Paeds · gastroenterology-hepatology-and-nutrition
Acute liver failure
Also known as Paediatric acute liver failure · PALF · Fulminant hepatic failure in children · Acute hepatic failure · Fulminant hepatitis
Fellowship guide to paediatric acute liver failure: the PALF diagnostic criteria in which encephalopathy is not required unlike adults, the age-dependent aetiology, the use of N-acetylcysteine including for non-acetaminophen causes, the critical point that the adult King's College Criteria are not validated in children, and the early pathway to liver transplant assessment.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A previously well child who develops jaundice, easy bruising, and altered consciousness over days has acute liver failure, one of the most time-critical emergencies in paediatrics. The defining problem is sudden, massive hepatocyte loss that destroys the liver's synthetic and detoxifying functions, producing coagulopathy, encephalopathy, and multiorgan failure that can progress to death within days without liver transplantation. [1]
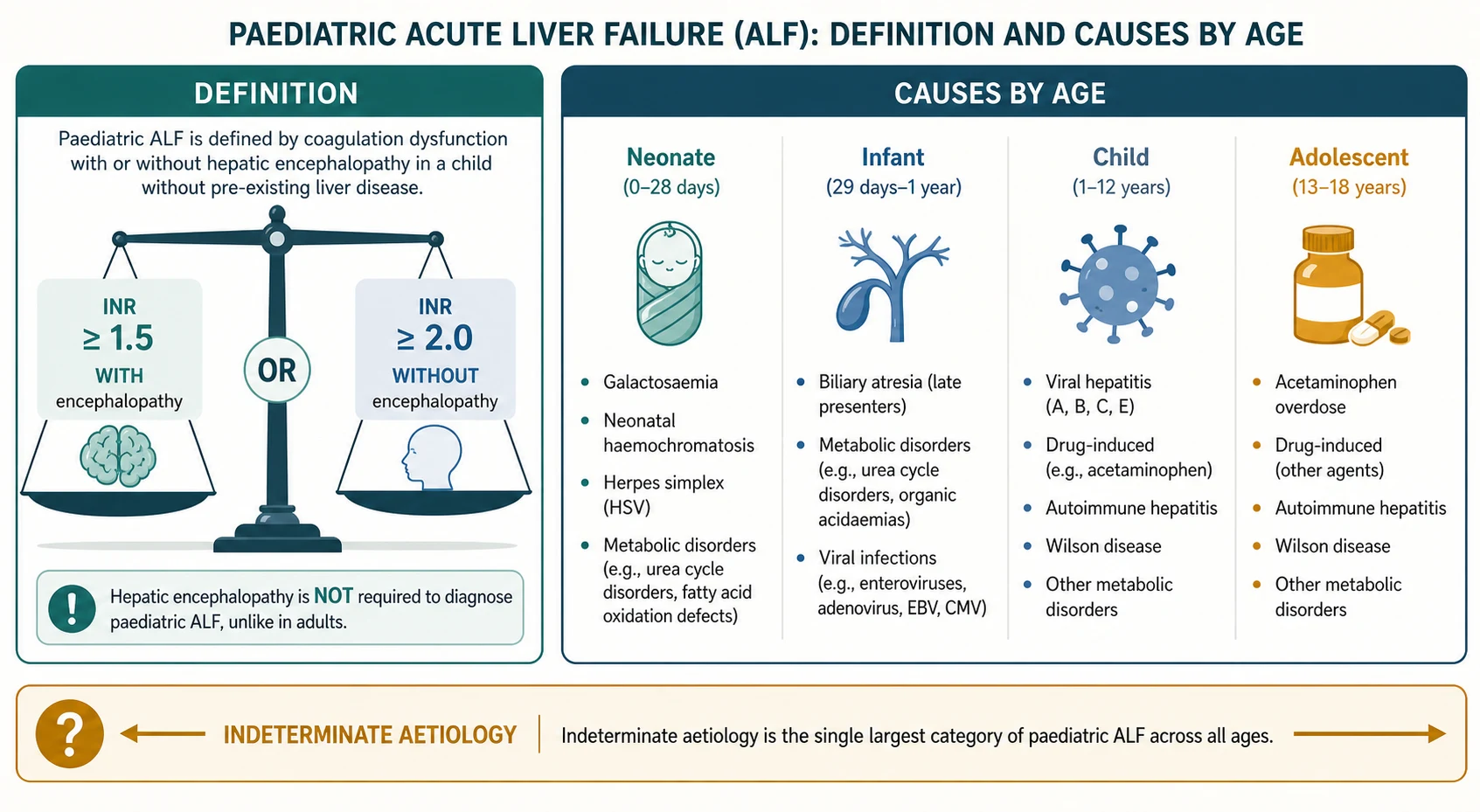
The paediatric definition differs from the adult one in one crucial respect, and examiners test this repeatedly. In adults, hepatic encephalopathy is required to diagnose acute liver failure. In children, encephalopathy is not required, because infants and young children may not show recognisable encephalopathy until very late, and waiting for it delays life-saving treatment. The Paediatric Acute Liver Failure Study Group definition requires acute liver injury with coagulopathy defined as an international normalised ratio of 1.5 or greater with any degree of hepatic encephalopathy, or an international normalised ratio of 2.0 or greater without encephalopathy, in a child with no evidence of chronic liver disease. [1]
The emergency is two-sided. The failing liver stops making clotting factors and clearing toxins, so the child bleeds and accumulates ammonia that swells the brain. At the same time the cause may be treatable, which is why every minute spent on resuscitation must run in parallel with a hunt for the cause and an early call to the liver transplant centre. The window between irreversible brain injury and a successful transplant is narrow, and the team that recognises failure early and escalates fast saves lives. [5]
Classification
Classification serves two purposes: it confirms that the child meets the diagnostic threshold, and it frames the cause, which drives every treatment decision. The diagnosis rests on the coagulopathy threshold and the absence of chronic liver disease. A child with a known chronic liver disease such as biliary atresia who decompensates has acute-on-chronic liver failure, which is a different entity with a different management calculus, and must not be confused with true acute liver failure. [8]
The cause is strongly age-dependent, and naming the likely cause by age accelerates the workup. In neonates and young infants, metabolic disease such as galactosaemia and hereditary tyrosinaemia, neonatal haemochromatosis now termed gestational alloimmune liver disease, herpes simplex virus infection, and sepsis dominate. In older infants and children, viral hepatitis, drug-induced liver injury including acetaminophen, autoimmune hepatitis, and Wilson disease become prominent, while in adolescents intentional acetaminophen overdose and Wilson disease are leading considerations. [6]
[6]The single largest diagnostic category across all ages is indeterminate, meaning no cause is found despite a thorough workup. Up to half of paediatric acute liver failure cases remain indeterminate in large cohorts, and this proportion rises as modern metabolic and genetic testing reclassifies some, but the message for the clinician is that an unknown cause is common and does not exclude the diagnosis or delay transplant assessment. [1]
Epidemiology & Risk Factors
Paediatric acute liver failure is rare but carries a mortality of 10 to 30 percent without transplantation, which places it among the most lethal non-malignant emergencies in paediatric hepatology. The incidence is estimated at one to two per 100,000 children per year in high-income settings, though the true figure is likely higher because mild or rapidly fatal cases may go unrecognised. [5]
