Paeds · gastroenterology-hepatology-and-nutrition
Acute vomiting in infants and children
Also known as Vomiting in children · Emesis in infants · Bilious vomiting · Projectile vomiting · Non-bilious vomiting · The vomiting child
Fellowship guide to acute vomiting in infants and children: the bilious-vomiting surgical emergency, the age-based differential from malrotation and pyloric stenosis to gastroenteritis and raised intracranial pressure, the vomiting reflex and its four afferent triggers, clinical dehydration assessment, oral rehydration and the role of ondansetron, the harmful-and-helpful antiemetic decision, and the dangerous non-gastrointestinal mimics of DKA, sepsis and brain tumour.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A green vomit in a newborn and a well toddler who vomits once after a viral tummy bug sit at opposite ends of the same complaint, and the whole art of managing the vomiting child is telling them apart quickly. Vomiting is the forceful, coordinated retrograde expulsion of gastric contents, driven by a brainstem reflex, and it must be separated from the effortless posseting and regurgitation of a thriving infant, which needs reassurance rather than investigation.[3]
Most acute vomiting in children is benign and self-limiting, usually viral gastroenteritis, and the task is to keep the child hydrated and safe at home.[2] The clinical danger is that the same symptom is the presenting sign of a short list of time-critical conditions: a twisting midgut, a telescoping bowel, a decompensating diabetic, an obstructing pylorus, an overwhelming sepsis, and a rising intracranial pressure. The examiner wants to see that you can hold the common and the catastrophic in mind at once.[10]
Classification
The single most useful first cut is the colour of the vomit, because it maps directly onto urgency. Bilious (green) vomiting means bile is refluxing above an obstruction distal to the ampulla of Vater, and in an infant it signals malrotation with midgut volvulus until imaging says otherwise.[10] Non-bilious vomiting is the reassuring colour but is not harmless, since it covers pyloric stenosis, gastroenteritis, reflux and the medical mimics.[6]
The second cut is the age of the child, because the differential shifts across childhood. A neonate who vomits raises malrotation, necrotising enterocolitis, sepsis and inborn errors of metabolism; an infant of two to eight weeks with projectile vomiting raises pyloric stenosis; a toddler raises gastroenteritis, intussusception and urinary infection; and a school-age child raises gastroenteritis, appendicitis, diabetic ketoacidosis, migraine and raised intracranial pressure.[2]
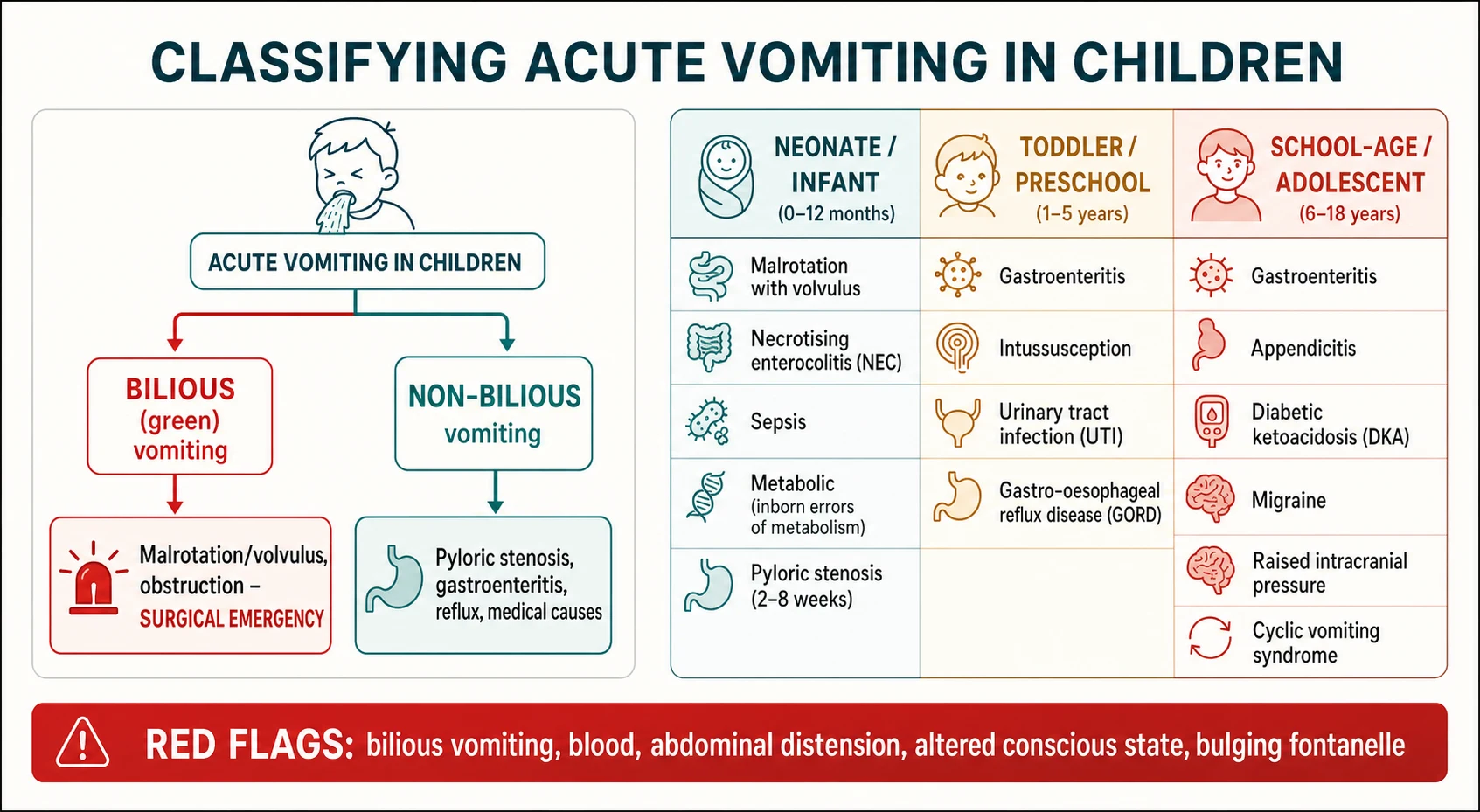
The third practical cut is surgical versus medical versus non-gastrointestinal. Surgical vomiting comes with obstruction or peritonism; medical gastrointestinal vomiting is gastroenteritis and reflux; and the non-gastrointestinal group covers infection outside the gut, metabolic crises, neurological pressure and toxins. Keeping these three buckets in view stops you anchoring on the gut when the cause is a brain tumour or a diabetic crisis.[13]
Epidemiology & Risk Factors
Acute gastroenteritis is the commonest cause of vomiting in children and one of the most frequent reasons for a paediatric presentation, with most young children experiencing several episodes in the first years of life.[2] Rotavirus was historically the dominant pathogen and remains important where vaccine coverage is low, while norovirus now drives much of the residual burden in high-coverage countries.[3]
