks alert, pink, maintains temperature in a warm wrap, and feeds when offered. Normal behaviour in the first 24 hours includes periods of quiet alertness interspersed with deep sleep. Stools transition from black meconium on day 1 to greenish-transitional by day 2 to 3, then yellow seedy once feeding is established. Urine output should be at least one wet nappy on day 1, increasing daily thereafter. [19]
The warning signs that a "routine" newborn is drifting toward pathology are subtle but consistent. Poor feeding — the inability to latch, sustain a suck, or produce audible swallows — is the single most important sentinel sign. It is never normal for a term newborn to refuse every feed for more than a few hours. [19] [20]
Temperature instability (axillary temperature below 36.0 C or above 37.5 C) is never "just cold" in a newborn. Hypothermia may signal sepsis, metabolic disease or environmental failure, and it worsens hypoglycaemia. Lethargy, hypotonia, irritability or a high-pitched cry all warrant senior review. [1]
Jaundice is visible when serum bilirubin exceeds approximately 5 mg/dL (85 micromol/L), usually first in the face and progressing cephalocaudally. Visible jaundice in the first 24 hours is pathological until proven otherwise — it implies haemolysis, infection or a metabolic process. Jaundice appearing after 24 hours is more likely physiological, but still needs hour-specific risk assessment. [3]
Weight loss is expected but bounded. Term newborns typically lose 5 to 7 percent of birth weight in the first few days, regaining it by 10 to 14 days. Loss exceeding 10 percent, or failure to feed adequately with falling output, requires assessment for dehydration and hypernatraemia. The degree of weight loss correlates with hypernatraemic dehydration when feeding intake is insufficient. [20] [19]
Differential Diagnosis
When a routine newborn shows a warning sign, the differential is broad because the baby cannot localise. The job is not to diagnose the exact cause at the bedside, but to recognise that the newborn has left the "healthy" category and escalate. [1] [19]
For poor feeding, the differential ranges from normal learning (common, resolves with lactation support) to sepsis, hypoglycaemia, congenital heart disease, metabolic disease, neurological abnormality, or a structural problem like cleft palate or tongue-tie. The discriminating question is whether feeding improves with support and whether other signs are present. [20]
For jaundice, the first 24 hours demands investigation for haemolysis (ABO or Rh incompatibility, G6PD deficiency), congenital infection, or sepsis. After 24 hours, physiological jaundice and breast-milk jaundice are more likely, but haemolysis and infection remain on the differential until risk assessment and measurement clarify. Conjugated hyperbilirubinemia (direct fraction elevated) is a different pathway — it suggests biliary obstruction or cholestasis and needs urgent investigation. [3]
For hypothermia, consider environmental exposure, sepsis, metabolic disease (especially fatty acid oxidation disorders), hypoglycaemia, or a cardiac cause with poor perfusion. Hypothermia in a warmed environment is a red flag, not a nuisance. [1]
For excessive weight loss, the differential is inadequate intake (most common), insufficient maternal milk supply, latch problems, or an underlying disease causing increased losses or poor absorption. Serum sodium above 150 mmol/L confirms hypernatraemic dehydration, which can cause cerebral venous thrombosis and seizures. [20]
When a parent declines vitamin K or any element of routine care, the differential of refusal includes genuine values-based choice, misinformation from unreliable sources, fear from previous healthcare experiences, access barriers, and, rarely, safeguarding concern if critical care is being systematically avoided. Start with respectful curiosity, not confrontation. [6] [8]
Clinical & Bedside Assessment
