Paeds · gastroenterology-hepatology-and-nutrition
Acute abdominal pain in children
Also known as Acute abdomen · Acute tummy pain · The surgical abdomen · Belly pain in children · Appendicitis assessment · Acute abdominal pain in children
Fellowship guide to acute abdominal pain in children: the disciplined emergency-department approach that separates the surgical abdomen (appendicitis, intussusception, malrotation with volvulus, and the adolescent torsions) from common medical mimics, the migration pattern and pain pathway, the age-based differential, the Pediatric Appendicitis Score and ultrasound-first imaging, resuscitation with early analgesia and antibiotics, enema reduction of intussusception, and the safety-netting that catches the deteriorating child.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who develops abdominal pain over hours rather than weeks demands a different mindset from the clinician than the child with chronic, recurrent pain. The single task is to find the few who have a surgical emergency before ischaemia, perforation or torsion causes irreversible harm, while sparing the majority with self-limiting medical causes the risks of unnecessary imaging and operation. Acute abdominal pain is therefore a problem of disciplined triage rather than exhaustive diagnosis. [2]
Acute abdominal pain in children is most usefully defined as pain of recent onset, evolving over hours to a few days, that is severe enough to bring the child to medical attention and that requires active exclusion of a surgical cause. The boundary with chronic pain matters because it changes the priorities: chronic pain asks the clinician to avoid over-investigation and to make a positive functional diagnosis, whereas acute pain asks the clinician to assume a surgical cause until it is ruled out. The two presentations share a differential, but the order of threat is reversed. [4]
The common surgical emergencies in children are appendicitis, intussusception and malrotation with midgut volvulus, joined in adolescence by ovarian and testicular torsion. Against these stand the frequent medical mimics: gastroenteritis, mesenteric adenitis, constipation, urinary tract infection, lower-lobe pneumonia and functional pain. A confident clinician moves through this list by age, by the character and site of the pain, and by the bedside examination rather than by reflexively ordering panels of tests. [2]
Classification
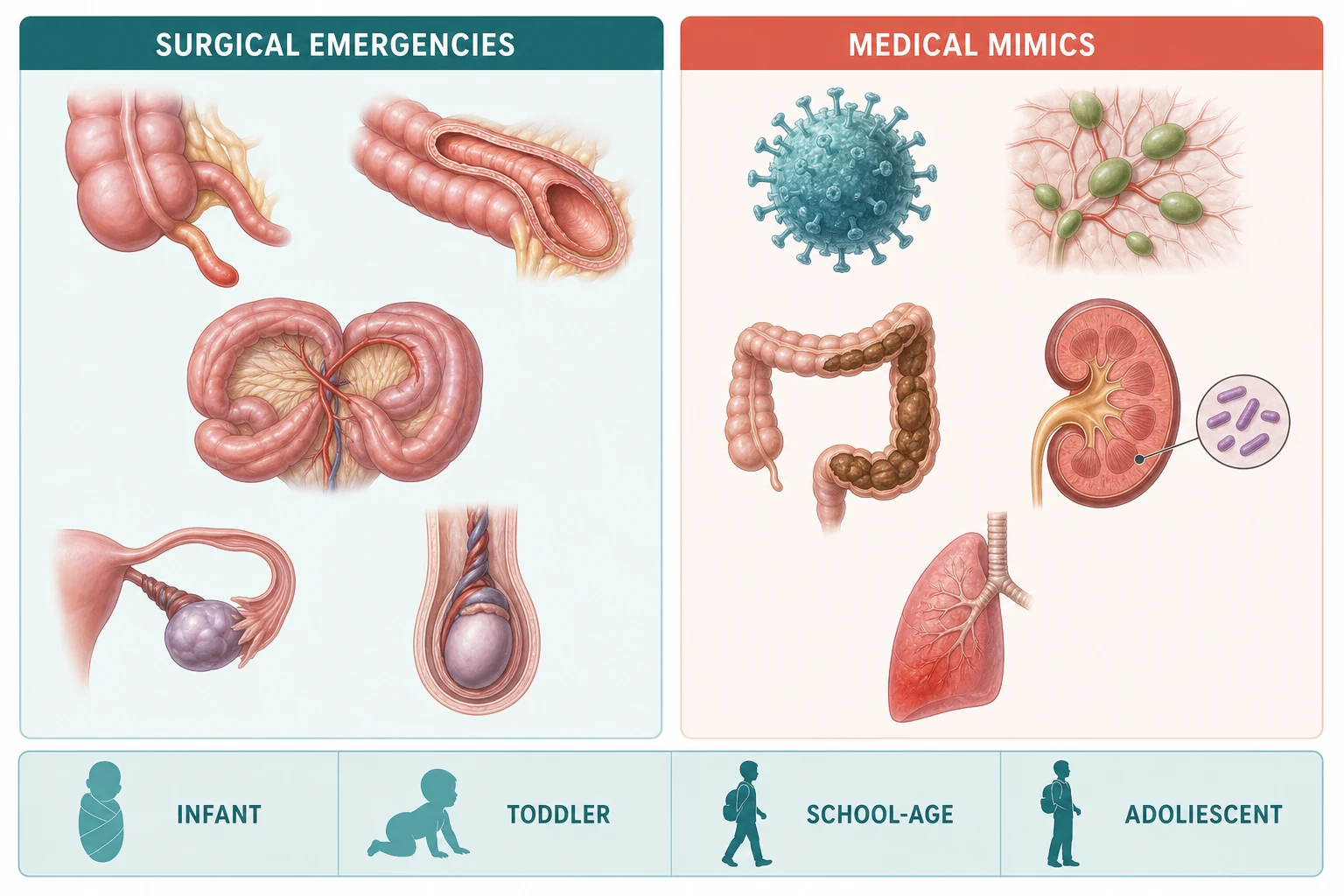
The most useful first split separates the child who needs a surgeon from the child who does not, because it governs everything that follows. Surgical causes threaten bowel or organ viability and demand theatre or an interventional reduction within hours, while medical causes are managed with fluids, analgesia and time. Within each group the age of the child then narrows the likely culprit quickly and reliably. [2]
In the infant the surgical threats are intussusception, malrotation with midgut volvulus, an incarcerated inguinal hernia and necrotising enterocolitis. Appendicitis is rare but does occur and is easily missed at this age because the presentation is non-specific. In the older child appendicitis dominates the surgical differential, with mesenteric adenitis as its closest and most easily confused mimic. [4]
In the adolescent the abdominal differential must always include the gonads. Ovarian torsion, ruptured ovarian cyst and ectopic pregnancy can masquerade as appendicitis or gastroenteritis in girls, while testicular torsion presents with abdominal or groin pain as often as with scrotal pain in boys, so the groin and scrotum are examined in every adolescent with acute abdominal pain. Pregnancy must be excluded with a test in any adolescent girl with acute pain. [10]
