Paeds · gastroenterology-hepatology-and-nutrition
Appendicitis and surgical abdomen
Also known as Acute appendicitis · Pediatric appendicitis score · Migratory right iliac fossa pain · McBurney point tenderness · Perforated appendicitis · Appendiceal mass · Laparoscopic appendicectomy · Non-operative appendicitis · Surgical abdomen · Fecolith
Fellowship guide to appendicitis as the paradigm of the paediatric surgical abdomen, built around the child with periumbilical pain that migrates to the right iliac fossa with anorexia, nausea and localised tenderness. The page covers the obstruct-ischaemia-perforate pathophysiology, the ten-point Pediatric Appendicitis Score, ultrasound as first-line imaging with magnetic resonance imaging as the radiation-sparing second line, resuscitation and analgesia that never delay diagnosis, laparoscopic appendicectomy as the standard against the evolving non-operative antibiotic option chosen by shared decision, and the recognition of the sick surgical abdomen in which a bilious vomit, guarding, a rigid abdomen or a torsed testis must never be missed.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture an eight-year-old who felt vaguely off at breakfast, refused his cereal, and by evening is curled on the sofa pointing to a sore spot just inside his right hip bone. That arc, from a vague central ache to a sharp, localised right iliac fossa pain with loss of appetite, is the signature of acute appendicitis. It is the commonest abdominal surgical emergency of childhood, and the condition that defines what examiners call the surgical abdomen: a child whose pain signals a problem that an operation, not a prescription, will solve. [3] [4]
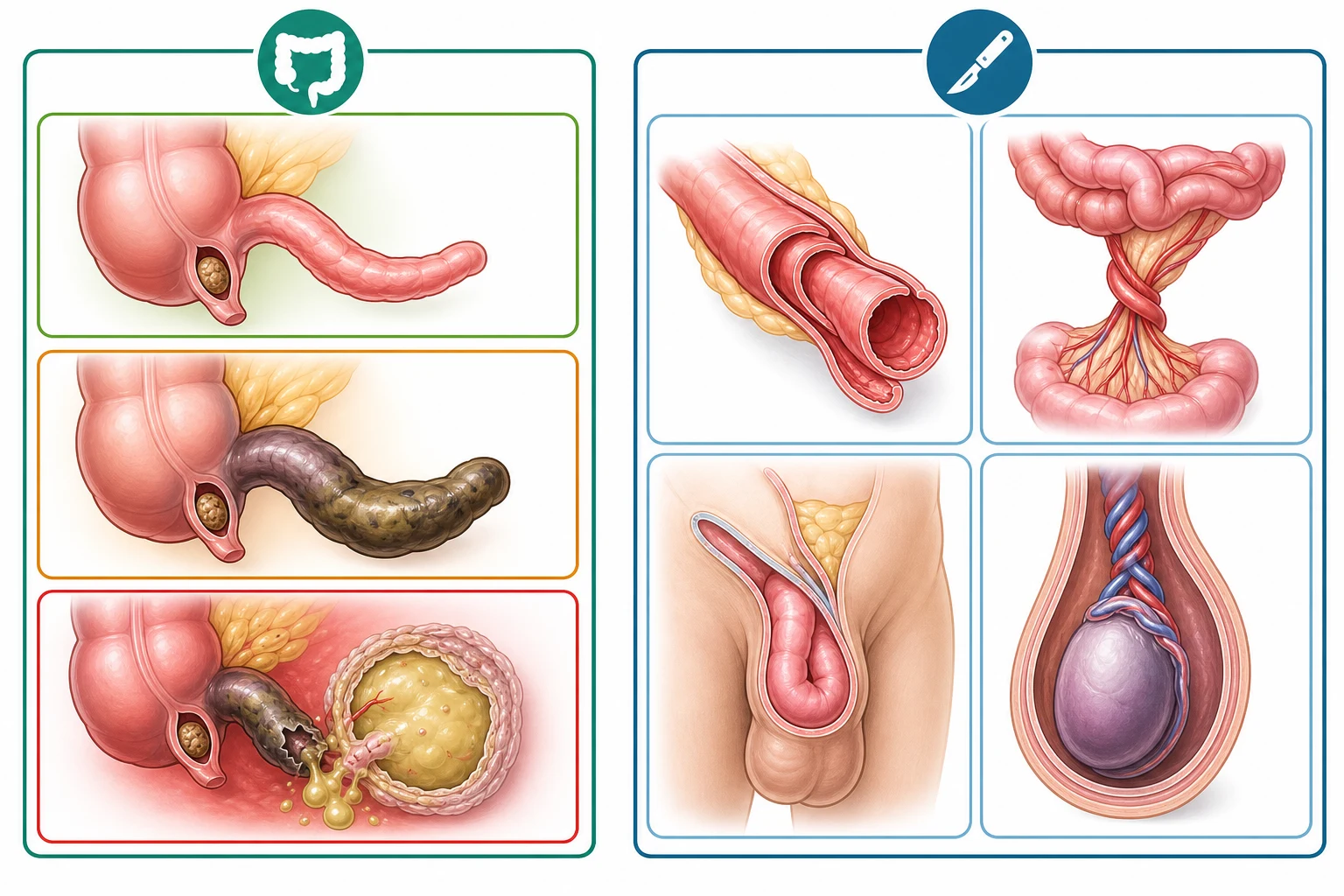
The danger unfolds in two ways. Locally, the obstructed appendix swells, becomes ischaemic and may perforate, spilling pus to cause peritonitis or a walled-off abscess. Systemically, a missed surgical abdomen such as a midgut volvulus, an incarcerated hernia or a torsed testis can cost bowel or a gonad within hours, which is why the discipline of the acute abdomen is to recognise the surgical patient first and name the diagnosis second. The art is to act on the migratory pain and the tenderness before the perforation arrives. [3] [1]
The governing principle is therefore recognition coupled with a graded response. You assess and resuscitate, apply the Pediatric Appendicitis Score to stratify risk, image with ultrasound first and reserve second-line magnetic resonance imaging or computed tomography for the equivocal case, and then choose between laparoscopic appendicectomy and, for selected uncomplicated cases, non-operative antibiotics through shared decision. Most children do well, which is exactly why catching the pattern early matters. [3] [6]
Classification
Sort the child at the bedside first by whether the abdomen is surgical or medical, because that single call sets the pace. A surgical abdomen is one in which a viscus is obstructed, ischaemic, torsed or perforated, and the red flags are a bilious vomit, colicky pain with distension, guarding and rigidity, a rigid or silent abdomen, shock, or a tender irreducible lump. Appendicitis is the paradigm of the inflammatory-perforating surgical abdomen, but it shares the triage with obstructive and ischaemic emergencies that must never be missed. [3]
Within appendicitis itself, the severity classification governs the operation and the antibiotics. Uncomplicated or simple appendicitis is an inflamed but intact, non-perforated appendix, and it is the case that may be managed non-operatively or with a straightforward laparoscopic appendicectomy and minimal antibiotics. Complicated appendicitis spans gangrenous change with a necrotic wall, frank perforation with purulent or faecal peritonitis, and a walled-off appendiceal mass or abscess, and it demands surgery, a longer antibiotic course and a longer stay. [3] [12]
