Paeds · gastroenterology-hepatology-and-nutrition
Acute gastroenteritis and infectious diarrhoea
Also known as Acute gastroenteritis · AGE · Infectious diarrhoea · Gastro · Viral gastroenteritis · Rotavirus gastroenteritis · Norovirus · Dysentery · Bloody diarrhoea · Acute diarrhoea · Diarrhoea and vomiting · Dehydration in children
Fellowship guide to acute gastroenteritis and infectious diarrhoea in children: the commonest reason a child becomes acutely dehydrated, and the condition in which getting rehydration right saves lives while over-investigation and needless drugs do harm. The page covers the viral, bacterial and parasitic causes and the split between watery and bloody diarrhoea, the mechanism by which fluid is lost and the reason oral rehydration solution works through the intact sodium-glucose co-transporter, the disciplined clinical assessment of dehydration, the evidence that oral rehydration therapy beats intravenous fluids for most children, and the layered management of rehydration, early feeding, zinc, ondansetron and the narrow indications for antibiotics, with rotavirus vaccine as prevention.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A toddler is brought in after two days of watery diarrhoea and vomiting. He has stopped eating, his nappies are drier than usual, and his mother is frightened. This is one of the commonest presentations in paediatrics, and the whole art of managing it lies in a single question: how dehydrated is this child, and can I put the fluid back safely by mouth? Everything else — the stool cultures, the antiemetics, the antibiotics — is secondary to answering that. [1] [2]
Acute gastroenteritis is an inflammation of the stomach and intestine, usually infectious, that causes a sudden increase in stool frequency or looseness, often with vomiting, fever and abdominal pain, and lasting less than two weeks. The clinical danger is not the infection itself, which is usually self-limiting, but the dehydration and electrolyte disturbance that follow the loss of water and salt in the stool and vomit. [2] [1]
The examiner's framework is simple and durable. Decide whether the child is dehydrated and how badly, rehydrate by the safest effective route, feed early, add the few adjuncts that help — zinc and, for the vomiting child, ondansetron — and reserve antibiotics for the narrow group who need them. Prevention through the rotavirus vaccine sits alongside treatment as the other half of the story. [1] [9]
Classification
Sort infectious diarrhoea first by the character of the stool, because watery and bloody diarrhoea point to different organisms and different management. Then sort by duration, since anything beyond fourteen days leaves the acute pathway and becomes persistent or chronic diarrhoea with its own work-up. These two axes, stool character and duration, do most of the clinical thinking before any test is sent. [2] [1]
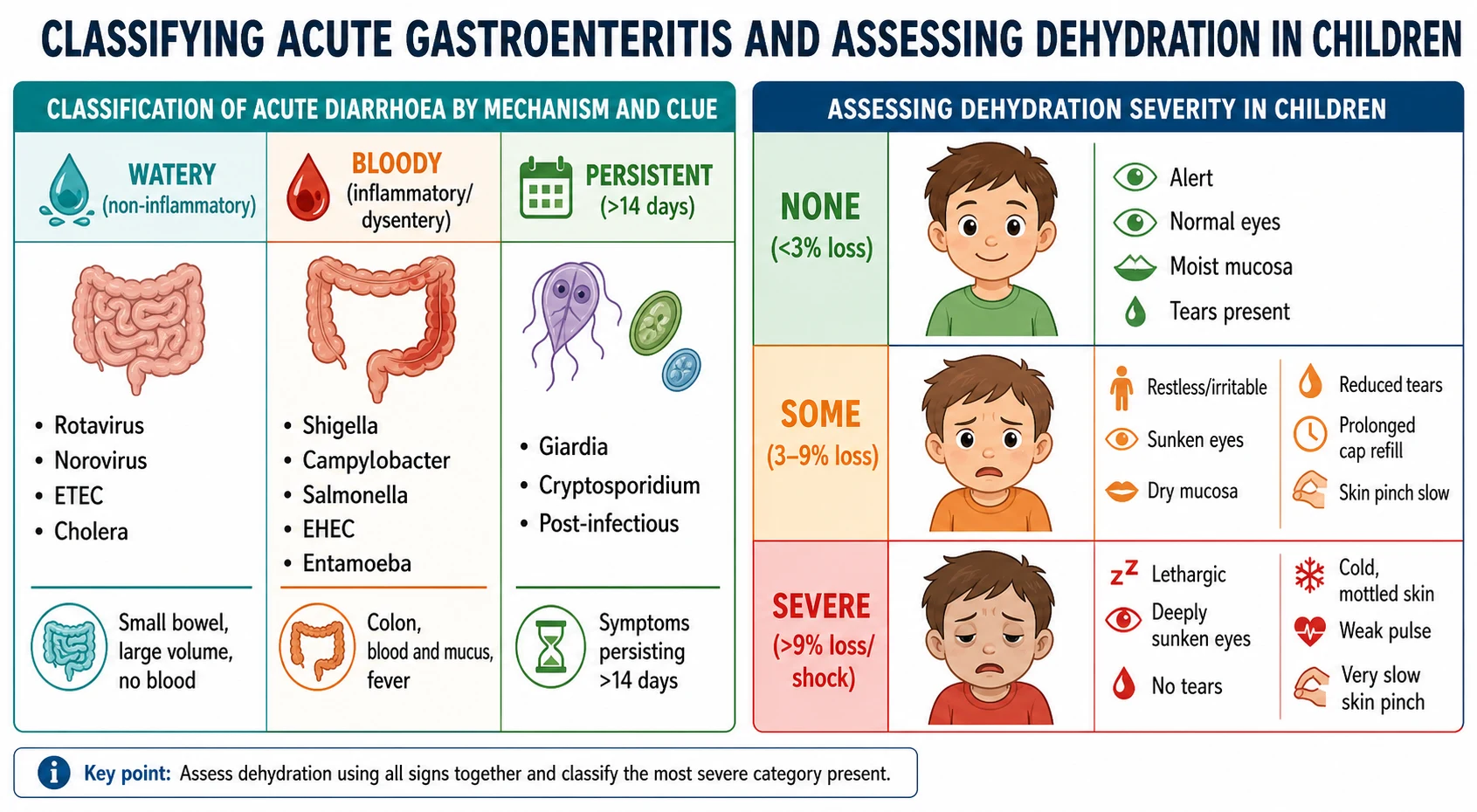
Watery diarrhoea, the commoner picture, comes from the small bowel and is usually viral. Rotavirus and norovirus dominate in children, with enterotoxigenic Escherichia coli and, in endemic settings, cholera producing the same high-volume watery losses. The stool has no blood, the illness is self-limiting, and the entire management is rehydration. This is the group in which oral rehydration therapy shines. [2] [8]
Bloody diarrhoea, or dysentery, comes from the colon and signals an invasive or Shiga-toxin-producing organism such as Shigella, Campylobacter, non-typhoidal Salmonella, enterohaemorrhagic Escherichia coli or Entamoeba histolytica. Blood and mucus with fever mark this group, and it is the one in which the antibiotic decision matters and in which enterohaemorrhagic Escherichia coli carries the specific threat of haemolytic uraemic syndrome. [11] [1]