[2]Epidemiology & Risk Factors
Acute abdominal pain is one of the most common reasons a child presents to an emergency department, and appendicitis is the most frequent surgical cause of acute abdominal pain in children beyond infancy. Appendicitis peaks in late childhood and early adolescence, between roughly ten and twenty years of age, and is uncommon under five years of age, where its atypical presentation contributes to a higher perforation rate at first presentation. [4]
Intussusception is the most common cause of intestinal obstruction in infants, with the classic age band of three months to three years and a peak between five and nine months. Most cases are idiopathic, attributed to hypertrophied Peyer patches after a viral upper-respiratory or enteric illness, while a pathological lead point such as a Meckel diverticulum or polyp becomes more likely in older children and demands a search for it. [5]
Several factors raise the risk of a missed or delayed diagnosis. Young age, an atypical or absent migration pattern, communication difficulty in children with developmental delay or autism, and language and cultural barriers all delay presentation and diagnosis. Delayed diagnosis of appendicitis is the strongest driver of perforation, which carries higher morbidity, longer admission and a greater risk of intra-abdominal abscess, and much of this delay is preventable. [4]
Pathophysiology
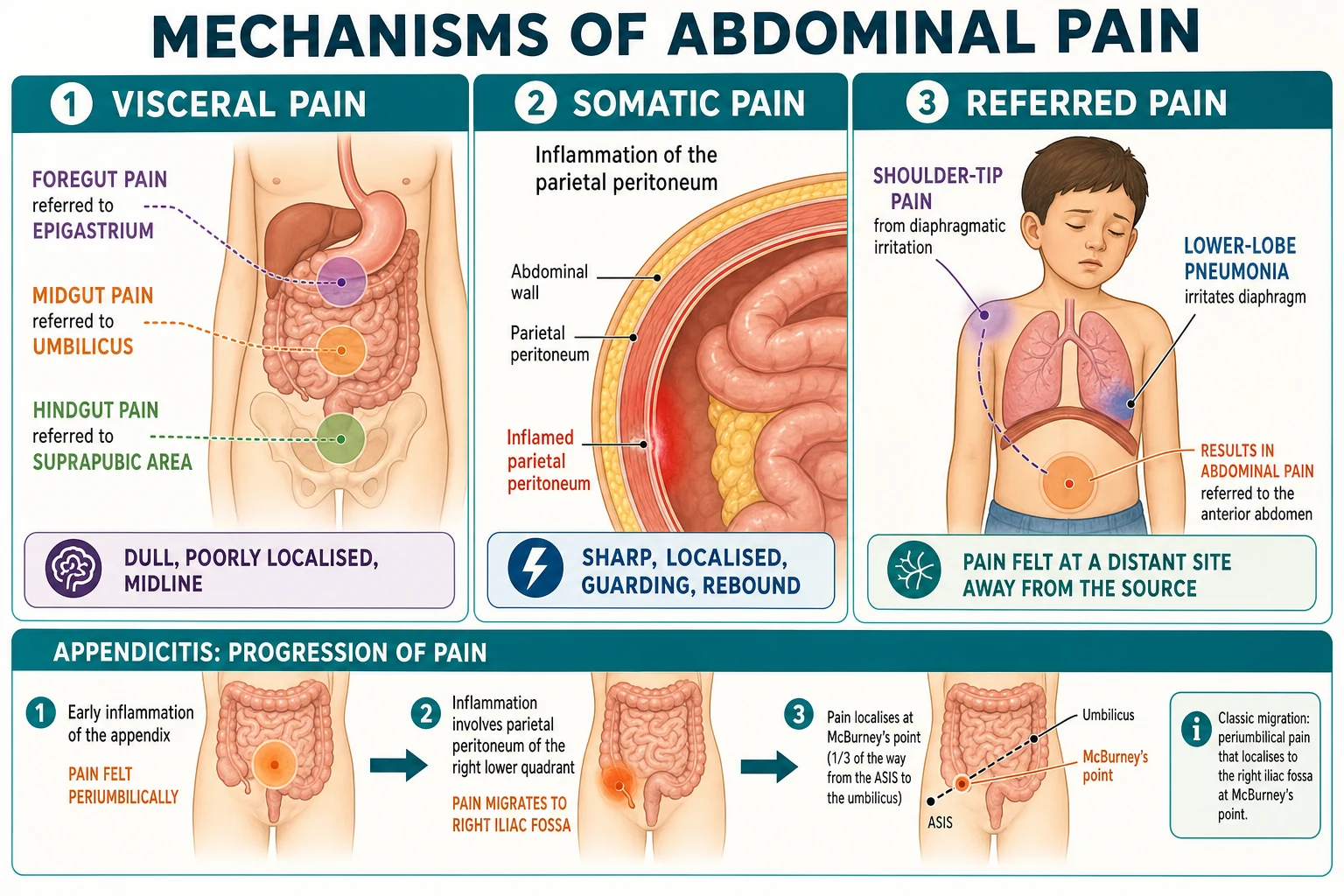
Understanding three pain pathways turns the symptom of abdominal pain into a diagnostic tool. Visceral pain arises from the walls of hollow organs and the visceral peritoneum and is carried by autonomic afferents, so it is dull, poorly localised and felt in the midline according to the embryological origin of the gut. Somatic pain arises from the parietal peritoneum and abdominal wall, which are supplied by spinal segmental nerves, and is sharp, precise and localised to the diseased area. Referred pain is felt at a site distant from the lesion because the lesion and that site share a spinal segment. [2]
The classic migration of appendicitis is the best illustration of this mechanism and the most useful single historical feature. Early obstruction and inflammation of the appendix irritate the midgut visceral afferents, which enter the spinal cord around the tenth thoracic segment, so the pain is felt as a vague central periumbilical ache. As the inflamed appendix touches the parietal peritoneum of the right lower quadrant, the pain sharpens and localises to the right iliac fossa, and the child limps or resists walking. This migration from central to right lower quadrant pain is far more discriminating for appendicitis than pain at a single site. [1]
The natural history of appendicitis runs from luminal obstruction through mucosal inflammation to transmural inflammation, ischaemia, gangrene and finally perforation with purulent or faecal peritonitis. Fever, tachycardia, guarding and rebound appear as the process advances, and the transition from simple to complicated appendicitis is the reason that early recognition and timely operation matter. The same principle of progression to ischaemia governs intussusception and volvulus, where the blood supply is mechanically compromised and delay costs bowel. [4]
Clinical Presentation
The clinical picture of appendicitis is built from a sequence rather than a snapshot. Pain classically begins as a central, dull, periumbilical ache and migrates over twelve to twenty-four hours to the right lower quadrant, where it becomes constant and worse with movement. Anorexia is the most consistent associated symptom, and nausea and low-grade fever follow the pain rather than precede it. Pain that precedes vomiting, rather than vomiting that precedes pain, is the rule in appendicitis and helps separate it from gastroenteritis. [1]