Simple appendicitis
- Inflamed but intact, non-perforated appendix
- Localised right iliac fossa pain and tenderness
- Laparoscopic appendicectomy with short antibiotics
- Eligible for non-operative antibiotics by shared decision
Complicated
- Gangrenous wall, perforation, abscess or mass
- Diffuse pain, guarding, fever, longer history in the young
- Surgery plus a prolonged intravenous antibiotic course
- Higher risk of wound infection, ileus and abscess
Surgical abdomen
- A viscus obstructed, torsed, ischaemic or perforated
- Bilious vomit, guarding, rigidity, shock or an irreducible lump
- Includes volvulus, intussusception, hernia and torsion
- Needs a surgeon, resuscitation and often the theatre
Epidemiology & Risk Factors
Appendicitis is principally a disease of older children and adolescents. The incidence rises steadily through the school-age years to a peak in the second decade, it is rare under two, and a slight male predominance runs through the series. Lifetime risk sits around seven to nine percent in the classic epidemiology, making it the commonest reason a child comes to an emergency department with an acute surgical abdomen. [4] [3]
Age bends the presentation and the perforation rate in an exam-critical way. The preschool child under five often cannot localise pain, has a short and atypical history, and presents late, so perforation is already present in roughly half to two-thirds of these young children at diagnosis, against about a fifth in adolescents. A family history of appendicitis and a fecalith raise the risk, and the seasonal peaks mirror respiratory and gastrointestinal illness. The lesson is simple and load-bearing: the younger the child, the lower the threshold for imaging and surgical review. [4] [1]
Pathophysiology
The mechanism is one of luminal obstruction running away into ischaemia. In most children a fecalith or a swollen lymphoid follicle blocks the narrow appendiceal lumen, the mucus secreted behind the blockage accumulates, and the appendix distends. Bacteria, chiefly Escherichia coli and Bacteroides, multiply in the trapped mucus, and the rising intraluminal pressure first compresses the thin-walled veins and lymphatics and then the arterial supply. [3] [1]
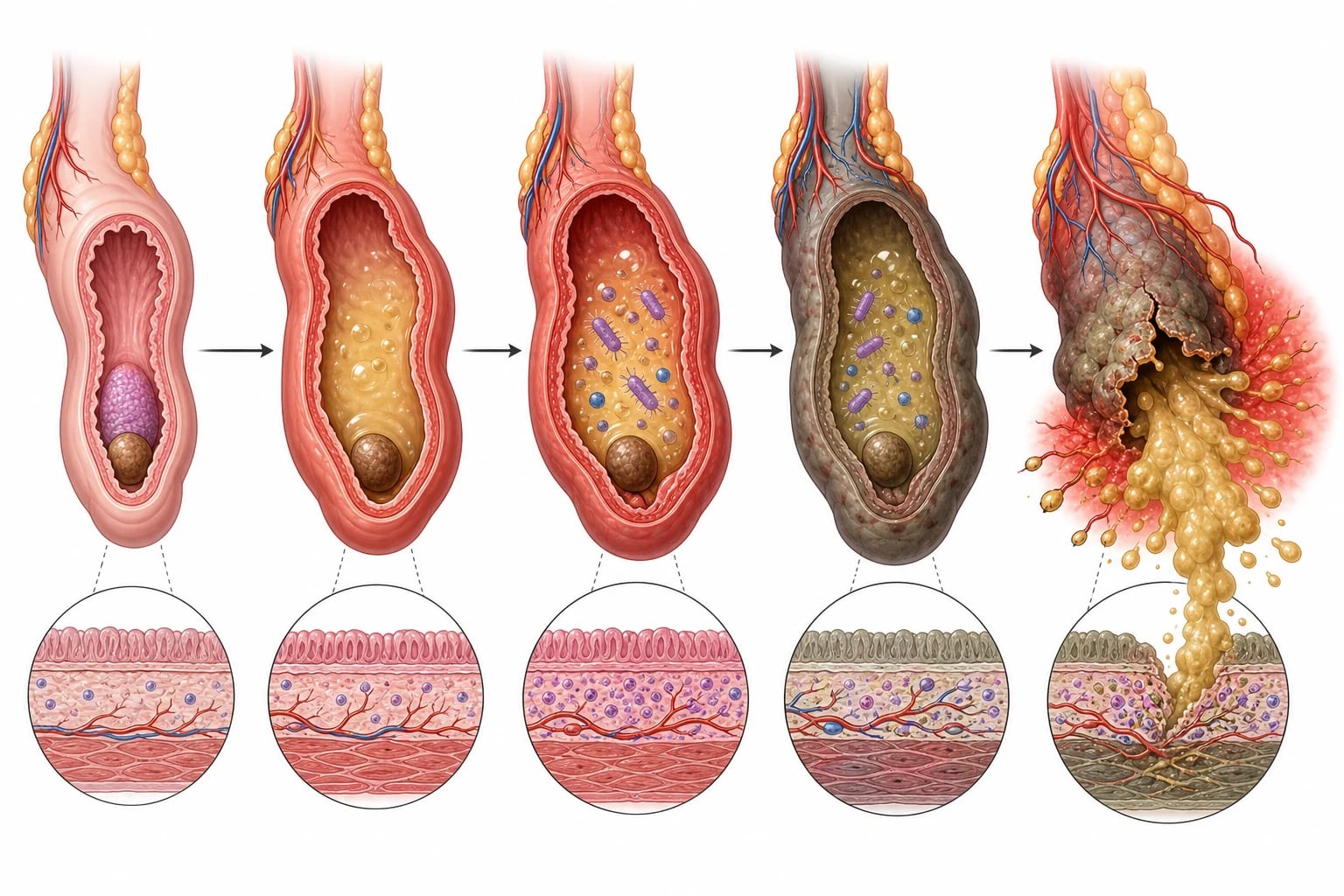
As the venous return is cut off, the wall becomes oedematous and ischaemic, the mucosa ulcerates, and full-thickness necrosis produces a gangrenous appendix that is poised to perforate. Once it ruptures, pus and faeculent material spill into the peritoneal cavity to cause diffuse peritonitis, or the omentum and bowel wall it off to form an appendiceal mass or abscess. The whole sequence typically runs over twenty-four to forty-eight hours in the older child, but it accelerates and is often complete at presentation in the preschool child. [3] [12]
The clinical signs follow directly from this anatomy. The visceral pain of early distension is felt in the peri-umbilical region because the midgut shares that embryological dermatome, and it migrates to the right iliac fossa only when the inflamed parietal peritoneum over the appendix is irritated, which is why migration is so specific. Localised tenderness, rebound and guarding are the somatic echo of that parietal irritation, and a cough, a hop or apercussion jolt reproduces them because they shake the inflamed peritoneum. [1] [3]
Clinical Presentation
The presentation is orderly and distinctive, and recognising its sequence is the whole skill. A previously well child develops a vague, central, peri-umbilical ache that over the next twelve to twenty-four hours shifts and sharpens into a localised right iliac fossa pain. Anorexia is the most consistent companion feature, nausea and vomiting follow the onset of pain rather than precede it, and a low-grade fever appears as the inflammation establishes. [1] [2]
