Paeds · fetal-neonatal-and-perinatal
Transition at birth and delayed cord clamping
Also known as Neonatal transition · Fetal-to-neonatal circulatory adaptation · Deferred cord clamping · Delayed cord clamping · Placental transfusion · Intact-cord resuscitation
Fellowship guide to neonatal transition and delayed (deferred) cord clamping: the physiology of fetal-to-neonatal circulatory adaptation, the placental transfusion, timing thresholds for term and preterm infants, when cord milking is contraindicated, intact-cord resuscitation, and the regional guideline differences across ANZ, UK, US, Canada and WHO.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A baby is born, the placenta is left behind, and in the next minute the entire circulation has to rewire itself. Neonatal transition is that rewiring — the shift from fetal placental gas exchange, with fluid-filled lungs and right-to-left shunting, to air breathing with closed shunts and the lungs doing the work. It is the single most important physiological event of early life, and most newborns accomplish it unaided. [12] [13]
The cord is the hinge on which transition turns. In fetal life the placenta holds a large share of the combined fetal-placental blood volume, and at birth that blood is meant to move from placenta to infant over the first one to three minutes — the placental transfusion. Clamping the cord immediately at birth cuts that transfer short; delayed (deferred) cord clamping deliberately leaves the cord intact so the transfusion completes. The distinction is not cosmetic: the placental transfusion delivers roughly a third of the newborn's eventual blood volume, raises haemoglobin and ferritin, smooths the preterm infant's haemodynamic entry into the world, and is now standard care for almost every newborn who does not need immediate resuscitation. [1] [15]
The key idea that organises everything else is simple: transition and cord management are the same event, viewed from two sides. Keeping the cord intact during the first minute is not an add-on to transition — it is how a healthy transition is meant to happen. The cord plan is settled before delivery, and it changes only when the infant forces it to, by needing resuscitation. [13] [14]
Classification
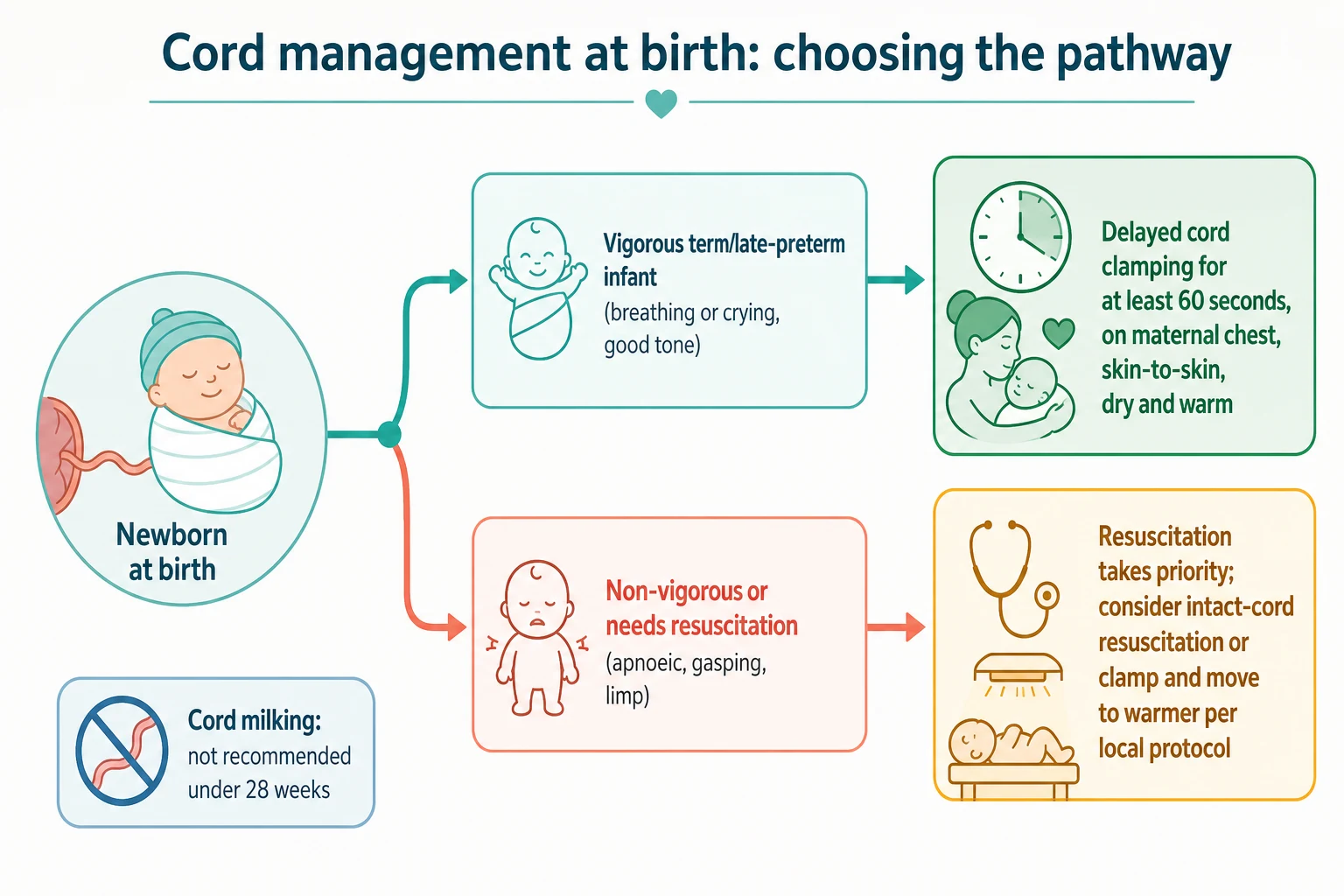
Think of cord management as a single decision tree, and the first branch is the only one that matters in the delivery room: is the infant vigorous, or does it need resuscitation? A vigorous term or late-preterm infant — breathing or crying, with good tone — stays on the maternal chest for deferred clamping of at least 60 seconds. A non-vigorous infant (apnoeic, gasping, or limp) needs resuscitation, and the cord plan yields to that: resuscitate with the cord intact if a bedside trolley and trained team are available, otherwise clamp and move to the warmer. [12] [13]
Once the pathway is set, the second layer of classification is the technique of placental transfusion. Four strategies exist, and they are not interchangeable: deferred (delayed) clamping (leave the cord intact for a set time), intact-cord resuscitation (resuscitate at the bedside with the cord still attached), cord milking (squeeze blood from placenta to infant — either cut-and-milk or intact-cord milk), and immediate (early) clamping (reserved for the rare infant needing instant separation). [15]
Four cord-management strategies compared
- Cord intact for at least 60 s (term) or 30 to 60 s (preterm)
- Default for vigorous term, late-preterm and stable preterm infants
- Baby stays skin-to-skin on mother
- Best-evidenced, lowest-risk option
- Resuscitate at a bedside trolley with cord attached
- For the infant who needs help but may still benefit from the transfusion
- Needs a dedicated trolley and trained team
- Evidence building, especially for the preterm
- Milk blood from placenta toward infant (cut-and-milk or intact)
- Faster transfusion than deferred clamping
- Not for infants under 28 weeks (excess severe IVH)
- Not routine for non-vigorous term or late-preterm infants
- Clamp within the first seconds
- Reserved for infants needing instant separation and resuscitation
- Cuts the placental transfusion short
- Not appropriate for the vigorous infant
Epidemiology & Risk Factors
The reassuring headline is that the overwhelming majority of newborns transition without help, and almost all are candidates for deferred clamping. About nine in ten need no active intervention, about one in ten needs some assistance to transition, and roughly one in a hundred needs advanced resuscitation with compressions or adrenaline. [12]