Start with the history that changes the plan. Gestation and birth weight place the infant in a risk category. Maternal diabetes, medications, blood group status, hepatitis B surface antigen, GBS status, and membrane rupture duration all change monitoring. Feeding intention, previous breastfeeding experience, social situation, transport to follow-up, and who will be at home all shape the discharge plan. [19] [17]
The routine newborn examination is systematic and covers every system. Examine in a warm, well-lit room with the baby settled. Check the red reflex in a dim corner — an absent or white reflex needs urgent ophthalmology referral. Listen to the heart in a quiet infant; a murmur in the first 24 hours may be flow-related and innocent, but absent femoral pulses are not — check them in every newborn. Examine the hips with Ortolani and Barlow if trained. Palpate the abdomen for organomegaly and masses. Inspect the spine and sacral region for dimples, hair tufts or sinus tracts. Examine the genitalia and check patency of the anus. Assess tone, alertness, the Moro reflex and symmetry of movement. [19]
Feeding assessment is the single most important bedside skill. Observe a full breastfeed: positioning, attachment (latch), audible swallowing, maternal comfort, and infant satiety cues afterward. A baby who sleeps through feeds, pops off repeatedly, or never produces a sustained rhythmic suck is not "settled" — they are not transferring milk. Document the assessment and act on it. [11]
Assess hydration and weight before discharge. Measure weight at birth and again at 24 to 48 hours. Calculate percentage weight loss. Check fontanelle (soft and flat, not sunken), mucous membranes, capillary refill and skin turgor. If weight loss exceeds 7 percent, increase feeding support and plan a repeat weight. If it exceeds 10 percent, assess serum sodium and consider medical review. [20] [19]
Temperature should be measured with an axillary thermometer. A reading below 36.0 C is hypothermia and needs active warming and reassessment. Do not discharge a hypothermic newborn. [9]
Jaundice is assessed visually first, but visual estimation is unreliable and influenced by skin tone and lighting. Any visible jaundice in the first 24 hours needs a serum or transcutaneous bilirubin measurement. After 24 hours, use a predischarge bilirubin with hour-specific risk assessment per the 2022 AAP guideline or your national equivalent. [3]
Investigations
Routine care of a genuinely healthy newborn requires remarkably few investigations. The newborn bloodspot screen, hearing screen and CCHD pulse oximetry screen are programmes, not acute tests, and have their own dedicated topic. Targeted investigations in routine care are risk-driven. [1] [19]
Blood glucose screening is indicated for at-risk infants as defined by the AAP clinical report: infants of diabetic mothers, late-preterm infants, large or small for gestational age, and those with perinatal stress. The operational threshold for intervention varies by gestation, age, and feeding status — follow the current AAP algorithm rather than a memorised single number. The approach is to screen, feed, recheck, and escalate to IV glucose only if the infant fails to maintain glucose after feeding. [1] [2]
Bilirubin measurement uses transcutaneous devices for screening and serum levels for confirmation near or above treatment thresholds. Interpret the result against postnatal age in hours, gestation, and neurotoxicity risk factors using the current AAP nomogram, not a single universal cut-off. The 2022 AAP guideline revised thresholds upward for infants 35 weeks or more — use the current implementation, not an older chart. [3]
For excessive weight loss or suspected dehydration, check serum sodium, creatinine and urea. A sodium above 150 mmol/L confirms hypernatraemic dehydration and mandates medical review, supervised refeeding, and monitoring for cerebral complications. [20]
Maternal hepatitis B surface antigen status must be known before discharge. If positive, the newborn needs hepatitis B vaccine plus HBIG within 12 hours of birth. If unknown and the mother is high-risk, administer vaccine and test the mother urgently. [17] [18]