The cause distribution reflects age and environment. In North American and European cohorts, indeterminate aetiology leads, followed by drug-induced liver injury dominated by acetaminophen, metabolic disease, and autoimmune hepatitis. In regions where viral hepatitis A and E are endemic, such as parts of South and Southeast Asia, viral infection is a leading cause, and the Indian Society consensus highlights hepatitis A and E alongside Wilson disease as dominant regional causes. [8]
Risk factors for a poor outcome include a younger age, an indeterminate cause, severe coagulopathy with a rapidly rising international normalised ratio, and the development of hepatic encephalopathy and multiorgan failure. Recognising these early helps the team decide how aggressively to pursue transplantation, because the child who is deteriorating despite maximal medical therapy has a transplant-free survival that falls steeply with each passing day. [7]
Pathophysiology
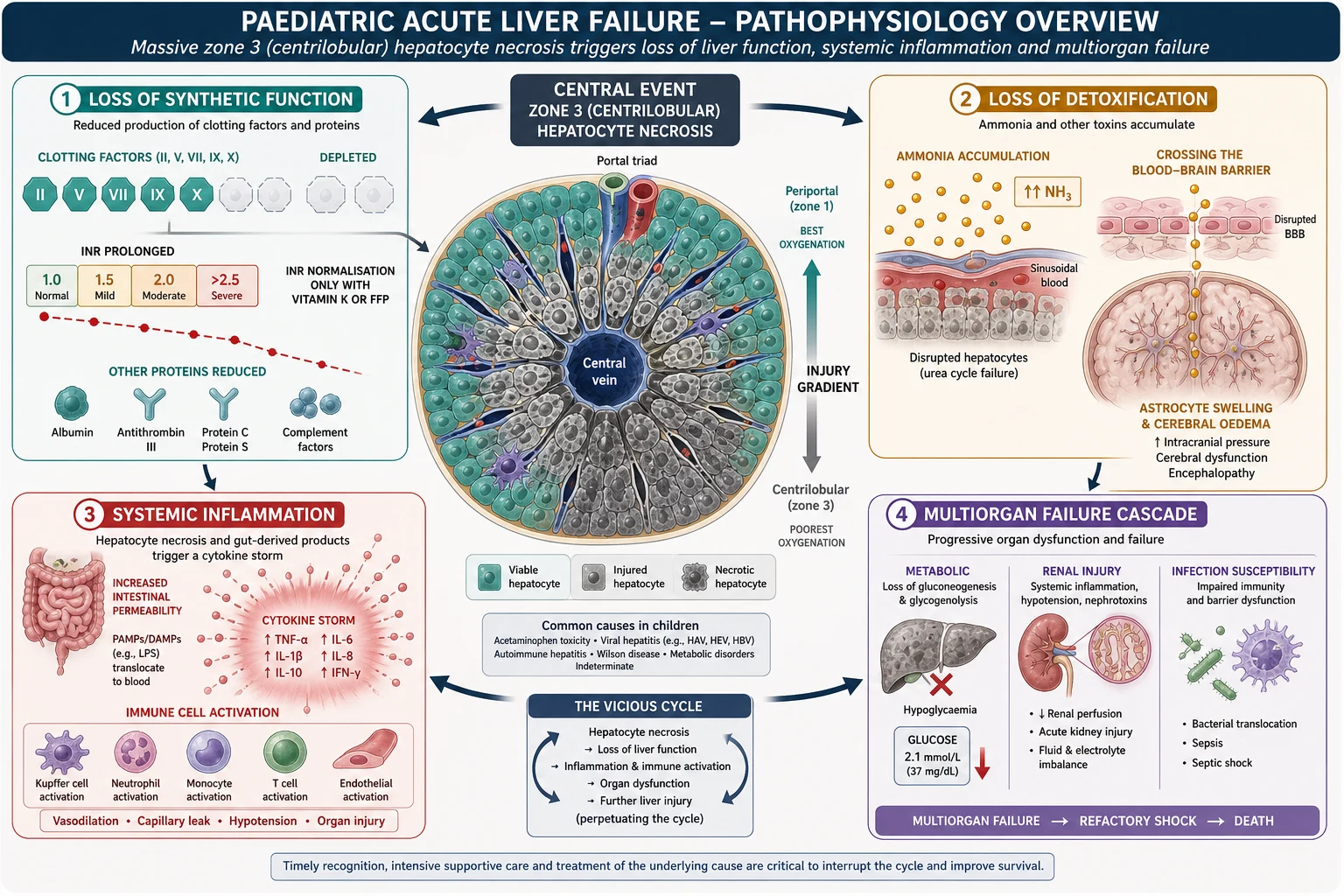
The core event is sudden, widespread hepatocyte death, most often centrilobular or zone 3 necrosis, because these hepatocytes around the central vein are the most metabolically active and the most vulnerable to hypoxic, toxic, and inflammatory injury. When enough hepatocytes die, the liver cannot perform its two essential jobs: synthesising proteins, including clotting factors, and clearing toxins, including ammonia. Every clinical feature of acute liver failure flows from the failure of these two functions. [10]
Loss of synthetic function produces coagulopathy because the liver makes nearly all the clotting factors except factor eight, which is also made by endothelial cells. The international normalised ratio rises as factors two, five, seven, and ten fall, and this rise is the single most useful marker of severity and trajectory. The liver also stops making glucose through gluconeogenesis, so hypoglycaemia is common and dangerous, and it stops clearing lactate, contributing to a metabolic acidosis that itself worsens prognosis. [5]
Loss of detoxification is the mechanism of hepatic encephalopathy and cerebral oedema. Ammonia, normally converted to urea by the liver, accumulates and crosses the blood-brain barrier, where astrocytes take it up and convert it to glutamine. The accumulated glutamine draws water into the astrocytes, causing them to swell, and this astrocyte swelling is the substrate for cerebral oedema, the most feared and often fatal complication of acute liver failure. In children, cerebral oedema can develop rapidly and may present with agitation, hypertension, and abnormal posturing before progressing to coma and brainstem herniation. [6]
A systemic inflammatory response accompanies the failing liver and drives multiorgan dysfunction. Damaged hepatocytes release damage-associated molecular patterns that activate innate immunity, producing a cytokine response that impairs circulation, worsens renal perfusion, and predisposes to secondary infection. This inflammatory cascade is one reason acute liver failure behaves like septic shock in its late stages, and it explains why vigilant infection surveillance and haemodynamic support are central to intensive care. [5]
Clinical Presentation
The presentation spans the spectrum from a child with new jaundice and bruising who is still alert, to a child in deep coma with multiorgan failure. The common thread is acute hepatic dysfunction in a child without known chronic liver disease, and the pace ranges from hyperacute, where encephalopathy develops within seven days of the first symptom, to subacute, where the course unfolds over weeks. [6]
Jaundice is usually present but may be absent in hyperacute presentations such as acetaminophen overdose, where massive transaminase elevation and coagulopathy precede visible jaundice. Easy bruising, bleeding from puncture sites, mucosal bleeding, and petechiae reflect the coagulopathy, and the team should ask about and look for these signs directly rather than waiting for laboratory confirmation. Nausea, vomiting, and right upper quadrant discomfort may accompany the hepatic injury itself. [10]
Hepatic encephalopathy in children is graded but is often harder to recognise than in adults, especially in infants. Grade one is subtle irritability or sleep disturbance, grade two is lethargy and disorientation, grade three is marked somnolence and confusion with abnormal reflexes, and grade four is coma. In infants, the earliest signs may be poor feeding, irritability, and a high-pitched cry, and the team must have a low threshold to suspect encephalopathy in any child with acute liver failure and coagulopathy. [6]