Watery (non-inflammatory)
- Small bowel; large volume, no blood
- Rotavirus, norovirus, ETEC, cholera
- Self-limiting; management is rehydration
- Oral rehydration therapy is the mainstay
Bloody (inflammatory/dysentery)
- Colon; blood and mucus, fever
- Shigella, Campylobacter, Salmonella, EHEC, Entamoeba
- Antibiotic decision matters here
- EHEC risks haemolytic uraemic syndrome
Persistent (over 14 days)
- Leaves the acute pathway
- Giardia, Cryptosporidium, post-infectious
- Consider malnutrition and immune deficiency
- Needs a different work-up
Epidemiology & Risk Factors
Diarrhoeal disease remains one of the leading causes of death in young children worldwide, despite being almost entirely preventable and treatable, and the global burden studies keep it near the top of the under-five mortality list. Most of those deaths are from dehydration that was never corrected, which is why the humble sachet of oral rehydration salts is one of the highest-impact interventions in child health. [10] [12]
The organisms shift with age, season and setting. Rotavirus was the classic cause of severe dehydrating diarrhoea in infants and toddlers, and norovirus is now prominent where rotavirus vaccine is in use; bacterial dysentery from Shigella and enterotoxigenic Escherichia coli carries a heavy burden in low-income settings. Young age, especially the first two years, and any degree of malnutrition sharply increase the risk of severe disease and death. [11] [10]
Transmission is faecal-oral, so the risk factors are those of contaminated water, poor sanitation, crowding and inadequate hand hygiene, and outbreaks follow in childcare centres, households and after floods or disasters. In Australia, New Zealand and comparable settings the disease is usually milder and rarely fatal, but it remains a common reason for presentation and admission, and it falls hardest on Indigenous, rural, remote and socioeconomically disadvantaged children. [10] [11]
Pathophysiology
To understand why a child with diarrhoea becomes dehydrated, and why oral rehydration solution rescues them, follow the water. The figure traces the whole chain from the ingested pathogen to dehydration and shows the point at which oral rehydration therapy intervenes. The core problem is a net loss of water and electrolytes from the gut that outpaces what the child can take in. [2] [8]
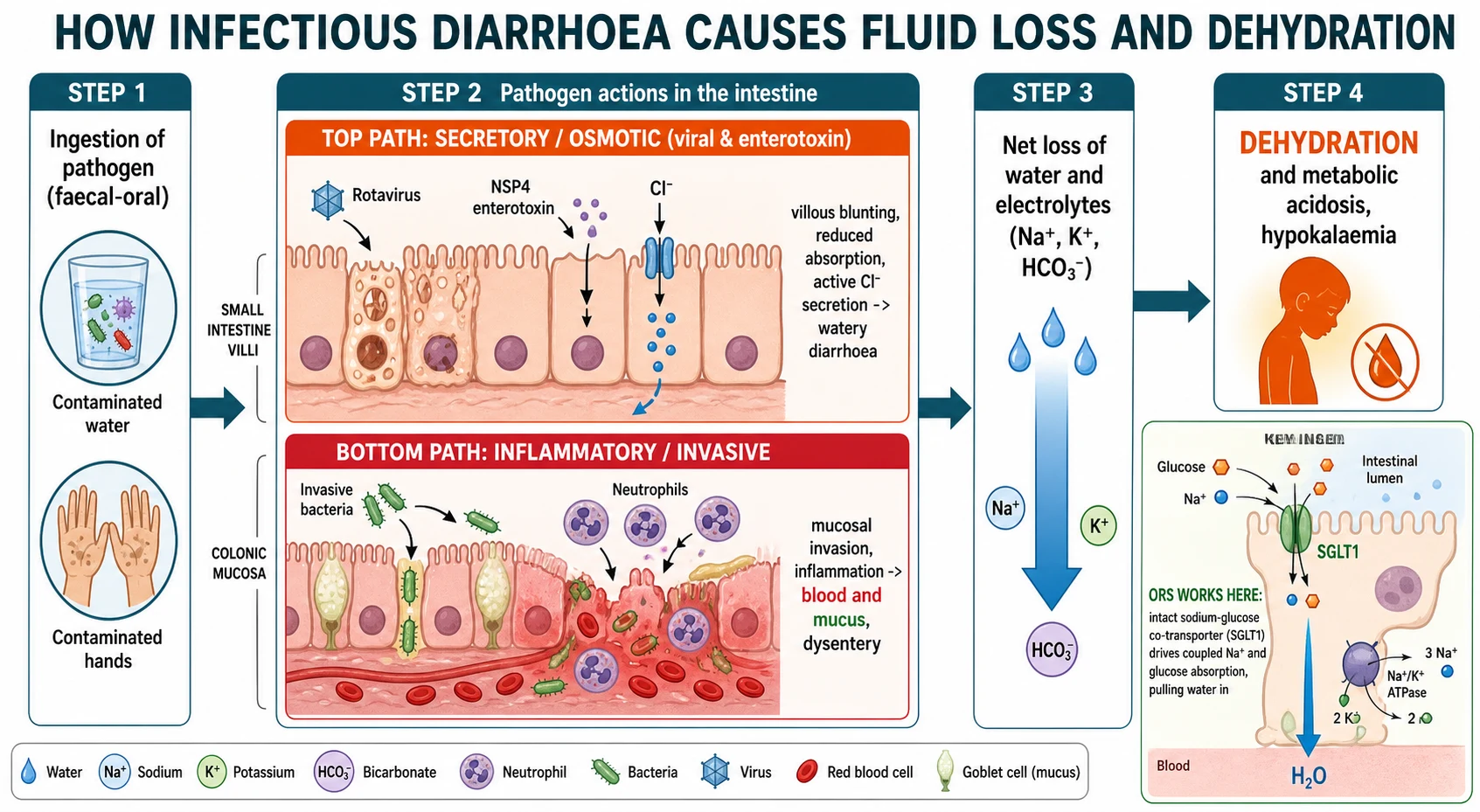
Viral and enterotoxigenic diarrhoea is mostly secretory and osmotic. Rotavirus damages the absorptive enterocytes at the villous tips and its NSP4 protein acts as an enterotoxin, so absorption falls while active chloride and water secretion rises, giving the large-volume watery stool with no blood. The gut is losing fluid faster than the child can drink, and the losses are rich in sodium, potassium and bicarbonate. [8] [2]
Invasive and Shiga-toxin organisms cause an inflammatory, colonic picture instead. Shigella, Campylobacter and enterohaemorrhagic Escherichia coli invade or injure the colonic mucosa, drawing in neutrophils and producing the blood and mucus of dysentery, often with fever and cramping. Enterohaemorrhagic Escherichia coli additionally releases Shiga toxin, which can damage the endothelium and precipitate haemolytic uraemic syndrome. [11] [1]
