Paeds · gastroenterology-hepatology-and-nutrition
Ascites and peritoneal disease
Also known as Paediatric ascites · Spontaneous bacterial peritonitis in children · Serum-ascites albumin gradient · Chylous ascites in children · Tuberculous peritonitis in children
Fellowship guide to ascites and peritoneal disease in children: the serum-ascites albumin gradient as the key diagnostic tool separating portal hypertension from non-portal causes, the spontaneous bacterial peritonitis polymorphonuclear threshold of 250 per cubic millimetre, the stepwise ascites management with sodium restriction, diuretics, large-volume paracentesis with albumin replacement and transjugular shunting, and the paediatric peritoneal conditions of chylous ascites, tuberculous peritonitis and meconium peritonitis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who is brought in with a swollen, tense abdomen and recent breathlessness on lying flat may be revealing ascites, the pathological accumulation of fluid within the peritoneal cavity, and the cause is far from obvious until a sample of that fluid is analysed. The single most powerful question the clinician can ask is whether the ascites is driven by portal hypertension or by something else, because that question is answered by the serum-ascites albumin gradient and it redirects the entire diagnostic and management pathway. Ascites is rarely a diagnosis in its own right. It is a sign that the liver, the heart, the kidneys, the lymphatics, or the peritoneum itself is failing to keep fluid where it belongs. [4]
Cirrhosis is the dominant cause of ascites encountered in paediatric hepatology, and in children the leading underlying disease is biliary atresia, followed by the inherited metabolic liver diseases, autoimmune hepatitis, and cystic fibrosis liver disease. In all of these the scarred liver resists portal blood flow, sinusoidal pressure rises, and the neurohormonal cascade that retains sodium and water drives fluid across the sinusoids into the peritoneal space. Ascites in this context is a marker of decompensated cirrhosis and it carries a prognosis that is transformed only by liver transplantation. [1]
Peritoneal disease broadens the picture beyond the liver. The peritoneum can be the primary site of disease in tuberculous peritonitis, in peritoneal seeding of malignancy, and in neonatal meconium peritonitis from in-utero bowel perforation. The lymphatics can fail in chylous ascites, producing milky fluid that points to a congenital lymphatic malformation in an infant or to obstruction in an older child. What unifies all of these is that the peritoneal cavity is telling a story, and the story is read by tapping it. [5]
Classification
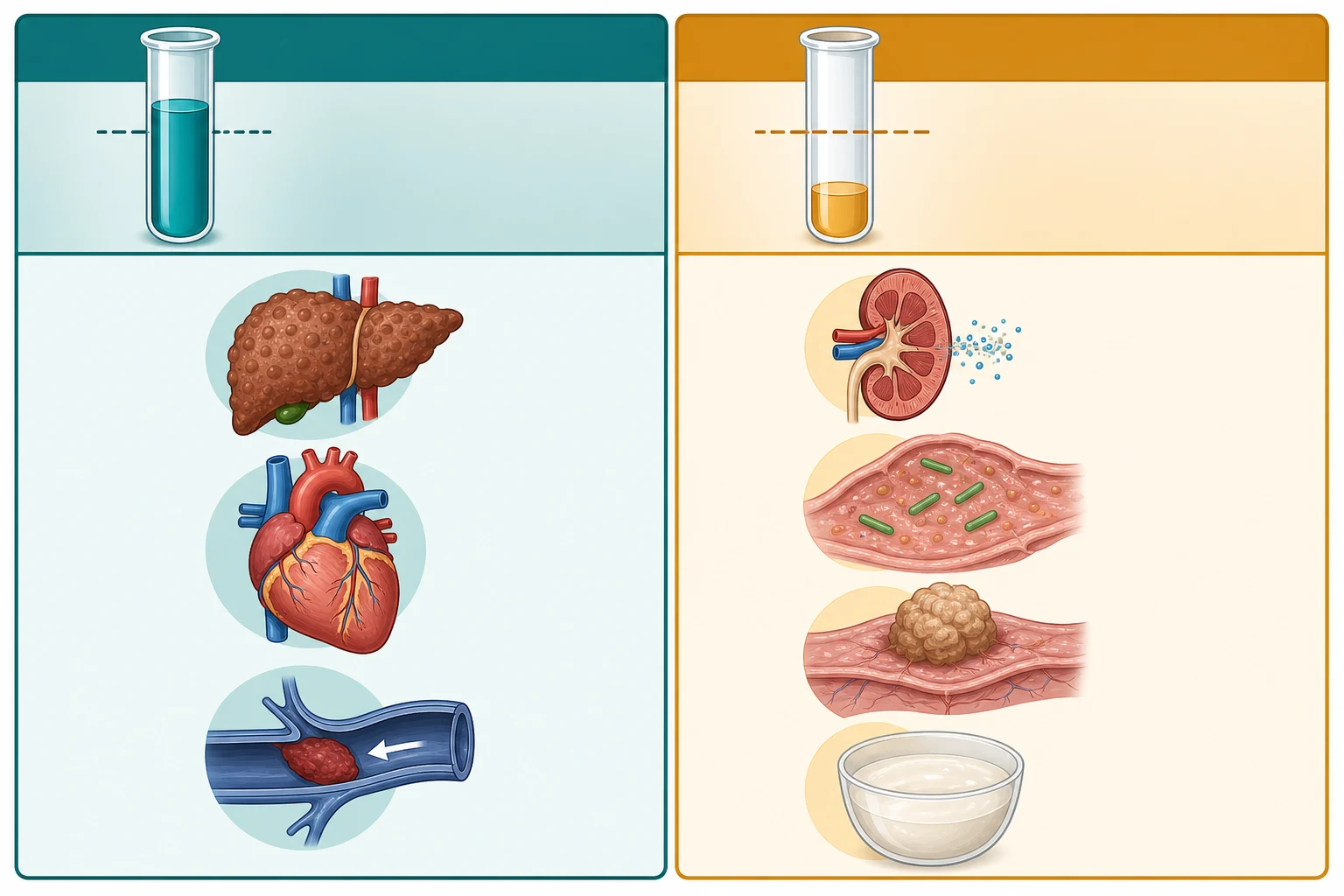
Ascites is classified by the serum-ascites albumin gradient, which is calculated by subtracting the albumin concentration of the ascitic fluid from the albumin concentration of a serum sample taken on the same day. A gradient of 11 g per litre or more, equivalent to 1.1 g per decilitre, indicates that portal hypertension is driving the ascites. A gradient under 11 g per litre indicates a non-portal cause. Runyon's landmark 1992 study demonstrated that this gradient correctly classified the cause in over 97 per cent of cases, displacing the older transudate-exudate concept that was based on total protein and performed far less well. [4]
[4]A second layer of classification refines the portal-hypertension group. The gradient tells the clinician that the portal system is under pressure, but it does not reveal where the obstruction sits. Cirrhosis is the intrahepatic cause. Right-sided heart failure and constrictive pericarditis are postcardiac causes in which the right heart backs up into the liver. Budd-Chiari syndrome, the obstruction of the hepatic veins, is a posthepatic cause that is rare in children but important because it produces ascites with preserved hepatocyte function and requires a different vascular approach. [10]