Recognising the deteriorating child with acute liver failure
Rapidly rising international normalised ratio over hours
Deepening encephalopathy from lethargy to somnolence or coma
Hypoglycaemia requiring increasing glucose infusion
Metabolic acidosis with a falling arterial pH
Renal dysfunction with falling urine output or rising creatinine
Clinical signs of cerebral oedema: hypertension, bradycardia, abnormal posturing
Signs of cerebral oedema are a pre-terminal warning. The Cushing triad of hypertension, bradycardia, and irregular respiration signals raised intracranial pressure, and abnormal posturing, pupillary changes, and loss of brainstem reflexes indicate impending herniation. A child reaching this stage needs immediate neuroprotection and an expedited transplant decision, because the window for a meaningful recovery closes once irreversible brain injury occurs. [6]
Differential Diagnosis
The first task is to separate true acute liver failure from its mimics, because the management and prognosis differ. Acute hepatitis with high transaminases but a normal or minimally abnormal international normalised ratio is not acute liver failure, and the distinction rests on the coagulopathy threshold. A child with isolated transaminitis and no coagulopathy may have viral hepatitis, drug injury, or another self-limited process that does not require transplant assessment. [1]
Acute-on-chronic liver failure is the other key exclusion. A child with known biliary atresia, autoimmune hepatitis, or metabolic liver disease who decompensates has acute-on-chronic failure, and while the resuscitation overlaps, the prognostic calculus and transplant urgency differ. A careful history for any prior liver disease, growth faltering, or chronic jaundice, and a focused examination for stigmata of chronic liver disease such as splenomegaly and spider naevi, help make this distinction at the bedside. [8]
[8]Sepsis with secondary hepatic dysfunction can mimic acute liver failure, and conversely acute liver failure predisposes to sepsis, so the two often coexist. A child in septic shock with disseminated intravascular coagulation and transaminitis may have a high international normalised ratio from the coagulopathy of sepsis rather than primary liver failure, and a conjugated bilirubin out of proportion to the transaminases or a history consistent with infection helps separate the two. In practice, the team treats both aggressively and does not delay resuscitation for the distinction. [5]
Clinical & Bedside Assessment
The assessment is performed in parallel with resuscitation and focuses on three questions: how severe is the failure, what is the cause, and is the child deteriorating toward transplant. The airway, breathing, and circulation are assessed and stabilised first, with particular attention to hypoglycaemia, which is common and easily missed. A bedside glucose must be checked immediately in any child with acute liver dysfunction, and hypoglycaemia treated with intravenous dextrose. [6]
The history targets the cause and the timeline. Ask about drug and toxin exposure including acetaminophen, herbal and complementary medicines, and recent new prescriptions, because drug-induced liver injury is a leading cause and is treatable. Ask about viral symptoms, foreign travel, blood transfusions, family history of liver disease or consanguinity suggesting metabolic disease, and any prior jaundice or growth faltering that would point to chronic disease. In adolescents, ask sensitively about intentional overdose and eating disorders, both linked to acetaminophen toxicity and Wilson disease. [10]
The examination assesses severity and seeks signs of chronic disease and cerebral oedema. Look for jaundice, bruising, petechiae, and bleeding, and palpate for hepatosplenomegaly and ascites. Examine for stigmata of chronic liver disease including spider naevi, palmar erythema, and clubbing. Perform a focused neurologic assessment for encephalopathy grade, and in the deteriorating child look specifically for the Cushing triad, abnormal posturing, and pupillary changes that signal raised intracranial pressure. Kayser-Fleischer rings suggest Wilson disease. [11]