Hip ultrasound is arranged selectively when examination is abnormal (positive Ortolani or Barlow) or risk factors are present (breech presentation, family history), following local DDH pathways. [19]
Management — Resuscitation
The healthy newborn does not need resuscitation — that is what "healthy" means. But routine care and resuscitation share a boundary: the newborn who looks well at birth and then decompensates. If a routine newborn develops respiratory distress, central cyanosis, hypothermia that does not correct with warming, hypoglycaemia that does not correct with feeding, or signs of sepsis, they have left routine care. [1] [9]
Immediate steps are universal. Call for senior and neonatal help. Support airway and breathing with positioning and oxygen guided by saturation monitoring. Check glucose. Establish access. Treat hypothermia actively with a radiant warmer. If sepsis is suspected, obtain cultures and start broad-spectrum antibiotics per local neonatal protocols — do not wait for confirmation in a deteriorating neonate. [1]
For hypoglycaemia that does not respond to feeding, the escalation is buccal 40 percent dextrose gel (200 mg/kg) combined with a feed and recheck, then IV 10 percent dextrose if the infant remains below threshold. The exact glucose concentration and rate should follow your local neonatal guideline — state that you would use the current protocol rather than improvising. [1] [2]
For suspected vitamin K deficiency bleeding, give parenteral vitamin K urgently, support with blood products as indicated, and investigate for intracranial bleeding when neurological signs are present. Prevention through prophylaxis is far better than rescue. [6] [8]
A newborn who becomes jaundiced in the first 24 hours needs urgent investigation for haemolysis and infection, not simply phototherapy. The bilirubin level must be interpreted hour-by-hour. [3]
Management — Definitive & Stepwise
The golden hour
Place the newborn skin-to-skin on the maternal chest immediately after birth, dry, cover with a warm blanket and hat. Delay cord clamping for at least 60 seconds (often 1 to 3 minutes) in the vigorous term newborn, as the Cochrane review confirms improved iron stores through 6 months without significant maternal harm. Encourage breastfeeding initiation within the first hour when mother and baby are ready. [9] [10]
Vitamin K prophylaxis
Give a single intramuscular dose of vitamin K to every newborn unless parents decline, as this is the most reliable route for preventing all forms of vitamin K deficiency bleeding including late VKDB. If parents decline IM injection after counselling, an oral regimen can be offered where locally available, but it requires complete multi-dose adherence and still leaves residual risk, especially with malabsorption. Document the discussion, the decision and the follow-up plan. [6] [7]
Hepatitis B birth dose
Administer hepatitis B vaccine within 24 hours of birth to all newborns per ACIP recommendations. For infants of hepatitis B surface antigen-positive mothers, give both vaccine and HBIG within 12 hours of birth. For mothers whose status is unknown, give vaccine within 12 hours and test the mother urgently. [17] [18]
Cord and skin care
Dry cord care (keeping the cord clean and dry without antiseptic application) is the AAP-recommended approach in high-resource settings with low infection rates. In settings with higher infection risk, chlorhexidine application to the cord may reduce omphalitis and neonatal mortality. Avoid routine bathing in the first 24 hours; the first bath is often delayed to 24 hours or more to preserve vernix and support thermoregulation. [12] [13] [14] [15]
Feeding support pathway
Initiate early
Skin-to-skin and first breastfeed within the golden hour
Observe and document
Assess latch, swallow and satiety at least once per shift
Support demand feeding
