Paeds · gastroenterology-hepatology-and-nutrition
Bilious vomiting and intestinal obstruction
Also known as Bilious vomiting · Green vomiting in the newborn · Neonatal intestinal obstruction · Malrotation · Midgut volvulus · Ladd bands · Ladd procedure · Duodenal atresia · Jejunoileal atresia · Meconium ileus · Double bubble
Fellowship guide to bilious vomiting and intestinal obstruction in children, built around the one rule that green vomiting in a neonate is malrotation with midgut volvulus until proven otherwise. The page covers the high versus low obstruction split, the anatomy that makes a narrow mesenteric base twist, the resuscitation and urgent imaging that precede the Ladd procedure, and the differential from duodenal atresia and meconium ileus to Hirschsprung disease and intussusception.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a three-day-old baby who fed well, then suddenly vomits a mouthful of bright green fluid. That single colour changes everything. Bile is green because it enters the gut beyond the second part of the duodenum, so green vomit means the obstruction sits at or below that point, and in a neonate the diagnosis you must exclude first is malrotation with midgut volvulus. This is the surgical emergency that can strangle the entire small bowel within hours. [1] [2]
Intestinal obstruction is the mechanical or functional blockage of the flow of gut contents, and in children it announces itself through vomiting, abdominal distension, pain and failure to pass stool or wind. The level of the blockage shapes the picture: a high obstruction vomits early and bile-stained with little distension, while a low obstruction distends the abdomen and delays the passage of meconium before it vomits. Reading that pattern points you towards the cause and its urgency. [6] [7]
The task in the emergency is therefore not to make the final anatomical diagnosis but to act on the pattern. You resuscitate the child, decompress the stomach, and involve a surgeon and radiologist without delay, because the cost of treating a benign cause as an emergency is small while the cost of missing a volvulus is the loss of the entire midgut. Most bilious vomiting will turn out to be something less dangerous, yet every episode earns the same urgent respect. [1] [3]
Classification
Sort obstruction first by its level, because that governs both the clinical picture and how fast you must move. A high obstruction lies in the duodenum or proximal jejunum and vomits bile early with a scaphoid or only mildly full abdomen. A low obstruction lies in the distal ileum or colon and distends the abdomen with delayed passage of meconium before vomiting appears. The figure lays these two patterns side by side with their common causes. [6] [7]