The right iliac fossa holds the findings. Tenderness localises at McBurney point, about a third of the way from the anterior superior iliac spine to the umbilicus, and rebound tenderness, guarding and rigidity reflect peritoneal irritation. Indirect signs help when the appendix lies oddly: Rovsing sign is right-sided pain on palpating the left iliac fossa, the psoas sign is pain on extending the hip for a retrocaecal appendix, and the obturator sign is pain on internal rotation for a pelvic appendix. [1] [3]
Atypical positions deceive. A pelvic appendix may cause dysuria, diarrhoea and suprapubic tenderness rather than right iliac fossa pain, a retrocaecal appendix hides behind the caecum and produces a quieter abdomen with a positive psoas sign, and a post-ileal appendix presents with vomiting and central pain that mimics obstruction. The young child may simply refuse to walk or to hop, cry on movement, or lie still, and that immobility in a previously active child is itself a sign of peritoneal irritation. [3] [2]
As the hours pass the picture darkens toward the complicated end. A spiking fever, a rigid abdomen, increasing distension and systemic toxicity signal perforation and peritonitis, while a tender mass may mark a walled-off abscess. Shock, with tachycardia, cool peripheries and a falling conscious state, transforms the picture into the resuscitation-first, theatre-next scenario that every candidate must own. [3] [12]
Differential Diagnosis
The differential clusters around the child with acute abdominal pain, and the first task is to separate the surgical emergencies from the medical mimics. Among the surgical causes, malrotation with midgut volvulus presents with bilious vomiting and must not be missed, intussusception brings rhythmic colicky pain and a mass in an infant, an incarcerated inguinal hernia is found by examining the groins, and Meckel diverticulitis can mimic appendicitis closely. [3]
The non-abdominal and atypical surgical causes are the classic traps. Testicular torsion presents as lower abdominal or groin pain, which is why every boy with abdominal pain must have the testes examined, and a lower-lobe pneumonia can cause referred abdominal pain and fever that masquerades as a surgical abdomen. In adolescent girls, ovarian torsion, a ruptured ovarian cyst, pelvic inflammatory disease and a tubal pregnancy must enter the differential, and a pregnancy test is part of the work-up. [3] [1]
Appendicitis
- Migratory peri-umbilical to right iliac fossa pain
- Anorexia, nausea after pain, low-grade fever
- McBurney point tenderness with rebound and guarding
- Ultrasound first, appendicectomy or non-operative care
Mesenteric adenitis
- Often follows a viral upper respiratory infection
- Pain less localised and less progressive
- Higher fever, widespread lymphadenopathy
- A diagnosis of exclusion after appendicitis is ruled out
Midgut volvulus
- Bilious vomiting in a previously well child
- Upper gastrointestinal contrast study is key
- Emergency Ladd procedure, not observation
- The bilious vomit must never be reassured away
The medical mimics round out the list. Acute gastroenteritis, urinary tract infection and constipation are common and usually distinguished by their dominant features, while mesenteric adenitis is the classic mimic that is diagnosed only after appendicitis is excluded. Diabetic ketoacidosis can present with abdominal pain and vomiting, and Henoch-Schonlein purpura causes colicky pain and sometimes an ileoileal intussusception. The discipline is to reach for the ultrasound and the surgeon whenever the pattern even hints at a surgical cause. [1] [3]