The surgical causes are much rarer but concentrated in specific windows. Hypertrophic pyloric stenosis affects roughly two to four per 1000 live births, presents classically between two and eight weeks, and is around four to five times commoner in boys, with a well-recognised first-born male predominance.[6] Intussusception peaks between three months and two years and is the commonest cause of intestinal obstruction in this age group.[8]
Malrotation with volvulus most often declares itself in the first month of life, and a Canadian tertiary review confirmed that delays in recognising bilious vomiting still occur and cost bowel.[10] Risk factors that raise the stakes for any vomiting child include young age with its small fluid reserve, prematurity, congenital cardiac or gastrointestinal anomalies, immunocompromise, disability with feeding difficulty, and socioeconomic disadvantage that delays presentation and complicates home rehydration.[2]
Pathophysiology
Vomiting is orchestrated by a brainstem network in the medulla, sometimes called the vomiting centre, which receives four main afferent streams and, when triggered, coordinates the retrograde expulsion of gastric contents through the diaphragm and abdominal wall.[11] Understanding these four inputs explains both the differential and the choice of antiemetic.[11]
The first input is the chemoreceptor trigger zone in the area postrema, which lies outside the blood-brain barrier and samples the blood for drugs, toxins and metabolic derangements such as ketones and uraemia; this is the pathway that makes a child in diabetic ketoacidosis vomit.[12] The second is the vagal and splanchnic afferents from a distended, obstructed or inflamed gut, which drive the vomiting of pyloric stenosis, intussusception and gastroenteritis.[8]
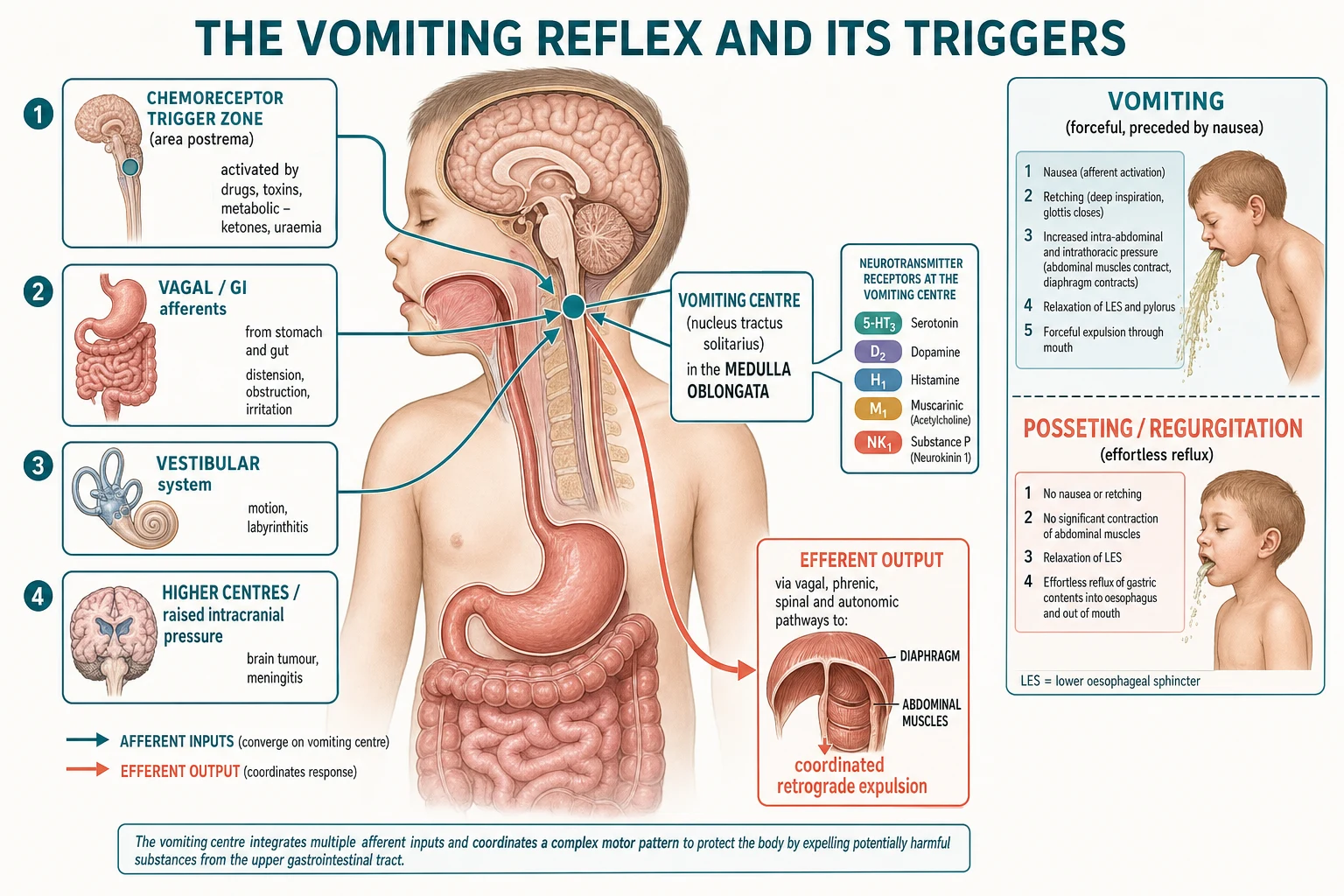
The third input is the vestibular apparatus, relevant in motion sickness and labyrinthitis, and the fourth is descending input from higher centres and, crucially, raised intracranial pressure, which produces the early-morning vomiting of a posterior fossa tumour.[13] Each pathway signals through characteristic receptors, which is why 5-HT3 antagonists such as ondansetron work well for the chemoreceptor and gut-driven vomiting of gastroenteritis and chemotherapy.[1]
The consequences of sustained vomiting flow from what is lost. Losing gastric fluid strips out hydrogen, chloride, potassium and sodium, and in pyloric stenosis this produces the classic hypochloraemic, hypokalaemic metabolic alkalosis, while the loss of any enteral intake in a small child rapidly causes dehydration, ketosis and, if severe, hypovolaemic shock.[6]
Clinical Presentation
The history does most of the diagnostic work. Ask the colour of the vomit first, then its force and timing, then whether it is bilious or blood-stained, then the pattern of feeds, stools and urine output, and finally the associated features of fever, pain, drowsiness, headache or rash.[3] A single reassuring examination is never enough in a young infant, whose deterioration can be rapid and whose signs are subtle.[10]
Gastroenteritis typically presents with vomiting that precedes or accompanies diarrhoea, often with low-grade fever and unwell contacts, and the vomiting usually settles within a day or two even when the diarrhoea persists.[2] Pyloric stenosis presents in a hungry infant of two to eight weeks with progressively projectile, non-bilious vomiting immediately after feeds, weight loss, and sometimes a visible left-to-right peristaltic wave and a palpable olive in the right upper quadrant.[6]