Rooming-in, feeding on cues, no scheduled intervals in the first days
Troubleshoot early
Lactation support within 24 hours if latch or transfer is inadequate
Confirm before discharge
At least 6 to 8 feeds in 24 hours, audible swallowing, settled baby, adequate output
Ophthalmia neonatorum prophylaxis
Eye prophylaxis against gonococcal ophthalmia neonatorum (erythromycin or other agent per local policy) is required in some jurisdictions (notably the US and Canada) but has been discontinued in others (such as the UK and Australia) where the evidence no longer supports routine universal application. Know the policy where you practise. [16]
Jaundice monitoring
Use a predischarge bilirubin strategy with hour-specific risk assessment for all newborns, as recommended by the 2022 AAP guideline for infants 35 weeks or more. Measure bilirubin before discharge, plot it on the hour-specific risk nomogram, and give a follow-up plan matched to risk category. High-risk infants need earlier and more intensive follow-up. [3]
Safe sleep counselling
Counsel every family before discharge on safe sleep: the baby sleeps alone, on the back, in a separate sleep surface (crib or bassinet) near the parents' bed. Use a firm flat surface with no soft objects, loose bedding, pillows or bumpers. Room-sharing without bed-sharing is recommended for at least the first 6 months. Avoid overheating, smoke exposure and alcohol or sedative use by caregivers. These are the 2022 AAP recommendations, and they are the single most evidence-based intervention to reduce sleep-related infant death. [4] [5]
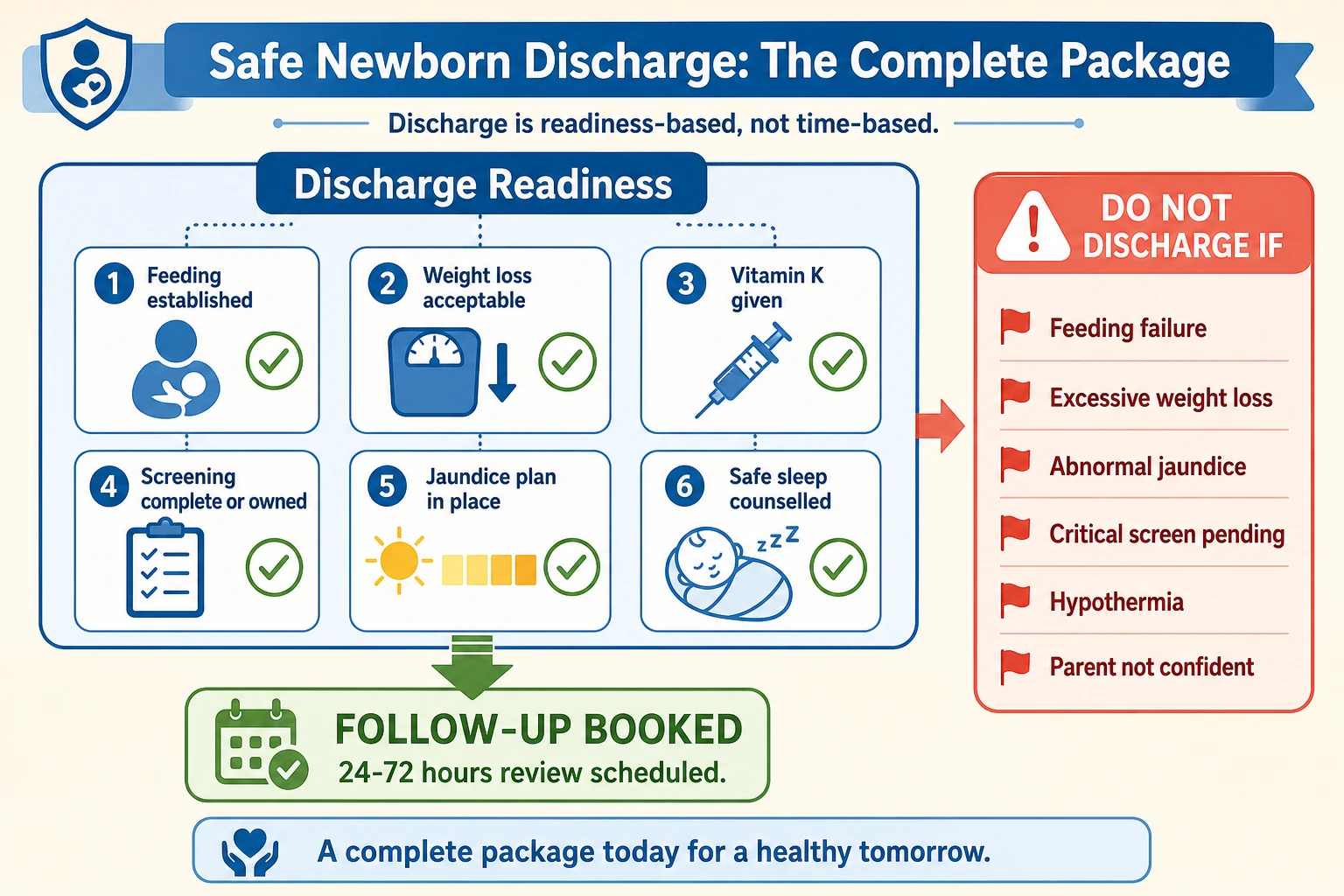
Discharge readiness
Confirm all of the following before discharge: feeding is established with adequate output, weight loss is within acceptable limits (typically under 10 percent), jaundice risk is assessed and a plan is in place, vitamin K has been given or a documented refusal pathway exists, the newborn examination is complete, safety-net advice is understood (teach-back), and follow-up is booked within 48 to 72 hours for higher-risk infants. [19] [21]
Specific Subtypes & Scenarios
Late-preterm infant (34 to 36+6 weeks). These infants look almost term but are not. They carry higher risk of hypoglycaemia, feeding difficulty, jaundice, temperature instability and readmission. Monitor glucose if at risk, assess feeding more intensively, do not discharge before feeding is clearly established, and arrange closer follow-up. They are not candidates for very early discharge. [1] [19]
Infant of a diabetic mother. Proactively screen glucose, expect hyperinsulinaemic hypoglycaemia that may be prolonged, assess for macrosomia-related complications (shoulder dystocia sequelae, clavicle fracture, brachial plexus injury, respiratory distress), and monitor feeding closely. [1] [2]
Early discharge (before 48 hours). Early discharge compresses the observation window and shifts risk to the community. It is acceptable only when all discharge criteria are met, a predischarge bilirubin risk assessment is done, feeding is established, and follow-up within 48 to 72 hours is confirmed. A vague instruction to "see the GP" is not follow-up. [19] [21]
Caesarean delivery. Maternal recovery and pain can delay breastfeeding initiation and complicate rooming-in. Support early skin-to-skin even in theatre where feasible. Delayed cord clamping is still possible and beneficial. Plan feeding support around maternal recovery. [9]
Home birth or delayed presentation. Treat the first clinical contact as the start of the routine care clock. Do not assume any element was completed. Verify vitamin K, feeding status, examination, and arrange screening. [19]
Parental decline of vitamin K. Explore the reasons with respect, correct specific misconceptions, offer the IM route as the evidence-based standard, present the oral alternative honestly (it requires full adherence and still carries residual risk), document the discussion, and ensure the infant is not lost to follow-up. Escalation to safeguarding is for clear risk of significant harm, not for every values-based refusal. [6] [8]