The severity assessment is dynamic. A single international normalised ratio tells you where the child is, but the trend over hours tells you where they are going. A child whose international normalised ratio is rising despite resuscitation, whose encephalopathy is deepening, or whose arterial pH is falling is heading toward transplant, and the team must escalate to a transplant centre before the child reaches a pre-terminal state. Repeated examinations and serial blood gases and coagulation studies are the backbone of this monitoring. [5]
Investigations
The investigations confirm the diagnosis, exclude chronic disease, seek the cause, and track the trajectory. The international normalised ratio is the cornerstone: a value of 1.5 or greater with encephalopathy or 2.0 or greater without encephalopathy, in a child without chronic liver disease, confirms acute liver failure. Liver function tests show markedly elevated transaminases, though the absolute value is less prognostic than the trend, and a falling transaminase with a rising international normalised ratio is an ominous sign of hepatic synthetic collapse. [1]
A comprehensive cause-directed workup runs from the first hour. Blood tests include an acetaminophen level in any case without a clear cause, autoimmune markers including antinuclear antibodies, anti-smooth muscle antibodies, and immunoglobulin G, a viral screen including hepatitis A, B, and E serology, Epstein-Barr virus, and herpes simplex virus polymerase chain reaction, and a metabolic screen including ammonia, lactate, ceruloplasmin, urinary copper, alpha-1 antitrypsin phenotype, and urinary reducing substances. An abdominal ultrasound with Doppler assesses liver texture, biliary tree, patency of the hepatic vasculature, and excludes Budd-Chiari syndrome. [10]
The ammonia level correlates roughly with encephalopathy severity and cerebral oedema risk, though it is not used alone to make decisions. An arterial or capillary blood gas tracks the pH, which is a powerful prognostic marker: a falling pH reflects accumulating lactate and failing clearance, and a pH below 7.3 with a rising international normalised ratio is a grave sign that in adults triggers the transplant pathway. Renal function, electrolytes, and a full blood count are monitored, and blood, urine, and when indicated cerebrospinal fluid cultures are sent to exclude and surveillance for sepsis, because infection is both a mimic and a complication. [5]
A liver biopsy is rarely performed in acute liver failure because of the coagulopathy, but transjugular biopsy may be considered when autoimmune hepatitis, malignancy, or a specific metabolic diagnosis would change management and the diagnosis remains unclear. The biopsy is not routine and the risk of bleeding must be weighed against the diagnostic yield in each case. [6]
Management — Resuscitation
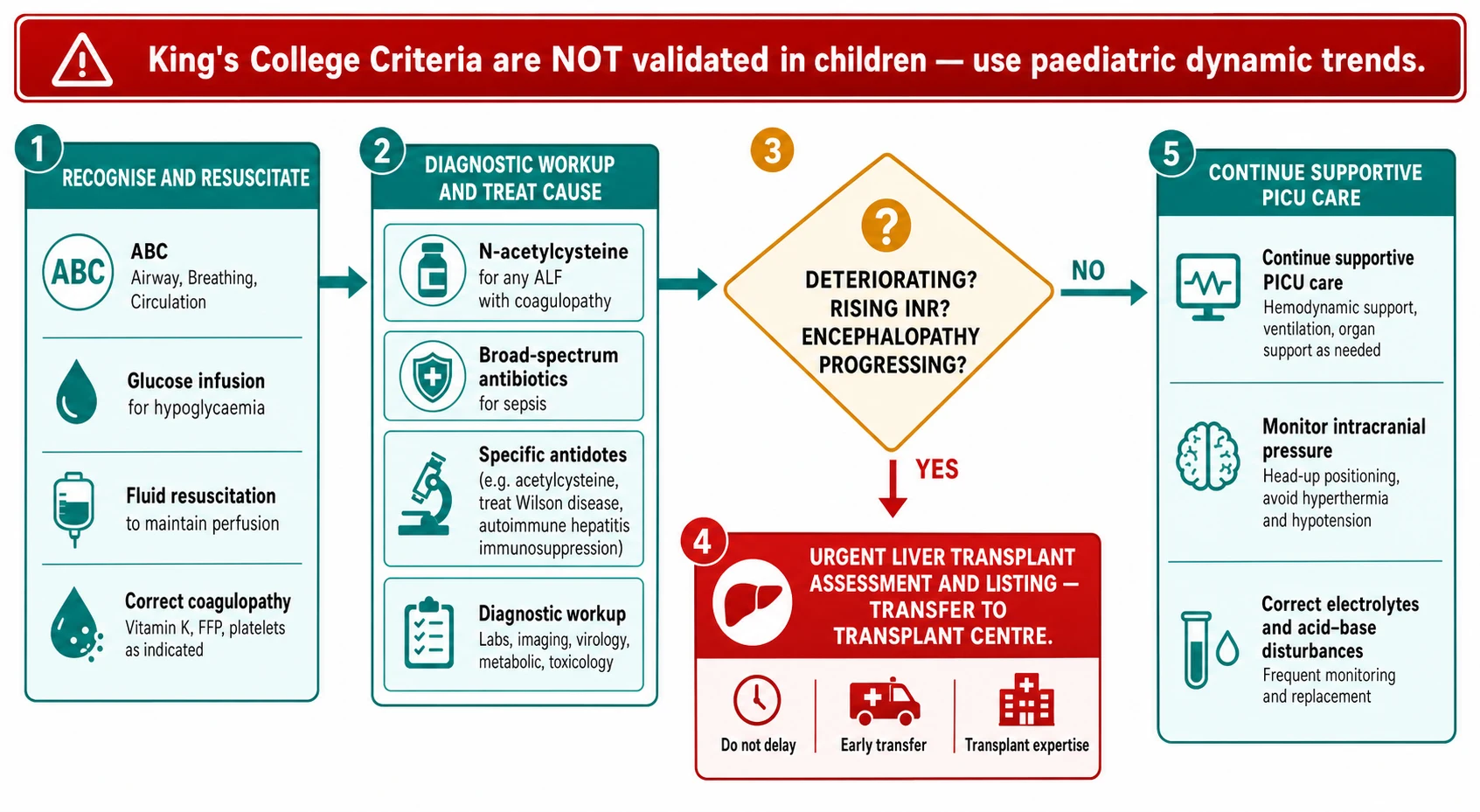
Resuscitation and cause-directed treatment run in parallel from the first contact, and the overriding principle is to stabilise the child while arranging urgent transfer to a paediatric liver transplant centre. The airway is secured in any child with grade three or four encephalopathy, because these children are at risk of aspiration and hypoventilation, and intubation is performed with careful sedation because oversedation masks the neurologic examination. Intravenous access is established, and fluid resuscitation supports the circulation, guided by clinical assessment and, in the intensive care unit, invasive monitoring. [6]
Hypoglycaemia is treated immediately and continuously. The failing liver cannot perform gluconeogenesis, so the child needs a continuous intravenous dextrose infusion, typically 6 to 8 milligrams per kilogram per minute of glucose, titrated to maintain normoglycaemia, with bedside glucose checked frequently. Untreated hypoglycaemia worsens encephalopathy and causes seizures, and it is a preventable cause of secondary brain injury in a child already at risk from hepatic encephalopathy. [6]
Coagulopathy is managed with restraint. The international normalised ratio is the most important prognostic trend, and giving fresh frozen plasma prophylactically masks that trend without preventing the most dangerous bleeding, which is intracranial. Fresh frozen plasma and other blood products are reserved for active bleeding or before invasive procedures such as central line insertion, and vitamin K is given to correct any related deficiency. This restraint allows the team to track the international normalised ratio accurately and to use it for transplant decisions. [1]