Clinical & Bedside Assessment
The assessment runs alongside resuscitation, never after it. Confirm the sequence yourself by asking whether the pain moved, whether the child is eating, and whether vomiting followed the pain, because that order is more discriminating than any single sign. Examine the airway, breathing and circulation first, since a child with a perforated appendix may already be dehydrated or septic, and grade the degree of dehydration against a recent weight. [1] [2]
The examination is systematic and includes the parts that catch the mimics. Inspect and gently palpate the abdomen for the point of maximal tenderness and for guarding, listen for bowel sounds, and examine the groin hernial orifices in every case because an incarcerated hernia is a quickly reversible mimic. Examine the testes in every boy, the lungs for a lower-lobe pneumonia, and perform a urinalysis, because a missed torsion, pneumonia or urinary infection is the classic avoidable error. [3] [1]
Serial reassessment is the safety net for the equivocal child. A child with a low probability score and a normal or equivocal ultrasound is observed with repeated examination over hours rather than discharged on a single assessment, because appendicitis declares itself by progression. Document the time course, reassess the tenderness and the vital signs, and have a low threshold to re-image or to involve the surgeon if the picture evolves. [2] [3]
Investigations
The Pediatric Appendicitis Score structures the bedside risk, and every candidate must know its ten points. Samuel described the score from a peri-umbilical-to-right-iliac-fossa population, and it assigns one point each for nausea or vomiting, migration of pain, anorexia, fever of 38 degrees or more, a white cell count over ten, and a neutrophil left shift, and two points each for right iliac fossa tenderness and for cough, percussion or hopping tenderness. Scores of 2 or below make appendicitis unlikely, 7 or above make it likely, and the broad middle requires imaging or active observation. [1] [2]
Pediatric Appendicitis Score — the ten-point PAST RICS
Ultrasound is the first-line investigation and the radiation-sparing workhorse of the paediatric pathway. A non-compressible blind-ending tube over 6 millimetres in diameter with wall thickening and surrounding inflammatory change confirms appendicitis at the bedside, and a confident positive scan is enough to proceed. Its sensitivity is operator- and patient-dependent and runs around three-quarters to nine-tenths, so a negative or equivocal scan in a child with ongoing concern must not dismiss the diagnosis. [6] [3]
Blood and urine tests serve the child and the decision rather than the diagnosis alone. A full blood count, C-reactive protein, electrolytes and a group and save are taken when the child is unwell or surgery is likely, and a raised white cell count with a left shift and a rising C-reactive protein support an inflammatory process. Urinalysis excludes a urinary infection and, in an adolescent girl, a pregnancy test rules out an ectopic pregnancy before any imaging or surgery. [3] [1]
Management — Resuscitation
Resuscitation runs in parallel with the surgical referral, never sequentially. Keep the child nil by mouth, secure intravenous access, and pass a nasogastric tube only if there is vomiting, distension or a concern about obstruction. Provide effective analgesia, because the evidence is clear that opioid analgesia does not obscure the abdominal examination or delay the diagnosis, and leaving a child in pain is neither diagnostic nor kind. [3] [1]