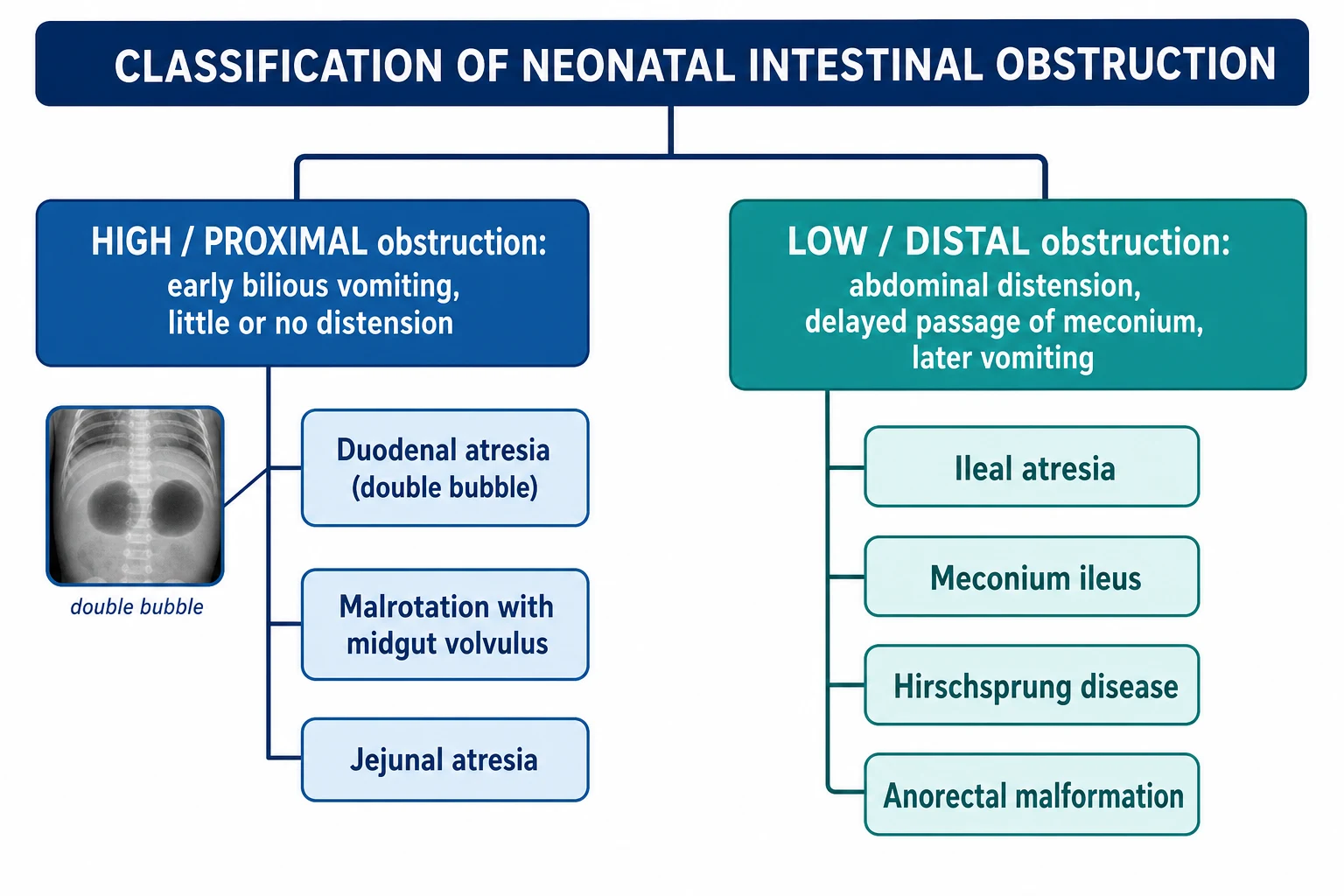
Among the high obstructions, duodenal atresia gives the classic double-bubble on the plain film and is often complete from birth, jejunal atresia lies a little further down, and malrotation with midgut volvulus is the one that can present in a previously well baby and threaten the whole midgut. The distinction that matters most at the bedside is that atresias are fixed and can be planned, whereas volvulus is a race against ischaemia. [6] [7]
Among the low obstructions, meconium ileus blocks the terminal ileum with thick meconium and points strongly to cystic fibrosis, Hirschsprung disease leaves an aganglionic segment that cannot relax, ileal atresia interrupts the bowel itself, and anorectal malformation is found on inspecting the perineum. A useful second axis is mechanism, separating mechanical blocks such as atresia and volvulus from functional ones such as Hirschsprung disease and, in the sick preterm, the ileus of necrotising enterocolitis. [7] [8]
High obstruction
- Duodenum or proximal jejunum
- Bilious vomiting early, little distension
- Duodenal atresia, jejunal atresia, malrotation with volvulus
- Volvulus is the time-critical emergency
Low obstruction
- Distal ileum or colon
- Abdominal distension, delayed meconium, later vomiting
- Ileal atresia, meconium ileus, Hirschsprung disease
- Contrast enema often both diagnostic and therapeutic
Functional obstruction
- No mechanical block but bowel does not propel
- Aganglionosis in Hirschsprung disease
- Ileus of necrotising enterocolitis or sepsis
- Needs decompression and treatment of the cause
Epidemiology & Risk Factors
Bilious vomiting is common and mostly benign, which is exactly what makes it dangerous. In series of newborns referred for bilious vomiting only a minority have a surgical cause, yet malrotation with volvulus hides within that minority, so the frequency of benign causes must never soften the response to any single episode. This is the tension the clinician manages every time. [1] [11]
Malrotation is the entity that dominates the exam and the emergency. It occurs in roughly one in five hundred people, most volvulus presents in the first month and the great majority within the first year, and the narrow mesenteric base that predisposes to twisting is present from birth. Malrotation also travels with other anomalies, being almost universal in exomphalos, gastroschisis and congenital diaphragmatic hernia and common in heterotaxy syndromes. [2] [3]