The consequences of the fluid loss are predictable. Loss of water and sodium contracts the circulating volume and, if unchecked, leads to shock; loss of bicarbonate in the stool produces a metabolic acidosis, seen clinically as the deep sighing breathing of acidotic children; and loss of potassium causes hypokalaemia. Rehydration corrects all three by restoring volume and letting the kidney do the fine tuning. [1] [2]
Clinical Presentation
The typical child has the sudden onset of loose or watery stools with vomiting, often with a low-grade fever and crampy abdominal pain, and a clear history of contact or an unwell sibling. Vomiting frequently comes first and then settles as the diarrhoea takes over, and the whole illness usually runs its course over several days to a week. The task at the bedside is less to prove the diagnosis, which is clinical, than to gauge how much fluid the child has lost. [2] [1]
Dehydration is read from the child, not from a formula. The most useful signs are a prolonged capillary refill time, abnormal skin turgor with a slow skin pinch, an abnormal or deep breathing pattern from acidosis, sunken eyes, absent tears, dry mucous membranes and reduced urine output, and the more of these that are present, the greater the fluid deficit. A general impression of a lethargic, floppy or inconsolable child weighs heavily. [3] [4]
Weigh the child if a recent well weight is available, because the difference is the most objective measure of the deficit, but never delay rehydration to chase it. Remember that a child can be significantly dehydrated with deceptively few signs early on, and that an obese child or one with hypernatraemia may look better hydrated than they are, so err towards treating rather than under-treating. [3] [1]
Differential Diagnosis
The first and most important fork is whether this really is gastroenteritis or a more dangerous mimic wearing its clothes. Vomiting and abdominal pain are the great pretenders: appendicitis, intussusception, malrotation with volvulus, a urinary tract infection, diabetic ketoacidosis, raised intracranial pressure and even pneumonia can all present with vomiting and loose stools in a child. Diarrhoea that is truly the dominant symptom makes gastroenteritis far more likely than any of these. [1] [2]
Within infectious diarrhoea, use the stool to sort the organism. Watery diarrhoea without blood points to a virus or an enterotoxigenic bacterium and needs only rehydration; bloody diarrhoea with fever points to an invasive or Shiga-toxin organism and changes the antibiotic and complication calculus; and diarrhoea persisting beyond fourteen days points to Giardia, Cryptosporidium or a post-infectious or malabsorptive process and leaves the acute pathway. [11] [2]
Simple gastroenteritis
- Diarrhoea is the dominant symptom
- Contact history or unwell sibling
- Soft, non-focal abdomen
- Self-limiting; needs rehydration only
Surgical/serious mimic
- Bilious vomiting, focal or severe abdominal pain
- Intussusception, volvulus, appendicitis, obstruction
- Distension, tenderness, absent bowel sounds
- Needs imaging and a surgical opinion
Non-gut source
- Vomiting out of proportion to diarrhoea
- Urinary tract infection, diabetic ketoacidosis, pneumonia
- Raised intracranial pressure, sepsis
- Look for the primary source before labelling gastro
Non-infectious causes of acute diarrhoea round out the list and are worth a thought when the story is atypical. Antibiotic-associated diarrhoea, a first presentation of inflammatory bowel disease, a food allergy or intolerance, and drug or toxin effects can all mimic infectious gastroenteritis, and the clue is usually in the history rather than the stool. When in doubt, the safe rule is to exclude the dangerous surgical and metabolic mimics first. [2] [1]