N-acetylcysteine for paediatric acute liver failure
Dose
Loading dose 150 mg per kg intravenously over 60 minutes, then 50 mg per kg over 4 hours, then 100 mg per kg over 16 hours, for a total 300 mg per kg over 21 hours
N-acetylcysteine is started early and broadly. For acetaminophen toxicity it is the specific antidote, replenishing glutathione and detoxifying the toxic metabolite, and the earlier it is given the better the outcome. For non-acetaminophen acute liver failure, the adult randomised trial showed that intravenous N-acetylcysteine improved transplant-free survival in early-stage disease, and the paediatric safety study confirmed it was safe and effective in children, so the NASPGHAN position paper supports its use in children with non-acetaminophen acute liver failure and coagulopathy. [3]
Encephalopathy and cerebral oedema are managed with neuroprotective intensive care. The head is kept midline and elevated 30 degrees, hypercapnia and hypoxia are avoided, and seizures are treated promptly. Intracranial pressure monitoring is controversial in children and is used selectively in centres with expertise, because the risk of infection and bleeding from the monitor must be weighed against the benefit of the data. Hypernatraemia is maintained modestly to control cerebral oedema, and osmotic agents such as hypertonic saline or mannitol are used when there is clinical or monitored evidence of raised intracranial pressure. [6]
Infection surveillance and treatment are integral, because the failing liver and its supportive interventions predispose to bacterial and fungal sepsis. Blood, urine, and other cultures are sent on admission and with any clinical deterioration, and broad-spectrum antibiotics and antifungal agents are started at the first sign of infection, because untreated sepsis drives multiorgan failure and is a leading cause of death. Renal dysfunction is managed with attention to volume status and, when needed, renal replacement therapy, which also helps control ammonia and fluid balance. [5]
Management — Definitive & Stepwise
Definitive management is cause-specific where a treatable cause is found, and centred on liver transplantation where the liver fails to recover. Acetaminophen toxicity is treated with N-acetylcysteine and supportive care, and most children recover. Autoimmune hepatitis is treated with corticosteroids once infection is excluded. Wilson disease presenting as acute liver failure usually requires transplantation because the injury is often irreversible, though chelation therapy is started and a transplant is arranged in parallel. Herpes simplex hepatitis is treated with intravenous aciclovir. Metabolic causes such as galactosaemia and hereditary tyrosinaemia are managed with dietary restriction and specific metabolic therapy. [10]
N-acetylcysteine dosing detail for non-acetaminophen PALF
Dose
Loading 150 mg per kg over 60 minutes, then maintenance infusion of 100 mg per kg over 16 hours, repeated or continued until the international normalised ratio falls below 1.5
Liver transplantation is the definitive treatment for acute liver failure that progresses despite maximal medical therapy, and the decision to list is the most consequential judgement in the disease. The challenge in children is that the adult King's College Criteria, developed by O'Grady and colleagues in 1989 for fulminant hepatic failure, are not validated in children and perform poorly in paediatric cohorts, with both false-positive and false-negative predictions. This is a high-yield exam point: the team must not apply the adult criteria rigidly to children. [2]
The paediatric approach to transplant listing is dynamic and multidisciplinary. The team tracks the trend in the international normalised ratio, the depth and progression of encephalopathy, the arterial pH and lactate, and the development of renal failure and other organ dysfunction, and a child who is worsening on maximal medical therapy is listed urgently. The Paediatric End-stage Liver Disease score and other dynamic markers inform the urgency, and the decision is made jointly by the paediatric hepatology, intensive care, and transplant surgery teams at a specialist centre. Early referral to a transplant centre, before the child is irretrievable, is the single most important principle, because transfer after multiorgan failure is established is often too late. [7]