Correct the fluid deficit briskly. Give an intravenous bolus of 10 to 20 mL per kilogram of isotonic crystalloid such as 0.9 percent sodium chloride or a balanced salt solution, reassess the perfusion and the capillary refill, and repeat as needed for dehydration or shock before moving to maintenance fluid. Check the glucose in any unwell young child, who is at risk of hypoglycaemia from poor intake, and give an antiemetic for persistent vomiting. [3] [12]
Isotonic crystalloid fluid bolus
Dose
10 to 20 mL per kilogram intravenously, reassess and repeat as needed for dehydration or shock
Involve the paediatric surgeon early and together with the radiologist, and start broad-spectrum intravenous antibiotics when perforation or complicated appendicitis is suspected. A regimen such as ceftriaxone with metronidazole covers the typical enteric Gram-negative and anaerobic flora, and it is continued postoperatively according to the severity. The aim of this phase is to deliver a well-resuscitated, comfortable child to the imaging suite or the theatre, not a dry, in-pain child in shock. [11] [3]
Management — Definitive & Stepwise
Definitive treatment follows one rule: remove the appendix when it is safe and necessary, and consider antibiotics alone only for selected uncomplicated cases through an explicit shared decision. The whole pathway runs from recognition and scoring, through ultrasound and second-line imaging, to the choice between laparoscopic appendicectomy and non-operative antibiotics, and finally to the management of perforation and the appendiceal mass. [3] [8]
Laparoscopic appendicectomy is the standard definitive treatment for confirmed appendicitis, and it is preferred over the open approach for its shorter stay, less pain and lower wound infection rate. It is performed under general anaesthesia soon after resuscitation for the straightforward case, and it is converted to an open operation or extended for the perforated appendix with diffuse peritonitis. Simple, non-perforated appendicitis needs only perioperative prophylaxis, while complicated disease needs a defined postoperative antibiotic course. [3] [12]
Appendicitis antibiotic regimen
Dose
Ceftriaxone 50 mg per kilogram intravenously once daily with metronidazole 7.5 mg per kilogram intravenously every eight hours; perioperative prophylaxis only for simple disease, prolonged for perforation
Non-operative management with antibiotics alone is an accepted option for selected children with uncomplicated appendicitis, chosen through shared decision-making with the family. The landmark adult trial showed antibiotics resolved about three-quarters of uncomplicated cases at one year, and the paediatric experience is similar at short term, but the advantage narrows over time as recurrence accumulates and about two-fifths of those treated non-operatively come to appendectomy within a few years. Candidates must have a clearly uncomplicated appendix, no evidence of perforation or a fecalith that predicts failure, and a family who understands the trade-off and the need to return. [5] [9]
The choice between surgery and antibiotics is explicitly a shared decision, and the evidence frames its terms. Non-operative management fails more often in children with a fecalith and in those with higher symptom scores, and a patient-activation tool has been shown to help families reach a choice consistent with their values. The reflex is therefore to lay out the one-year success of around three-quarters, the accumulating long-term recurrence, and the option of surgery, and to let an informed family decide rather than defaulting one way. [7] [8]
Specific Subtypes & Scenarios
Perforated appendicitis is the scenario that dominates the young child and the late presentation. A perforation produces purulent or faeculent peritonitis or a walled-off abscess, and it demands laparoscopic or open appendicectomy with a thorough washout and a prolonged intravenous antibiotic course guided by the clinical response. The duration is dictated by the return of fever control, a falling inflammatory marker and the resumption of feeding, rather than by a fixed number of days. [3] [12]