Intussusception classically presents with sudden, severe, colicky abdominal pain that comes in waves every 15 to 20 minutes, during which the child draws up the legs and screams, followed by pallor and lethargy between episodes; the late redcurrant-jelly stool is a sign of mucosal ischaemia and a reason to act sooner, not a diagnostic prerequisite.[8] The intervening lethargy can be so profound that a decreased conscious level, rather than the pain, is the presenting complaint.[8]
The dangerous non-gastrointestinal presentations must be actively sought. A child with diabetic ketoacidosis vomits, has abdominal pain, is dehydrated and breathes deeply; a child with raised intracranial pressure vomits in the early morning with headache, and may have abnormal eye movements or a change in behaviour; and a septic infant vomits, feeds poorly and is mottled and lethargic.[12]
Differential Diagnosis
The differential is best organised by age and by the surgical-medical-mimic framework rather than as a flat list. In the neonate, the priorities are malrotation with volvulus, necrotising enterocolitis, congenital obstruction such as duodenal or jejunal atresia, sepsis, and an inborn error of metabolism presenting with vomiting, poor feeding and encephalopathy.[10] Any bile in a neonatal vomit moves surgery to the top of the list.[10]
In the infant, pyloric stenosis is the classic non-bilious projectile presentation, while gastroenteritis, intussusception, urinary tract infection, gastro-oesophageal reflux, cow's milk protein allergy and overfeeding fill out the rest of the list.[6] The key discriminator between reflux and pyloric stenosis is the trajectory: reflux is effortless and the infant thrives, whereas pyloric vomiting is forceful, progressive and accompanied by weight loss.[6]
In the older child, gastroenteritis remains commonest, but appendicitis, diabetic ketoacidosis, urinary infection, migraine, raised intracranial pressure, toxic ingestion and cyclic vomiting syndrome all present with vomiting.[11] Appendicitis classically causes pain that precedes the vomiting, which is the reverse of the gastroenteritis sequence and a useful bedside discriminator.[2]
Cyclic vomiting syndrome deserves separate mention because it is a diagnosis of exclusion made only after structural, metabolic and neurological causes are ruled out; it presents with stereotyped, recurrent, self-limiting episodes of intense vomiting separated by symptom-free intervals, often with a personal or family history of migraine.[11]
Clinical & Bedside Assessment
Start with an across-the-room assessment of how sick the child looks, then move to airway, breathing, circulation and disability, because a drowsy or shocked vomiting child needs resuscitation before a diagnosis.[12] A capillary glucose is a mandatory early bedside test in any seriously vomiting child, as it detects both the hypoglycaemia of a metabolic crisis and the hyperglycaemia of diabetic ketoacidosis.[12]
The abdominal examination is directed at the surgical causes. Look for distension, feel for tenderness, guarding and masses, listen for the high-pitched or absent bowel sounds of obstruction, and in the young infant perform a test feed to look for a peristaltic wave and to palpate for a pyloric olive.[6] A rectal examination and inspection of the stool may reveal the blood of intussusception, and the hernial orifices must always be checked.[8]