The other causes carry their own associations. Duodenal atresia is linked to trisomy 21 and to polyhydramnios seen on the antenatal scan, meconium ileus is a presentation of cystic fibrosis, and Hirschsprung disease is more common in boys and in trisomy 21. Prematurity and, in a well term baby, therapeutic hypothermia for hypoxic-ischaemic encephalopathy are recognised settings for benign bilious aspirates that mimic obstruction. Knowing these links sharpens the pre-test probability at the cot side. [7] [11]
Pathophysiology
To understand why malrotation is so dangerous, follow the embryology. The midgut normally herniates into the cord, rotates a total of two hundred and seventy degrees counter-clockwise around the superior mesenteric artery, and returns so that the duodenojejunal flexure is fixed high on the left and the caecum low on the right. This broad diagonal fixation gives the mesentery a wide, safe base. When rotation is incomplete the base stays short and narrow, and the whole midgut dangles from a stalk it can twist around. [2] [3]
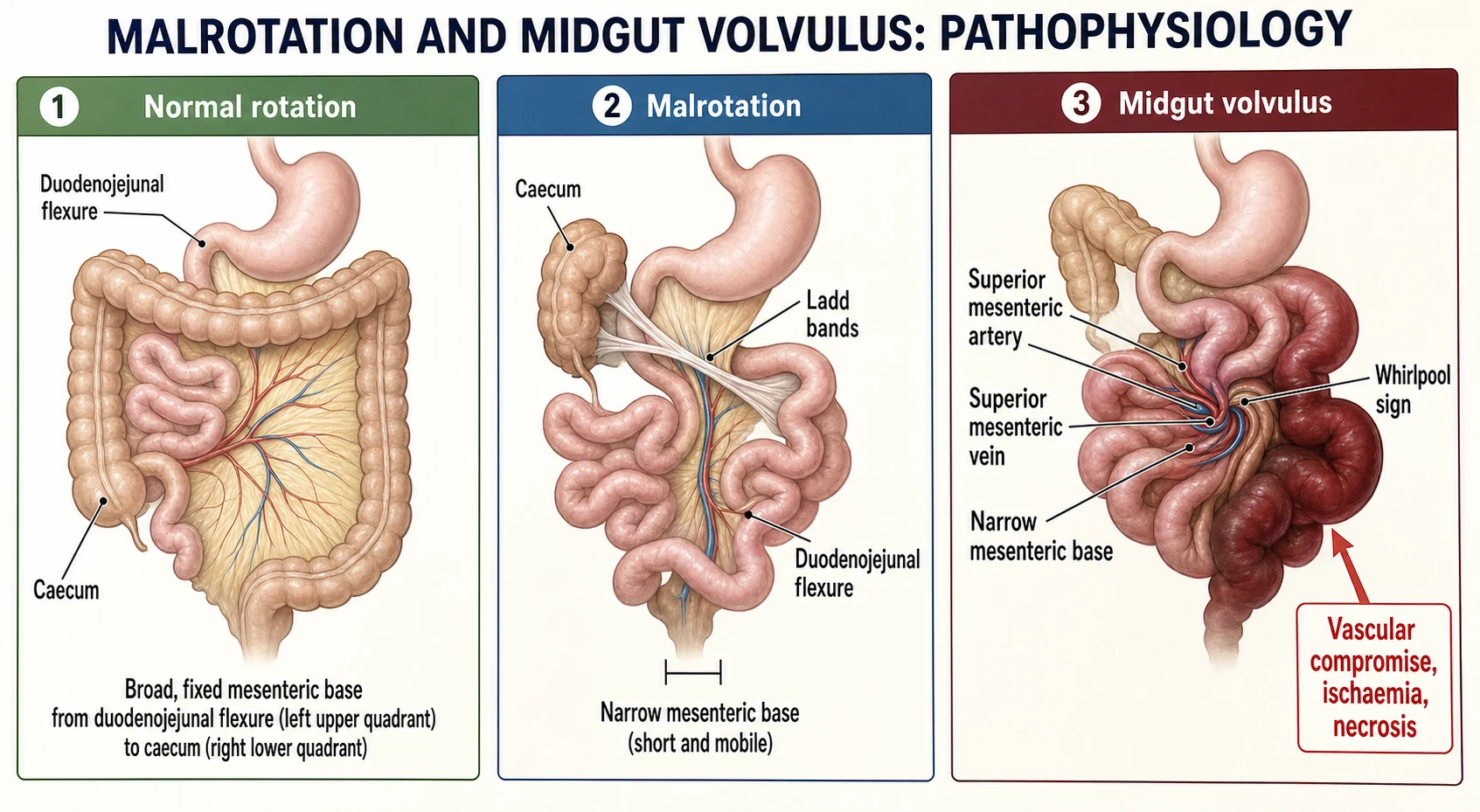
Two mechanisms then obstruct the gut. Peritoneal Ladd bands run from the malpositioned caecum across the duodenum and can compress it, producing obstruction without any twist. The far greater danger is the volvulus itself, where the midgut rotates clockwise around the narrow pedicle, kinking the bowel and, critically, occluding the superior mesenteric artery and vein within the twist. The result is bilious vomiting from the duodenal kink and, if the twist tightens, ischaemia of everything the artery supplies. [2] [12]
The timeline of ischaemia is what drives the urgency. At first the twist obstructs and the baby vomits bile while still looking well, then venous congestion makes the bowel boggy and passes blood per rectum, and finally arterial occlusion infarcts the midgut, bringing distension, peritonitis, shock and, if unrelieved, loss of the small bowel and short-gut syndrome. In fixed obstructions such as atresia the mechanism is simpler: proximal bowel dilates and vomits while the distal bowel is unused, but there is no vascular clock ticking. [2] [7]
Clinical Presentation
The neonatal presentation is deceptively gentle at the start. A baby who has fed and stooled normally suddenly vomits bile, and on first inspection may be alert with a soft, only slightly full abdomen, which is precisely why the vomit colour must be believed over the reassuring appearance. As the volvulus tightens the baby becomes irritable then lethargic, feeds poorly, develops abdominal distension and tenderness, and may pass blood in the stool as the bowel becomes ischaemic. [1] [2]
