Paeds · gastroenterology-hepatology-and-nutrition
Abdominal wall and umbilical disorders
Also known as Gastroschisis · Exomphalos · Omphalocele · Umbilical hernia · Inguinal hernia · Umbilical granuloma · Omphalitis · Patent processus vaginalis · Giant omphalocele · Epigastric hernia
Fellowship guide to abdominal wall and umbilical disorders in children, built around the rule that gastroschisis sits to the right of a normally inserted cord with bare bowel and no sac, while an omphalocele sits in the midline with its contents covered by a sac and carries chromosomal and cardiac associations. The page covers the embryology of the two wall defects, the surgical versus expectant management of umbilical and inguinal herniae, the salt or silver nitrate treatment of the umbilical granuloma, and the red flag of omphalitis progressing to necrotising fasciitis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a newborn delivered at a tertiary obstetric unit whose intestines lie exposed beside the umbilical cord, or an infant in clinic whose mother points to a soft bulge at the belly button that pops in and out. These two children anchor the two ends of abdominal wall and umbilical disease in paediatrics. At one end sit the congenital wall defects, gastroschisis and omphalocele, which are life-threatening surgical emergencies recognised at birth or before. At the other end sit the common herniae and minor umbilical conditions that a general paediatrician manages every week. [3] [4]
The single discriminating fact to hold above all others is the relationship between the defect, the sac and the cord. In gastroschisis the bowel herniates through a full-thickness defect to the right of a normally inserted cord and lies uncovered. In an omphalocele, or exomphalos, the midline defect sits at the umbilicus, the contents are wrapped in a translucent sac, and the cord inserts onto that sac. This one anatomical difference predicts the chromosomal and cardiac associations, the urgency and the prognosis. [1] [3]
The governing principle is therefore to classify the defect first by its anatomy, then to apply the correct urgency. A congenital wall defect at birth needs protection of the bowel, vascular access and immediate transfer to a neonatal surgical centre. An umbilical hernia in a thriving toddler needs reassurance and a plan to observe. An inguinal hernia in any infant needs a prompt surgical referral because it will not close on its own and can incarcerate. Matching the anatomical diagnosis to the right timeline of action is the whole skill. [4] [7]
Classification
Sort the anterior abdominal wall defects first by whether the bowel is covered by a sac, because that single feature separates gastroschisis from omphalocele and predicts the associated anomalies. Gastroschisis is an uncovered paraumbilical defect with bare bowel and almost no chromosomal association. Omphalocele is a covered midline defect whose contents sit within a peritoneal-amniotic sac and whose rate of associated chromosomal and cardiac anomalies is high. [3] [6]
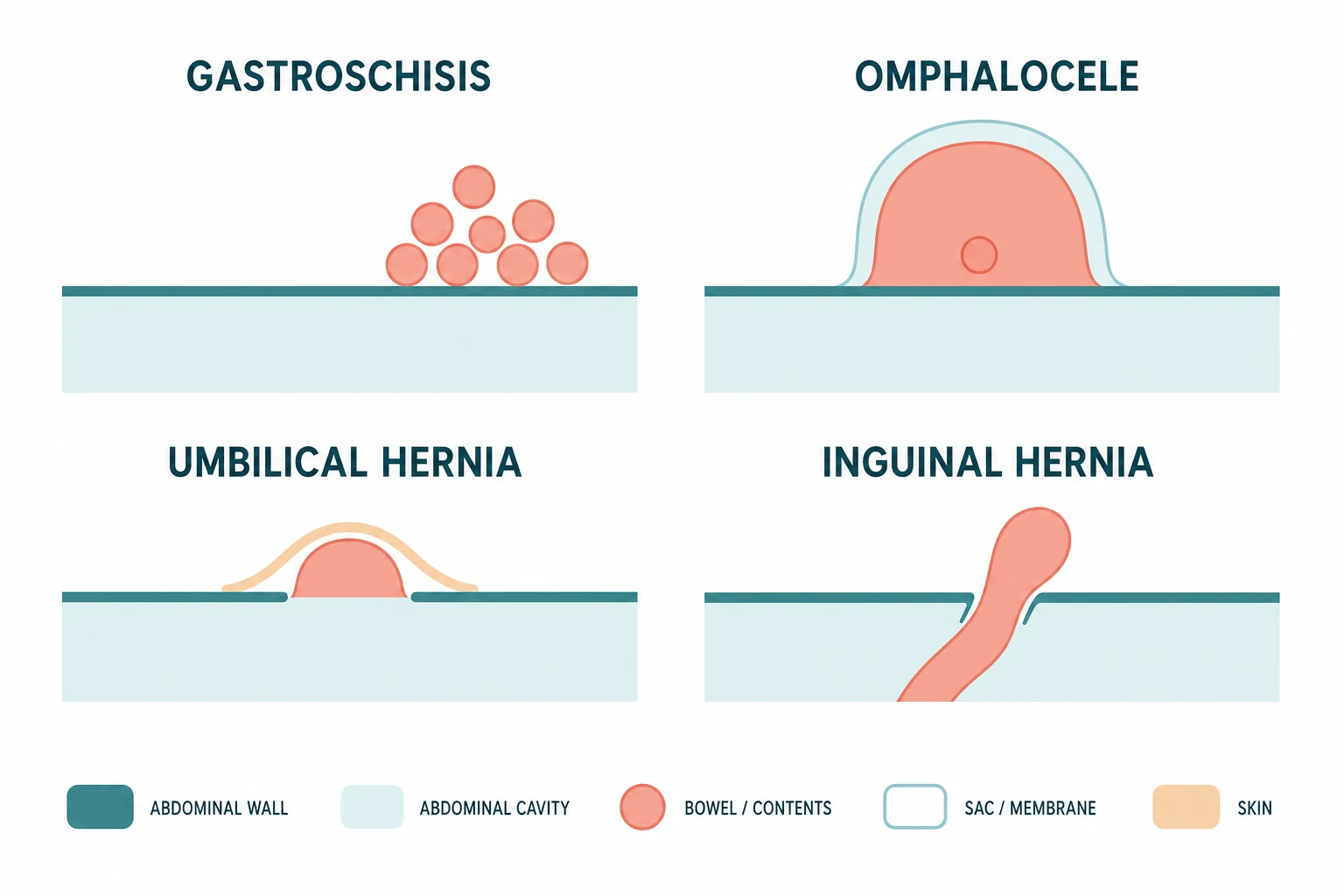
The second axis separates the common herniae of childhood by their natural history. An umbilical hernia is a fascial defect at the umbilical ring covered by intact skin, and because the ring continues to close after birth, most of these herniae resolve spontaneously. An inguinal hernia follows a patent processus vaginalis, and because that tract never closes on its own, every inguinal hernia in a child ultimately needs an operation. This natural-history split, one closes and one does not, is the fact candidates must own. [10] [7]
Gastroschisis
- Defect to the right of a normally inserted cord
- Bare bowel, no covering sac
- Usually isolated, low chromosomal association
- Rising incidence, linked to young maternal age
Omphalocele
- Midline defect at the umbilicus
- Contents covered by a peritoneal-amniotic sac