Quantifying dehydration drives the fluid plan, and the most reliable clinical signs of significant dehydration are a prolonged capillary refill, abnormal skin turgor, an abnormal respiratory pattern and sunken eyes.[5] The Clinical Dehydration Scale, developed and then validated in young children with gastroenteritis, turns these signs into a reproducible score that separates minimal, some and moderate-to-severe dehydration.[4]
The synthesis for an exam is a one-sentence problem representation that names the age, the colour and pattern of the vomit, the hydration state and the leading diagnosis with its immediate plan. A model statement is that a three-week-old boy with two weeks of progressive non-bilious projectile vomiting, weight loss and a hypochloraemic alkalosis has pyloric stenosis and needs fluid and electrolyte correction before surgery.[6]
Investigations
Investigation is guided by the differential, not ordered as a reflex panel. A well, mildly dehydrated child with clear gastroenteritis needs no blood tests, and routine electrolytes are not required before oral rehydration.[3] When dehydration is moderate to severe, when intravenous fluids are started, or when the diagnosis is unclear, check urea, electrolytes, glucose, venous blood gas and ketones.[12]
In suspected pyloric stenosis the diagnostic test is an ultrasound showing a thickened, elongated pyloric muscle, and the essential blood test is a venous gas and electrolytes to detect the hypochloraemic, hypokalaemic metabolic alkalosis that must be corrected before theatre.[6] In suspected intussusception the investigation of choice is an abdominal ultrasound, which shows the target or doughnut sign with high sensitivity and specificity.[8]
When malrotation is suspected in a stable child, an urgent upper gastrointestinal contrast study is the gold standard, showing an abnormally placed duodenojejunal flexure and the corkscrew appearance of a volvulus; a shocked child with a surgical abdomen goes to theatre without waiting for imaging.[10] A urine sample for microscopy and culture is important in the vomiting infant, because urinary tract infection is a common and easily missed cause.[2]
Neuroimaging is reserved for the child with features of raised intracranial pressure, and the HeadSmart data underline that persistent vomiting combined with headache or neurological signs should trigger imaging rather than repeated reassurance.[13] A septic screen, including blood cultures and a lumbar puncture where meningitis is possible, is indicated in the unwell febrile infant.[2]
Management — Resuscitation
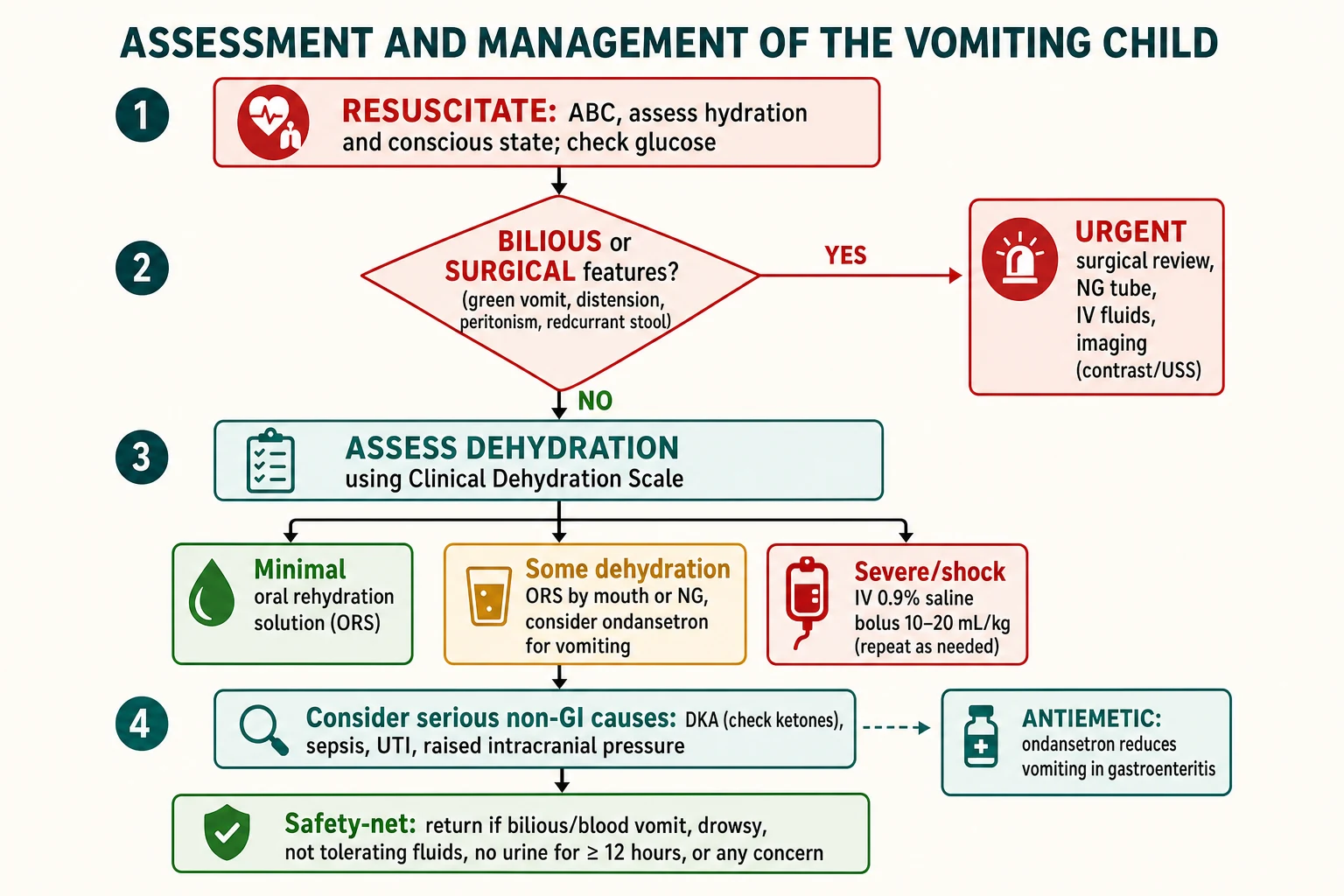
The first task in a sick vomiting child is to resuscitate before diagnosing: secure the airway, give oxygen if hypoxic, assess and support the circulation, and check a glucose.[12] A child in hypovolaemic shock from any cause receives a bolus of 10 to 20 mL/kg of isotonic crystalloid such as 0.9 per cent sodium chloride, reassessed after each bolus, with escalation to critical care if shock persists.[2]
The surgical emergencies interrupt the medical pathway. A child with bilious vomiting or signs of obstruction needs immediate surgical review, a wide-bore nasogastric tube on free drainage to decompress the stomach, nil by mouth, intravenous fluid resuscitation and maintenance, and urgent imaging or theatre; a suspected volvulus is a race against midgut infarction.[10] Do not persist with oral rehydration in a child who may have a surgical abdomen.[10]