Among the non-portal causes, the fluid analysis carries the diagnosis. Nephrotic ascites has a very low albumin and often a high cholesterol-rich fluid. Tuberculous peritonitis yields a lymphocytic exudate with high protein and low glucose. Chylous ascites is strikingly milky-white with a triglyceride concentration far above that of serum. Peritoneal malignancy, rare in children, gives a fluid that may contain malignant cells. Each pattern changes the management decisively, which is why ascitic fluid analysis is never optional. [5]
Epidemiology & Risk Factors
In paediatric hepatology practice, ascites is overwhelmingly a feature of decompensated chronic liver disease. Biliary atresia is the single most common underlying diagnosis, and ascites in a child with a Kasai portoenterostomy signals that fibrosis has progressed to cirrhosis and portal hypertension. Beyond biliary atresia, the children at risk are those with alpha-1-antitrypsin deficiency, Wilson disease, tyrosinaemia, progressive familial intrahepatic cholestasis, autoimmune hepatitis, and cystic fibrosis liver disease. The Baveno VII consensus recognises that the development of ascites marks the transition from compensated to decompensated cirrhosis, a prognostic watershed. [2]
Outside the hepatology setting, the paediatric differential of ascites is dominated by nephrotic syndrome in the preschool child, by congestive cardiac failure at any age, and by the rarer peritoneal and lymphatic conditions. Tuberculous peritonitis is an important consideration in children from endemic regions or with household contact, and it can mimic cirrhotic ascites if the gradient is not measured. Chylous ascites in a neonate or young infant suggests a congenital lymphatic malformation, while the same finding in an older child raises the question of lymphatic obstruction from a retroperitoneal mass or trauma. [5]
Spontaneous bacterial peritonitis complicates approximately 10 to 30 per cent of hospitalised children with cirrhotic ascites, mirroring the adult experience. The risk is highest in the child with low ascitic protein, severe liver disease, and prior episodes of SBP. Bacterial translocation from the gut, facilitated by the cirrhotic gut's increased permeability and impaired reticuloendothelial clearance, allows enteric organisms to seed the sterile ascitic fluid. The AASLD guidance reinforces that the prevention, prompt diagnosis, and treatment of SBP are central to reducing mortality in cirrhosis. [6]
Pathophysiology
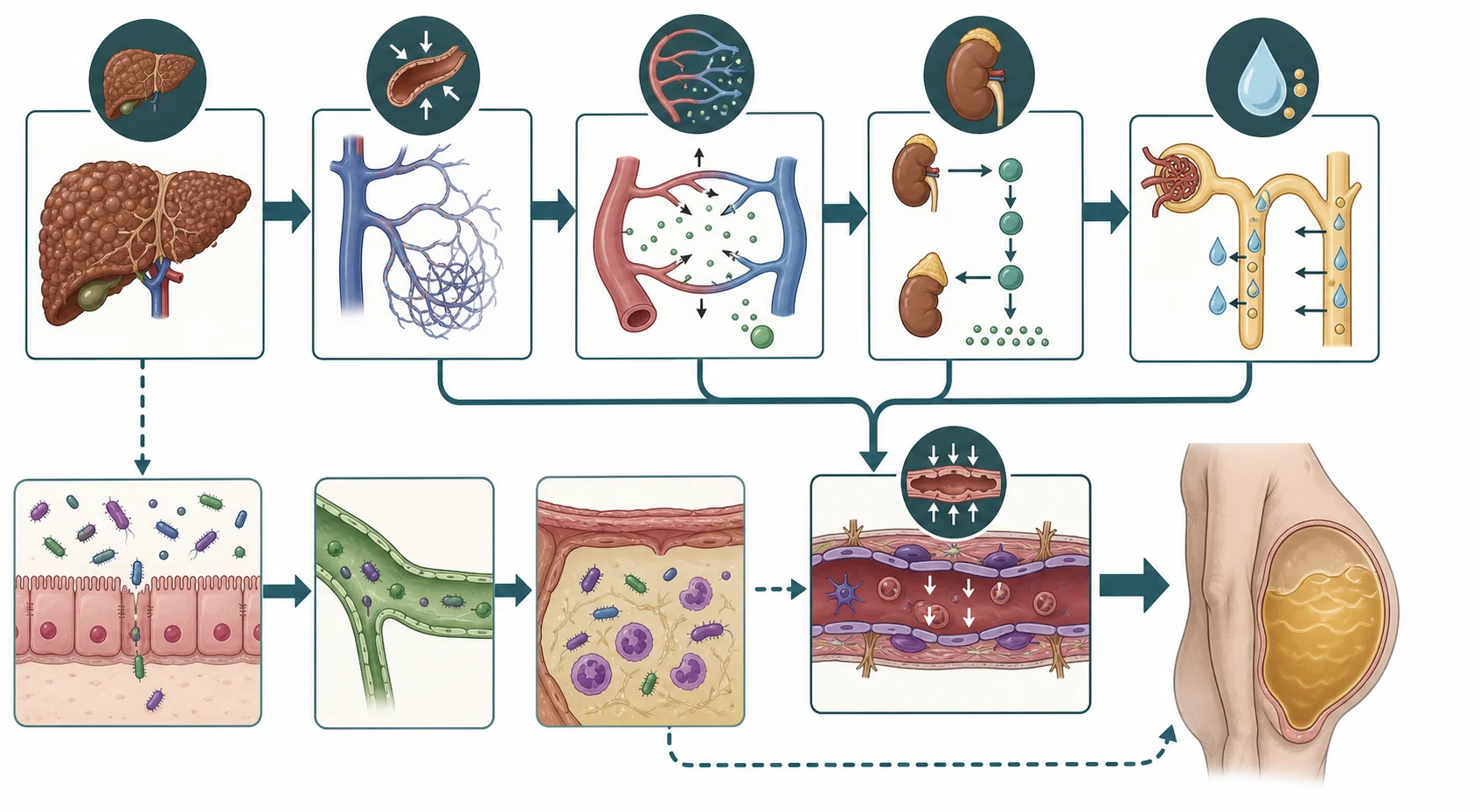
Cirrhotic ascites forms because two forces conspire to push fluid into the peritoneal space and keep it there. The first force is sinusoidal hypertension. As fibrosis and regenerative nodules distort the hepatic architecture, resistance to portal blood flow rises, and the pressure within the hepatic sinusoids climbs. When the sinusoidal pressure exceeds a critical threshold, fluid is driven across the sinusoidal membrane into the space of Disse and onward into the peritoneal cavity. Baveno VII emphasises that ascites appears only once portal hypertension is established, and clinically significant ascites correlates with advanced disease. [2]
The second force is sodium and water retention driven by the neurohormonal cascade. Splanchnic vasodilation, mediated by locally released nitric oxide and other vasodilators, expands the splanchnic vascular bed and reduces the effective circulating blood volume. The body perceives this as underfilling and activates the renin-angiotensin-aldosterone system, the sympathetic nervous system, and non-osmotic vasopressin release. Aldosterone promotes distal renal sodium reabsorption, vasopressin promotes free-water retention, and the result is total-body sodium and water overload that feeds the ascites and frequently produces dilutional hyponatraemia. [1]
These two forces operate together and explain why the management must address both. Diuretics attack the sodium retention, while paracentesis physically removes the accumulated fluid. The hyperdynamic splanchnic circulation also explains why non-selective beta-blockers, which reduce portal inflow, are part of the broader portal-hypertension strategy, though they are not first-line agents for ascites itself. The kidney is an innocent bystander that becomes progressively entrained, which is why the hepatorenal syndrome is the feared end-stage renal complication of cirrhotic ascites. [6]