- Cord inserts onto the sac
- High rate of chromosomal and cardiac anomalies
Umbilical hernia
- Fascial defect at the umbilical ring, intact skin
- Most close spontaneously by age four to five
- Incarceration is rare
- Repair only if persistent or large
Inguinal hernia
- Patent processus vaginalis, bowel enters the canal
- Never closes spontaneously
- Incarceration risk highest in the first year
- Needs elective surgical repair
The minor umbilical conditions form a practical third group. An umbilical granuloma is a pink, moist, fleshy nodule left after cord separation and is treated with common salt or silver nitrate. Omphalitis is a bacterial infection of the stump that ranges from local cellulitis to life-threatening necrotising fasciitis. A patent urachus drains urine from the umbilicus, and an epigastric hernia is a small fat-containing defect in the linea alba above the umbilicus that usually needs repair. [11] [12]
Epidemiology & Risk Factors
Gastroschisis is the commoner of the two congenital wall defects and its incidence is rising worldwide, now around three to five per ten thousand live births in many high-income countries. The strongest and most consistent risk factor is young maternal age, with mothers under twenty carrying several times the risk of older mothers. Maternal smoking, recreational drug use, low socioeconomic status and primiparity also raise the risk, and the steady rise in teenage pregnancies in some regions is part of the explanation for the increasing incidence. [1] [2]
Omphalocele is less common, at roughly two to two and a half per ten thousand live births, and its incidence has been stable. Unlike gastroschisis, the omphalocele cluster of risk factors is chromosomal and developmental rather than environmental. Associated anomalies drive the prognosis, with chromosomal abnormalities such as trisomy 13 and trisomy 18 found in up to half of cases, cardiac defects in about a third, and syndromic associations including Beckwith-Wiedemann syndrome and Pentalogy of Cantrell. [3] [6]
The herniae of childhood have their own epidemiology. Inguinal hernia affects one to five percent of all children but up to thirty percent of premature and low-birth-weight infants, and boys outnumber girls by several fold. The risk of incarceration is highest in the first year of life, particularly in ex-preterm babies, which is why neonatal inguinal herniae are repaired promptly. Umbilical hernia is even more common, present in about ten to twenty percent of infants and in the great majority of very premature babies, yet it closes spontaneously in most and incarceration is rare. [7] [9]
Pathophysiology
The embryology of the anterior abdominal wall explains why gastroschisis and omphalocele look so different at birth. During the fourth to fifth week of gestation the embryo folds along two axes. The lateral folds move inwards to meet in the midline and close the body wall, while the cranial and caudal folds form the umbilical ring. The midgut then herniates normally into the umbilical cord from the sixth week and returns to the abdomen by the tenth week as the cavity enlarges. [3] [4]
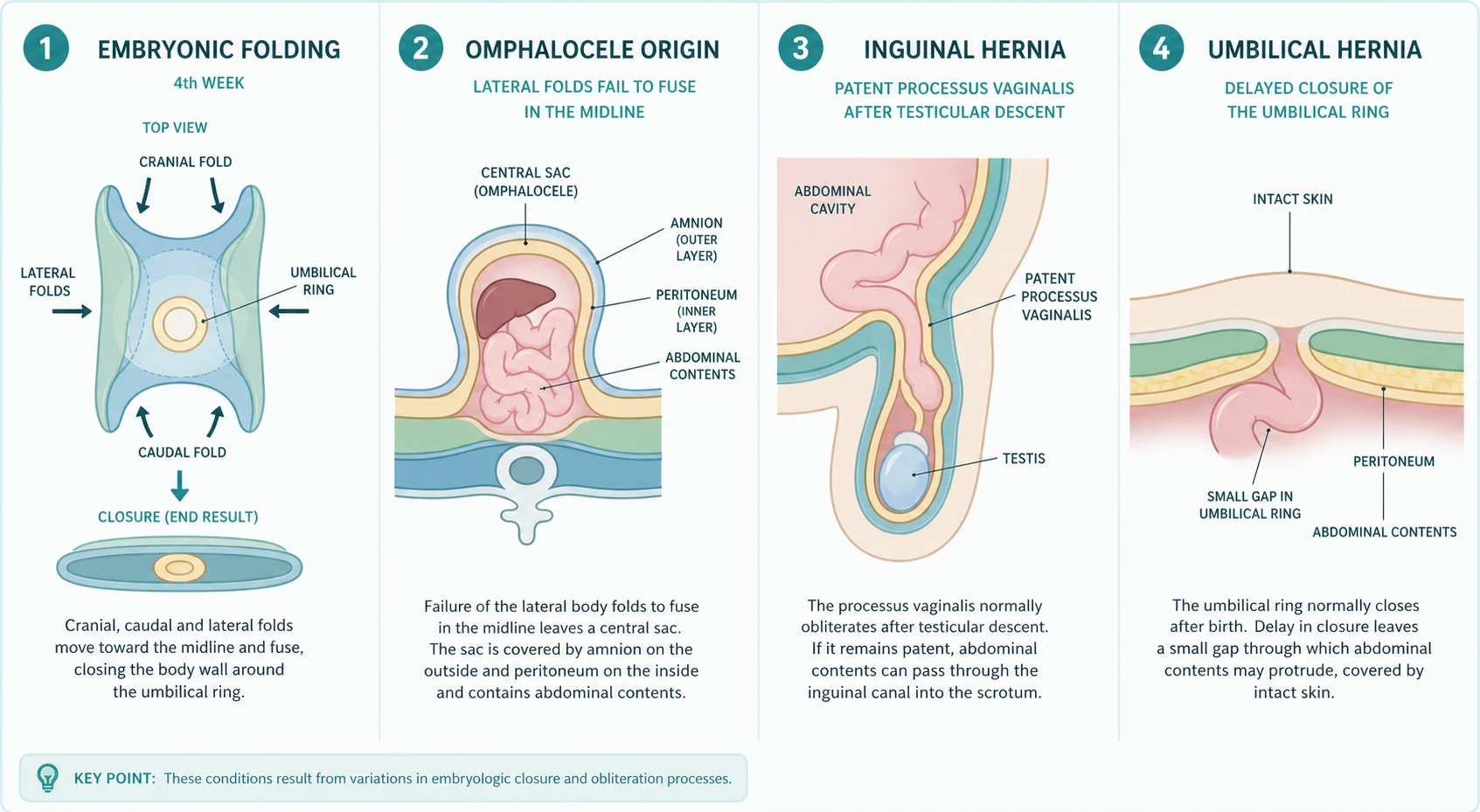
An omphalocele arises when the lateral folds fail to meet, so the midline gap never closes and the midgut remains outside the abdomen within its sac. Because this failure occurs early, during the period of organogenesis, it coincides with the formation of the heart and other organs, which explains the high rate of associated cardiac and chromosomal anomalies. When the sac is very large and contains the liver, the condition is called a giant omphalocele, and the small abdominal cavity cannot accommodate the organs, which makes primary closure difficult or impossible. [3] [5]