Examination reveals localised tenderness, and the key signs follow from peritoneal irritation: tenderness at McBurney point, pain on coughing, hopping or percussion, and rebound tenderness. Rovsing sign, psoas sign and obturator sign are peritoneal irritation manoeuvres that the candidate should be able to name. Fever and tachycardia reflect progressing inflammation, and guarding or rigidity signals established peritonitis. Atypical presentations are common in the very young, where diarrhoea, lethargy and fever may dominate and the focal signs are absent or late. [1]
Intussusception presents differently because it is an obstructive rather than an inflammatory process in an infant. The cardinal features are episodic, colicky abdominal pain during which the infant draws up the legs and goes pale, followed by vomiting that becomes bilious, and the eventual passage of redcurrant-jelly stool. The classic triad of colicky pain, vomiting and bloody stool is present in only a minority at first presentation, so its absence never excludes the diagnosis. Between attacks the infant may appear deceptively well, and a sausage-shaped mass may be palpable in the right upper quadrant. [5]
Malrotation with midgut volvulus announces itself with bilious vomiting and pain in an infant, and the urgency comes from the risk of mesenteric ischaemia. Ovarian torsion in an adolescent girl causes sudden, severe, unilateral lower abdominal pain with nausea and vomiting, while testicular torsion in a boy may present as abdominal or groin pain rather than scrotal pain, which is why the scrotum is examined in any boy with acute abdominal pain. [10]
High-yield features to elicit in the history
Onset and timing: did the pain precede or follow the vomiting
Character and site: dull periumbilical ache migrating to the right iliac fossa
Aggravation by movement, coughing, hopping or walking
Associated anorexia, nausea, fever, diarrhoea or urinary symptoms
Quality of vomit: bilious, projectile, or bloody
For adolescents: menstrual history, sexual history and a pregnancy test
Differential Diagnosis
A broad differential is best disciplined by working through the common and the dangerous together, rather than by listing every rare cause. The dangerous conditions share a thread of mechanical obstruction or torsion that compromises blood supply and demands action within hours: appendicitis, intussusception, malrotation with volvulus, and ovarian and testicular torsion. The common medical causes, in contrast, settle with supportive care. [2]
Gastroenteritis is the most frequent mimic and is suggested by vomiting and diarrhoea that precede or accompany the pain, a benign abdomen and a self-limiting course. Mesenteric adenitis, lymphadenitis of the mesenteric nodes after a viral illness, closely resembles appendicitis with right lower quadrant pain and fever, and is largely a diagnosis of exclusion reached when appendicitis has been confidently ruled out. Constipation causes cramping abdominal pain with a loaded rectum and is easily overlooked. [2]
Extra-intestinal causes must stay on the differential because they are missed when attention stays fixed on the abdomen. Lower-lobe pneumonia causes referred abdominal pain through the lower thoracic nerves, urinary tract infection causes abdominal pain with dysuria and frequency, and diabetic ketoacidosis causes abdominal pain with deep sighing breathing and dehydration. In the infant, an incarcerated inguinal hernia and necrotising enterocolitis must be considered, and in the adolescent girl ectopic pregnancy, pelvic inflammatory disease and a ruptured ovarian cyst are added to ovarian torsion. [4]