Clinical & Bedside Assessment
The assessment is a focused history and examination aimed squarely at hydration and at excluding the mimics. Ask about the number and character of stools, whether there is blood, the frequency of vomiting and whether it is bilious, the child's fluid intake and urine output, and any contact, travel or antibiotic history. A validated clinical dehydration scale, scoring general appearance, eyes, mucous membranes and tears, helps translate these signs into a grade and a plan. [4] [3]
Examine the abdomen deliberately to exclude the surgical mimics: look for distension, focal tenderness, guarding, a mass or absent bowel sounds, and note bilious vomiting. Check for the signs that point elsewhere, such as a urinary source, ketotic breath or respiratory distress, and assess conscious level and perfusion. This examination is what separates the child who needs rehydration from the one who needs a surgeon or a resuscitation bay. [1] [2]
Investigations
Most children with gastroenteritis need no investigations at all, and this is a genuine examination point. The diagnosis is clinical, the illness is self-limiting, and routine bloods and stool tests neither change management nor benefit the well-hydrated child, so they should be avoided. Investigation is targeted to the child who is severely dehydrated, who is not responding as expected, or who has red flags. [1] [2]
Blood tests earn their place in the sick or severely dehydrated child. Measure electrolytes, urea, creatinine and glucose when a child needs intravenous fluids, when dehydration is severe, or when the clinical picture suggests a sodium disturbance, because hypernatraemic and hyponatraemic dehydration change the rehydration plan and hypoglycaemia is common and dangerous in young children. A venous gas showing acidosis supports significant dehydration. [1] [3]
Stool testing follows the same logic of targeting. Culture, microscopy or molecular panels are worthwhile when there is blood in the stool, in the immunocompromised or systemically unwell child, in outbreaks or for public-health notification, in returned travellers, and when diarrhoea is persistent, because in these situations the result may change treatment or contact-tracing. For the well child with watery diarrhoea, a stool test is a waste of time and money. [11] [2]
Management — Resuscitation
The first job in any acutely unwell child with diarrhoea is to identify and treat shock. A child with severe dehydration — lethargy, cold mottled peripheries, a weak fast pulse, prolonged capillary refill and deeply sunken eyes — needs immediate intravenous or intraosseous access and a rapid fluid bolus, and this is one of the few situations in gastroenteritis where the oral route is set aside. Restore the circulation first, then correct the remaining deficit. [1] [3]
Give an isotonic crystalloid bolus of ten to twenty millilitres per kilogram of 0.9 percent sodium chloride, reassessing after each and repeating as needed until perfusion improves, and check glucose early because hypoglycaemia is common and easily missed in a sick child. Once the child is out of shock, calculate and replace the remaining fluid deficit over the following hours alongside maintenance and ongoing losses, using measured electrolytes to guide the choice of fluid. [1] [3]