The appendiceal mass or abscess sits at the complicated end and is managed non-operatively at first. A stable child with a well-contained abscess is treated with broad-spectrum intravenous antibiotics, with percutaneous drainage when the collection is large or persistent, and surgery is reserved for failure or deterioration. Interval appendicectomy after resolution was once routine, but a systematic review found recurrent appendicitis after successful non-operative treatment of a mass or abscess to be modest, so the practice is increasingly selective rather than universal. [10] [3]
The atypical and young-child scenarios deserve a separate suspicion. A preschool child with a short, vague history is often perforated at presentation and needs a low threshold for imaging and surgery, while a pelvic or retrocaecal appendix may present with dysuria, diarrhoea or a positive psoas sign rather than classic right iliac fossa tenderness. The non-operative candidate is a distinct population too, defined by an uncomplicated appendix, no fecalith and an informed family, and counselled about the accumulating long-term recurrence. [4] [9]
Complications & Pitfalls
The complications follow the twin threats of perforation and delay. Perforation leads to peritonitis, intra-abdominal abscess, wound infection, postoperative ileus and, rarely, portal pyelophlebitis with liver abscesses, while extensive contamination in the very young can leave adhesions and, exceptionally, bowel obstruction or infertility concerns in girls. Early appendicectomy prevents most of these, which is why time to surgery for the perforated case is a key prognostic lever. [3] [12]
The pitfalls cluster around underestimating the atypical presentation and over-relying on a single tool. The commonest error is to dismiss the anorectic, tender child because the white cell count is normal or the ultrasound is equivocal, when appendicitis is a clinical diagnosis supported by investigations rather than the reverse. A second error is to treat a bilious vomit as gastroenteritis and miss a midgut volvulus, and a third is to forget the testes and the lungs in a child with abdominal pain. [1] [3]
Stump appendicitis, though rare, is the late pitfall after appendicectomy, in which the residual stump becomes inflamed, and it must be considered in any child with right iliac fossa pain after a previous appendicectomy. The broader message is that a negative appendicectomy rate is acceptable and preferable to a missed or perforated appendix, so the threshold to operate on a convincing clinical picture, even with normal imaging, remains defensible. [3] [2]
Prognosis & Disposition
Outcome is dominated by whether the appendix has perforated and by the speed of recognition. Simple appendicitis treated by timely laparoscopic appendicectomy has an excellent prognosis, a short hospital stay and a swift return to normal activity. Perforated appendicitis carries a longer stay, a higher complication rate and a greater antibiotic burden, which is why catching the disease before it perforates, especially in the young child, is the central prognostic goal. [3] [12]
For the uncomplicated case, the time to theatre is less critical than for the perforated one, and a stable child can wait for a daytime list without a rise in perforation or complication, provided they are observed and resuscitated. This evidence reassures the candidate who fears that every appendicitis is an immediate emergency, while sharpening the distinction from the perforated or ischaemic abdomen that cannot wait. [3] [10]