Complications & Pitfalls
The most common and dangerous complication of routine newborn care is the failure to detect a problem that was brewing silently. Hypernatraemic dehydration from missed feeding failure is preventable with attentive feeding assessment and weight monitoring — but it still happens and can cause seizures and cerebral venous thrombosis when sodium exceeds 150 mmol/L. [20]
Late vitamin K deficiency bleeding in infants whose parents declined prophylaxis is the most devastating preventable outcome. It typically presents as intracranial haemorrhage at 2 to 12 weeks with seizures, vomiting, bulging fontanelle and high mortality or neurodisability. A single IM dose prevents almost all cases. [7] [8]
The discharge-before-readiness trap is the classic exam scenario. A newborn is sent home because they "look well" and feeding "seemed OK", without confirming weight trajectory, bilirubin risk, or follow-up. Readmission within 48 hours for dehydration, sepsis or congenital heart disease follows. The defence is a checklist mindset, not a time-based one. [19] [21]
Over-investigating normal physiology is the opposite pitfall. Mild jaundice on day 3, weight loss of 5 to 7 percent, and variable feeding in the first 24 hours are normal. Treating every variation as pathology creates parental anxiety, unnecessary blood tests and prolonged admissions. Risk-stratify rather than test reflexively. [3]
Inadequate safe sleep counselling is a pitfall with delayed consequences. A family sent home without clear advice on back-sleeping, firm surfaces and no bed-sharing may place the baby at risk of sudden unexpected death in infancy in the weeks and months ahead. Counsel every family before discharge. [4] [5]
Prognosis & Disposition
A well term newborn who receives the complete routine care package and meets all discharge criteria has an excellent prognosis. Weight is typically regained by 10 to 14 days. Exclusive breastfeeding at discharge is strongly predicted by early and effective lactation support. The 2022 AAP safe sleep guidance, when followed, reduces sleep-related infant death risk. [4] [11]
Disposition from the postnatal ward is home, not an observation unit. The criteria are feeding established, weight within limits, jaundice safe, screening complete or owned, and follow-up booked. For infants at higher risk (late-preterm, diabetic mother, significant weight loss, early discharge), follow-up should be within 48 to 72 hours by a clinician who can assess feeding, weight, jaundice and parental confidence — not simply a "check-up". [19] [21]
Readmission rates after early discharge vary but are typically 5 to 10 percent in the first 2 weeks, most commonly for jaundice, feeding problems and suspected sepsis. Structured follow-up programmes reduce readmission by catching problems before they become emergencies. [21]
Special Populations
Late-preterm infants need the most adapted routine care: more intensive feeding support, glucose screening, temperature monitoring, and jaundice surveillance. They should not be treated as "almost term." [1]
Indigenous, rural and remote families need discharge plans that match real travel times, not urban default assumptions. For Aboriginal, Torres Strait Islander, Maori and Pacific families, culturally safe communication, family involvement and realistic follow-up pathways are essential. A 48-hour review is meaningless if the nearest clinic is 4 hours away and transport is uncertain. [19]
Migrant, refugee and asylum-seeking families may need interpreter-supported education, lack of continuity in antenatal records, and assistance navigating the healthcare system. Hepatitis B status may be unknown; test and vaccinate accordingly. [17]
Families with social complexity — housing instability, mental health concerns, first-time parenthood with limited support, or safeguarding concerns — need more intensive follow-up and a safety-net that does not rely on the family self-advocating. Plan follow-up based on what the family can actually access. [19]