Spontaneous bacterial peritonitis adds an infectious layer to this pathophysiology. The cirrhotic gut has increased permeability and impaired motility, and the reticuloendothelial system within the liver is blunted. Enteric bacteria translocate across the intestinal wall into mesenteric lymph nodes and the systemic circulation, and when they reach the protein-poor ascitic fluid, which itself has poor opsonic activity, they multiply. The clinical result is infection without an obvious intra-abdominal source, which is why it is called spontaneous. [5]
Clinical Presentation
The presentation of ascites in a child ranges from mild abdominal distension noticed by a parent to tense ascites causing respiratory distress and renal impairment. The earliest complaint is usually increasing abdominal girth, often described as a swollen belly or unexpected weight gain. As the fluid accumulates, the child may lose appetite, feel early satiety from gastric compression, and develop umbilical or inguinal herniation from raised intra-abdominal pressure. Scrotal or labial swelling is a common accompanying feature in infants and young children. [1]
The physical signs depend on the volume of fluid. A fluid thrill is elicited when an assistant places the edge of their hand on the midline of the abdomen and the examiner taps one flank, transmitting a shock wave to the opposite flank. Shifting dullness is the more sensitive sign and is demonstrated by percussing from the resonant midline laterally until the note becomes dull, then rolling the child and finding that the previously dull area becomes resonant as the fluid shifts. Visible distension with everted umbilicus and, in portal hypertension, a caput medusae of recanalised periumbilical veins complete the picture. [1]
Spontaneous bacterial peritonitis may present subtly in children, which is the central danger. The classic features are fever, abdominal pain, and altered mental status, but a cirrhotic child may simply become quieter, feed less, or show a worsening of hepatic encephalopathy. Any unexplained clinical deterioration in a child with known ascites must be assumed to be SBP until a diagnostic paracentesis proves otherwise. The threshold to tap is therefore very low. [5]
Chylous ascites has a distinctive presentation. The fluid is milky-white, and the child may have lymphoedema of the limbs if the lymphatic abnormality is widespread. In a neonate with congenital lymphatic dysplasia, the ascites may be present from birth and may be accompanied by pleural effusions. In tuberculous peritonitis, the course is more subacute, with fever, weight loss, night sweats, and a doughy abdomen on palpation, often in a child with a known contact or risk factors. [5]
Differential Diagnosis
The differential diagnosis of ascites in a child is best organised by the serum-ascites albumin gradient, because the gradient immediately narrows the field. A high gradient points to portal hypertension and demands an answer to where the obstruction sits, whether in the liver itself, in the hepatic veins, or in the right heart. A low gradient points away from the portal system toward the kidney, the peritoneum, or the lymphatics. This single calculation therefore replaces a long and unfocused list with two short and focused ones. [4]
[4]Among the portal-hypertension causes, the clinician must separate cirrhosis from cardiac ascites and Budd-Chiari syndrome. Cardiac ascites typically has a high ascitic fluid protein because the sinusoids are healthy and leak protein-rich lymph, and the examination reveals an elevated jugular venous pressure, a gallop rhythm, and hepatomegaly rather than a shrunken nodular liver. Budd-Chiari syndrome presents with painful hepatomegaly and ascites of abrupt onset, and Doppler ultrasound reveals absent or reversed hepatic venous flow. [10]
Among the non-portal causes, nephrotic syndrome is the most common in children and is suggested by generalised oedema, heavy proteinuria on urinalysis, and a low serum albumin. Tuberculous peritonitis is suggested by a lymphocyte-predominant exudate with high protein and low glucose, and by a positive interferon-gamma release assay or acid-fast bacilli in the centrifuged fluid. Chylous ascites is immediately suspected when the fluid is milky and is confirmed by a triglyceride concentration exceeding that of serum. Each of these requires a fundamentally different treatment from cirrhotic ascites. [5]