Disposition reflects the acuity and the access. A confirmed or suspected appendicitis needs a centre with paediatric surgery, so a child presenting in a rural or remote hospital is resuscitated, given analgesia and antibiotics if indicated, and retrieved while the receiving team is mobilised. After an uncomplicated appendicectomy the child is discharged within a day or two with clear safety-netting, while the perforated case stays for the antibiotic course and the return of feeding. [3] [4]
Special Populations
The preschool child deserves a separate threshold. Under five, appendicitis is uncommon but, when it occurs, is typically perforated at presentation because the history is short and atypical and the child cannot localise pain, so a tender, irritable toddler who refuses to walk or to be handled warrants a low threshold for ultrasound and surgical review. The same logic applies to the child with a disability or communication difficulty, in whom pain behaviour may be the only sign. [4] [1]
The adolescent girl widens the differential and the work-up. Ovarian torsion, a ruptured ovarian cyst, pelvic inflammatory disease and a tubal pregnancy all mimic appendicitis, so a pregnancy test is part of the assessment, and ultrasound of the pelvis is included alongside the appendix. The informed-adolescent population is also the group most often offered the non-operative option, where the shared-decision conversation about recurrence and the return to activity matters most. [3] [8]
Resource-limited and remote communities face the steepest gradient. An Indigenous or remote Australian and New Zealand child may be hours from imaging and surgery, and late presentation drives the higher perforation and complication rates seen in under-served cohorts, so early recognition, resuscitation, analgesia and prompt retrieval are what protect the bowel. Treating a tender, anorectic child as appendicitis until proven otherwise is here an equity issue as much as a clinical one. [4] [10]
Evidence, Guidelines & Regional Differences
The evidence base blends scoring, imaging and the non-operative trials. Samuel established the ten-point Pediatric Appendicitis Score and its validation by Bhatt showed its limits as a standalone rule-out, while the imaging meta-analysis established magnetic resonance imaging as the radiation-sparing second-line test that matches computed tomography. These two threads anchor the modern pathway of score, ultrasound, then magnetic resonance imaging for the equivocal case. [1] [6]
The non-operative story is the most examined piece of guideline-level evidence. The landmark adult trial showed antibiotics resolved about three-quarters of uncomplicated appendicitis at one year, the paediatric trials replicated this short-term success but identified the fecalith as a predictor of failure, and the long-term follow-up found that recurrence accumulates so that a substantial minority come to appendectomy within a few years. The shared-decision trial showed that helping families understand this trade-off leads to choices aligned with their values. [5] [9]
The antibiotic and surgical evidence has refined practice in the last few years. A network meta-analysis supports broad-spectrum enteric and anaerobic cover for the acute regimen, a large recent cohort showed that gangrenous but non-perforated disease does not benefit from prolonged postoperative antibiotics beyond prophylaxis, and a systematic review of the appendiceal mass and abscess found recurrence low enough to make routine interval appendicectomy selective. Regional practice is consistent in principle, with ultrasound first and laparoscopy standard in high-income settings, though the capacity to deliver prompt imaging and surgery varies and matters most where access is least. [11] [12]