The infants who are not simple candidates for deferred clamping are precisely those who may fail transition, and they concentrate where risk can be anticipated. Prematurity, low birthweight, fetal distress, emergency caesarean, instrumental delivery, meconium-stained liquor, chorioamnionitis, maternal diabetes, pre-eclampsia and known congenital anomaly all raise the chance that the infant will need resuscitation rather than a quiet 60 seconds on the cord. For these, the team and the cord plan are settled before delivery so that resuscitation can begin without delay if the infant is non-vigorous at birth. [12] [13]
Gestation changes the equation twice over. The more preterm the infant, the greater the benefit of a placental transfusion — the preterm circulation tolerates abrupt loss of placental return poorly, and a gentler haemodynamic transition lowers intraventricular haemorrhage and transfusion need. But the same infants are also more likely to need active resuscitation and to become hypothermic if held on the cord, which is why preterm cord management is a rehearsed team event with active warming rather than a casual wait. [2] [7]
The term infant in a low-resource setting is the population in whom deferred clamping has the largest public-health value, because the iron-store advantage translates directly into less iron-deficiency anaemia across infancy. WHO has therefore recommended deferred clamping for one to three minutes for all newborns for over a decade, with particular emphasis where iron deficiency is prevalent. [1] [4]
Pathophysiology
To understand why the cord matters, follow the blood. In fetal life the lungs are filled with fluid, the pulmonary arterioles are clamped shut by low oxygen, and blood bypasses the lungs through two right-to-left channels: the foramen ovale, shunting right-atrial blood to the left atrium, and the ductus arteriosus, shunting pulmonary-artery blood to the aorta. The placenta, not the lungs, is the organ of gas exchange. [13] [14]
At birth three events must occur together, and they are triggered by the first breaths. Lung fluid is cleared and replaced by air, which drops pulmonary vascular resistance and pulls blood into the lungs. Left-atrial pressure rises as pulmonary venous return increases and right-sided pressure falls, functionally closing the foramen ovale. Rising blood oxygen constricts then closes the ductus arteriosus. As the cord is clamped and placental return ceases, systemic vascular resistance climbs. In a handful of minutes the circulation converts from a parallel right-to-left shunt to the normal adult-type series circuit. [12] [13]
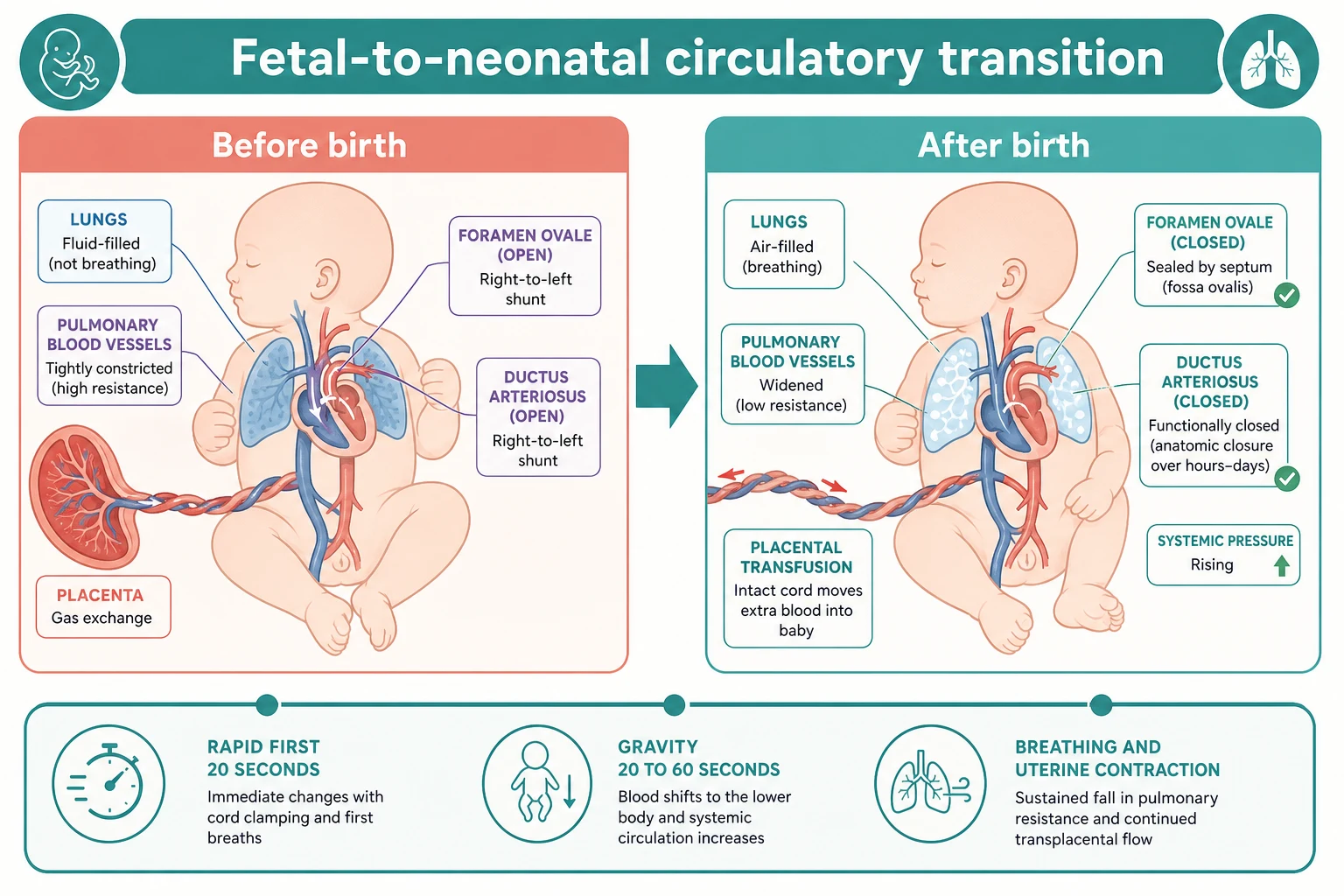
The placental transfusion is the half of this story the cord controls. It proceeds in three phases: a rapid phase in the first 20 seconds as uterine contraction and the first breaths shift blood, a slower gravity-dependent phase over the next 40 seconds, and a final phase driven by ongoing breathing and a further uterine contraction that completes the transfer by about three minutes. In a term infant the transfusion is roughly 80 to 100 mL — about a third of the newborn's blood volume — and raises haemoglobin by a clinically meaningful margin. [7] [15]
Why this matters mechanistically is easiest to see in the preterm infant. The extremely preterm circulation has little reserve, and abrupt loss of placental return produces a sudden drop in systemic and cerebral blood flow that the fragile germinal-matrix vasculature cannot absorb — a setup for intraventricular haemorrhage. A gentler, transfusion-supported transition preserves venous return and stabilises the right heart and cerebral perfusion, which is the physiological basis for the preterm outcomes that follow. [2] [8]
In the term infant the mechanism is metabolic rather than haemodynamic: the extra iron bound in the transfused red cells is laid down in stores that sustain haemoglobin synthesis through the months when dietary iron is scarce, which is why a one-minute cord decision measurably changes ferritin at four to six months of age. [4] [1]
Clinical Presentation
The vigorous newborn who is eligible for deferred clamping announces it in the first seconds: breathing or crying, good tone, and a healthy colour developing as the oxygen rises. This infant is dried, placed skin-to-skin on the mother, and simply observed through the intact-cord minute — heart rate rising toward normal, colour improving, tone maintained, and regular breathing established. [12]