Gastroschisis arises later, after the body wall has closed, when the paraumbilical region disrupts, almost always on the right. The bowel escapes through a small full-thickness defect and is exposed to amniotic fluid, which produces the characteristic inflammatory peel, a thickened, oedematous, fibrin-coated bowel that distinguishes complex gastroschisis from the simple form. Because the failure happens after organogenesis, gastroschisis is usually isolated, and the associated morbidity comes from bowel damage, intestinal atresia or perforation rather than from chromosomal anomalies. [2] [1]
The common herniae follow simpler mechanisms. An inguinal hernia reflects a patent processus vaginalis, the peritoneal diverticulum that guided the testis into the scrotum and that should obliterate after birth. When it remains open, intra-abdominal contents, usually bowel or an ovary in girls, can enter the canal and form a hernia that cannot close spontaneously. An umbilical hernia reflects delayed fibrous closure of the umbilical ring after the cord separates, leaving a fascial defect that the rectus muscles gradually approximate and close in most children over the first few years. [7] [10]
Clinical Presentation
A congenital wall defect is usually diagnosed antenatally on the routine mid-trimester anatomy scan, so the presentation at birth is a planned delivery at a tertiary centre with neonatal surgery on standby. At delivery the diagnosis is immediately visible. In gastroschisis, loops of thickened, inflamed bowel protrude through a defect to the right of an otherwise normal umbilical cord, with no covering membrane. In an omphalocele, a central mass covered by a translucent sac protrudes from the umbilicus, the cord inserts onto the sac, and the size can range from a small sac containing a few bowel loops to a giant defect containing the entire liver. [3] [4]
An umbilical hernia presents as a soft, painless bulge at the umbilicus that enlarges with crying or straining and reduces easily with gentle pressure or when the child lies flat. The overlying skin is normal and intact. An inguinal hernia presents as an intermittent bulge in the groin or scrotum that appears with crying or straining and reduces spontaneously or with gentle pressure. The parent often notices it first at bath time or during a feed, and the examination may be normal between episodes, so asking the parent to photograph the bulge is a useful practical tip. [7] [9]
The minor umbilical conditions have their own presentations. An umbilical granuloma appears after the cord separates as a small, pink, glistening, moist nodule at the base of the umbilicus that produces a slight serous discharge but is painless. Omphalitis presents in the neonatal period with redness and induration around the stump, a purulent or foul-smelling discharge, and sometimes systemic signs of sepsis. A patent urachus presents with urine dribbling from the umbilicus during micturition. Each pattern points to its own management. [11] [12]
Differential Diagnosis
The congenital wall defects are rarely confused with each other after birth because the sac and the cord insertion are unambiguous, but the clinician must confirm which is present because the associated work-up differs. The key question is whether there is a covering sac and where the cord inserts. A sac with the cord on it is an omphalocele and triggers a chromosomal and cardiac evaluation. Bare bowel beside a normal cord is gastroschisis and the focus shifts to the bowel itself. [3] [6]
The groin swelling in an infant has a broader differential. A reducible bulge in the inguinal canal that appears with straining is an indirect inguinal hernia. A hydrocele is a fluid-filled scrotal sac that transilluminates brilliantly and does not reduce unless it communicates, and it usually resolves by age two. An undescended testis may present as an empty scrotum with a palpable groin mass, and an inguinal lymph node sits below and lateral to the canal rather than at the external ring. The discipline is to examine the groin and scrotum together and to feel whether the mass reduces into the abdomen. [7] [9]