Clinical & Bedside Assessment
The focused examination of a child with ascites begins with an assessment of how unwell the child is and whether the ascites is causing physiological compromise. Tachypnoea, accessory-muscle use, and splinting suggest diaphragmatic compression from tense ascites. Tachycardia, cool peripheries, and oliguria suggest circulatory compromise. These findings move the assessment from elective workup to urgent therapeutic paracentesis. A complete set of vital signs, weight, and abdominal girth documented serially provides the baseline against which the response to treatment is measured. [1]
Abdominal examination seeks the signs of ascites and the stigmata of its cause. Shifting dullness is the most reliable bedside sign in a cooperative child. The clinician then searches for splenomegaly and a hard nodular liver edge pointing to cirrhosis, for an elevated jugular venous pressure and hepatomegaly pointing to cardiac failure, and for prominent abdominal wall veins suggesting portal hypertension. Tenderness or guarding in a cirrhotic child with ascites raises SBP as the leading concern and mandates paracentesis without delay. [1]
The general examination adds the peripheral clues. Spider naevi, palmar erythema, jaundice, and easy bruising suggest chronic liver disease. Digital clubbing and cyanosis raise hepatopulmonary syndrome. Lymphoedema of the limbs points to a lymphatic cause of chylous ascites. Growth parameters are essential, because failure to thrive in a cholestatic child worsens the PELD score and transplant priority. The examination is incomplete without a careful history of fever, abdominal pain, and change in mental state, because these are the triggers for SBP. [6]
Diagnostic paracentesis is performed at the bedside, typically in the left lower quadrant two centimetres medial and two centimetres superior to the anterior superior iliac spine, using a sterile technique and local anaesthetic. The fluid is sent for cell count and differential, albumin, total protein, culture in blood culture bottles, and, when indicated, triglyceride, cytology, and acid-fast staining. The procedure is safe in the child with cirrhosis even in the presence of a mild coagulopathy, and the risk of bleeding is very low when the correct site and technique are used. [5]
Investigations
The investigation of ascites serves to confirm the presence of fluid, to classify it by the gradient, and to detect its complications. Ultrasound confirms the fluid and assesses its volume, and it allows evaluation of the liver architecture, the portal vein patency and flow, the spleen size, and the presence of collaterals. Doppler is essential to exclude Budd-Chiari syndrome by confirming hepatic venous patency and flow direction, and to identify portal vein thrombosis. [1]
Ascitic fluid analysis is the cornerstone. The cell count is the single most important test, because a polymorphonuclear count of 250 per cubic millimetre or more makes the diagnosis of SBP regardless of the culture result or the clinical picture. Albumin is measured in both the fluid and the serum drawn the same day to calculate the gradient. Total protein helps refine the picture, with a low protein under 25 g per litre identifying the fluid at highest risk of SBP. Culture in blood culture bottles inoculated at the bedside increases the yield. [5]
Blood tests support the assessment of the underlying cause and the severity. A full blood count reveals the thrombocytopenia of hypersplenism and the leucocytosis of infection. Liver function tests with a low albumin and prolonged INR indicate impaired synthetic function. Urea, creatinine, and electrolytes screen for hepatorenal syndrome and hyponatraemia. Serum triglyceride confirms chylous ascites when the fluid is milky. A urinalysis for proteinuria excludes nephrotic syndrome, and an interferon-gamma release assay or ascitic adenosine deaminase supports tuberculous peritonitis. [1]
