Paeds · fetal-neonatal-and-perinatal
Transient tachypnoea of the newborn
Also known as wet lung syndrome · type II respiratory distress syndrome · retained fetal lung fluid
Self-limiting neonatal respiratory distress caused by delayed clearance of fetal lung fluid, most common in term and late-preterm infants delivered by elective caesarean without labour.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A well, term or late-preterm baby who is grunting and breathing fast in the first few hours of life is the classic presentation that turns out to be transient tachypnoea of the newborn (TTN). The problem is delayed clearance of the fluid that normally fills the fetal alveoli, so the lungs behave as if they are still partly "wet" until absorption catches up over the first day or two. [2]
TTN is also called "wet lung syndrome" or type II respiratory distress, and it is the single most common cause of respiratory distress in term and late-preterm infants. The reassuring feature is the course: symptoms peak within the first day and almost always resolve within 72 hours without surfactant or invasive ventilation, provided oxygen needs stay modest and an alternative diagnosis has been excluded. [1]
Epidemiology & Risk Factors
TTN affects roughly 5 to 6 per 1000 term infants, and the incidence rises sharply when babies are born before labour has done its work. Anything that removes the catecholamine surge of labour or the mechanical squeeze of the birth canal tilts the balance toward retained fluid, which is why elective caesarean before the onset of labour is the dominant risk factor. [3]
Other recognised contributors are male sex, being large or hypoglycaemic from a diabetic pregnancy, precipitous delivery, and assisted or breech delivery where the thoracic squeeze is abnormal. The mode of anaesthesia also matters: cohort data show that the obstetric anaesthetic technique used at caesarean section influences neonatal respiratory morbidity, reinforcing how heavily the condition depends on the circumstances of delivery. [10]
Pathophysiology
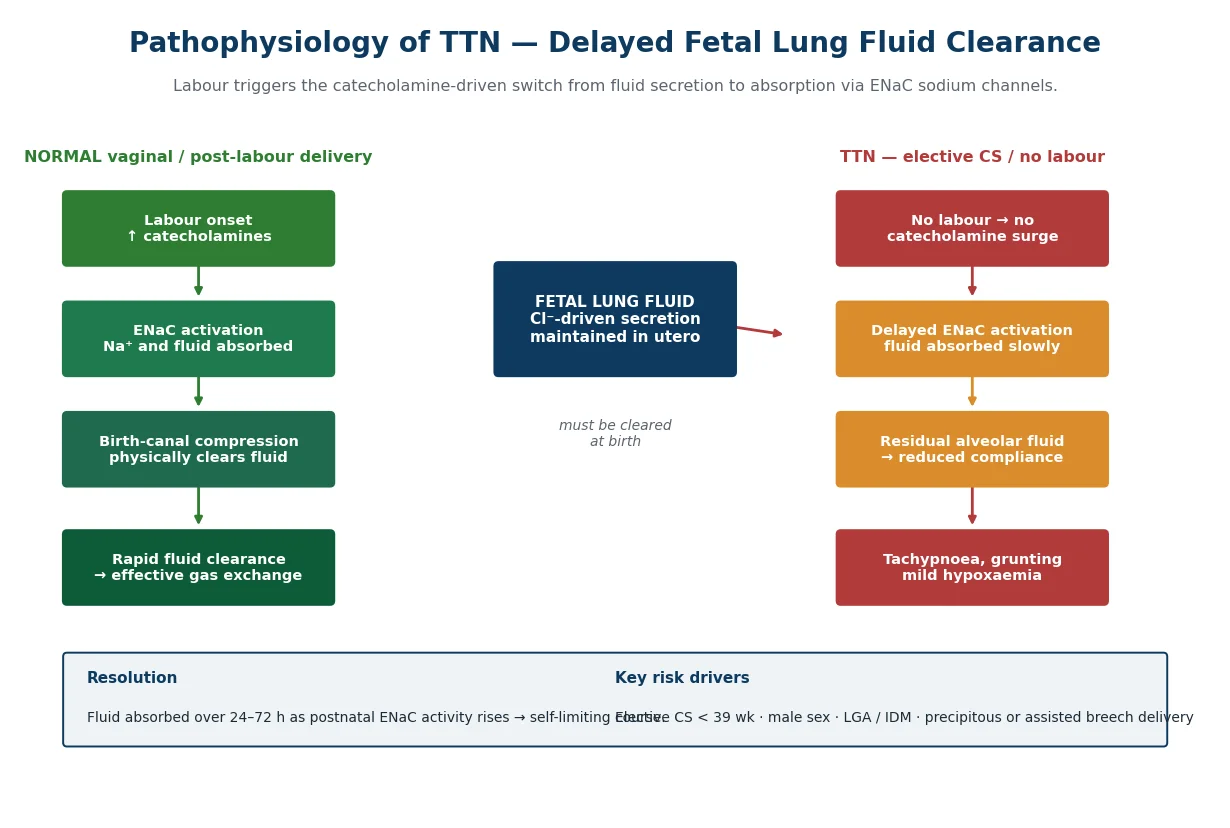
Throughout gestation the fetal lung actively secretes chloride-driven fluid to keep the airways expanded and growth stimulated. At birth this fluid must be cleared, and clearance is driven by activation of amiloride-sensitive epithelial sodium channels (ENaC) on the alveolar epithelium, which pull sodium — and water with it — out of the lumen and into the interstitium for lymphatic and venous removal. Labour is the master switch: the catecholamine surge at delivery upregulates ENaC, converting secretion to absorption. [2]