Live donor liver transplantation is an important option in regions with deceased donor shortage, and dedicated paediatric programmes report outcomes comparable to deceased donor transplantation for acute liver failure, making it a viable bridge to definitive care where a suitable donor is identified. The logistics of donor evaluation add time, which reinforces the need for early referral and concurrent workup of the family. [9]
Specific Subtypes & Scenarios
Wilson disease presenting as acute liver failure is a distinctive and high-yield scenario. The child, usually older than three years and often an adolescent, presents with Coombs-negative haemolytic anaemia, a low or normal alkaline phosphatase relative to the bilirubin, and acute liver failure, often with Kayser-Fleischer rings on slit-lamp examination. The combination of haemolysis and liver failure with a low alkaline phosphatase-to-bilirubin ratio is nearly pathognomonic, and the condition usually requires liver transplantation because the hepatic injury is often irreversible by the time of presentation, though chelation with penicillamine or zinc is started and a donor is evaluated in parallel. [11]
Neonatal and infant acute liver failure has a different cause spectrum and a particularly high metabolic yield. Neonatal haemochromatosis, now understood as gestational alloimmune liver disease, presents in the first days to weeks of life with liver failure and extrahepatic iron deposition and is treated with double-volume exchange transfusion and intravenous immunoglobulin, with a dramatic improvement in survival when treated promptly. Galactosaemia presents with liver failure, cataracts, and Escherichia coli sepsis after the introduction of galactose-containing feeds, and hereditary tyrosinaemia, hereditary fructose intolerance, and mitochondrial hepatopathies enter the differential in young infants. A focused metabolic workup is essential and time-critical in this age group. [6]
Acetaminophen-induced acute liver failure is the most readily treatable form and the one where time matters most. The toxicity follows a predictable course: a latent phase with falling acetaminophen levels, then a phase of rising transaminases and international normalised ratio peaking around 72 hours, then either recovery or progression to failure. The Rumack-Matthew nomogram guides treatment after a single acute ingestion, but N-acetylcysteine is given regardless of the level or timing in any child with evidence of hepatotoxicity, because it remains effective even after the injury has begun. Early N-acetylcysteine prevents most deaths from acetaminophen toxicity, which is why it is started empirically in any case of acute liver failure without a clear alternative cause. [5]
[7]Complications & Pitfalls
The complications of paediatric acute liver failure span the brain, the blood, and the other organs, and they are the direct causes of death. Cerebral oedema with raised intracranial pressure and brainstem herniation is the most feared complication and was historically the leading cause of death before modern neurointensive care and transplantation. Bleeding from the coagulopathy, particularly intracranial and gastrointestinal haemorrhage, is the second major danger. Renal failure, often a hepatorenal pattern or acute tubular necrosis, complicates the late stages and may require renal replacement therapy, which also helps control ammonia and fluid. [6]
Infection is both a complication and a driver of deterioration. The failing liver impairs immune function, and the invasive monitoring and interventions of intensive care create portals for bacterial and fungal entry, so sepsis is a leading cause of death and a common reason for a child to decompensate from a recoverable to an irretrievable state. Hypoglycaemia, if untreated, causes seizures and worsens encephalopathy. Pancreatitis, aspiration, and the complications of prolonged intensive care add to the burden in the child who survives the acute phase but remains dependent on supportive therapy for weeks. [5]