The PELD score, used for children under twelve, and the MELD score, used for those twelve and older, predict short-term mortality and guide transplant listing in cirrhotic ascites. Refractory ascites, SBP, and hepatorenal syndrome are each independent markers that escalate transplant priority. The AASLD guidance reinforces that the development of ascites complications should prompt formal transplant assessment, because medical therapy alone cannot reverse the underlying decompensation. [6]
Management — Resuscitation
Resuscitation begins with an assessment of the airway, breathing, and circulation. A child with tense ascites and respiratory compromise is positioned upright and given supplemental oxygen, and the fluid is drained by therapeutic paracentesis. If the child is in shock, intravenous access is established and crystalloid is given judiciously, because the cirrhotic child tolerates both overfilling and underfilling poorly. The principle is to relieve the mechanical compromise first and then to address the cause. [1]
When SBP is suspected, empirical antibiotic therapy is started immediately after the diagnostic tap and should not await the culture result. A third-generation cephalosporin such as cefotaxime or ceftriaxone at 50 to 100 mg per kg per day covers the typical enteric organisms and is continued for 5 to 7 days. Intravenous albumin is given at 1.5 g per kg on day 1 and 1 g per kg on day 3, because the landmark trial by Sort and colleagues showed that albumin reduces the incidence of hepatorenal syndrome and improves survival in SBP. [3]
Cefotaxime or ceftriaxone for spontaneous bacterial peritonitis
Dose
50 to 100 mg per kg per day in divided doses
The child with suspected hepatorenal syndrome, suggested by a rising creatinine and falling urine output in the setting of cirrhosis, requires careful fluid assessment and often albumin expansion followed by vasoconstrictor therapy under specialist guidance. This is a pre-terminal event in decompensated cirrhosis and is an indication for urgent transplant assessment. Early involvement of the paediatric hepatology, nephrology, and intensive care teams is essential. [6]
Management — Definitive & Stepwise
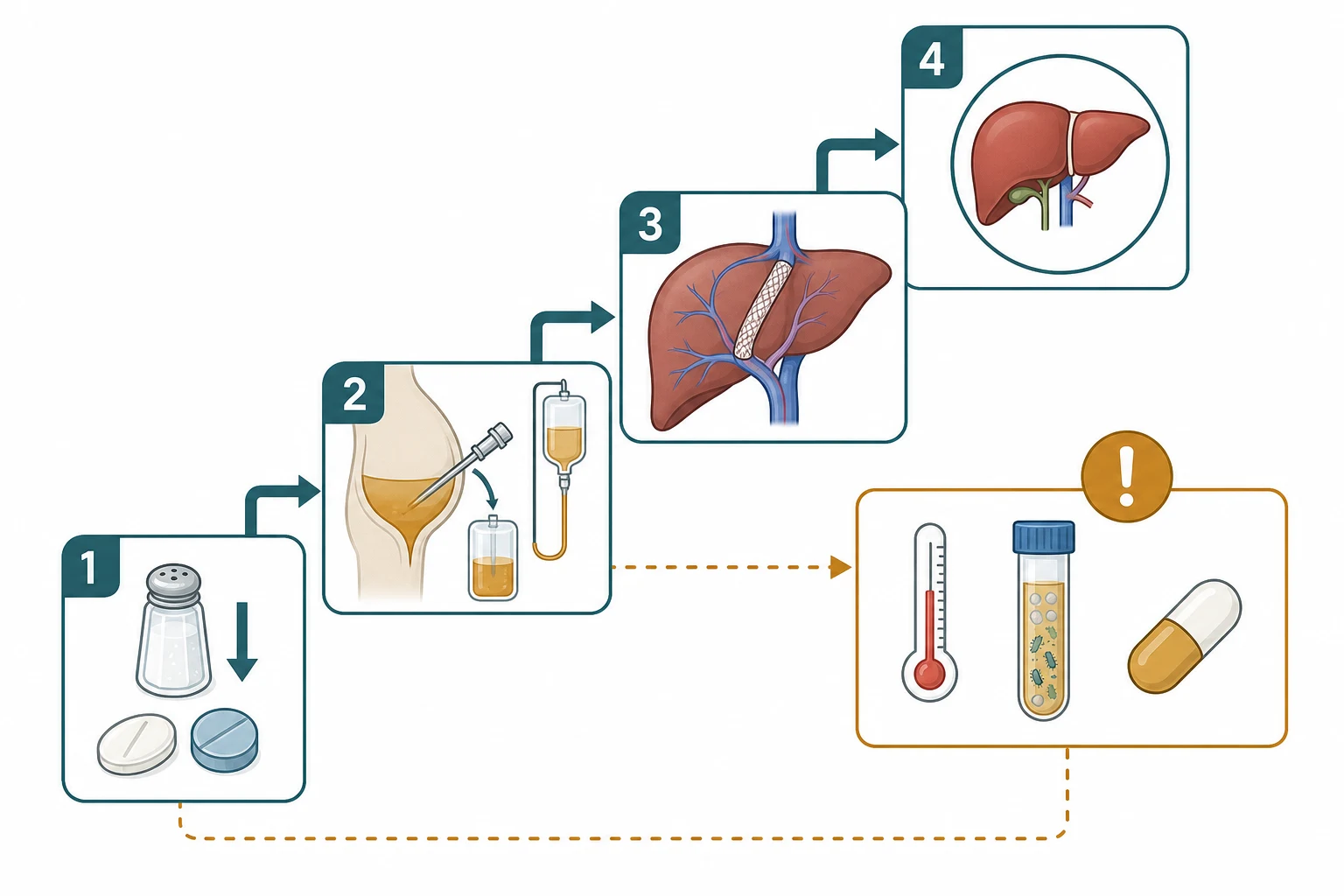
The definitive management of cirrhotic ascites proceeds in a stepwise fashion, with each step reserved for those who have failed the previous one. The foundation is dietary sodium restriction, typically to 1 to 2 mmol per kg per day in children, combined with advice against added salt and processed foods. Fluid restriction is reserved for the child with dilutional hyponatraemia, because most children with ascites retain sodium far more than they retain water. Sodium restriction alone controls ascites in only a minority, so it is paired with diuretic therapy. [1]
The first-line diuretic is spironolactone, which blocks the aldosterone-driven sodium retention at the distal tubule. The starting dose is 1 to 3 mg per kg per day, and furosemide at 0.5 to 1 mg per kg per day is added to maintain a balanced potassium and to increase the natriuretic response. The aim is a daily weight loss of no more than 0.5 kg, because faster diuresis risks intravascular depletion and precipitates hepatorenal syndrome. The spironolactone-to-furosemide ratio of roughly 5 to 2 by dose preserves normokalaemia. [1]
Spironolactone and furosemide for cirrhotic ascites
Dose
Spironolactone 1 to 3 mg per kg per day plus furosemide 0.5 to 1 mg per kg per day
For tense or refractory ascites, large-volume paracentesis is performed. The landmark randomised trial by Gines and colleagues established that when more than 5 litres is removed, albumin must be given at 6 to 8 g per litre of fluid drained to prevent paracentesis-induced circulatory dysfunction, a syndrome of effective hypovolaemia that precipitates hepatorenal syndrome and shortens survival. For smaller volumes, albumin is less critical but is often given in the cirrhotic child. Daily weight and renal function are monitored closely afterwards. [9]
Management of a cirrhotic child with new ascites
Measure weight, abdominal girth, bloods and ascitic fluid analysis
Confirm cirrhotic origin with serum-ascites albumin gradient of 11 g per litre or more
Start sodium restriction to 1 to 2 mmol per kg per day
Start spironolactone 1 to 3 mg per kg per day plus furosemide 0.5 to 1 mg per kg per day