Clinical & Bedside Assessment
The history and examination are the highest-yield tools in the acute abdomen and remain more important than any single investigation. The clinician characterises the pain by onset, site, migration, character, aggravation by movement and relationship to vomiting, then screens for systemic features of fever, anorexia and dehydration. A full abdominal and groin examination completes the bedside assessment. [2]
Abdominal examination begins with inspection for distension and scars, proceeds to gentle palpation for tenderness, guarding, rigidity, masses and organomegaly, and ends with auscultation for bowel sounds. The examiner must palpate the hernial orifices in every child and examine the testes in every boy, because a torsed testis in the abdomen or groin is easily missed when the scrotum is not checked. A digital rectal examination is rarely needed in children and is avoided as a routine, though inspection for fissures, skin tags or perianal disease is appropriate when indicated. [2]
General examination is not optional. Plot or estimate the weight for drug dosing, assess hydration and perfusion from capillary refill, pulse and skin temperature, and look for pallor, jaundice, rashes such as the purpura of Henoch-Schonlein purpura, and respiratory signs that point to pneumonia. Serial observation is itself an investigation: a child who is re-examined over several hours reveals whether the pain is settling, as in mesenteric adenitis, or sharpening and localising, as in appendicitis. [1]
Investigations
Investigation supports a clinical diagnosis rather than replacing it, and the guiding principle in children is to image with ultrasound first and to avoid computed tomography whenever possible because of the lifetime cancer risk from ionising radiation. Blood tests confirm inflammation and guide resuscitation but seldom make the diagnosis on their own, and over-investigation of the clearly medical child is a recognised pitfall. [2]
In suspected appendicitis, the Pediatric Appendicitis Score combines eight clinical and laboratory variables into a ten-point score that stratifies the child's risk and rationalises the decision to observe, image or call a surgeon. The components are right lower quadrant tenderness and pain on coughing, hopping or percussion, each worth two points, and migration of pain, anorexia, nausea or vomiting, fever, leukocytosis and neutrophilia, each worth one point. In the original study a score of six or more was highly suggestive of appendicitis, while in practice a low score supports discharge with safety-netting, a high score prompts surgical referral, and an equivocal score prompts ultrasound or a period of observation. [1]
Ultrasound is the first-line imaging modality in suspected appendicitis, and a systematic review has confirmed its accuracy even when performed by non-radiologists, supporting a frontline role in emergency settings. Computed tomography is more sensitive but is reserved for cases where ultrasound is equivocal and the child remains a diagnostic concern, and magnetic resonance imaging is an alternative in some centres to avoid radiation. A target sign on ultrasound, the target lesion or doughnut of intussusception, confirms that diagnosis and precedes enema reduction. [8]
For the unwell or potentially surgical child, baseline bloods include a full blood count, C-reactive protein, urea, electrolytes and creatinine, a venous gas and glucose to exclude diabetic ketoacidosis, and a group and hold if operation is likely. A urinalysis and urine culture exclude infection, and a pregnancy test is mandatory in any adolescent girl before imaging. Imaging for intussusception is ultrasound, and contrast or pneumatic enema serves as both the diagnostic confirmation and the therapeutic reduction in the stable child. [5]