The non-vigorous infant looks different and forces the cord decision. Poor tone at the moment of birth is an early global sign of a failing transition. Breathing may be absent (apnoea), inadequate (gasping), or simply not vigorous enough to clear fluid. A heart rate that stays low, or a baby who remains pale, limp or dusky despite warmth and stimulation, is an infant who needs active resuscitation — and whose cord plan must yield. [12] [13]
Between these two sits the preterm infant, who may be vigorous enough for deferred clamping but is fragile enough that the cord minute must be supervised. The signs of a successful intact-cord transition here are the same — rising heart rate, improving perfusion and tone, breathing that is adequate — but they are watched more closely, and the threshold to abandon the cord and resuscitate is lower. [2] [13]
The features that point away from a simple intact-cord minute toward a specific problem are worth holding in mind. Acute blood loss at birth (vasa praevia, cord rupture, twin-to-twin transfusion) presents with pallor and poor perfusion rather than cyanosis, and the infant may need volume. A scaphoid abdomen with respiratory distress suggests diaphragmatic hernia. Cyanosis unresponsive to oxygen may be duct-dependent cardiac disease. These infants are resuscitated per the standard algorithm; the cord is a footnote to their care, not the headline. [13]
Differential Diagnosis
When a newborn fails to transition despite an intact cord, work through the causes by what is commonest and most reversible — exactly as in resuscitation, because the differentials of failed transition are the resuscitation differentials. The leading cause, by a wide margin, is failed aeration: the lung has not been recruited, so pulmonary resistance stays high and the circuit stays fetal. [12]
A short list of alternatives changes management, and each has a tell: [12] [13]
Why an infant may fail transition (and the tell)
- Fluid not cleared, lung not recruited
- Commonest cause; ventilation is the fix
- Run the corrective steps before escalating
- Acute blood loss: vasa praevia, cord rupture, twin transfusion
- Pallor, poor perfusion, weak pulses
- Give intravenous volume or blood
- Opioids, magnesium sulfate, general anaesthesia
- Respiratory depression with preserved heart rate
- Ventilate; naloxone is not a resuscitation drug
- Diaphragmatic hernia, choanal atresia, airway malformation
- Often suspected antenatally
- Tailor the airway and ventilation plan
- Cyanosis unresponsive to oxygen as the ductus closes
- Declares after the first hours
- Prostaglandin E1, not more resuscitation
A separate differential question is whether deferred clamping is contraindicated in a given infant. The clearest contraindications are the need for immediate resuscitation without intact-cord equipment, a major congenital anomaly requiring instant surgical or airway intervention, and acute blood loss in which the infant is hypovolaemic rather than under-transfused. Rhesus haemolytic disease and polycythaemia are relative considerations, not absolute bars — the infant still usually benefits from a placental transfusion, and management is individualised. [12] [15]
Clinical & Bedside Assessment
The assessment of a newborn with the cord intact is the same first-minute assessment as any resuscitation, performed without separating the baby from the placenta. Receive the infant, start the clock, dry and stimulate, and assess the three things that drive every decision: tone, breathing, and heart rate. A vigorous infant — good tone, breathing or crying — stays on the cord; a non-vigorous infant moves to resuscitation. [12]
Heart rate is the number that decides escalation, so get it right. Auscultation over the precordium with a stethoscope is the quickest bedside method while the cord is intact; palpation of the cord base underestimates the rate and should not be trusted alone. When the rate is low or uncertain, three-lead electrocardiography within the first minute gives an accurate, objective reading — both the AHA and ERC recommend ECG when the heart rate is being used to direct resuscitation. [12] [13]
During the intact-cord minute, the practical question is when to stop waiting and act. The answer is the same as in resuscitation: if the infant is apnoeic or gasping, or the heart rate is under 100, begin positive-pressure ventilation. Deferred clamping is never a reason to delay ventilation in an infant who needs it — the options are to ventilate with the cord intact (if a bedside trolley and team are ready) or to clamp and move. [12] [13]