Inguinal hernia
- Intermittent groin or scrotal bulge with straining
- Reduces with gentle pressure or spontaneously
- Does not transillumate unless fluid is also present
- Needs elective surgical repair
Hydrocele
- Fluid-filled scrotal sac that transilluminates
- Usually resolves by age two if communicating
- No bowel in the sac, no reduction impulse
- Observe unless persistent or large
Undescended testis
- Empty scrotum with a palpable mass in the groin
- Cannot milk the testis into the scrotum
- Distinguished from a retractile testis that can be brought down
- Refer for orchidopexy if still undescended by six months
The umbilical bulge also has a short differential. An umbilical hernia is central, reducible and covered by skin. An omphalocele minor, a small sac-covered defect, is present from birth and is covered by its membrane. An epigastric hernia sits above the umbilicus in the linea alba and usually contains only preperitoneal fat. A granuloma is a small red nodule at the base after separation, while omphalitis is an infected, cellulitic stump. The site, the skin covering and the timing distinguish them. [10] [11]
Clinical & Bedside Assessment
The assessment of a newborn with a wall defect begins at delivery and runs alongside resuscitation. Confirm whether the bowel is covered by a sac. Protect any exposed bowel from heat and fluid loss by wrapping the defect in a clean plastic bowel bag up to the axillae, which keeps the bowel moist and limits evaporative heat loss. Establish intravenous access, pass a nasogastric tube to decompress the stomach, and keep the child nil by mouth. These steps make the child safe for transfer to the surgical centre. [3] [4]
For the child with an umbilical or groin swelling in clinic, palpate the defect and its edges. Measure the umbilical fascial ring with a finger or callipers, because a ring wider than about one and a half centimetres is less likely to close spontaneously and may warrant earlier referral. For an inguinal hernia, confirm that the mass reduces and examine both sides, because a contralateral patent processus vaginalis is common. For a suspected granuloma, distinguish the pink, moist nodule from a small amount of granulation tissue that is normal during healing. [10] [7]
Investigations
Most abdominal wall and umbilical disorders are diagnosed clinically and need few investigations. The congenital wall defects are confirmed antenatally by ultrasound and sometimes by fetal echocardiography and amniocentesis when an omphalocele is found, because the chromosomal and cardiac associations change the counselling and the plan. After birth, a chest radiograph and an echocardiogram are obtained for an omphalocele to define the cardiac anatomy before surgery, while gastroschisis needs no chromosomal work-up unless dysmorphic features suggest a separate syndrome. [3] [6]
The herniae need no imaging in most cases because the diagnosis is clinical. An ultrasound of the groin can confirm a patent processus vaginalis when the examination is equivocal, and it is useful for the suspected hydrocele that does not transilluminate clearly or for a suspected incarcerated hernia where the viability of the bowel is in question. For the umbilical conditions, the diagnosis is visual, and the only investigation needed is a swab and blood cultures for a neonate with omphalitis and systemic signs, to guide antibiotic therapy. [9] [12]
Gastroschisis versus omphalocele — the mnemonic RIGHT SAC
Management — Resuscitation
The newborn with a congenital wall defect needs resuscitation that protects the bowel and the baby in parallel. Place the baby in a clean plastic bowel bag up to the axillae to keep the exposed bowel moist and warm and to limit evaporative heat and fluid loss, which is substantial from bare intestine. Establish intravenous access, give a dextrose-containing crystalloid for maintenance and extra losses, and pass a large-bore nasogastric tube on free drainage to decompress the stomach and prevent further distension of the herniated bowel. [3] [2]