When a baby is delivered by elective caesarean without labour, that catecholamine signal is blunted and the mechanical "squeeze" of the birth canal is lost, so ENaC activation is delayed and residual alveolar fluid persists. Animal work confirms the mechanism, showing that beta-agonists acting on epithelial sodium channels can accelerate fluid clearance in injured neonatal lungs. The result is reduced lung compliance, splinting with tachypnoea and grunting, and mild hypoxaemia that corrects as postnatal ENaC activity climbs. [9]
Classification
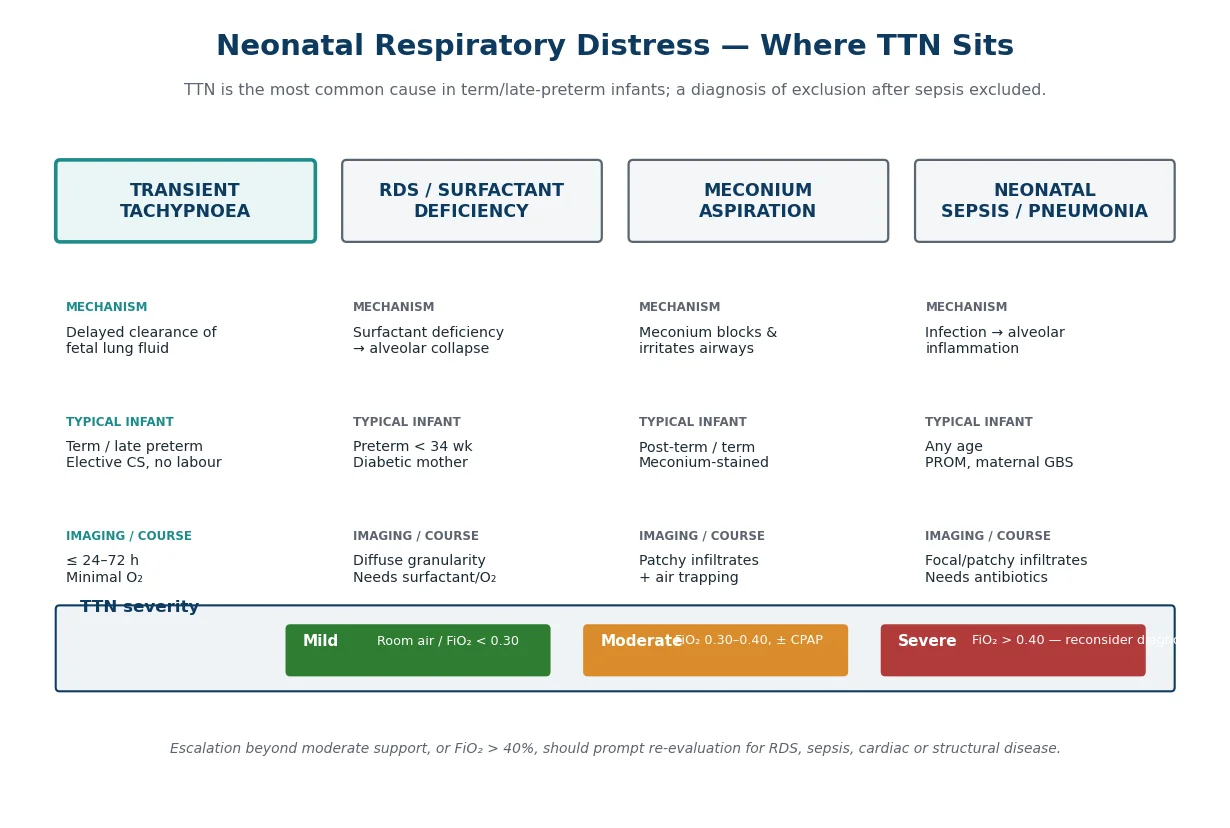
TTN is best classified by how much support the baby needs, because oxygen requirement is the practical gauge of severity and the trigger to reconsider the diagnosis. Mild disease is managed in room air or with low-flow oxygen below an FiO₂ of 0.30; moderate disease needs between 0.30 and 0.40 and may warrant bubble CPAP; severe disease — anything above 0.40 — should prompt re-evaluation. [1]
The other useful axis is the differential, since TTN sits among four overlapping causes of neonatal respiratory distress. It is worth holding the four patterns side by side so that a baby labelled "TTN" does not turn out to have surfactant deficiency, meconium aspiration, or neonatal sepsis that needs antibiotics. [1]
Clinical Presentation
The hallmark is tachypnoea beginning within the first six hours of life, with a respiratory rate that crosses 60 breaths per minute and often sits between 80 and 100. Affected babies show the work-of-breathing triad of expiratory grunting (to maintain alveolar recruitment), nasal flaring, and mild to moderate subcostal and intercostal recession. [3]
Most infants are systemically well: they are pink in the right amount of oxygen, feed intermittently, and have a normal cardiovascular examination. Cyanosis is uncommon at presentation and should raise suspicion of an alternative or more serious cause. Because the distress is driven by fluid rather than infection or structural disease, the baby generally looks much better than the respiratory rate alone would suggest. [3]
TTN at a glance — the THREE F's
Differential Diagnosis
The diagnosis of TTN is one of exclusion, and the dangerous mistake is anchoring on a benign label while a treatable cause worsens. Respiratory distress syndrome from surfactant deficiency is the chief mimic in any premature or diabetic-mother infant, presenting with worsening distress and a ground-glass chest radiograph rather than fluid in the fissures. [1]
Meconium aspiration, transient pulmonary hypertension, congenital heart disease (especially duct-dependent lesions), congenital diaphragmatic hernia, and neonatal sepsis or pneumonia must each be considered and actively excluded. A pre-post-ductal oxygen saturation difference, abnormal cardiac examination, or a baby who looks genuinely unwell should pull the clinician away from TTN toward these alternatives without delay. [1]
Clinical & Bedside Assessment