The classic pitfalls are diagnostic delay and the misapplication of adult criteria. Because encephalopathy is not required for the diagnosis in children, a child with acute coagulopathy and liver dysfunction may be mislabelled as having self-limited hepatitis until the international normalised ratio climbs and encephalopathy appears, by which point the transplant window may have narrowed. The mirror error is applying the adult King's College Criteria to children, either to deny transplant listing to a deteriorating child who does not meet the adult thresholds or to list a child who meets them but is actually recovering. The paediatric approach uses dynamic trends, not a single adult score, and the team that internalises this avoids the two most dangerous errors. [2]
Prognosis & Disposition
The prognosis depends on the cause, the severity at presentation, and the trajectory, and it has improved with early N-acetylcysteine, modern intensive care, and liver transplantation. Acetaminophen-induced failure has the best prognosis when treated early, with the majority of children recovering with supportive care and N-acetylcysteine. Indeterminate and Wilson disease acute liver failure have a poorer transplant-free survival and more often require transplantation. Overall, the survival of children with acute liver failure now exceeds 70 percent in modern cohorts, with transplantation contributing substantially to the improvement. [7]
Children who undergo liver transplantation for acute liver failure face a different but manageable set of long-term challenges, including immunosuppression, graft dysfunction, and the complications of lifelong transplant care. The first year after acute liver failure, whether managed medically or with transplantation, carries a measurable burden of impaired health-related quality of life and neurocognitive function, and these children benefit from structured follow-up that addresses cognition, school performance, and psychosocial adjustment alongside the hepatic outcome. [12]
All children with acute liver failure are managed at a specialist paediatric hepatology and intensive care centre with liver transplantation capability, and retrieval services link regional hospitals to the tertiary unit. The discharge plan addresses the cause, the medication and monitoring regimen, and the psychosocial needs of the child and family, including mental health support where intentional overdose was the cause. Long-term follow-up monitors hepatic recovery or graft function, neurocognitive development, and quality of life, because the consequences of acute liver failure extend well beyond the acute admission. [12]
Special Populations
Neonates and infants warrant particular care because the cause spectrum is dominated by metabolic disease and infections that have specific, time-critical treatments. Gestational alloimmune liver disease, galactosaemia, hereditary tyrosinaemia, and herpes simplex hepatitis all have treatments that change the outcome if started early, and the metabolic workup must be sent before the administration of products that would obscure the results, such as fresh frozen plasma affecting the diagnosis of coagulopathy-related metabolic disease. Early involvement of a metabolic and hepatology team is essential in this age group. [6]
Adolescents who present with intentional acetaminophen overdose require parallel medical and psychiatric management. The medical treatment with N-acetylcysteine is the same, but the admission must include a psychosocial assessment, risk evaluation, and the engagement of mental health services, because the underlying self-harm behaviour determines the long-term outcome as much as the hepatic recovery. A non-judgemental, confidential, and adolescent-friendly approach is essential, and the team must recognise that the medical and psychiatric needs are equally urgent. [5]
Children from socioeconomically disadvantaged backgrounds and those in rural or remote areas face barriers to the rapid transfer and specialist care that acute liver failure demands. Practical support with retrieval coordination, telehealth liaison with the transplant centre, and assistance for families with travel and accommodation helps close this gap, and a named coordinator can prevent the fragmentation that disproportionately affects vulnerable families. In lower-resource settings, the priority is early recognition, empirical N-acetylcysteine, and rapid referral to the nearest centre with transplant capability, because the window for effective treatment is narrow and does not respect geography. [8]