Cord MAP — decide the cord pathway in the first minute
Investigations
In the intact-cord minute almost no investigation is needed or appropriate — assessment is clinical. The one exception is cord blood gases, which are sampled from the clamped cord after the deferred period and reflect the infant's acid-base status at birth. Deferred clamping does not invalidate cord gases, but it does mean the timing of the clamp is documented so the gas is interpreted correctly. [13]
After the baby is stable, the investigations that matter are the ones that confirm the benefit or watch for the complications of the placental transfusion. A haemoglobin and ferritin at four to six months confirms the iron-store benefit in the term infant and is the measure used in the landmark trials. In the preterm, admission temperature, perfusion, glucose and a bilirubin trend are monitored, because the complications worth catching early are hypothermia, hypoglycaemia and a rising bilirubin. [4] [2]
A bedside haematocrit immediately after birth is occasionally measured in the polycythaemic or anaemic infant to judge the adequacy or excess of the transfusion, but it is not routine. When symptomatic polycythaemia is suspected (plethora, lethargy, poor feeding), a venous haematocrit guides the decision on partial exchange — remembering that symptomatic polycythaemia after deferred clamping is genuinely rare. [1] [15]
Management — Resuscitation
The immediate, time-critical bundle is the golden minute, and it coexists with the cord plan rather than competing with it. Receive the infant, provide warmth, dry and remove wet towels, stimulate by rubbing the back or flicking the soles, and assess tone, breathing and heart rate. For the vigorous infant these steps happen on the maternal chest with the cord intact. [12] [13]
The golden minute with an intact cord
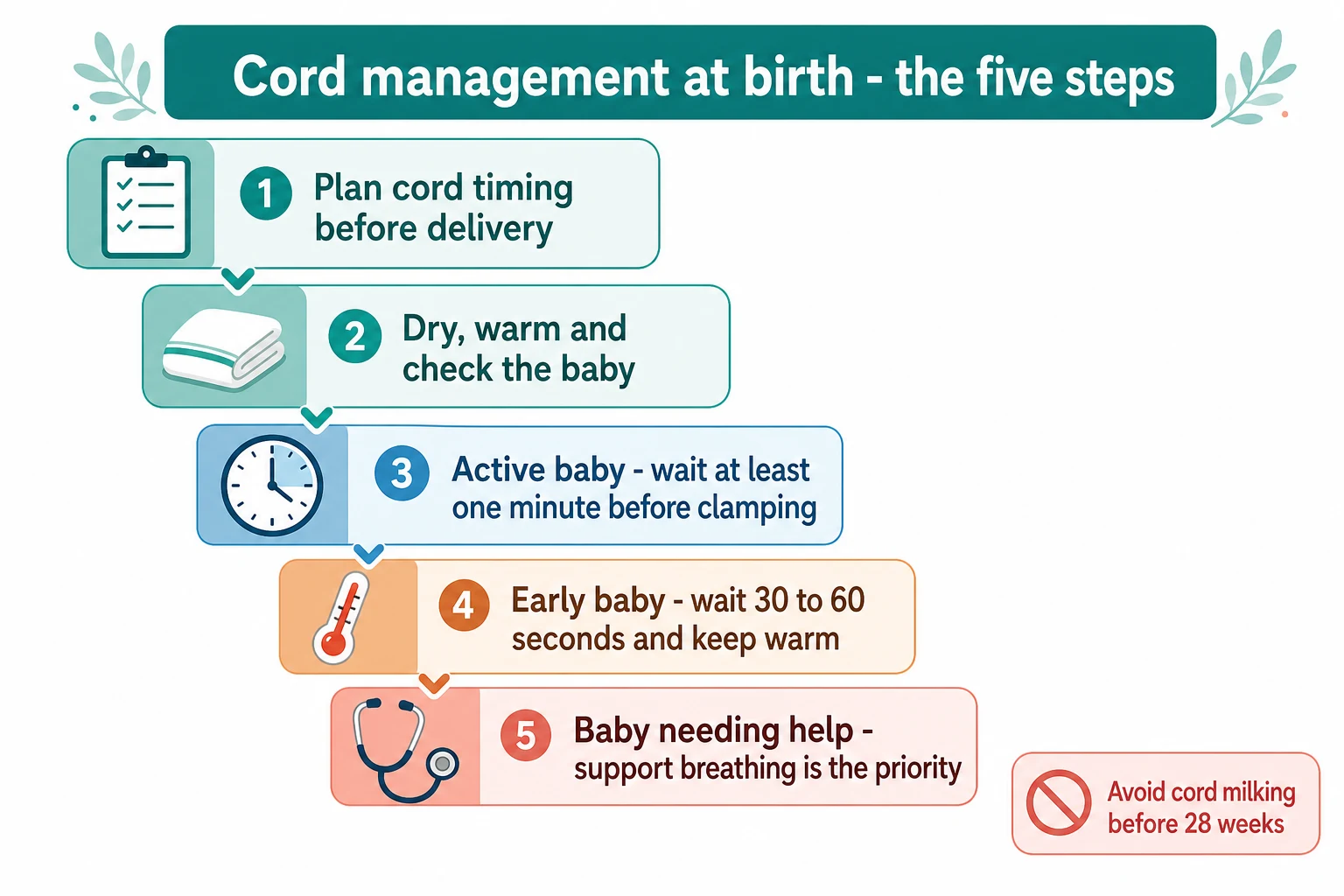
Plan the cord strategy before delivery — gestation, expected vigour, team and equipment
Receive the infant; start the clock; dry, warm and stimulate
Assess tone, breathing and heart rate in the first 60 seconds
Vigorous infant: keep cord intact for at least 60 s (term) or 30 to 60 s (preterm), skin-to-skin
Non-vigorous infant: resuscitate — intact-cord if a bedside trolley and team are ready, otherwise clamp and move
Document the cord-clamp time, the team and the infant's response
Warmth is a treatment, not comfort, and it is the resuscitation step most often compromised by the cord plan. Hold the temperature at 36.5 to 37.5 degrees from the moment of birth. For the term infant this is warm towels, a hat and skin-to-skin. For the preterm it is a plastic bag or wrap applied without drying, an exothermic thermal mattress, a hat, and a raised ambient temperature — and at caesarean section an active plan to prevent the cold drop that can otherwise accompany a longer cord minute. [12] [13]
If the infant is apnoeic or gasping or the heart rate is under 100, begin positive-pressure ventilation without delay — at 40 to 60 breaths per minute, air for the term infant and low oxygen for the preterm, using the lowest pressure that gives gentle chest rise. Ventilation is the single most effective resuscitation act, and a baby who needs it should not wait on the cord. The decision is only where to ventilate: with the cord intact if a bedside trolley and trained team are present, or after clamping and moving to the warmer. [12]
Positive-pressure ventilation during intact-cord resuscitation
Dose
40 to 60 breaths per minute; lowest pressure giving gentle chest rise (about 20 to 25 cm H2O in most term infants; preterm often needs PEEP 5 cm H2O)
Management — Definitive & Stepwise
The definitive procedure is the deferred clamp itself, and it is simple once the decision is made. At vaginal delivery, deliver the infant, dry and stimulate, place skin-to-skin on the mother, and hold the cord at the level of the infant or below to allow gravity to assist the transfusion. Wait at least 60 seconds for a vigorous term or late-preterm infant, then clamp. At caesarean section the same principle applies, with the infant held at or below the level of the placenta and kept warm — the technical challenge is thermoregulation and theatre teamwork, not the clamp itself. [12] [1]