Multiple-birth newborns (twins, triplets) are often delivered earlier, smaller, and by caesarean. Feeding support is more complex (two babies, one mother, possible supplementation), and follow-up needs to track each infant individually. [11]
Evidence, Guidelines & Regional Differences
The Cochrane review by McDonald and colleagues established that delayed cord clamping (at least 60 seconds) in term infants improves iron stores through 6 months without significant maternal harm, though it slightly increases the need for phototherapy for jaundice. Meta-analysis confirms the haematological benefit. This evidence underpins current guidelines recommending delayed clamping for vigorous newborns. [9] [10]
Vitamin K prophylaxis evidence consistently favours intramuscular administration as the most reliable route for preventing all forms of VKDB, including late disease. Oral regimens reduce but do not eliminate risk, and require complete adherence. Narrative reviews continue to support IM as the standard. [6] [7]
The revised Baby-Friendly Hospital Initiative (2018) updated the Ten Steps to Successful Breastfeeding, integrating them into a broader framework of maternal and newborn care, and expanding beyond the facility to community support. The evidence for early skin-to-skin, rooming-in and demand feeding remains strong for healthy term newborns. [11]
The 2022 AAP hyperbilirubinemia guideline revised thresholds for infants 35 weeks or more, moving away from a single exchange transfusion line toward a risk-stratified, hour-specific approach. The 2022 AAP safe sleep recommendations reaffirm back-sleeping, firm flat surfaces, room-sharing without bed-sharing, and avoidance of soft objects and overheating. [3] [4] [5]
Australia and Aotearoa New Zealand follow national postnatal care guidelines with state-based variations. Vitamin K IM prophylaxis is standard. Hepatitis B birth dose is universal. Routine eye prophylaxis is not practiced. Dry cord care is standard. Culturally safe follow-up for Aboriginal, Torres Strait Islander, Maori and Pacific families includes realistic geography and whanau participation. [9] [6]
United Kingdom follows NICE postnatal care guidance (NG194) and the NIPE examination. Vitamin K is offered to all parents. Hepatitis B vaccine is given at birth only to at-risk infants, not universally. Ophthalmia neonatorum prophylaxis is not practiced. Newborn blood spot, hearing and physical examination screening are delivered through national programmes. [12] [17]
United States follows AAP guidelines for hyperbilirubinemia, safe sleep and hypoglycaemia. Hepatitis B birth dose is universal per ACIP. Ophthalmia neonatorum prophylaxis with erythromycin is still required in most states. Cord care is dry care. Discharge timing and follow-up intensity vary by state and insurance. [3] [4] [17]
Canada follows Canadian Paediatric Society guidance. Hepatitis B birth dose strategy varies by province. Ophthalmia neonatorum prophylaxis policy has shifted away from universal use in several provinces. Discharge and follow-up are provincially organised. [16]
WHO and low-resource settings emphasise essential newborn care: warmth, cleanliness, breastfeeding and cord care. Chlorhexidine for cord care is recommended in high-mortality settings. Skin-to-skin and breastfeeding support are universal priorities. [13]
Exam Pearls
- A well newborn can become unwell within hours. "Looks fine" is not a discharge criterion. [19]
- Late-preterm infants are not term. They need more monitoring and are not candidates for very early discharge. [1]
- First-24-hour jaundice is never physiological. Investigate for haemolysis and infection. [3]
- Vitamin K refusal → late VKDB → intracranial haemorrhage. IM is the standard; document any refusal. [6] [8]
- Weight loss above 10 percent needs sodium check and medical review, not just "more feeding". [20]
- Safe sleep: alone, on back, firm flat surface, room-share, no soft objects. [4]