Fluid management is aggressive because the exposed bowel loses large volumes of fluid and protein. Give intravenous fluids at about one and a half times maintenance, monitor the urine output, and correct electrolyte losses as guided by blood tests. Broad-spectrum antibiotics are started because the exposed bowel risks bacterial colonisation. Keep the child nil by mouth and begin parenteral nutrition early, because the bowel will not function for days to weeks, and the inflammatory peel prolongs the ileus. [2] [1]
Involve the neonatal surgical team from the moment of delivery and transfer the baby to a tertiary surgical centre if not already in one. For an incarcerated inguinal hernia, give analgesia and a dose of broad-spectrum antibiotic, attempt gentle taxis reduction under sedation if the child is stable, and prepare for theatre. For a neonate with omphalitis and systemic signs, take cultures, start broad-spectrum intravenous antibiotics without delay, and assess for necrotising fasciitis, which requires urgent surgical debridement. [9] [12]
Management — Definitive & Stepwise
Definitive management follows the anatomical diagnosis and its natural history. For gastroschisis, the aim is to return the bowel to the abdomen and close the defect safely. For omphalocele, the plan depends on the size, the associated anomalies and whether the abdominal cavity can accommodate the contents. For an umbilical hernia, the plan is to observe and to repair only those that persist. For an inguinal hernia, the plan is prompt elective repair to prevent incarceration, reserving urgent surgery for the incarcerated case. [4] [7]
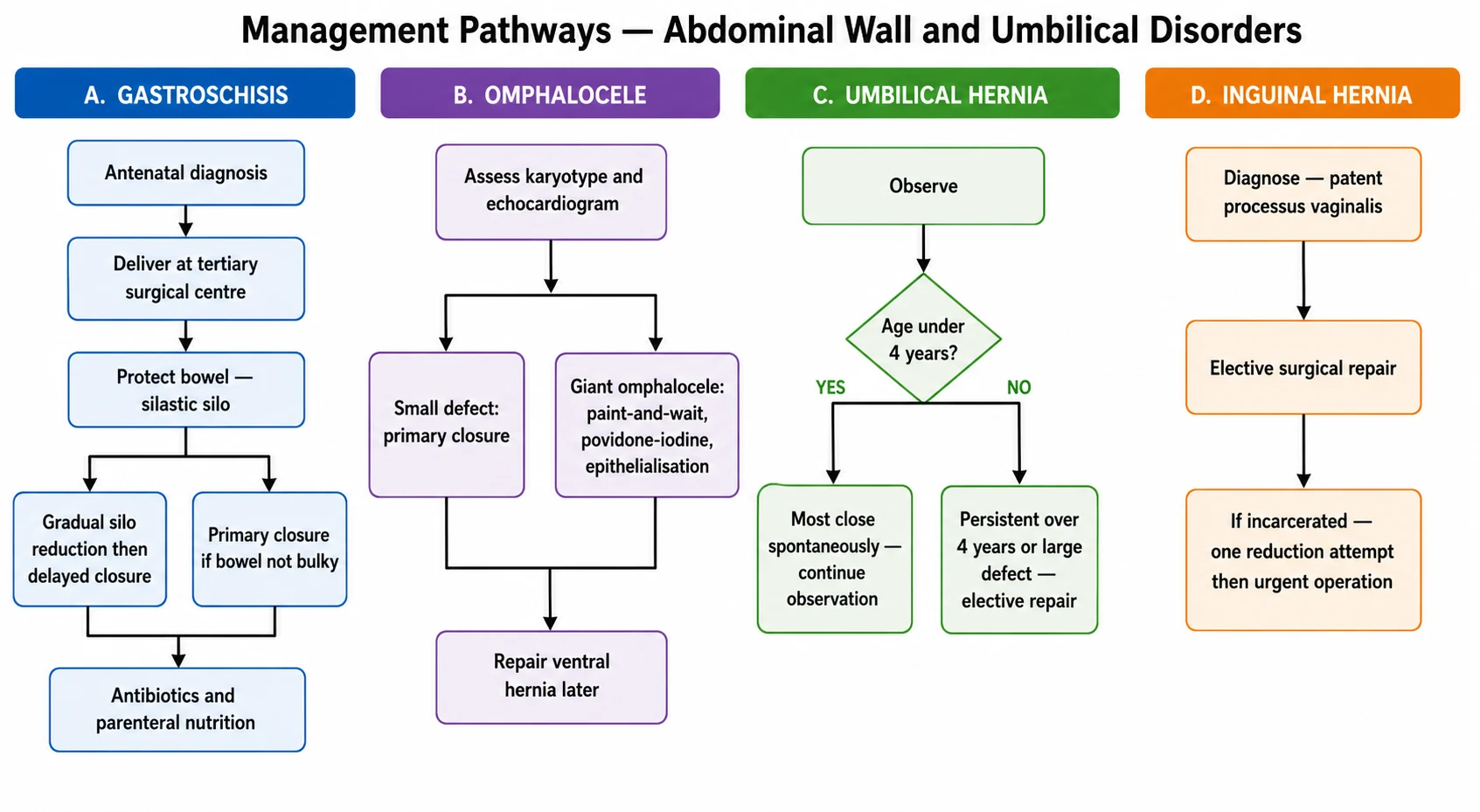
For gastroschisis, when the bowel is not too thickened or oedematous, a primary closure at the bedside or in theatre is performed soon after birth. When the bowel is too bulky to return safely, a preformed silastic silo is placed over the eviscerated bowel and suspended, and the bowel is gradually reduced into the abdomen over several days as the oedema settles and the cavity stretches, followed by delayed closure. Simple gastroschisis, where the bowel is intact and continuous, has an excellent outcome, while complex gastroschisis with atresia, perforation or necrosis needs additional bowel surgery and a longer course of parenteral nutrition. [1] [2]
Umbilical granuloma
Dose
Apply common table salt or silver nitrate stick to the granuloma surface
For omphalocele, a small defect with a small sac can be closed primarily after confirming the cardiac and chromosomal status. A giant omphalocele whose contents will not fit the cavity uses a paint-and-wait strategy, in which the sac is left intact and painted with an escharotic agent such as povidone-iodine to promote epithelialisation over weeks to months, building a tough ventral hernia that is repaired later in infancy. This conservative approach avoids the abdominal compartment syndrome that a forced primary closure would cause, and a European consensus supports it as the standard for the giant form. [5] [3]
For the herniae, the plans diverge on natural history. An umbilical hernia is observed, because the fascial ring continues to close and most resolve by age four to five; repair is offered for those persisting beyond that age, for a large ring that is unlikely to close, or in the rare event of incarceration. An inguinal hernia is referred for elective surgical repair as soon as practical, because it never closes on its own and the incarceration risk is highest in infancy, especially in premature babies in whom many surgeons operate within days of diagnosis. [10] [8]
Specific Subtypes & Scenarios