Take particular care with the sodium. Hypernatraemic dehydration, in which water is lost in excess of sodium, must be corrected slowly to avoid cerebral oedema, and the febrile, doughy-skinned, irritable child is the classic picture; hyponatraemic dehydration also needs measured correction. This is why electrolytes are checked before and during intravenous rehydration in the severely dehydrated child, rather than reaching for a fixed regimen. [1] [3]
Management — Definitive & Stepwise
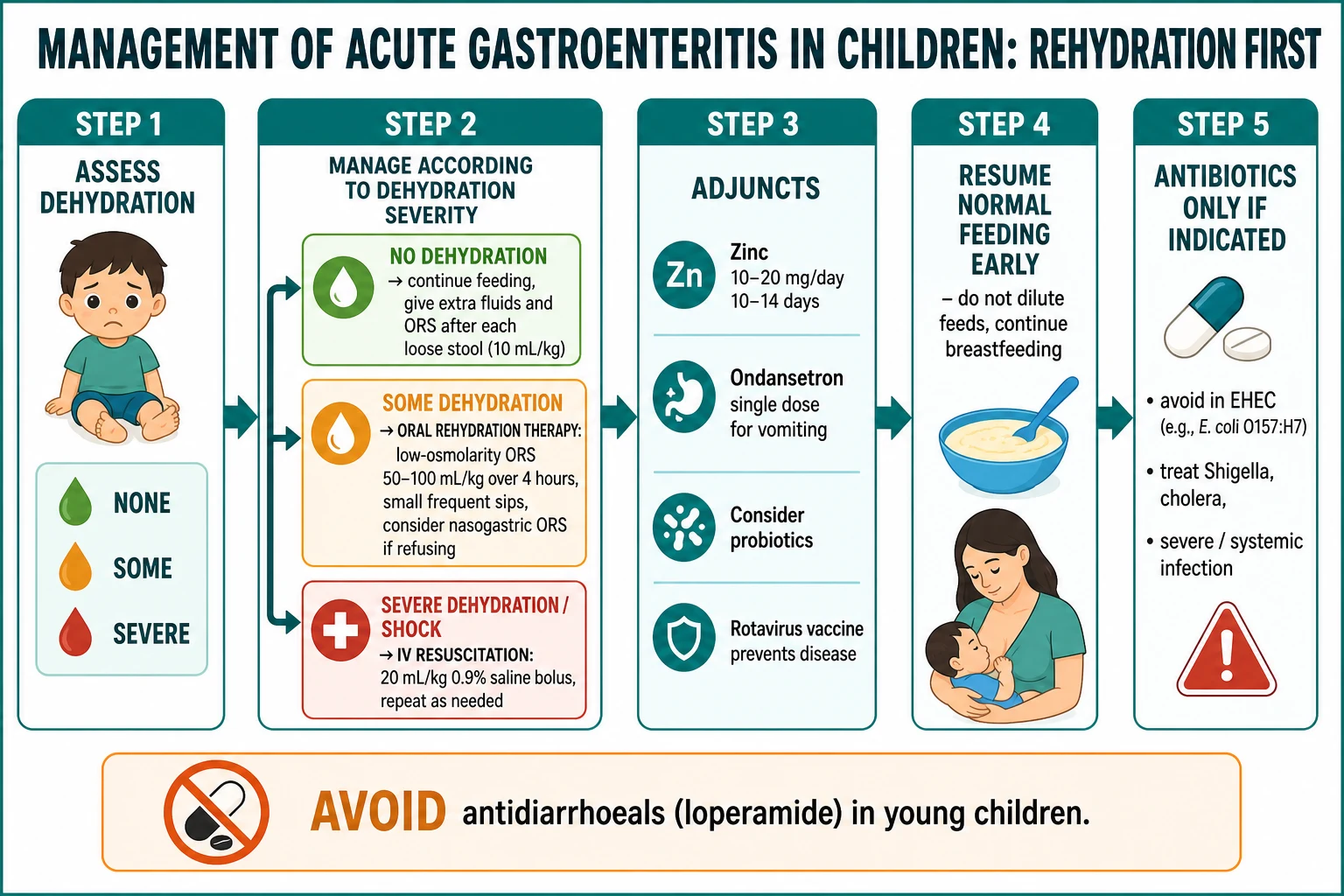
For the great majority of children, who have no or some dehydration, the definitive treatment is oral rehydration therapy, and the figure lays out the whole pathway from assessment through rehydration, adjuncts, feeding and the narrow place of antibiotics. Oral rehydration solution given as small frequent sips is as effective as intravenous fluid for mild-to-moderate dehydration, has fewer complications, is cheaper and can often keep a child out of hospital, so it is the default route. [1] [8]
Use low-osmolarity oral rehydration solution, which has replaced the older higher-osmolarity formulation because it reduces stool output, vomiting and the need for intravenous fluids. For some dehydration, give roughly fifty to one hundred millilitres per kilogram over four hours in small, frequent sips, then reassess; for a child with no dehydration, replace ongoing losses with about ten millilitres per kilogram after each loose stool while continuing normal fluids. When a child will not drink or vomits repeatedly, nasogastric oral rehydration is preferred to intravenous fluid and works just as well. [8] [1]
Rehydration and adjuncts in paediatric gastroenteritis
Feed early and keep the adjuncts few but evidence-based. Resume the child's normal age-appropriate diet as soon as the initial rehydration is done, do not dilute feeds and continue breastfeeding throughout, because early feeding shortens the illness. Zinc supplementation reduces the duration and severity of diarrhoea in children, with the greatest benefit in low-income settings and in those over six months. A single dose of ondansetron reduces vomiting and the need for intravenous fluids and admission, and probiotics have a modest role, while antidiarrhoeal drugs such as loperamide are avoided in young children. [5] [13] [7]
Antibiotics are the exception, not the rule. Most gastroenteritis is viral or self-limiting and needs none; antibiotics are reserved for confirmed or strongly suspected shigellosis, for cholera, for the systemically unwell, immunocompromised or very young infant, and for specific parasitic infections such as symptomatic giardiasis. They are actively avoided in enterohaemorrhagic Escherichia coli because of the haemolytic uraemic syndrome risk, and in most non-typhoidal Salmonella because they prolong carriage without benefit. [11] [1]
Specific Subtypes & Scenarios
Rotavirus gastroenteritis is the archetype of severe dehydrating diarrhoea in infants and toddlers, with profuse watery stools, vomiting and fever, and it is the disease against which the rotavirus vaccine is directed. Its management is pure rehydration, and its story is now as much about prevention as treatment, since routine infant vaccination has markedly reduced severe rotavirus disease and hospitalisation. [9] [1]
Bacterial dysentery is the scenario in which the antibiotic and complication decisions bite. Shigella is the classic cause of high fever with bloody, mucoid stools and may be treated with antibiotics; Campylobacter and non-typhoidal Salmonella usually need only supportive care; and enterohaemorrhagic Escherichia coli is the one to fear, because it produces Shiga toxin and can lead to haemolytic uraemic syndrome, so antibiotics are withheld and the child watched for pallor, bruising and falling urine output. [11] [1]