Assessment begins with the pattern and rate of breathing, the work of breathing, and the baby's overall appearance in the first golden hour. Respiratory rate, oxygen saturation in room air and then in oxygen, heart rate, temperature, and capillary refill give a rapid bedside picture, while the Silverman-Anderson retraction score quantifies distress and tracks response to support. [1]
A focused examination checks for dysmorphism, equal air entry, added sounds, murmur, abdominal distension, and skin integrity, because a single finding — a murmur, asymmetric breath sounds, or a scaphoid abdomen — can redirect the whole plan. Continuous oxygen saturation monitoring with a defined target of 91–95% keeps supportive therapy proportionate. [1]
Investigations
A chest radiograph is the core investigation: TTN shows prominent perihilar streaking, increased lung volumes with hyperinflation, fluid in the minor (horizontal) fissure, and occasionally mild cardiomegaly and pleural fluid. These findings contrast with the diffuse, low-volume granularity of surfactant deficiency. [1]
Lung ultrasound has become a powerful adjunct because the "double lung point" — a sharp transition between superior B-lines and inferior normal pleura — is highly specific for TTN and helps separate it from RDS. Meta-analytic data now confirm strong diagnostic accuracy for lung ultrasound in TTN, supporting its bedside use where sonographers are trained. [1]
Blood tests are directed at excluding alternatives rather than confirming TTN: a full blood count and C-reactive protein with blood culture are taken to cover sepsis, and serial inflammatory markers guide when empirical antibiotics can safely stop. Capillary or arterial blood gas assesses the degree of hypoxaemia and carbon dioxide retention, and a pre-post-ductal comparison screens for shunting. [6]
Management — Resuscitation
Most babies with TTN never need active resuscitation, but the approach follows standard neonatal resuscitation principles: warmth, drying, positioning, and stimulation, with supplementary oxygen titrated to keep saturations in the 91–95% range. Intubation and surfactant are not part of TTN management and, if they appear necessary, signal that the diagnosis is wrong. [3]
The immediate priorities are to establish adequate gas exchange, secure intravenous access if feeds must be withheld, and begin the sepsis work-up so that empirical antibiotics are not delayed. Gentle, clustered handling reduces the oxygen cost of agitation in a baby whose reserves are limited. [3]
Management — Definitive & Stepwise
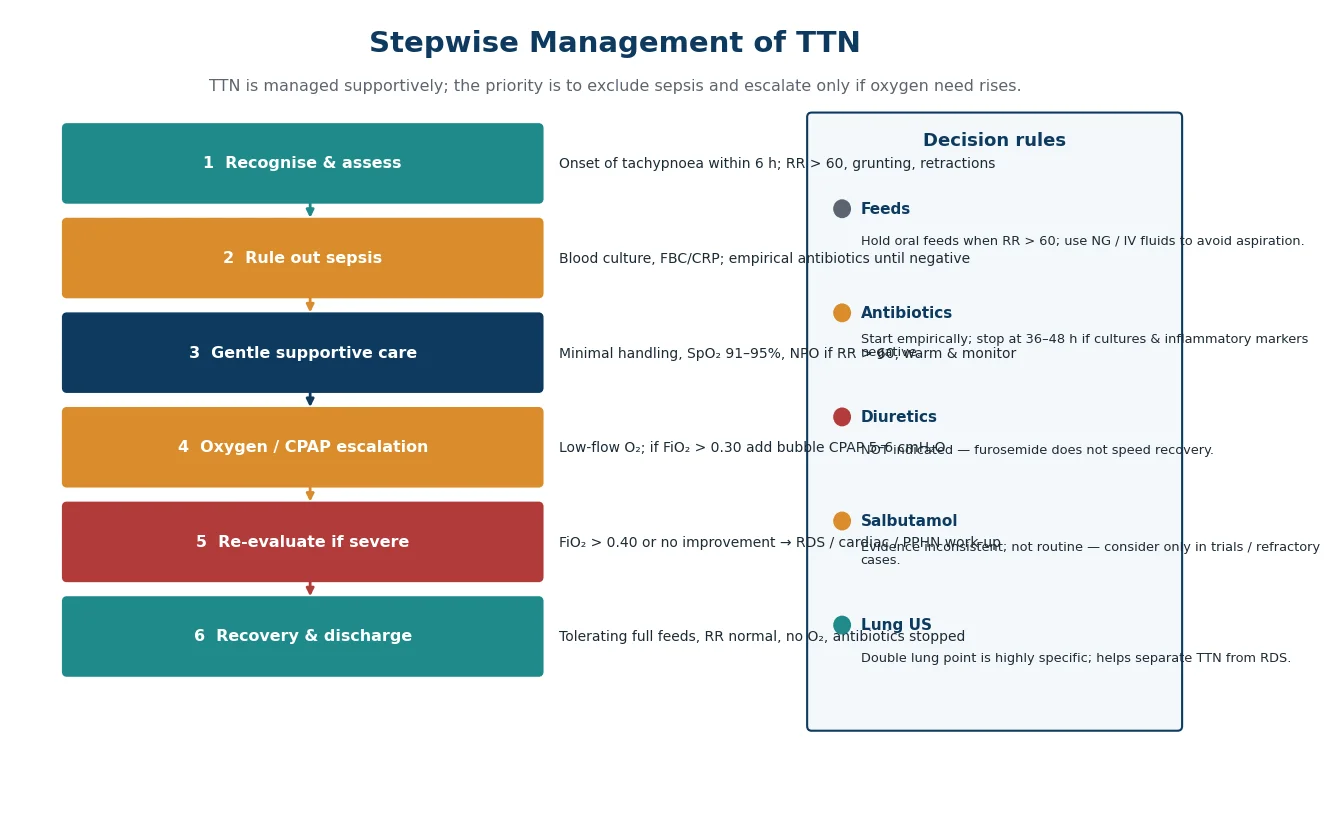
Definitive care is supportive while the lung fluid clears over the first one to three days. Oxygen is delivered by low-flow nasal cannula or head box to maintain the target saturation, oral feeds are held when the respiratory rate exceeds 60 and replaced with nasogastric or intravenous fluids to avoid aspiration, and empirical antibiotics are started after cultures and stopped at 36–48 hours if cultures and inflammatory markers are negative. [1]