Beyond the newborn period the picture broadens. A low obstruction such as Hirschsprung disease, ileal atresia or meconium ileus presents with progressive abdominal distension, delayed or absent passage of meconium in the first day or two of life, and vomiting that becomes bilious as the block backs up. An older child or adolescent with an undiagnosed malrotation may have recurrent bilious vomiting, intermittent colicky central pain and faltering growth from repeated partial volvulus, a pattern that is easily mislabelled as functional. [5] [8]
Differential Diagnosis
The first fork in bilious vomiting is whether the cause is surgical or not, and the safest habit is to assume it is until proven otherwise. Non-surgical bilious vomiting does occur, for example the transient bilious aspirates of a term baby undergoing therapeutic hypothermia or the reflux of bile in an unwell preterm, but these are diagnoses of exclusion made only after a surgical cause has been actively ruled out with senior review and imaging. [1] [11]
Malrotation with volvulus
- Sudden bilious vomiting in a previously well neonate
- May look well early; blood in stool and shock are late
- Upper gastrointestinal contrast is the key test
- Emergency Ladd procedure if volvulus confirmed
Duodenal or jejunal atresia
- Vomiting from the first hours, often antenatal polyhydramnios
- Double bubble on plain film in duodenal atresia
- Trisomy 21 association in duodenal atresia
- Planned surgical repair, not a race
Low obstruction
- Distension and delayed meconium dominate
- Meconium ileus points to cystic fibrosis
- Hirschsprung disease has a contracted distal segment
- Contrast enema helps diagnose and can treat
Once a surgical cause is assumed, the level of obstruction narrows the list. High obstruction with early bilious vomiting suggests malrotation with volvulus, duodenal atresia or jejunal atresia, and the plain film often separates them by showing a double bubble or a few dilated loops. Low obstruction with distension and delayed meconium suggests ileal atresia, meconium ileus, Hirschsprung disease or an anorectal malformation, and here the perineal inspection and the contrast enema do much of the work. [6] [7]
In the older child the differential shifts towards intussusception, adhesional obstruction after previous surgery, an incarcerated hernia and intermittent volvulus on a missed malrotation. Intussusception classically brings colicky pain, a sausage-shaped mass and redcurrant-jelly stool, and is often reduced without an operation. The discipline throughout is to attribute the vomiting to a level and a mechanism confirmed by imaging rather than to settle on a comfortable non-surgical label too early. [5] [10]
Clinical & Bedside Assessment