For the stable preterm infant, defer for at least 30 to 60 seconds, ideally delivered with intact-cord stabilisation at a bedside trolley (such as a LifeStart or Concordance trolley) that allows warming, assessment and ventilation without separating the infant from the placenta. Active warming is non-negotiable: a preterm infant held cold on the cord for a minute can lose more than it gains. [2] [13]
In Australia and Aotearoa New Zealand, national and state or territory perinatal guidelines support deferred cord clamping for at least 60 seconds in vigorous term infants and for at least 30 to 60 seconds in stable preterm infants, with intact-cord stabilisation recommended where equipment and trained staff are available; culturally safe practice is expected for Aboriginal, Torres Strait Islander, Maori and Pacific families. [13]
Cord milking is the alternative technique, and it has a narrow and clearly bounded place. In cut-and-milking, the cord is cut and then milked from the placental end toward the infant two to four times; in intact-cord milking, the cord is milked while still attached. Milking delivers the transfusion faster than deferred clamping and was proposed as a way to give preterm infants the benefit of a placental transfusion when a full deferral is impractical. [5] [15]
The boundary on milking is absolute and must be stated plainly: do not milk the cord in any infant under 28 weeks. The Katheria 2019 JAMA trial found that intact-cord milking, compared with deferred clamping, was associated with an excess of severe intraventricular haemorrhage in infants under 28 weeks, and the trial was stopped early on that basis. [3]
For the non-vigorous term or late-preterm infant, cord milking is not routine either. The MINVI trial and its two-year follow-up examined milking in non-vigorous infants born at 35 weeks or more: milking produced transiently better haemodynamics but no clear clinical benefit and a signal of harm at two years, so current guidance is that resuscitation per the standard algorithm — not milking — is the priority, with intact-cord resuscitation considered where the setup allows. [10] [11]
The escalation ladder holds the whole strategy together. Plan before delivery; for the vigorous infant, defer on the cord; for the infant needing help, resuscitate with the cord intact if possible; if the infant cannot be stabilised with the cord intact, clamp and move for advanced resuscitation; and escalate to compressions and adrenaline by heart rate only after ventilation is effective. Each step has a trigger, and the team is briefed on all of them in advance. [12] [13]
The cord-management escalation ladder
Documentation closes the loop. Record the cord-clamp time, the team, the technique (deferred, intact-cord resuscitation, milking, or immediate), the infant's heart rate and tone through the intact-cord period, and any escalation. This is both the medico-legal record and the audit data that drives uptake of deferred clamping as standard care. [15]
Specific Subtypes & Scenarios
The very and extremely preterm infant (under 32 and under 28 weeks) is the population in which cord management changes the most and matters the most. Deferred clamping for at least 30 to 60 seconds, ideally with intact-cord stabilisation and aggressive warming, is the standard. The line that must be held is the milking one: under 28 weeks, deferred clamping yes, milking no. Every preterm delivery should have the cord plan, the warming choreography and the trolley settled before the infant arrives, because the hypothermia and haemodynamic cost of an improvised minute is high. [2] [3]
Caesarean section makes deferred clamping technically harder but not contraindicated. The infant is held at or below the level of the placenta to preserve gravity-assisted flow, and the warming plan is intensified because theatre environments are cold and the exposed wet preterm infant cools fast. The obstetric and neonatal teams coordinate the cord-clamp timing as part of the planned procedure. [1] [13]
Multiple gestation is managed infant by infant. The first twin is handled as a singleton. The second twin's cord plan depends on its presentation and stability — monitoring for twin-to-twin transfusion or growth restriction is part of the antenatal plan, and a second team and equipment set are ready. Deferred clamping is feasible for both, with the cord plan adapted to each infant's vigour. [15]
The infant of a mother living with HIV no longer requires immediate clamping on the basis of HIV alone. Current WHO guidance recommends deferred cord clamping even for mothers on effective antiretroviral therapy, because the iron-store and haemodynamic benefits apply and the HIV transmission rationale for early clamping has fallen away with effective treatment. [15]