[8]Evidence, Guidelines & Regional Differences
The NASPGHAN position paper on the diagnosis and management of paediatric acute liver failure, published in 2022, is the current North American guideline and codifies the paediatric definition, the cause workup, the use of N-acetylcysteine including for non-acetaminophen causes, and the approach to transplant assessment. It emphasises that the adult King's College Criteria are not validated in children and that paediatric decisions rely on dynamic trends, and it supports empirical N-acetylcysteine in any child with coagulopathy while the cause is sought. [1]
The ISPGHAN consensus, published in 2024, provides region-specific guidance for South Asia, where viral hepatitis A and E and Wilson disease are leading causes and where access to deceased donor transplantation is limited. It emphasises early empirical N-acetylcysteine, a cause-directed workup tailored to the regional aetiology, and the role of live donor liver transplantation, and it complements the NASPGHAN framework with practical guidance for resource-limited settings. [8]
[3]The evidence base for N-acetylcysteine in non-acetaminophen acute liver failure rests on the adult randomised trial showing improved transplant-free survival in early-stage disease and the paediatric safety and efficacy study confirming benefit in children. The King's College Criteria, derived from O'Grady's 1989 cohort of adults with fulminant hepatic failure, remain the most widely cited prognostic score in adults but have repeatedly underperformed in paediatric validation studies, which is why they are explicitly not recommended for paediatric transplant decisions. The outcome data from the paediatric acute liver failure study group, including the transplant listing analyses, provide the empirical foundation for the dynamic, trend-based paediatric approach. [2]
Exam Pearls
LIVER for the emergency priorities in paediatric acute liver failure
References
- [1]Squires JE, Alonso EM, Ibrahim SH, Kehar M, Martuszewski A, Rao S, et al North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition Position Paper on the Diagnosis and Management of Pediatric Acute Liver Failure. J Pediatr Gastroenterol Nutr, 2022.PMID 34347674
- [2]O'Grady JG, Alexander GJ, Hayllar KM, Williams R Early indicators of prognosis in fulminant hepatic failure. Gastroenterology, 1989.PMID 2490426
- [3]Lee WM, Hynan LS, Rossaro L, Fontana RJ, Stravitz RT, Larson AM, et al Intravenous N-acetylcysteine improves transplant-free survival in early stage non-acetaminophen acute liver failure. Gastroenterology, 2009.PMID 19524577
- [4]Kortsalioudaki C, Taylor RM, Cheeseman P, Bansal S, Mieli-Vergani G, Dhawan A Safety and efficacy of N-acetylcysteine in children with non-acetaminophen-induced acute liver failure. Liver Transpl, 2008.PMID 18161828
- [5]Squires JE, McKiernan P, Squires RH Acute Liver Failure: An Update. Clin Liver Dis, 2018.PMID 30266162
- [6]Devictor D, Tissieres P, Durand P, Debray D Acute liver failure in neonates, infants and children. Expert Rev Gastroenterol Hepatol, 2011.PMID 22017699
- [7]Kulkarni SS, Goss CW, Khan AS, Bezerra JA, Bucuvalas JC, Himes RW, et al Outcomes Analyses of Pediatric Acute Liver Failure Subjects Listed for Liver Transplantation. J Pediatr Gastroenterol Nutr, 2022.PMID 35442235
- [8]Lal BB, Khanna R, Sood V, Sharma MK, Wadhawan M, Alam S, et al Diagnosis and management of pediatric acute liver failure: consensus recommendations of the Indian Society of Pediatric Gastroenterology, Hepatology, and Nutrition (ISPGHAN). Hepatol Int, 2024.PMID 39212863
- [9]Pamecha V, Patil NS, Falari S, Goja S, Bhangui P, Kumar S, et al Live donor liver transplantation for pediatric acute liver failure: challenges and outcomes. Hepatol Int, 2023.PMID 37587287
- [10]Squires RH Jr Acute liver failure in children. Semin Liver Dis, 2008.PMID 18452115
- [11]Kerkar N, Rana A Wilson Disease in Children. Clin Liver Dis, 2022.PMID 35868686
- [12]Sorensen LG, Neighbors K, Hardison RM, Mazariegos GV, Squires RH, Alonso EM, et al Health Related Quality of Life and Neurocognitive Outcomes in the First Year after Pediatric Acute Liver Failure. J Pediatr, 2018.PMID 29551316