The assessment runs in parallel with resuscitation, not after it. Look first at the vomit and confirm it is truly bile-stained green rather than milky or yellow, then assess the airway, breathing and circulation, because a child with obstruction may already be shocked from third-space and gastric losses. Examine the abdomen for distension, tenderness, guarding, visible peristalsis and any discolouration of the wall, and check every hernial orifice, since an incarcerated hernia is an easily missed mechanical cause. [1] [6]
The bedside then completes the picture that guides urgency. Inspect the perineum for an imperforate anus, feel for a mass suggesting intussusception, and perform a gentle rectal examination where Hirschsprung disease is suspected, watching for the explosive passage of stool and gas that follows. Weigh the baby, chart the passage or absence of meconium, and record the losses from the nasogastric tube, because these numbers drive the fluid replacement as much as they support the diagnosis. [6] [8]
Investigations
Investigation is deliberately fast and targeted, because in suspected volvulus the imaging must not delay the surgeon. The first film is the plain supine abdominal radiograph, which may show a double bubble of duodenal obstruction, a few dilated loops of high jejunal obstruction, many dilated loops of low obstruction, or a gasless abdomen in a tight volvulus. A normal film never excludes malrotation, so it reassures about nothing when the suspicion is volvulus. [6] [2]
The remaining tests confirm specific causes and prepare the child for theatre. A contrast enema shows the microcolon of ileal atresia or meconium ileus and the transition zone of Hirschsprung disease, and in meconium ileus a gastrografin enema can be therapeutic as well as diagnostic. Bloods for a gas, lactate, electrolytes, glucose and a group and save quantify the metabolic disturbance and the losses, a rising lactate warning of ischaemic bowel. A sweat test or genetics follows a diagnosis of meconium ileus, and a suction rectal biopsy is the definitive test for Hirschsprung disease. [7] [9]
A neonate with bilious vomiting — the mnemonic BILE
Management — Resuscitation
Resuscitation follows one governing rule: stabilise and decompress while you summon the surgeon, and never let a scan delay a child who is already peritonitic or shocked. Keep the child nil by mouth, secure intravenous access, and pass a wide-bore nasogastric tube on free drainage to decompress the stomach and reduce the risk of aspiration. These first minutes make the child safe for imaging or for theatre. [1] [6]
Correct the circulation with volume and the biochemistry alongside it. Give a fluid bolus of 10 to 20 mL/kg of isotonic saline and repeat it as needed for shock, then run maintenance fluids with added potassium once urine flows, replacing the nasogastric losses millilitre for millilitre with saline and potassium because they are rich in electrolytes. Start broad-spectrum intravenous antibiotics when ischaemia, perforation or sepsis is suspected, and monitor the gas, lactate and urine output to judge the response. [1] [6]