Diabetic ketoacidosis has its own resuscitation rules that differ from routine shock. Fluids are given cautiously to avoid cerebral oedema, insulin is started after fluids and not as a bolus, potassium is replaced early, and the child is managed against a strict protocol with hourly neurological observations.[12] The take-home for the generalist is to recognise the ketoacidosis, avoid over-rapid fluids, and involve the diabetes and critical-care teams.[12]
Correct hypoglycaemia promptly with intravenous glucose, and remember that a young infant who has been vomiting and not feeding can become hypoglycaemic quickly, which itself causes further vomiting and drowsiness.[12] Antiemetics have no place in the initial resuscitation of a surgical or undiagnosed abdomen, where they mask progression.[1]
Management — Definitive & Stepwise
For the common problem of gastroenteritis, oral rehydration therapy is the first-line treatment for mild and moderate dehydration and is as effective as intravenous fluids with fewer complications.[2] Give a hypo-osmolar oral rehydration solution in small, frequent amounts, replacing the estimated deficit over about four hours, and continue breastfeeding throughout.[3]
A single dose of oral ondansetron reduces vomiting, increases the success of oral rehydration and reduces the need for intravenous fluids and admission in children with gastroenteritis, and it is the one antiemetic with strong paediatric evidence.[1] It is used selectively to rescue oral rehydration in the vomiting child rather than routinely, and metoclopramide and prochlorperazine are avoided in young children because of extrapyramidal side effects.[1]
Red flags in the vomiting child — 'VOMITING'
The definitive treatment of the surgical causes is procedural. Pyloric stenosis is corrected by pyloromyotomy after the electrolyte derangement is corrected, and both the open and laparoscopic approaches are effective, with the laparoscopic route offering faster recovery in trained hands.[7] Intussusception in a stable child is reduced non-operatively by air or hydrostatic enema, which succeeds in most cases and avoids surgery, with surgery reserved for failed reduction, perforation or peritonitis.[9]
If intravenous rehydration is needed, replace the deficit and provide maintenance with an isotonic fluid, monitor electrolytes and glucose, and reintroduce oral feeds early once vomiting settles, because prolonged gut rest offers no benefit.[2] Probiotics were once widely recommended but a large multicentre trial found no benefit in children with gastroenteritis, and they are no longer routinely advised.[14]
Specific Subtypes & Scenarios
The bilious-vomiting neonate is the scenario examiners return to most, because the stakes and the required speed are highest. A newborn with green vomit needs a nil-by-mouth order, a nasogastric tube, intravenous fluids, an immediate surgical opinion and an urgent contrast study, because malrotation with volvulus can infarct the midgut and the delay from a missed diagnosis is measured in lost bowel.[10]
Pyloric stenosis is the classic metabolic subtype. The infant loses acid and chloride in the vomit, producing a hypochloraemic, hypokalaemic metabolic alkalosis with paradoxical aciduria, and the correct order of management is always fluid and electrolyte resuscitation first and surgery second, because operating on an alkalotic infant risks postoperative apnoea.[6]