When distress is moderate, bubble or nasal CPAP at around 5–6 cmH₂O splints alveoli and improves oxygenation while avoiding intubation; escalation beyond this should trigger re-evaluation rather than tighter labelling. Diuretics such as furosemide do not accelerate recovery and are not indicated. [1]
TTN management ladder
Assess: RR, work of breathing, SpO₂ 91–95% target
Exclude sepsis: culture, FBC, CRP; start empirical antibiotics
Support: oxygen by low-flow or head box; hold oral feeds if RR exceeds 60
Escalate: bubble CPAP 5–6 cmH₂O if FiO₂ above 0.30
Re-evaluate: if FiO₂ above 0.40, reconsider RDS, cardiac disease, PPHN
Recover: full feeds, normal RR, no oxygen, antibiotics stopped
The place of beta-agonists is the main therapeutic controversy. Salbutamol acts on the beta-receptors that drive ENaC-mediated sodium and fluid absorption, giving it a plausible mechanism, yet randomised trial evidence is inconsistent. A 2025 randomised controlled trial found nebulised salbutamol shortened the duration of tachypnoea, and an earlier dose-ranging study evaluated 2.5 mg versus 1.25 mg regimens against placebo, but routine use is not yet standard. [4]
Because the evidence does not consistently favour benefit, salbutamol should be reserved for trial or clearly refractory cases rather than given to every infant, and a lung-ultrasound aeration score is increasingly used to quantify any treatment effect. The safest stance for an exam answer is that TTN is managed supportively, with beta-agonists as an investigational adjunct rather than first-line therapy. [5]
Specific Subtypes & Scenarios
Late-preterm infants (34 to 36 weeks) are over-represented among TTN cases because their ENaC machinery is less mature and their surfactant reserve is lower, blurring the line between TTN and early RDS. These babies need closer monitoring and a lower threshold to evaluate for surfactant deficiency or hypoglycaemia from immature metabolic control. [3]
TTN after elective caesarean is its own scenario and the most preventable form: cord-hormone studies confirm that the absence of a labour catecholamine surge underlies the excess respiratory morbidity seen with planned delivery before 39 weeks. Scheduling elective caesarean at or after 39 completed weeks, and allowing a trial of labour where appropriate, reduces the incidence substantially. [3]
Complications & Pitfalls
The commonest complication is iatrogenic — unnecessary antibiotics, prolonged admission, or parental anxiety — but the serious pitfall is diagnostic anchoring. A baby labelled TTN who actually has sepsis, a duct-dependent cardiac lesion, or persistent pulmonary hypertension can deteriorate while the team waits for fluid to clear. [1]