The giant omphalocele is the subtype that demands the most judgement. Because the liver and much of the bowel lie outside a small, underdeveloped abdominal cavity, a forced primary closure raises intra-abdominal pressure to dangerous levels, causing an abdominal compartment syndrome that compromises ventilation, venous return and renal perfusion. The paint-and-wait strategy avoids this by allowing slow epithelialisation of the intact sac, and the resulting ventral hernia is repaired electively months later when the cavity has grown. The trade-off is a long hospital stay and a prolonged risk of sac rupture. [5] [6]
Complex gastroschisis is the subtype that predicts a long and difficult course. When the exposed bowel has suffered an atresia, a perforation, a volvulus or segmental necrosis, the child faces additional bowel surgery, a prolonged period of parenteral nutrition, and the risk of short-bowel syndrome. The intrauterine inflammatory peel that coats the bowel is a marker of this severity, and ultrasound findings of dilated, thickened bowel antenatally predict a complex course. Simple gastroschisis, by contrast, typically closes within weeks and feeds are established quickly. [2] [1]
The premature infant with an inguinal hernia is a scenario of its own. The incidence is as high as thirty percent in very low-birth-weight babies, the incarceration risk is greatest, and the anaesthetic risk of surgery in a small ex-preterm infant is real. Most paediatric surgeons therefore repair a hernia in a premature baby before discharge from the neonatal unit or soon after, balancing the surgical urgency against the need for the infant to be robust enough for anaesthesia and for post-operative apnoea monitoring. [7] [9]
Complications & Pitfalls
The complications of the congenital wall defects follow the bowel and the cavity. After gastroschisis closure, the most important complications are prolonged ileus from the inflammatory peel, the need for long-term parenteral nutrition, intestinal failure and short-bowel syndrome in the complex form, and the rare abdominal compartment syndrome from a closure under too much tension. The outcome is dominated by the state of the bowel at birth, which is why simple and complex gastroschisis have such different courses. [1] [2]
The pitfalls cluster around misclassifying the defect and underestimating the herniae. The classic error is to assume that any defect at the umbilicus is an omphalocele and to miss the bare, uncovered bowel of gastroschisis to the right, which changes the work-up entirely. A second error is to observe an inguinal hernia in the expectation that it will close, when in fact it never does and will incarcerate. A third is to use silver nitrate carelessly on an umbilical granuloma, causing a chemical burn to the surrounding skin, when common salt is safer. [3] [11]
Omphalitis carries its own cascade of complications, from localised cellulitis to septicaemia and necrotising fasciitis. The newborn immune system is immature, and infection of the stump can spread rapidly along the abdominal wall fascia, causing tissue necrosis that needs urgent debridement. The risk factors include home delivery, poor cord care and low birth weight, and the presentation demands a low threshold for intravenous antibiotics and surgical assessment. [12] [11]
Prognosis & Disposition
Gastroschisis has an excellent prognosis in the simple form, with survival over ninety percent in high-income settings and most children establishing full enteral nutrition within weeks of closure. The complex form, with atresia or necrosis, has a longer and harder course with prolonged parenteral nutrition and the risk of short-bowel syndrome, but survival is still good when modern neonatal surgery and nutrition are available. Time to full feeds and the length of the hospital stay are the main markers of severity. [1] [2]