Two further scenarios recur in examinations. The child who vomits everything is the ideal candidate for a single dose of ondansetron followed by a trial of oral rehydration, which frequently avoids a drip. The returned traveller or the child with persistent watery diarrhoea should prompt thought of Giardia and Cryptosporidium, tested with stool microscopy or molecular panels and treated specifically, since these cross from the acute into the persistent-diarrhoea territory. [13] [14]
Complications & Pitfalls
The dominant complication is dehydration and its sequelae: hypovolaemic shock, acute kidney injury, electrolyte disturbance with hyponatraemia or hypernatraemia, hypokalaemia, metabolic acidosis and hypoglycaemia, any of which can turn a benign illness dangerous. The pathogen-specific complications matter too, above all haemolytic uraemic syndrome after Shiga-toxin Escherichia coli, and, after any infectious diarrhoea, transient lactose intolerance and post-infectious irritable bowel symptoms. [1] [11]
Escalating severity of dehydration in gastroenteritis
Severe dehydration / shock
Lethargic, cold mottled, weak pulse, very slow skin pinch, anuria; IV/IO resuscitation
The pitfalls are mostly errors of over- and under-treatment. The commonest is under-recognising dehydration, or abandoning oral rehydration too early and reaching for a drip that was never needed; conversely, over-investigating the well child with routine bloods and stool cultures wastes resources and delays feeding. Giving empirical antibiotics for bloody diarrhoea, using antidiarrhoeals in young children, and diluting feeds or stopping breastfeeding are all classic and avoidable mistakes. [1] [2]
The subtle traps catch the unwary examiner candidate. Missing a surgical mimic behind vomiting, missing hypoglycaemia in a sick young child, correcting hypernatraemia too quickly and causing cerebral oedema, and failing to safety-net a family so they return if the child deteriorates or cannot keep fluids down are the errors that harm children. Each is prevented by discipline rather than by any test. [3] [1]
Prognosis & Disposition
For the well-managed child the outlook is excellent. Acute gastroenteritis is self-limiting and, provided dehydration is recognised and corrected, the child recovers fully within days without sequelae. The prognosis worsens sharply only when dehydration goes uncorrected or when a specific complication such as haemolytic uraemic syndrome supervenes, which is why the whole emphasis of care is on rehydration and on identifying the few children who are more than simply dehydrated. [1] [10]
Most children are managed entirely at home or after a short period of oral rehydration in the emergency department, and the disposition decision turns on hydration, the ability to tolerate oral fluids, and the reliability of follow-up. Discharge the child who is rehydrated and drinking with clear advice on continuing oral rehydration solution, resuming feeding, and the warning signs that should prompt return, and safety-net actively for the family who live far from care. [1] [12]
Admit the child who is severely dehydrated or shocked, who continues to vomit despite ondansetron and cannot maintain oral or nasogastric rehydration, who has a significant electrolyte disturbance or a suspected surgical or serious cause, or whose family cannot safely manage at home. The threshold is lower for young infants, the malnourished, the immunocompromised and those in remote settings, in whom deterioration is faster and follow-up harder. [1] [11]
Special Populations