Management — Resuscitation
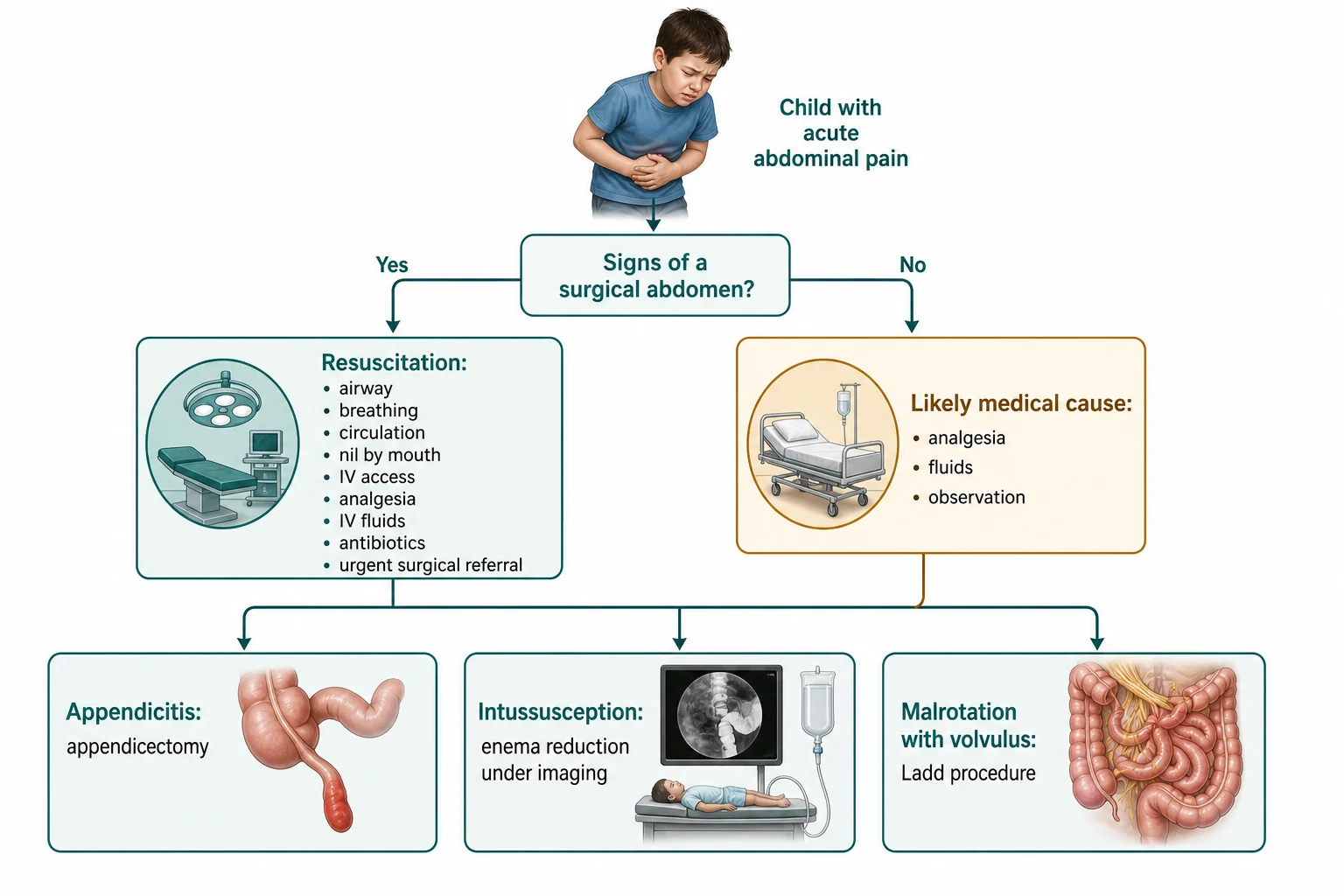
A child with a surgical abdomen or shock is resuscitated along airway, breathing and circulation lines in parallel with the surgical referral, and the surgical call is made early rather than after every test returns. The child is kept nil by mouth, intravenous access is secured, analgesia is given, fluid is started for dehydration or shock, and bloods are taken. A nasogastric tube decompresses the stomach in obstruction, and a urinary catheter guides fluid resuscitation in the shocked child. [2]
Early analgesia is a standard of care and is given without delay, because the fear that opioids mask the surgical abdomen and delay diagnosis is unfounded. A review of studies in children with undifferentiated abdominal pain found that opioid analgesia provided effective pain relief without changing the accuracy of examination or the rate of correct diagnosis, so withholding analgesia to preserve the abdominal signs is neither necessary nor defensible. The dose is titrated to comfort and the child is reassessed after each dose. [3]
Intravenous fluid resuscitation uses an isotonic crystalloid such as normal saline or a balanced solution. A child in shock receives a bolus of ten to twenty millilitres per kilogram, repeated as guided by clinical response, and dehydration is corrected with isotonic maintenance fluid while electrolytes are checked. Glucose is checked and treated in every seriously unwell child, and antibiotics that cover enteric Gram-negative organisms and anaerobes are given once sepsis, perforation or peritonitis is suspected, before theatre. [2]
Morphine for acute abdominal pain (titrated)
Dose
0.1 to 0.2 mg per kg intravenously, repeated as needed to comfort, in a child with a suspected surgical abdomen
Resuscitation priorities in the surgical abdomen
Assess airway, breathing, circulation and perfusion in parallel
Keep nil by mouth; secure intravenous access and send bloods
Give early titrated analgesia; do not withhold it
Fluid bolus of 10 to 20 mL per kg isotonic crystalloid for shock, repeated to response
Check glucose; give antibiotics for sepsis, perforation or peritonitis
Decompress with a nasogastric tube in obstruction; call the surgeon early
Management — Definitive & Stepwise
Definitive treatment depends on the diagnosis and the child's stability, and the pathway is built around the principle that the surgical child reaches theatre promptly while the medical child is supported and observed. For appendicitis the standard treatment has long been prompt appendicectomy, and the World Society of Emergency Surgery guidelines reaffirm surgery as the reference standard while recognising a role for antibiotics in selected uncomplicated cases. [2]
The place of antibiotics alone in uncomplicated appendicitis is an active question, and a Cochrane review comparing appendicectomy with antibiotic treatment found that antibiotics can avoid operation in a proportion of children but carry a higher risk of recurrence and subsequent appendicectomy, so surgery remains the definitive option and antibiotics are reserved for selected patients or when an operation is contraindicated. The candidate should present this as a nuanced, shared decision rather than a simple either-or. [9]
For complicated appendicitis with perforation, peritonitis or abscess, intravenous antibiotics and source control are central, and a contained abscess may be drained radiologically before or instead of immediate operation. For intussusception, the stable child is reduced by pneumatic or hydrostatic enema under fluoroscopic or ultrasound guidance, and a meta-analysis found pneumatic and liquid enema reduction broadly comparable, with choice guided by local expertise and resources. [6]