Cord blood banking sits in direct tension with deferred clamping, because the two compete for the same placental blood. In public banking, deferred clamping takes priority — the infant's transfusion is not sacrificed for a stored unit. In directed or family banking the family is counselled that deferred clamping reduces the volume available for storage, and the decision is made in advance, not at the bedside. [15]
Low-resource and out-of-hospital settings are where deferred clamping has its greatest value and its simplest execution. With no trolley, no blender and no NICU, the irreducible cord plan is still possible: dry the infant, place skin-to-skin on the mother, keep warm, and defer the clamp for one to three minutes. This alone improves iron stores across infancy at no cost, which is why WHO frames deferred clamping as an essential newborn-care intervention for every setting. [1] [4]
Complications & Pitfalls
The two complications families and trainees worry about most are jaundice and polycythaemia, and the evidence on both is reassuring. The Cochrane term review found that deferred clamping produces a small rise in bilirubin and a small increase in the need for phototherapy, but no significant increase in clinical jaundice or harmful hyperbilirubinaemia; the iron-store benefit clearly outweighs the jaundice cost, and phototherapy is a manageable, reversible event. [1]
Symptomatic polycythaemia and hyperviscosity are genuinely rare after deferred clamping — the meta-analyses do not show a clinically important increase in infants needing partial exchange. Holding these two facts together is the counselling that examiners reward: deferred clamping trades a marginal, manageable rise in bilirubin for a real, lasting gain in iron stores, and it does not meaningfully raise the rate of symptomatic polycythaemia. [1] [15]
The complication that does matter is delaying resuscitation in a non-vigorous infant by clinging to the cord plan. Deferred clamping is never a reason to postpone ventilation in a baby who is apnoeic, gasping, or bradycardic. The error is to treat the cord as more important than the airway; the correction is to resuscitate first (intact-cord if possible, otherwise clamp and move) and let the cord plan serve the infant, not the other way around. [12] [13]
Hypothermia during the cord minute is the silent harm of a poorly planned deferral, especially in the preterm at caesarean section. A cold infant raises oxygen consumption, worsens acidosis and impairs surfactant — undoing the very benefit the placental transfusion was meant to deliver. The defence is rehearsed warming: plastic wrap without drying, a thermal mattress, a hat, raised ambient temperature, and a trolley that keeps the preterm infant warm with the cord attached. [2] [13]
The harm of cord milking in the wrong infant is the final pitfall, and it is the one most often tested. Under 28 weeks, milking causes excess severe intraventricular haemorrhage; in non-vigorous term and late-preterm infants it offers no benefit and a signal of harm at two years. The classic viva trap is the candidate who reaches for milking in a 26-week infant "because deferral is too slow" — the correct answer is deferred clamping with active warming. [3] [11]
Prognosis & Disposition
For the term infant, the lasting benefit of deferred clamping is metabolic: improved haemoglobin and ferritin through four to six months, and less iron-deficiency anaemia across infancy. The Andersson BMJ trial showed better iron status at four months, and the effect is largest where dietary iron is scarce, which is why the public-health value is greatest in low-resource populations. [4] [1]
For the preterm infant, the benefit is haemodynamic and survives longer: lower rates of intraventricular haemorrhage, fewer blood transfusions, better circulatory stability, and in some analyses lower mortality. The preterm meta-analyses are consistent on the transfusion and IVH signals, and the Mercer trial suggested better motor outcomes at 18 months. [2] [5] [8]
Andersson 2011 (BMJ) — iron stores at 4 months
Population: Vigorous term newborns at a Swedish hospital
Key finding
Significantly higher ferritin at 4 months in the delayed-clamp group, with no major harm
Practice change
A single cord-clamp decision measurably improves infant iron stores — the foundation of universal deferred clamping for term infants