Management — Definitive & Stepwise
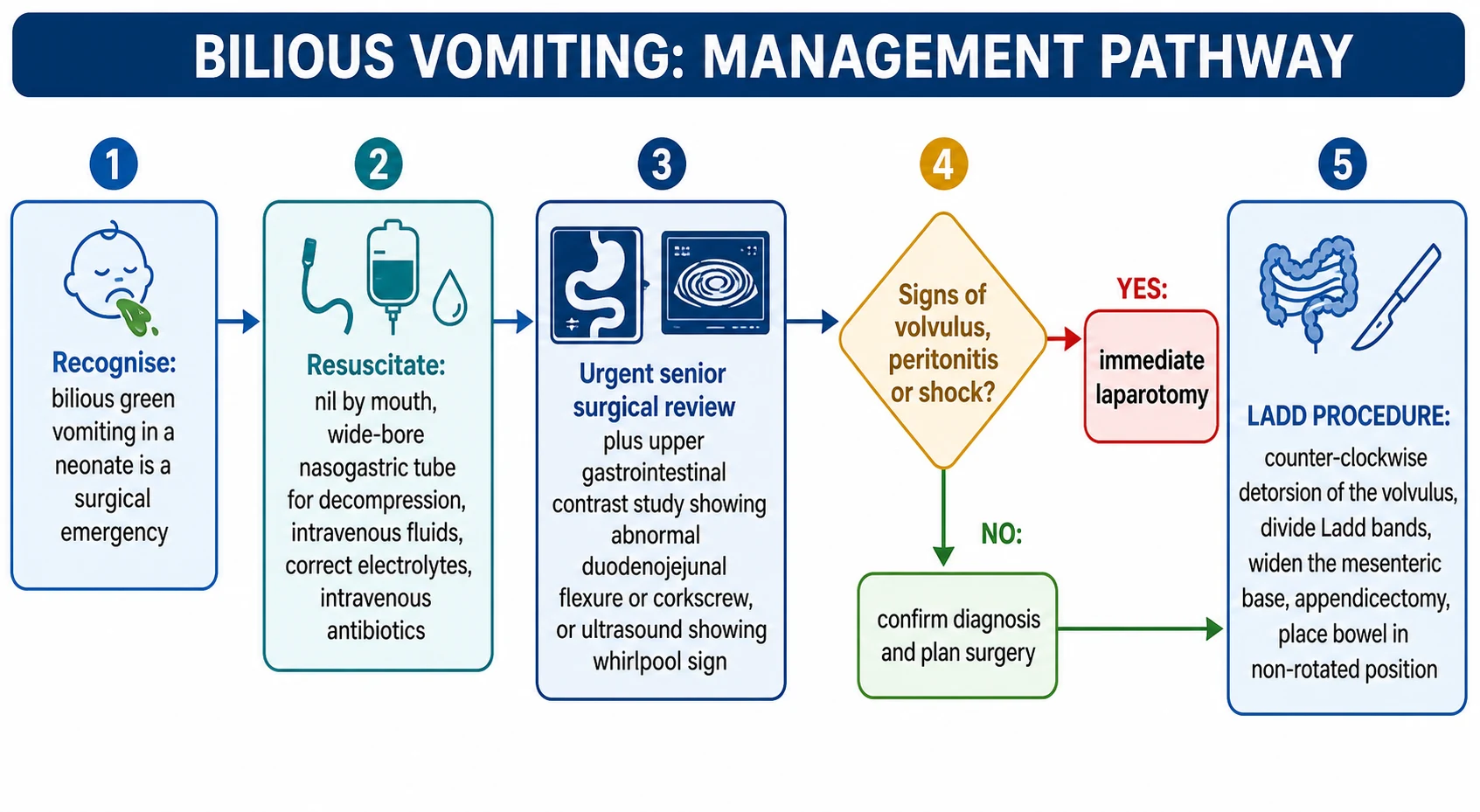
Definitive care depends on the cause, but the pathway from bilious vomiting to theatre is a single disciplined sequence. The figure sets out the whole route from recognition and resuscitation, through urgent imaging and the emergency decision, to the operation itself. The art is to run recognition and resuscitation together and to escalate to surgery the moment volvulus or peritonitis is suspected rather than after it is proven. [1] [12]
For malrotation with volvulus the operation is the Ladd procedure. The surgeon delivers the bowel, untwists the volvulus counter-clockwise to restore perfusion, divides the obstructing Ladd bands between the caecum and duodenum, widens the narrow mesenteric base to prevent re-twisting, and removes the appendix because the caecum will lie in an atypical position. The bowel is left in a non-rotated position with the small intestine on the right and the colon on the left. Frankly necrotic bowel is resected, and a second-look laparotomy may be planned when viability is borderline. [12] [2]
The fixed and functional causes each have their own definitive treatment. Duodenal atresia is repaired by a duodenoduodenostomy and jejunoileal atresia by resection and anastomosis, both planned rather than emergent once the baby is stable. Meconium ileus may resolve with a gastrografin enema but often needs surgery, and it commits the family to cystic fibrosis care. Hirschsprung disease is managed by decompression and washouts followed by a pull-through to remove the aganglionic segment. [7] [9]
Specific Subtypes & Scenarios
Malrotation with midgut volvulus is the scenario every candidate must own. The classic case is a term neonate in the first weeks who vomits bile, and the correct reflex is resuscitation, decompression, urgent surgical referral and an upper gastrointestinal contrast study, moving straight to laparotomy if the child is unstable. The prize for speed is a viable midgut and a Ladd procedure, and the penalty for delay is short-gut syndrome from a necrotic small bowel. [2] [12]
Asymptomatic and older malrotation raise their own questions. Malrotation is sometimes found incidentally on imaging done for another reason, and because the lifetime risk of volvulus is real the usual advice is an elective Ladd procedure, weighed against operative risk in each child. Older children and adolescents with recurrent bilious vomiting, intermittent central pain and poor growth can harbour an intermittent volvulus that is repeatedly missed, so a low threshold for an upper gastrointestinal contrast study is the key to diagnosis. [4] [5]