Surgery is required for intussusception when the child is shocked, has peritonitis or has failed enema reduction, and predictors of failed enema reduction identified in a systematic review guide the surgical decision. For malrotation with midgut volvulus the operation is the Ladd procedure, with detorsion of the volvulus, division of Ladd bands, widening of the mesenteric base, removal of the appendix and correct placement of the bowel, and both open and laparoscopic approaches are safe and effective. [7]
[6]Specific Subtypes & Scenarios
Appendicitis in the very young child is the scenario most prone to error, because the classic sequence is often absent and fever, diarrhoea and irritability may be the only clues. Perforation is consequently more common at first presentation under five years of age, and a low threshold for ultrasound and surgical review in the unwell young child is the safeguard. A short period of structured observation and re-examination distinguishes the child whose pain is settling from the child whose pain is sharpening. [4]
Intussusception in the infant demands confidence in the diagnosis and the reduction pathway. The cardinal history of intermittent colicky pain with drawing up of the legs, pallor and vomiting is followed by redcurrant-jelly stool only late, and a sausage-shaped mass may be felt in the right upper quadrant. Ultrasound shows the target sign, and the stable child proceeds to pneumatic or liquid enema reduction, reserving surgery for the unstable child, peritonitis or failed reduction. [5]
Malrotation with midgut volvulus presents with bilious vomiting and abdominal pain in an infant and is a time-critical surgical emergency because a volvulus can infarct the entire midgut within hours. The response is nil by mouth, nasogastric decompression, fluid resuscitation and an urgent surgical opinion, with an upper gastrointestinal contrast study confirming the diagnosis in the stable child and theatre proceeding without imaging in the child with peritonitis. Definitive treatment is the Ladd procedure. [7]
Ovarian torsion in the adolescent girl causes sudden severe lower abdominal pain with nausea and vomiting, and the diagnosis is urgent because the ovary becomes non-viable within hours. Pelvic ultrasound with Doppler is the investigation of choice, and a negative or equivocal scan does not exclude torsion, so a high clinical suspicion prompts urgent gynaecological assessment and laparoscopy. Testicular torsion in the adolescent boy may present with abdominal or groin pain, and the scrotum must be examined in every boy with acute abdominal pain so that a salvageable testis is not lost. [10]
[2]Complications & Pitfalls
The complications of acute abdominal pain are chiefly those of delayed recognition of a surgical cause. Perforation of the appendix with peritonitis and intra-abdominal abscess is the most common serious complication, and it lengthens the admission and raises the morbidity through sepsis, ileus and adhesive obstruction. The loss of bowel or a gonad from delayed recognition of volvulus or torsion is rarer but catastrophic, and is the reason these diagnoses are treated as time-critical. [4]
Iatrogenic harm arises in two opposite directions. The first is the missed surgical diagnosis, where atypical features, young age or communication difficulty lead to a label of gastroenteritis and discharge, and the perforated appendix or torsed organ is found too late. The second is the negative appendicectomy and the radiation exposure from unnecessary computed tomography, which carry their own harms. A study of delayed appendicitis diagnosis found that a substantial proportion of cases were preventable with better recognition of the clinical features, underlining that clinical skill, not more scanning, is the chief safeguard. [4]