A small proportion of infants with apparent TTN have transient pulmonary hypertension contributing to hypoxaemia, and failing to detect a pre-post-ductal gradient delays the recognition of right-to-left shunting. Any baby whose course deviates from the expected rapid improvement, or whose oxygen need climbs above 40%, must be re-evaluated rather than reassured. [8]
Prognosis & Disposition
The outlook is excellent: virtually all term infants recover fully within 72 hours with no long-term respiratory sequelae, and discharge is appropriate once the baby tolerates full feeds, breathes normally in room air, and has completed its antibiotic course. Most infants can be managed on the postnatal ward or a level-II nursery and never need tertiary intensive care. [1]
An intriguing longer-term association is the link between TTN and subsequent wheezing. Population data suggest that TTN may be an early clinical manifestation of wheezing symptoms in childhood, and a recent birth-cohort study found TTN increased the risk of bronchiolitis in the first two years. These associations do not change acute management but are worth mentioning to parents as the reason some children wheeze more after a TTN admission. [7]
Special Populations
Infants of diabetic mothers carry a dual risk: they are more often large and delivered by caesarean, and they have immature surfactant kinetics, so respiratory distress that looks like TTN can mask early RDS. These babies warrant a lower threshold for surfactant evaluation and close glucose monitoring. [3]
In the elective-caesarean population, the intervention is obstetric rather than neonatal: deferring planned delivery to 39 weeks and choosing anaesthetic technique to minimise neonatal respiratory depression measurably reduce TTN and more serious respiratory morbidity. Counselling expectant parents about the respiratory cost of early elective delivery is part of prevention. [10]
Evidence, Guidelines & Regional Differences
The strongest, most actionable evidence in TTN is preventive: avoiding elective delivery before 39 weeks lowers the incidence of respiratory distress across all severities. On the diagnostic side, lung ultrasound has matured from a research tool into a bedside standard, with meta-analysis confirming high accuracy for distinguishing TTN from other causes of neonatal respiratory distress. [1]
The therapeutic debate centres on salbutamol. Trials of nebulised salbutamol give conflicting results — some shorten the duration of tachypnoea and improve lung-ultrasound aeration, while dose-ranging work on 2.5 mg versus 1.25 mg regimens has not produced consensus guidelines — so most national guidelines still describe TTN as a condition requiring supportive care alone. [4]
Across ANZ, European and North American practice, the consensus is supportive care with SpO₂ targets around 91–95%, empirical antibiotics until sepsis is excluded, and escalation only for rising oxygen need. The regional differences are minor and mostly concern the uptake of lung ultrasound and the exact saturation target band. [5]