Intussusception in the toddler is the classic non-operative-reduction scenario. A stable child with a confirmed ileocolic intussusception and no signs of perforation is reduced by an air or hydrostatic enema under radiological control, and the family is warned about the small risk of recurrence in the following days.[9] A shocked child, or one with peritonitis or perforation, goes to theatre.[8]
Cyclic vomiting syndrome is the recurrent scenario in an older child. Once structural and metabolic causes are excluded, management combines avoidance of triggers, abortive treatment of acute episodes with rehydration and antiemetics, and prophylaxis in frequent cases, often with agents borrowed from migraine practice.[11] A raised-intracranial-pressure presentation, such as a posterior fossa tumour, must always be considered before the label of cyclic vomiting is applied.[13]
Complications & Pitfalls
The complications of vomiting itself are dehydration, electrolyte disturbance, hypoglycaemia, aspiration and, with forceful vomiting, a Mallory-Weiss mucosal tear.[2] The complications of the underlying cause are far more serious: midgut infarction from a missed volvulus, bowel ischaemia and perforation from an unreduced intussusception, and cerebral oedema from mismanaged diabetic ketoacidosis.[12]
The classic pitfalls are worth memorising because examiners return to them. The first is treating bilious vomiting as gastroenteritis and losing the bowel to volvulus.[10] The second is missing pyloric stenosis by not weighing the infant or not checking a gas, and operating before correcting the alkalosis.[6]
The third pitfall is anchoring on the gut and missing raised intracranial pressure, so that a child with early-morning vomiting and subtle neurology is repeatedly reassured until the tumour is advanced.[13] The fourth is failing to check a glucose in a drowsy vomiting child and missing hypoglycaemia or ketoacidosis.[12]
The fifth is over-investigating the well child: routine bloods, antiemetics and admission for a thriving toddler with a single day of viral vomiting cause harm and cost without benefit, when a good history, examination, oral rehydration and a clear safety-net are the correct management.[3]
Prognosis & Disposition
Most acute vomiting in children resolves quickly with supportive care, and a well child who tolerates oral rehydration, is not clinically dehydrated, has a benign abdomen and a caregiver who understands the safety-net can be managed at home.[3] The vomiting of gastroenteritis usually settles within a day or two even when diarrhoea continues, and full recovery is the rule.[2]
The surgical causes have excellent outcomes when treated early. Pyloromyotomy is curative with a low complication rate, and intussusception reduced promptly by enema has a good prognosis, but both deteriorate sharply if diagnosis is delayed.[7] The prognosis of malrotation with volvulus depends almost entirely on how fast it reaches theatre, which is why bilious vomiting is a time-critical emergency.[10]
The disposition thresholds for admission are failure of oral rehydration, moderate-to-severe or worsening dehydration, a suspected surgical or metabolic cause, an unwell or high-risk infant, or social circumstances that make safe home care unlikely.[2] A child discharged home is given clear return advice and, where needed, early review.[3]
Special Populations