Neurodevelopmental data are accumulating. Berg's follow-up of deferred clamping to three years suggested developmental benefit, while the MINVI two-year analysis of cord milking in non-vigorous infants showed no benefit and a harm signal — reinforcing that deferred clamping, not milking, is the evidence-supported approach. [9] [11]
After deferred clamping, disposition follows the infant. A vigorous term infant stays skin-to-skin, then enters routine newborn care — feeding, vitamin K, examination and screening. A preterm or resuscitated infant is admitted to the neonatal unit for monitoring, with attention to temperature, glucose and bilirubin. The family is told what was done, why, and what to watch for, and routine follow-up is arranged. [12] [13]
Special Populations
The extremely preterm infant (under 28 weeks) gets deferred clamping, not milking, delivered with intact-cord stabilisation and aggressive warming. The cord plan, the trolley and the thermal choreography are settled before delivery, because this infant cannot absorb a cold, improvised minute. [3] [2]
The growth-restricted or asphyxiated term infant may already be hypovolaemic or, conversely, polycythaemic, and the cord plan is individualised. Most still benefit from a placental transfusion, but the team is alert to the infant who needs volume rather than more blood, and to the rare polycythaemic infant in whom the transfusion is curtailed. [15]
The infant of an anaemic or iron-deficient mother is the term infant in whom the iron-store benefit is greatest — the placental transfusion partially offsets the depleted maternal-fetal iron endowment. Deferred clamping is strongly indicated here, and postnatal iron status is followed. [4] [1]
In low-resource settings, deferred clamping is reframed from a perinatal nicety to an essential public-health intervention. At no cost and with no equipment beyond warmth and patience, it reduces iron-deficiency anaemia across infancy — which is why it is a WHO priority and a skill every clinician should carry into any setting. [1]
The late-preterm infant and the infant of a diabetic mother is resuscitated and transitioned as usual but watched for the predictable early hypoglycaemia; the cord plan does not change, but glucose monitoring is part of the postnatal care. Multiple births have a team and a plan for each infant, and out-of-hospital births use the irreducible core — warmth, skin-to-skin and a one-to-three-minute deferral. [12] [13]
Evidence, Guidelines & Regional Differences
The evidence base for deferred clamping is one of the strongest in neonatal medicine. The Cochrane term review (McDonald 2013) established that deferred clamping improves iron stores through six months without significant maternal harm, including no increase in postpartum haemorrhage. The Cochrane preterm review (Rabe 2019) and the Fogarty meta-analysis established the preterm benefits — fewer transfusions and less intraventricular haemorrhage. [1] [2] [5]
What the landmark evidence changed
- Cochrane review
- Better iron stores through 6 months
- No significant rise in maternal postpartum haemorrhage
- Cochrane review
- Fewer blood transfusions and less IVH
- Lower mortality in some analyses
- Term RCT
- Higher ferritin at 4 months
- Foundation of universal deferred clamping
- Preterm milking vs deferred clamping
- Excess severe IVH under 28 weeks
- Stopped milking in the extremely preterm
The Katheria 2019 JAMA trial is the evidence that closed milking for the extremely preterm: intact-cord milking was associated with excess severe intraventricular haemorrhage under 28 weeks and the trial was stopped early. The MINVI trial and its two-year follow-up extended the caution to non-vigorous term and late-preterm infants — milking produced no clinical benefit and a harm signal at two years. [3] [10] [11]
The guidelines now align closely. WHO has recommended deferred clamping for one to three minutes for all newborns since 2014. The AHA 2020 neonatal guideline recommends deferred clamping for vigorous term and preterm infants who do not need resuscitation, and states that routine cord milking is not recommended under 28 weeks. The ERC 2021 guideline recommends deferred clamping for at least 60 seconds in term infants and intact-cord stabilisation for the preterm. NICE, ACOG and CPS guidance is concordant, and ANZ national and jurisdictional guidance aligns. [12] [13] [1]