Exam Pearls
For written and viva exams, TTN is a high-yield topic because it is common, has a clean mechanism, and tests whether you can justify a reassuring plan while naming the diagnoses you must exclude. Be ready to draw the mechanism: labour catecholamines activate ENaC, sodium drives fluid absorption, and elective caesarean without labour is the key risk factor because it removes that signal. [2]
Examiners love the differentials and the chest radiograph: perihilar streaking with fluid in the fissure and hyperinflation is the pattern, contrasted with the ground-glass, low-volume appearance of RDS. State that management is supportive — oxygen, hold feeds if tachypnoeic, CPAP for moderate distress, empirical antibiotics until sepsis excluded — and that diuretics are not indicated while salbutamol remains investigational. [1]
References
- [1]Niu Y, Han D, Kou C Diagnostic accuracy of lung ultrasound for transient tachypnea of the newborn: a meta-analysis. Front Pediatr, 2026.PMID 42422445
- [2]Süvari L, Janér C, Helve O Postnatal gene expression of airway epithelial sodium transporters associated with birth stress in humans. Pediatr Pulmonol, 2019.PMID 30920175
- [3]Atasay B, Ergun H, Okulu E The association between cord hormones and transient tachypnea of newborn in late preterm and term neonates who were delivered by cesarean section. J Matern Fetal Neonatal Med, 2013.PMID 23311764
- [4]Dhaka A, Kumar S, Singh P Nebulized salbutamol for the treatment of transient tachypnea of the newborn: a randomized controlled trial. J Perinatol, 2025.PMID 39690178
- [5]Choobdar FA, Vahedi Z, Mazouri A Safety and Efficacy of 2.5 mg and 1.25 mg Nebulized Salbutamol Compared with Placebo on Transient Tachypnea of the Newborns: A Triple-Blind Phase II/III Parallel Randomized Controlled Trial. J Aerosol Med Pulm Drug Deliv, 2024.PMID 38687321
- [6]Priyadarshi M, Kaur A, Dhaka A Effect of Nebulized Salbutamol on Lung Ultrasound Aeration Score in Transient Tachypnea of Newborn. Indian J Pediatr, 2026.PMID 41483397
- [7]Liem JJ, Huq SI, Ekuma O Transient tachypnea of the newborn may be an early clinical manifestation of wheezing symptoms. J Pediatr, 2007.PMID 17586187
- [8]Can Oksay S, Sahin MK, Bilgin G Is Transient Tachypnea of the Newborn a Risk Factor for Bronchiolitis in the First Two Years of Life? A Population-Based Birth Cohort Study. Medeniyet Med J, 2025.PMID 41018067
- [9]Lu K, Chen X, Zhu W Terbutaline alleviates the lung injury in the neonatal rats exposed to endotoxin: Potential roles of epithelial sodium channels. Pediatr Pulmonol, 2019.PMID 30644180
- [10]Alhowary AA, Altal O, Khasawneh W Mode of Anesthesia During Cesarean Section and Neonatal Morbidity and Mortality: A Cohort Study. Local Reg Anesth, 2026.PMID 42305645