- Discharge without confirmed follow-up within 48 to 72 hours is unsafe for higher-risk infants. [21]
- Delayed cord clamping improves iron stores through 6 months. Give it to every vigorous newborn. [9]
- A baby who does not feed is not "settled" — they are not transferring milk. [11]
- Dose-like statements in a viva: state you would use the current national protocol, not a memorised number. [1]
SAFE-HAND
References
- [1]Adamkin DH; Committee on Fetus and Newborn Postnatal glucose homeostasis in late-preterm and term infants. Pediatrics, 2011.PMID 21357346
- [2]Adamkin DH Metabolic screening and postnatal glucose homeostasis in the newborn. Pediatric Clinics of North America, 2015.PMID 25836704
- [3]Kemper AR, Newman TB, Slaughter JL, et al. Clinical Practice Guideline Revision: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation. Pediatrics, 2022.PMID 35927462
- [4]Moon RY, Carlin RF, Hand I, et al.; Task Force on Sudden Infant Death Syndrome and the Committee on Fetus and Newborn Sleep-Related Infant Deaths: Updated 2022 Recommendations for Reducing Infant Deaths in the Sleep Environment. Pediatrics, 2022.PMID 35726558
- [5]Moon RY, Carlin RF, Hand I, et al. Evidence Base for 2022 Updated Recommendations for a Safe Infant Sleeping Environment to Reduce the Risk of Sleep-Related Infant Deaths. Pediatrics, 2022.PMID 35921639
- [6]Mirone A, Mannino D, et al. Vitamin K Prophylaxis in Newborns: A Narrative Review of the Molecular Basis, Clinical Evidence, and Comparative Effectiveness of Intramuscular Versus Oral Administration and Parental Hesitation. International Journal of Molecular Sciences, 2026.PMID 41751806
- [7]Perrone S, Beretta V, Raitano V, et al. Vitamin K Biochemistry and Pharmacokinetics: The Basis of Late Vitamin K Deficiency Intracranial Bleeding in Early Infancy. International Journal of Molecular Sciences, 2026.PMID 42123580
- [8]Dogan M, Varol R, et al. Late-Onset Vitamin K Deficiency Bleeding in Four Infants: A Forensic Pathology Case Series With Clinical-Autopsy Correlation. Academic Forensic Pathology, 2026.PMID 42311238
- [9]McDonald SJ, Middleton P, Dowswell T, Morris PS Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database of Systematic Reviews, 2013.PMID 23843134
- [10]Gomersall J, Berber S, et al. Umbilical Cord Management at Term and Late Preterm Birth: A Meta-analysis. Pediatrics, 2021.PMID 33632933
- [11]Aryeetey R, Dykes F Global implications of the new WHO and UNICEF implementation guidance on the revised Baby-Friendly Hospital Initiative. Maternal and Child Nutrition, 2018.PMID 29952432
- [12]Stewart D, Benitz W, et al.; Committee on Fetus and Newborn Umbilical Cord Care in the Newborn Infant. Pediatrics, 2016.PMID 27573092
- [13]Coffey PS, Brown SC Umbilical cord-care practices in low- and middle-income countries: a systematic review. BMC Pregnancy and Childbirth, 2017.PMID 28219420
- [14]Dyer JA Newborn skin care. Seminars in Perinatology, 2013.PMID 23419756
- [15]Priyadarshi M, Balachander B, et al. Timing of first bath in term healthy newborns: A systematic review. Journal of Global Health, 2022.PMID 35972992
- [16]Moore DL, MacDonald NE; Canadian Paediatric Society, Infectious Diseases and Immunization Committee Preventing ophthalmia neonatorum. Paediatrics and Child Health, 2015.PMID 25838784
- [17]Schillie S, Vellozzi C, Reingold A, et al. Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recommendations and Reports, 2018.PMID 29939980
- [18]Liu JF, Chen TY, Mao RC Vertical transmission of hepatitis B virus: propositions and future directions. Chinese Medical Journal, 2021.PMID 34636774
- [19]Lindblad V, Gaardsted PS, et al. Early discharge of first-time parents and their newborn: A scoping review. European Journal of Midwifery, 2021.PMID 34708193
- [20]Goff DA, Higinio V Hypernatremia. Pediatrics in Review, 2009.PMID 19797486
- [21]De Carolis MP, Cocca C, et al. Individualized follow up programme and early discharge in term neonates. Italian Journal of Pediatrics, 2014.PMID 25024007