Young infants are the highest-risk group because their small fluid reserve, immature physiology and non-specific signs allow rapid deterioration, and the surgical and metabolic emergencies cluster in the first weeks of life.[10] Any vomiting neonate deserves a lower threshold for assessment, a glucose and, if the vomit is bilious, an immediate surgical opinion.[10]
Children with disability, neurodevelopmental conditions or feeding difficulty may have atypical or attributed vomiting, and there is a real risk of diagnostic overshadowing in which a serious cause is dismissed as part of the underlying condition; each new pattern of vomiting deserves fresh assessment.[2] Children with diabetes need explicit sick-day rules, because vomiting can precipitate ketoacidosis and must never be assumed to be simple gastroenteritis.[12]
Indigenous children and those in rural and remote communities may present later, have less access to surgical services, and carry a higher burden of gastroenteritis and its complications; a bilious-vomiting neonate in a remote centre is a retrieval priority.[2] Socioeconomic disadvantage compounds the risk through delayed presentation and the practical difficulty of maintaining home oral rehydration, so the safety-net conversation must be concrete and the follow-up accessible.[3]
Immunocompromised children, including those on chemotherapy, both vomit from their treatment and are at higher risk of serious infection, and their vomiting is managed with a lower threshold for investigation and admission and with effective antiemetics such as ondansetron.[1]
Evidence, Guidelines & Regional Differences
The management of the commonest cause rests on well-established evidence. The ESPGHAN and ESPID European guidelines and the NICE guidance on diarrhoea and vomiting in children under five both endorse oral rehydration with a hypo-osmolar solution as first-line, early refeeding, and a selective rather than routine role for medication.[2] These two documents are the anchor references for any exam answer on gastroenteritis.[3]
The evidence for ondansetron is strong and practice-changing. A landmark emergency-department randomised trial showed that a single oral dose reduced vomiting and the need for intravenous fluids, and it has since become the standard antiemetic where one is indicated, always used as an adjunct to oral rehydration rather than a substitute.[1] The evidence against routine probiotics is equally clear, with a large multicentre trial showing no benefit in acute gastroenteritis.[14]
The surgical evidence favours minimally invasive and non-operative approaches where possible. A Cochrane review found open and laparoscopic pyloromyotomy comparably safe and effective, and a meta-analysis of enema reduction for intussusception supports non-operative reduction, with the choice between air and hydrostatic enema guided by local expertise.[7] Regional practice differs mainly in operational detail: rotavirus vaccination coverage shapes the gastroenteritis burden, and access to paediatric surgery and retrieval shapes how quickly the bilious-vomiting infant reaches definitive care.[9]
The diagnostic-delay literature is a recurring theme across the dangerous causes. The HeadSmart work quantified the diagnostic interval for childhood brain tumours and drove awareness that persistent vomiting with neurological features warrants imaging, and the malrotation delay data make the same point for bilious vomiting.[13]
Exam Pearls