Perform large-volume paracentesis for tense ascites with albumin 6 to 8 g per litre if over 5 litres
Consider TIPS for refractory ascites and assess for liver transplantation
Screen for and treat spontaneous bacterial peritonitis at every deterioration
Refractory ascites, defined by the failure of diuretics at maximum tolerated doses or the development of diuretic-induced complications, is managed with serial large-volume paracentesis or a transjugular intrahepatic portosystemic shunt. TIPS decompresses the portal system and reduces ascites formation, but it carries risks of hepatic encephalopathy and is used selectively in children. Refractory ascites is an ominous prognostic marker and is a firm indication for liver transplant assessment, because it signals that the liver can no longer maintain compensation. [6]
Secondary prophylaxis against SBP, after a first episode, is with an oral quinolone such as norfloxacin or with trimethoprim-sulfamethoxazole, continued indefinitely until transplantation. A meta-analysis of randomised trials confirmed that quinolone prophylaxis reduces the recurrence of SBP and may reduce mortality in high-risk cirrhotic patients. Primary prophylaxis is reserved for the child with low ascitic protein and advanced liver disease, because routine prophylaxis risks selecting resistant organisms. [8]
Specific Subtypes & Scenarios
Chylous ascites is a distinctive entity in which the fluid is milky-white and rich in triglyceride. In neonates and young infants, congenital lymphatic malformations and lymphangiectasia dominate, and the management is conservative, with a high-protein, low-fat diet supplemented with medium-chain triglycerides that are absorbed directly into the portal vein and bypass the lymphatics. Total parenteral nutrition and somatostatin analogues such as octreotide may reduce lymphatic flow in refractory cases. Spontaneous resolution is common in the congenital form. [5]
Tuberculous peritonitis is an important cause of low-gradient ascites in children from endemic regions or with household contact. The fluid is a lymphocyte-predominant exudate with high protein and low glucose, and the diagnosis is supported by a high ascitic adenosine deaminase and confirmed by acid-fast staining or culture of the centrifuged sediment. Treatment is standard antitubercular therapy, and the prognosis is good with early recognition. The pitfall is mistaking it for cirrhotic ascites if the gradient is not measured, because diuretics will not control a tuberculous effusion. [5]
Neonatal meconium peritonitis results from in-utero perforation of the bowel, with leakage of meconium into the peritoneal cavity producing a sterile chemical peritonitis that calcifies. It may be detected antenatally as fetal ascites or calcification, or postnatally as a distended, tender abdomen with bilious vomiting. Most cases require surgical exploration to repair the underlying atresia or perforation. It is a peritoneal disease of the newborn that is entirely separate from the cirrhotic ascites of older children. [5]
Budd-Chiari syndrome, the obstruction of hepatic venous outflow, presents with the triad of painful hepatomegaly, ascites, and abdominal pain. In children it is often associated with inherited thrombophilia, myeloproliferative disorders, or compression by a mass. The ascites is typically high in protein and may be bloody. Management combines anticoagulation, endovascular angioplasty or stenting of the obstruction, TIPS, and ultimately liver transplantation for those with fulminant or progressive disease. [10]
Complications & Pitfalls
The complications of cirrhotic ascites span the infectious, renal, and respiratory systems. Spontaneous bacterial peritonitis is the infectious complication and carries a one-year mortality of 50 to 70 per cent, which is why every episode mandates transplant assessment. Hepatorenal syndrome is the renal complication, a functional injury from intense renal vasoconstriction in the setting of splanchnic vasodilation, and it carries a grave prognosis without transplantation. Tense ascites causes respiratory compromise from diaphragmatic splinting and predisposes to pleural effusion, the so-called hepatic hydrothorax. [6]