The classic pitfalls cluster around false reassurance. A normal early examination in appendicitis does not exclude it, because the focal signs develop as the inflammation reaches the parietal peritoneum, and the child who is sent home must be re-examined if the pain worsens or localises. Redcurrant-jelly stool in intussusception is a late sign, and its absence must never be used to exclude the diagnosis. Bilious vomiting is always pathological and is never dismissed as feeding difficulty. [5]
Prognosis & Disposition
The outlook is excellent when the diagnosis is made promptly. Children with simple appendicitis recover quickly after appendicectomy and most return home within days, while the majority of children with medical causes such as gastroenteritis or mesenteric adenitis settle with supportive care. The prognostic lever across the whole topic is timeliness: the earlier the surgical cause is recognised, the lower the rate of perforation and the shorter the recovery. [4]
Disposition follows the diagnosis and the response to treatment. A child with a clear surgical diagnosis, peritonitis or shock is admitted for operation, while a child with an equivocal presentation is observed with serial examination and a plan that specifies the threshold for imaging, surgical review and return. A child with a confident medical diagnosis, a benign abdomen, adequate hydration and a reliable family is discharged with clear, written safety-netting. [2]
The safety-net is the single most important discharge tool and is communicated in plain language. The family is told to return immediately if the pain worsens, localises or becomes constant, if the vomit turns green or bloody, if the child becomes drowsy, floppy or feverish, or if the child cannot keep fluids down or stops passing urine. Asking the family to repeat the warning signs back confirms understanding and is the best protection against a missed deterioration at home. [2]
Special Populations
Children with developmental disability or autism may be unable to localise or describe pain in the expected way, and their discomfort may show as agitation, self-injury, change in routine or refusal to eat. Assessment is adapted to the child's communication, carers are asked to interpret changes from baseline, and a lower threshold for imaging and senior review compensates for the less reliable examination. These children are over-represented among those with delayed diagnosis. [4]
Migrant and refugee families, and families facing socioeconomic disadvantage, may present late because of language barriers, financial cost, distance from care or unfamiliarity with the health system. Interpreter services are used routinely rather than relying on family members, transport and financial barriers are addressed practically, and the safety-net is given in the family's language in writing. Late presentation raises the risk of perforation and complications and makes these children a priority for thorough assessment. [4]
Adolescents need the abdominal and gynaecological differential applied in full. Pregnancy is excluded with a test before imaging, sexual and menstrual history are taken sensitively and confidentially, and ovarian torsion, ectopic pregnancy and pelvic inflammatory disease join appendicitis on the list. Testicular torsion is excluded by examining the scrotum in every adolescent boy. Confidentiality, consent and a non-judgemental approach build the trust needed for an accurate history. [10]
[5]Evidence, Guidelines & Regional Differences