The young infant is the most vulnerable, because a small body has little fluid reserve and can dehydrate rapidly, hypoglycaemia is common, and the signs are easy to miss. Breastfeeding should continue throughout, the threshold for review and admission is lower, and rehydration and glucose need close attention. The malnourished child dehydrates and dies more readily and needs particularly careful, cautious rehydration with attention to electrolytes. [1] [10]
The immunocompromised child, including those on chemotherapy or with primary immune deficiency, is at risk of more severe, prolonged and unusual infections, including Cryptosporidium and cytomegalovirus, and warrants a lower threshold for stool testing and specialist involvement. In these children, antibiotics and antivirals have a wider role than in the well child, and diarrhoea is less likely to be simply self-limiting. [11] [1]
Equity is a defining issue in Australia, New Zealand and comparable settings. Indigenous, rural, remote and socioeconomically disadvantaged children carry a disproportionate burden of gastroenteritis and its complications, face barriers of distance, water quality and access to care, and benefit most from rotavirus vaccination, clean water, and community education about oral rehydration. Improving the uptake of oral rehydration therapy remains one of the highest-yield public-health goals. [12] [9]
Evidence, Guidelines & Regional Differences
The evidence base is strong and unusually consistent. International guidelines, led by the European society statements, converge on the same core: assess dehydration clinically, rehydrate orally with low-osmolarity solution as first choice, feed early, use zinc and selective antibiotics, and avoid routine investigation and antidiarrhoeals. The superiority of low-osmolarity over the original oral rehydration salts, and the equivalence of oral and nasogastric rehydration to intravenous fluid for mild-to-moderate dehydration, are well established. [1] [8]
The adjuncts rest on good trial evidence. Zinc reduces the duration and severity of diarrhoea in children, most clearly in low-income settings, and is a World Health Organization recommendation; a single dose of ondansetron reduces vomiting, intravenous fluid use and admission, although multidose courses after discharge add little; and probiotics have a modest, strain-specific effect that recent position papers treat cautiously. [5] [13] [7]
Regional differences are practical rather than definitional. The organisms, the severity and the mortality differ enormously between high- and low-income settings, so zinc, antibiotics for dysentery and public-health measures carry far more weight where the burden is high, while in Australia and New Zealand the emphasis is on rotavirus vaccination, avoiding over-investigation, keeping children out of hospital through oral rehydration, and closing the equity gap for Indigenous and remote children. [10] [12]
Exam Pearls
Hold one sentence for the viva: a young child with acute watery diarrhoea and vomiting is managed by grading dehydration clinically as none, some or severe, rehydrating with low-osmolarity oral rehydration solution as small frequent sips (or nasogastric if refusing) for the first two grades and intravenous 0.9 percent saline for shock, feeding early, adding zinc and a single dose of ondansetron, and reserving antibiotics for specific indications. Oral rehydration therapy is the treatment of choice and the highest-yield fact on the page. [1] [8]