Exam Pearls
Hold one sentence above all others: a child with periumbilical pain that migrates to the right iliac fossa, with anorexia, nausea and localised tenderness, has appendicitis until proven otherwise, confirmed by ultrasound and treated by laparoscopic appendicectomy. State the reflex that follows: score with the Pediatric Appendicitis Score, image with ultrasound first and magnetic resonance imaging second, resuscitate with fluids and analgesia that does not delay the diagnosis, and reserve non-operative antibiotics for the selected uncomplicated case by shared decision. [1] [6]
Get the frequently tested facts exactly right. The Pediatric Appendicitis Score awards one point for nausea, migration, anorexia, fever of 38 degrees or more, white cell count over ten and left shift, and two points each for right iliac fossa tenderness and for cough, percussion or hopping tenderness, for a total of ten. A score of 2 or below is low probability and 7 or above is high, but the score never rules appendicitis out alone. Ultrasound first and magnetic resonance imaging second spare radiation. [1] [2]
The high-yield pairings do the work in a viva. A migratory pain with anorexia needs an ultrasound and the Pediatric Appendicitis Score; peritonitis or shock converts the plan straight to surgery; testicular torsion must be examined for in every boy; non-operative antibiotics resolve about three-quarters at one year but recurrence accumulates to a substantial minority long-term; and analgesia does not delay diagnosis. Always resuscitate before you operate, and never reassure a bilious vomit. [3] [9]
References
- [1]Samuel M Pediatric appendicitis score. J Pediatr Surg, 2002.PMID 12037754
- [2]Bhatt M; Joseph L; Ducharme FM; et al Prospective validation of the pediatric appendicitis score in a Canadian pediatric emergency department. Acad Emerg Med, 2009.PMID 19549016
- [3]Bhangu A; Søreide K; Di Saverio S; et al Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet, 2015.PMID 26460662
- [4]Addiss DG; Shaffer N; Fowler BS; et al The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol, 1990.PMID 2239906
- [5]Salminen P; Paajanen H; Rautio T; et al Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis: The APPAC Randomized Clinical Trial. JAMA, 2015.PMID 26080338
- [6]Eng KA; Abadeh A; Ligocki C; et al Acute Appendicitis: A Meta-Analysis of the Diagnostic Accuracy of US, CT, and MRI as Second-Line Imaging Tests after an Initial US. Radiology, 2018.PMID 29916776
- [7]Minneci PC; Hade EM; Gil LA; et al Demographic and Clinical Characteristics Associated With the Failure of Nonoperative Management of Uncomplicated Appendicitis in Children: Secondary Analysis of a Nonrandomized Clinical Trial. JAMA Netw Open, 2022.PMID 35499827
- [8]Minneci PC; Cooper JN; Leonhart K; et al Effects of a Patient Activation Tool on Decision Making Between Surgery and Nonoperative Management for Pediatric Appendicitis: A Randomized Clinical Trial. JAMA Netw Open, 2019.PMID 31173118
- [9]Pátková B; Svenningsson A; Almström M; et al Long-Term Outcome of Nonoperative Treatment of Appendicitis. JAMA Surg, 2023.PMID 37556160
- [10]van Amstel P; Sluckin TC; van Amstel T; et al Management of appendiceal mass and abscess in children; early appendectomy or initial non-operative treatment? A systematic review and meta-analysis. Surg Endosc, 2020.PMID 32710216
- [11]Wang CH; Yang CC; Hsu WT; et al Optimal initial antibiotic regimen for the treatment of acute appendicitis: a systematic review and network meta-analysis with surgical intervention as the common comparator. J Antimicrob Chemother, 2021.PMID 33792691
- [12]Cramm SL; Graham DA; Blakely ML; et al Postoperative Antibiotics, Outcomes, and Resource Use in Children With Gangrenous Appendicitis. JAMA Surg, 2024.PMID 38324276