The 2025 World Society of Emergency Surgery Jerusalem guidelines provide the current international reference for the diagnosis and treatment of acute appendicitis, reaffirming clinical assessment and ultrasound, setting the place of computed tomography and magnetic resonance imaging, and defining the role of antibiotics alongside appendicectomy. They are the standard against which local protocols are written. [2]
The Pediatric Appendicitis Score, published in 2002, remains the most widely used paediatric risk-stratification tool, and its components and thresholds are examined directly. The evidence on analgesia, established by reviews including a paediatric synthesis of four studies, settles the older debate: opioid analgesia relieves pain in children with acute abdominal pain without reducing diagnostic accuracy, and its early use is now standard practice. Imaging evidence continues to favour ultrasound first, with a systematic review confirming acceptable accuracy even for non-radiologist-performed scans. [3]
[2]Controversies and regional differences remain. The choice between prompt appendicectomy and a trial of antibiotics for uncomplicated appendicitis is debated and a Cochrane review finds antibiotics avoid some operations at the cost of recurrence, so practice varies between centres and is individualised. The optimal method of enema reduction for intussusception, pneumatic or liquid, varies by local expertise, and access to paediatric surgeons and interventional radiology differs between regions and countries. The consistent thread is that recognition of the surgical abdomen and timely action are the non-negotiable priorities everywhere. [9]
Exam Pearls
MIGRATE for the appendicitis history
References
- [1]Samuel M Pediatric appendicitis score. J Pediatr Surg, 2002.PMID 12037754
- [2]Podda M, Ceresoli M, De Simone B, Fugazzola P, Coccolini F, Montori G, Compagnoni M, et al. Diagnosis and Treatment of Acute Appendicitis: 2025 Edition of the World Society of Emergency Surgery Jerusalem Guidelines. JAMA Surg, 2026.PMID 41604201
- [3]Sharwood LN, Babl FE The efficacy and effect of opioid analgesia in undifferentiated abdominal pain in children: a review of four studies. Paediatr Anaesth, 2009.PMID 19453578
- [4]Michelson KA, Reeves SD, Grubenhoff JA, Cruz AT, Harper MB, Bachur RG, Neuman MI Clinical Features and Preventability of Delayed Diagnosis of Pediatric Appendicitis. JAMA Netw Open, 2021.PMID 34463745
- [5]Kim PH, Hwang J, Yoon HM, Lee JY, Kim JR, Jung AY, Kim KM Predictors of failed enema reduction in children with intussusception: a systematic review and meta-analysis. Eur Radiol, 2021.PMID 33974147
- [6]Qafesha RM, Sharabati I, Kashbour M, Elbadry M, Slim M, Elshimi T, Negida A, Ismail K, Luai A, Elhadi M, Elfil M Pneumatic versus liquid enema reduction in the management of pediatric intussusception: an updated systematic review and meta-analysis. Ann Med Surg (Lond), 2025.PMID 41180717
- [7]Lang Y, Chen Q, Wu M, Chen G, Zhang Y, Wu M Laparoscopic Vs Open Ladd's Procedure for Intestinal Malrotation in Infants and Children: A Systematic Review and Meta-Analysis. Surg Innov, 2026.PMID 42264504
- [8]Oh SK Diagnostic Accuracy of Non-Radiologist-Performed Ultrasound for Diagnosing Acute Appendicitis in Pediatric Patients: A Systematic Review and Meta-Analysis. Medicina (Kaunas), 2025.PMID 40731937
- [9]Doleman B, Fonnes S, Lund JN, Boyd-Carson H, Vimalachandran D, Abercrombie J, Mohiuddin M, et al. Appendectomy versus antibiotic treatment for acute appendicitis. Cochrane Database Syst Rev, 2024.PMID 38682788
- [10]Newman M, Smith T, Hammond P Paediatric and adolescent ovarian torsion: a eight-year retrospective cohort study and literature review. Acta Chir Belg, 2025.PMID 41217937