The prognosis of an omphalocele is driven less by the defect itself than by its associated anomalies. When the karyotype is normal and the heart is structurally sound, the outcome after closure or paint-and-wait is good. When the omphalocele is part of a lethal trisomy or a severe cardiac malformation, the prognosis is guarded and the counselling before and after birth reflects that. A giant omphalocele managed conservatively needs months of care but achieves a repairable ventral hernia in most survivors. [5] [6]
Disposition reflects the acuity. A newborn with a wall defect is managed in a tertiary neonatal surgical centre, so a baby born in a rural hospital without surgery is resuscitated, the bowel is protected, and the child is retrieved while the surgical team is mobilised. A child with an uncomplicated inguinal or umbilical hernia is managed as an outpatient with a planned elective repair. The incarcerated inguinal hernia and the omphalitis with cellulitis are the two scenarios that convert an outpatient plan into an emergency admission. [3] [12]
Special Populations
The premature and low-birth-weight infant deserves separate attention for both herniae. These babies have a very high rate of inguinal hernia, up to thirty percent, and the greatest risk of incarceration, so the threshold for repair before or soon after neonatal discharge is low. They also have the highest rate of umbilical hernia, nearly universal, yet these almost all close spontaneously, so the approach remains observation. The balance for the inguinal hernia is the surgical urgency against the anaesthetic risk of operating on a small, ex-preterm baby. [7] [9]
Remote and resource-limited communities face the steepest gradient for the congenital wall defects. A baby born with gastroschisis in a centre without neonatal surgery needs the bowel protected and an urgent retrieval, and the distance and the delay increase the risk of bowel damage and sepsis. Antenatal diagnosis and planned delivery at a tertiary centre, where possible, are the strongest protective measures, and they are an equity issue as much as a clinical one. The rising incidence of gastroschisis in young mothers, who may have the least access to antenatal care, compounds this. [1] [2]
The child with a syndromic omphalocele is a population in its own right. Beckwith-Wiedemann syndrome brings macrosomia, macroglossia and a risk of neonatal hypoglycaemia and Wilms tumour, and Pentalogy of Cantrell combines the omphalocele with a diaphragmatic, cardiac and sternal defect. These children need a coordinated plan that addresses the syndrome alongside the wall defect, and the karyotype and the cardiac assessment direct that plan. [3] [6]
Evidence, Guidelines & Regional Differences
The evidence base for gastroschisis combines systematic reviews of diagnosis and outcome with large cohort studies of surgical technique. A systematic review confirmed that the rising incidence is real and worldwide, that young maternal age is the dominant risk factor, and that outcomes for simple gastroschisis are excellent while complex gastroschisis drives the morbidity through bowel atresia and short-bowel syndrome. The choice between primary closure and a silo with delayed closure remains partly surgeon-dependent, with both approaches widely used. [1] [2]
The guideline-level evidence for the herniae comes from the European Hernia Society and Americas Hernia Society guidelines for umbilical and epigastric herniae, and from the European Paediatric Surgeons Association guideline for inguinal herniae. The umbilical hernia guideline supports observation through the preschool years because most close spontaneously, with repair for those persisting beyond that age. The inguinal hernia guideline and its recent update confirm operative repair as the standard, with the debate centring on the role of laparoscopy and on contralateral exploration rather than on whether to operate. [10] [8]