Several pitfalls deserve emphasis. The first is failing to perform a diagnostic paracentesis in a cirrhotic child with ascites who deteriorates, because SBP can be clinically silent. The second is aggressive diuresis, because rapid fluid loss precipitates intravascular depletion and hepatorenal syndrome; the target weight loss is no more than 0.5 kg per day. The third is omitting albumin during large-volume paracentesis, because paracentesis-induced circulatory dysfunction is preventable and carries a mortality cost. The fourth is confusing cirrhotic ascites with cardiac or tuberculous ascites by failing to calculate the gradient and analyse the fluid. [9]
Diuretic complications are common and require vigilance. Spironolactone causes hyperkalaemia and, with chronic use, gynaecomastia in adolescents. Furosemide causes hypokalaemia, dehydration, and hyponatraemia. Both can precipitate hepatic encephalopathy through dehydration and electrolyte disturbance. The child on diuretics needs regular monitoring of weight, renal function, and electrolytes, and the doses must be titrated to the clinical response rather than escalated reflexively. [1]
Prognosis & Disposition
The prognosis of paediatric ascites depends almost entirely on the underlying cause and, for cirrhotic ascites, on the timeliness of liver transplantation. The development of ascites marks the transition from compensated to decompensated cirrhosis, and Baveno VII places it as a defining event in the natural history of chronic liver disease. Children with cirrhotic ascites have a substantially worse prognosis than those with compensated disease, and the appearance of refractory ascites, SBP, or hepatorenal syndrome each independently shortens survival. [2]
Non-portal causes carry a different prognosis. Chylous ascites in an infant often resolves with conservative management. Tuberculous peritonitis resolves with antitubercular therapy. Nephrotic ascites responds to steroid therapy for the underlying nephrotic syndrome. Cardiac ascites responds to optimisation of cardiac failure management. The prognosis is therefore cause-specific, which is why classifying the ascites by the gradient and the fluid analysis is prognostically as well as therapeutically essential. [5]
Disposition reflects the severity. The child with tense ascites, SBP, or hepatorenal syndrome is managed in hospital, often in a high-dependency or intensive care setting, with specialist paediatric hepatology involvement. The stable child with new cirrhotic ascites is managed as an inpatient for initial workup and stabilisation, then as an outpatient with serial weight and renal monitoring. All children with cirrhotic ascites are referred to a specialist paediatric hepatology service and assessed for transplantation, with structured transition to adult care in adolescence. [6]
Special Populations
Children with biliary atresia surviving with their native liver are the largest single group at risk for cirrhotic ascites in paediatric hepatology. These children require ongoing surveillance for decompensation, with serial assessment of synthetic function, and ascites is an early marker that the Kasai benefit is waning. Nutritional support is critical because ascites and cholestasis impair nutrition, and growth failure worsens the PELD score. Fat-soluble vitamin supplementation and a high-calorie, adequate-protein diet are essential despite the anorexia of tense ascites. [2]
Neonates and infants with chylous ascites form a distinct population. The congenital lymphatic malformations that drive neonatal chylous ascites often improve with conservative management, and surgery or interventional lymphatic embolisation is reserved for refractory cases. A medium-chain triglyceride diet is the mainstay, because these fats are absorbed directly into the portal venous system and reduce lymphatic flow. Parenteral nutrition and octreotide are second-line measures for persistent high-output lymph loss. [5]
Children from regions where tuberculosis is endemic, or with household contact, are at risk for tuberculous peritonitis. The presentation is subacute and the diagnosis is easily missed if the ascites is assumed to be cirrhotic. The key is to measure the gradient and to send the fluid for cell count, protein, glucose, adenosine deaminase, and acid-fast studies. Immigrant and refugee children with ascites should be evaluated for tuberculosis alongside liver and renal causes, particularly when the gradient is low. [5]