State the frequently tested facts correctly. Use low-osmolarity ORS, roughly 50 to 100 mL/kg over 4 hours for some dehydration and 10 mL/kg after each stool for none; give an IV bolus of 10 to 20 mL/kg 0.9 percent saline for shock. Zinc is 10 mg/day under 6 months and 20 mg/day at 6 months and over for 10 to 14 days. Oral rehydration works because the sodium-glucose co-transporter (SGLT1) stays intact. Avoid antibiotics in enterohaemorrhagic Escherichia coli because of haemolytic uraemic syndrome, and avoid antidiarrhoeals in young children. [5] [8] [11]
The high-yield pairings do the diagnostic work: watery diarrhoea with no blood means viral or enterotoxigenic — rehydrate only; bloody diarrhoea with fever means invasive or Shiga-toxin — think antibiotics carefully and watch for haemolytic uraemic syndrome; the child who vomits everything means single-dose ondansetron then oral rehydration; bilious vomiting or a tender distended abdomen means surgical cause, not gastro; and diarrhoea beyond fourteen days means persistent diarrhoea and a new work-up. Always grade dehydration first and rehydrate by the safest effective route. [13] [3]
References
- [1]Guarino A; Ashkenazi S; Gendrel D; et al European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. J Pediatr Gastroenterol Nutr, 2014.PMID 24739189
- [2]Pieścik-Lech M; Shamir R; Guarino A; et al Review article: the management of acute gastroenteritis in children. Aliment Pharmacol Ther, 2013.PMID 23190209
- [3]Steiner MJ; DeWalt DA; Byerley JS Is this child dehydrated? JAMA, 2004.PMID 15187057
- [4]Bailey B; Gravel J; Goldman RD; et al External validation of the clinical dehydration scale for children with acute gastroenteritis. Acad Emerg Med, 2010.PMID 20624137
- [5]Lazzerini M; Wanzira H Oral zinc for treating diarrhoea in children. Cochrane Database Syst Rev, 2016.PMID 27996088
- [6]Collinson S; Deans A; Padua-Zamora A; et al Probiotics for treating acute infectious diarrhoea. Cochrane Database Syst Rev, 2020.PMID 33295643
- [7]Szajewska H; Berni Canani R; Domellöf M; et al Probiotics for the Management of Pediatric Gastrointestinal Disorders: Position Paper of the ESPGHAN Special Interest Group on Gut Microbiota and Modifications. J Pediatr Gastroenterol Nutr, 2023.PMID 36219218
- [8]Lifschitz C; Kozhevnikov O; Oesterling C; et al Acute gastroenteritis-changes to the recommended original oral rehydrating salts: a review. Front Pediatr, 2023.PMID 38192370
- [9]Henschke N; Bergman H; Hungerford D; et al The efficacy and safety of rotavirus vaccines in countries in Africa and Asia with high child mortality. Vaccine, 2022.PMID 35184924
- [10]GBD 2023 Diarrhoeal Diseases Collaborators Global burden of enteric infectious diseases, diarrhoeal diseases, and corresponding aetiologies, 1990-2023: a systematic analysis for the Global Burden of Disease Study 2023. Lancet Infect Dis, 2026.PMID 42229499
- [11]Mwendera CA; Yilma M; Wairimu C; et al Burden of Shigella and enterotoxigenic Escherichia coli infections among children under 5 years in Ethiopia, Kenya and Malawi: a systematic review and meta-analysis. BMJ Glob Health, 2026.PMID 41771662
- [12]Shankar J; Nagpal R; Patil A; et al From Barriers to Best Practices: Enhancing Oral Rehydration Therapy Utilization for Diarrhea Management in India. J Assoc Physicians India, 2025.PMID 40955904
- [13]Freedman SB; Williamson-Urquhart S; Plint AC; et al Multidose Ondansetron after Emergency Visits in Children with Gastroenteritis. N Engl J Med, 2025.PMID 40673584
- [14]Sumner M; Xie J; Williamson-Urquhart S; et al Persistent Vomiting Among Children With Acute Gastroenteritis: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw Open, 2026.PMID 42090154