Carry these single-testable facts into the written and clinical exam. Bilious vomiting is a surgical emergency at any age. A glucose is mandatory in every seriously vomiting child. Pyloric stenosis presents at two to eight weeks with projectile non-bilious vomiting and a hypochloraemic, hypokalaemic metabolic alkalosis that must be corrected before surgery.[6]
Intussusception presents with colicky pain, lethargy between episodes and a target sign on ultrasound, and is reduced first by air or hydrostatic enema.[9] Oral rehydration solution is first-line for mild and moderate dehydration, ondansetron is used to rescue oral rehydration in the vomiting child, and metoclopramide is avoided in young children because of extrapyramidal effects.[1]
The dangerous mimics are the marks that separate a safe candidate: diabetic ketoacidosis, sepsis and raised intracranial pressure all present with vomiting, and each is missed by anchoring on the gut.[12] Early-morning vomiting with headache or abnormal eye movements is raised intracranial pressure until neuroimaging proves otherwise, and the Clinical Dehydration Scale should replace a subjective guess when grading fluid loss.[13]
References
- [1]Freedman SB, Adler M, Seshadri R, et al. Oral ondansetron for gastroenteritis in a pediatric emergency department. N Engl J Med, 2006.PMID 16625009
- [2]Guarino A, Ashkenazi S, Gendrel D, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. J Pediatr Gastroenterol Nutr, 2014.PMID 24739189
- [3]Khanna R, Lakhanpaul M, Burman-Roy S, et al. Diarrhoea and vomiting caused by gastroenteritis in children under 5 years: summary of NICE guidance. BMJ, 2009.PMID 19386673
- [4]Friedman JN, Goldman RD, Srivastava R, et al. Development of a clinical dehydration scale for use in children between 1 and 36 months of age. J Pediatr, 2004.PMID 15289767
- [5]Goldman RD, Friedman JN, Parkin PC Validation of the clinical dehydration scale for children with acute gastroenteritis. Pediatrics, 2008.PMID 18762524
- [6]Vinycomb TI, Laslett K, Gwini SM, et al. Presentation and outcomes in hypertrophic pyloric stenosis: An 11-year review. J Paediatr Child Health, 2019.PMID 30677197
- [7]Staerkle RF, Lunger F, Fink L, et al. Open versus laparoscopic pyloromyotomy for pyloric stenosis. Cochrane Database Syst Rev, 2021.PMID 33686649
- [8]del-Pozo G, Albillos JC, Tejedor D, et al. Intussusception in children: current concepts in diagnosis and enema reduction. Radiographics, 1999.PMID 10194781
- [9]Liu L, Zhang L, Fang Y, et al. Air enema reduction versus hydrostatic enema reduction for intussusceptions in children: A systematic review and meta-analysis. PLoS One, 2024.PMID 38498581
- [10]Filion L, Beaunoyer M, Miron MC, et al. Infant malrotation with midgut volvulus: A retrospective review of clinical presentation and delays in care at a Canadian tertiary paediatric centre. Paediatr Child Health, 2025.PMID 41049711
- [11]Li BUK Managing cyclic vomiting syndrome in children: beyond the guidelines. Eur J Pediatr, 2018.PMID 30076469
- [12]Wolfsdorf JI, Glaser N, Agus M, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Pediatr Diabetes, 2018.PMID 29900641
- [13]Shanmugavadivel D, Liu JF, Murphy L, et al. Accelerating diagnosis for childhood brain tumours: an analysis of the HeadSmart UK population data. Arch Dis Child, 2020.PMID 31653616
- [14]Freedman SB, Williamson-Urquhart S, Farion KJ, et al. Multicenter Trial of a Combination Probiotic for Children with Gastroenteritis. N Engl J Med, 2018.PMID 30462939