[2]Evidence, Guidelines & Regional Differences
The AASLD practice guideline on the management of ascites due to cirrhosis, published by Runyon in 2012 and 2013, remains the foundational document for the diagnostic and management approach. It established the serum-ascites albumin gradient as the primary classification tool, the polymorphonuclear threshold of 250 per cubic millimetre for SBP, the role of albumin in SBP and large-volume paracentesis, and the framework for refractory ascites. While adult-focused, its principles are applied to children by extrapolation. [1]
The Baveno VII consensus, published in 2022, provides the current international framework for portal hypertension and its complications, including ascites. It defines the transition from compensated to decompensated cirrhosis by the appearance of ascites, and it refines the approach to risk stratification and management. The AASLD practice guidance of 2024 adds the most recent North American recommendations on portal hypertension and varices, reinforcing the link between ascites management and the broader decompensation phenotype. [2]
[1]The evidence for albumin in chronic liver disease has consolidated in recent years. The Sort trial of 1999 demonstrated that intravenous albumin at 1.5 g per kg on day 1 and 1 g per kg on day 3 reduced renal impairment and mortality in SBP, a finding that has become a cornerstone of management. The Gines trial of 1988 established albumin replacement during large-volume paracentesis, and the review by Tufoni and colleagues in 2020 synthesised the indications for albumin across chronic liver disease. These trials underpin the albumin doses used in the management sections. [7]
The honest limitation of this evidence base is that it is overwhelmingly adult-derived. High-quality randomised trials in paediatric ascites and SBP are lacking, and paediatric practice relies on extrapolation from adult guidelines and on cohort data. This is the candid answer to a common exam question about the strength of the paediatric evidence: the principles are sound and widely applied, but the specific thresholds and doses in children are adapted from adult data rather than proven in paediatric trials. [6]
Exam Pearls
HIGH-LOW for the serum-ascites albumin gradient
250-SBP for spontaneous bacterial peritonitis
References
- [1]Runyon BA, AASLD Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline management of adult patients with ascites due to cirrhosis 2012. Hepatology, 2013.PMID 23463403
- [2]de Franchis R, Bosch J, Garcia-Tsao G, Reiberger T, et al Baveno VII - Renewing consensus in portal hypertension. J Hepatol, 2022.PMID 35120736
- [3]Sort P, Navasa M, Arroyo V, et al Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N Engl J Med, 1999.PMID 10432325
- [4]Runyon BA, Montano AA, Akriviadis EA, et al The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites. Ann Intern Med, 1992.PMID 1616215
- [5]Fernández J, Bauer TM, Navasa M, et al Diagnosis, treatment and prevention of spontaneous bacterial peritonitis. Baillieres Best Pract Res Clin Gastroenterol, 2000.PMID 11139350
- [6]Kaplan DE, Ripoll C, Thiele M, Fortune BE, et al AASLD Practice Guidance on risk stratification and management of portal hypertension and varices in cirrhosis. Hepatology, 2024.PMID 37870298
- [7]Tufoni M, Zaccherini G, Caraceni P, et al Albumin: Indications in chronic liver disease. United European Gastroenterol J, 2020.PMID 32213034
- [8]Malvi A, Verma N, Khatib MN, et al Impact of Quinolone Prophylaxis on Spontaneous Bacterial Peritonitis and Mortality in Cirrhosis Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. JGH Open, 2025.PMID 40247847
- [9]Ginès P, Titó L, Arroyo V, et al Randomized comparative study of therapeutic paracentesis with and without intravenous albumin in cirrhosis. Gastroenterology, 1988.PMID 3360270
- [10]Rudra OS, Poyekar S, Nagral A Pediatric Budd-Chiari Syndrome: A Systematic Review of Etiology, Diagnosis, and Management. J Clin Exp Hepatol, 2026.PMID 42232136