Regional practice is consistent in principle but varies in access and timing. The pathway of tertiary delivery, bowel protection, surgical closure and parenteral nutrition for the wall defects is universal in high-income settings, while the capacity for antenatal diagnosis and planned delivery varies. For the inguinal hernia, the principle of prompt elective repair is shared across Australia, New Zealand, the United Kingdom and North America, though the exact timing for the ex-preterm neonate and the use of laparoscopic repair differ between centres. [9] [3]
Exam Pearls
Hold one sentence above all others: gastroschisis is bare bowel to the right of a normal cord with no sac and no chromosomal association, while an omphalocele is a covered sac in the midline with the cord on the sac and a high rate of chromosomal and cardiac anomalies. State the action that follows: protect the bowel, resuscitate, and transfer to a tertiary surgical centre, with chromosomal and cardiac work-up reserved for the omphalocele. [3] [6]
Get the herniae facts exactly right. An umbilical hernia is covered by skin, closes spontaneously in most, and is repaired only if it persists beyond age four to five or if the ring is large. An inguinal hernia follows a patent processus vaginalis, never closes on its own, and carries its highest incarceration risk in the first year, so it is referred for prompt elective repair. The umbilical granuloma is treated with common salt or silver nitrate, with salt now favoured for its lower burn risk. [10] [8]
The high-yield pairings do the work in a viva. A covered midline mass with the cord on the sac is an omphalocele that needs a karyotype and echocardiogram before surgical planning. Bare bowel beside a normal cord is gastroschisis that needs bowel protection and silo or primary closure. A reducible groin bulge in a crying infant is an inguinal hernia that needs elective repair, while a tender irreducible groin mass is incarcerated and needs urgent surgery after a single careful attempt at reduction. A cellulitic umbilical stump in a neonate is omphalitis that needs intravenous antibiotics and assessment for necrotising fasciitis. [9] [12]
References
- [1]Ferreira RG; Mendonça CR; Gonçalves Ramos LL; et al Gastroschisis: a systematic review of diagnosis, prognosis and treatment. J Matern Fetal Neonatal Med, 2022.PMID 33899664
- [2]Bhat V; Moront M; Bhandari V Gastroschisis: A State-of-the-Art Review. Children (Basel), 2020.PMID 33348575
- [3]Bence CM; Wagner AJ Abdominal wall defects. Transl Pediatr, 2021.PMID 34189105
- [4]Slater BJ; Pimpalwar A Abdominal Wall Defects. NeoReviews, 2020.PMID 32482700
- [5]Saxena AK; Hayward RK; Mutanen A; et al European Paediatric Surgeons' Association Consensus Statement on the Management of Giant Omphalocele. Eur J Pediatr Surg, 2025.PMID 40389219
- [6]Ayub SS; Taylor JA Cardiac anomalies associated with omphalocele. Semin Pediatr Surg, 2019.PMID 31072458
- [7]Abdulhai S; Glenn IC; Ponsky TA Inguinal Hernia. Clin Perinatol, 2017.PMID 29127966
- [8]Morini F; Dreuning KMA; Janssen Lok MJH; et al Surgical Management of Pediatric Inguinal Hernia: A Systematic Review and Guideline from the European Pediatric Surgeons' Association Evidence and Guideline Committee. Eur J Pediatr Surg, 2022.PMID 33567466
- [9]Morgado M; Holland AJ Inguinal hernias in children: Update on management guidelines. J Paediatr Child Health, 2024.PMID 39319467
- [10]Henriksen NA; Montgomery A; Kaufmann R; et al Guidelines for treatment of umbilical and epigastric hernias from the European Hernia Society and Americas Hernia Society. Br J Surg, 2020.PMID 31916607
- [11]Haftu H; Bitew H; Gebrekidan A; et al The Outcome of Salt Treatment for Umbilical Granuloma: A Systematic Review. Patient Prefer Adherence, 2020.PMID 33154632
- [12]Kaplan RL Omphalitis: Clinical Presentation and Approach to Evaluation and Management. Pediatr Emerg Care, 2023.PMID 36853079