The active controversies are narrower than they were. Intact-cord resuscitation is the main frontier — bedside trolleys allow resuscitation with the cord intact, and the evidence for the preterm is building, though uptake depends on equipment and team training. The optimal starting point for the preterm who needs ventilation, the place of sustained inflation during intact-cord stabilisation, and the exact duration of deferral that maximises benefit are still refined. Answer with the current guideline, name the source, and acknowledge where the evidence is still moving. [13] [15]
Exam Pearls
- Deferred cord clamping for a vigorous term infant: at least 60 seconds, skin-to-skin on the mother. [12] [1]
- Deferred cord clamping for a stable preterm infant: at least 30 to 60 seconds, with active warming and intact-cord stabilisation where available. [2] [13]
- Do not milk the cord under 28 weeks — excess severe intraventricular haemorrhage (Katheria 2019 JAMA). [3]
- The placental transfusion is about 80 to 100 mL, roughly a third of neonatal blood volume, and completes by about three minutes. [7]
- Resuscitation always takes priority — a non-vigorous infant is ventilated, not left on the cord. [12]
- Deferred clamping does not significantly increase maternal postpartum haemorrhage. [1]
- Iron-store benefit (ferritin at four to six months) is the headline term-infant gain — Andersson 2011 BMJ. [4]
- Fewer transfusions and less IVH are the headline preterm gains — Rabe 2019 Cochrane and Fogarty 2018. [2] [5]
- The jaundice trade-off is real but small and manageable — a marginal rise in bilirubin and phototherapy need, outweighed by the iron-store benefit. [1]
- Cord milking in non-vigorous term or late-preterm infants offers no benefit and a two-year harm signal — the MINVI legacy. [11]
- Intact-cord resuscitation is the evidence frontier — bedside trolley, trained team, transfusion plus ventilation together. [13]
- HIV in the mother is no longer a reason for immediate clamping when antiretroviral therapy is effective — defer the clamp. [15]
References
- [1]McDonald SJ; Middleton P; Dowswell T; Morris PS Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database Syst Rev, 2013.PMID 23843134
- [2]Rabe H; Gyte GM; Díaz-Rossello JL; Duley L Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst Rev, 2019.PMID 31529790
- [3]Katheria A; Reister F; Essers J; Mendler M Association of Umbilical Cord Milking vs Delayed Umbilical Cord Clamping With Death or Severe Intraventricular Hemorrhage Among Preterm Infants. JAMA, 2019.PMID 31742630
- [4]Andersson O; Hellström-Westas L; Andersson D; Domellöf M Effect of delayed versus early umbilical cord clamping on neonatal outcomes and iron status at 4 months: a randomised controlled trial. BMJ, 2011.PMID 22089242
- [5]Fogarty M; Osborn DA; Askie L; Seidler AL Delayed vs early umbilical cord clamping for preterm infants: a systematic review and meta-analysis. Am J Obstet Gynecol, 2018.PMID 29097178
- [6]Seidler AL; Gyte GML; Rabe H; et al Umbilical Cord Management for Newborns <34 Weeks' Gestation: A Meta-analysis. Pediatrics, 2021.PMID 33632931
- [7]Ghavam S; Batra D; Mercer J; et al Effects of placental transfusion in extremely low birthweight infants: meta-analysis of long- and short-term outcomes. Transfusion, 2014.PMID 24843886
- [8]Mercer JS; Erickson-Owens DA; Vohr BR; et al Effects of Placental Transfusion on Neonatal and 18 Month Outcomes in Preterm Infants: A Randomized Controlled Trial. J Pediatr, 2016.PMID 26547399
- [9]Berg JHM; Isacson M; Basnet O; et al Effect of Delayed Cord Clamping on Neurodevelopment at 3 Years: A Randomized Controlled Trial. Neonatology, 2021.PMID 33965945
- [10]Katheria A; Mercer J; Poeltler D; et al Hemodynamic Changes with Umbilical Cord Milking in Nonvigorous Newborns: A Randomized Cluster Cross-over Trial. J Pediatr, 2023.PMID 36914049
- [11]Katheria AC; El Ghormli L; Clark E; et al Two-Year Outcomes of Umbilical Cord Milking in Nonvigorous Infants: A Secondary Analysis of the MINVI Randomized Clinical Trial. JAMA Netw Open, 2024.PMID 38949814
- [12]Aziz K; Lee CHC; Escobedo MB; et al Part 5: Neonatal Resuscitation 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Pediatrics, 2021.PMID 33087555
- [13]Madar J; Roehr CC; Ainsworth S; et al European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation, 2021.PMID 33773829
- [14]Wyllie J; Bruinenberg J; Roehr CC; et al European Resuscitation Council Guidelines for Resuscitation 2015: Section 7. Resuscitation and support of transition of babies at birth. Resuscitation, 2015.PMID 26477415
- [15]Rabe H; Mercer J; Erickson-Owens D What does the evidence tell us? Revisiting optimal cord management at the time of birth. Eur J Pediatr, 2022.PMID 35112135