The distal obstructions complete the set. Meconium ileus obstructs the terminal ileum with tenacious meconium and is a strong pointer to cystic fibrosis, so its diagnosis triggers a sweat test and genetic testing alongside its enema or surgical treatment. Hirschsprung disease should be suspected in any term baby who fails to pass meconium in the first day, distends and vomits, and is confirmed by rectal biopsy, with enterocolitis its dangerous complication. [8] [9]
Complications & Pitfalls
The complications of obstruction follow the twin threats of ischaemia and delay. A volvulus that is not relieved in time infarcts the midgut and leaves the child with short-gut syndrome, lifelong dependence on parenteral nutrition and its liver and line complications, and in the worst case death. Perforation seeds peritonitis and sepsis, and the metabolic cost of vomiting and third-space loss is dehydration and electrolyte derangement that can cause collapse before the abdomen ever looks dramatic. [2] [7]
The pitfalls cluster around underestimating bilious vomiting. The classic error is to be reassured by a well-looking baby with a soft abdomen and to delay imaging or referral, allowing an early volvulus to progress to infarction. A second error is to accept a normal plain film as reassurance, when only the upper gastrointestinal contrast study or the operation can exclude malrotation. A third is to under-resuscitate, treating the diagnosis while ignoring the shock the losses have already caused. [1] [6]
Prognosis & Disposition
Outcome is dominated by how quickly a volvulus is relieved. When the diagnosis is made and the Ladd procedure performed before infarction, the great majority of children recover fully with an excellent long-term prognosis and a low, though real, risk of recurrent volvulus or later adhesional obstruction. When diagnosis is delayed and extensive midgut is lost, the child faces short-gut syndrome, prolonged parenteral nutrition and a far harder course, which is why time to theatre is the single most important prognostic lever. [3] [12]
The other causes generally do well with timely surgery. Duodenal and jejunoileal atresias have good outcomes after repair, tempered by any associated anomalies such as trisomy 21 or the length of bowel lost in complex atresia. Meconium ileus does well surgically but carries the lifelong trajectory of cystic fibrosis, and Hirschsprung disease has generally good functional results after a pull-through, with continence and enterocolitis the issues to follow. [7] [9]
Disposition reflects the acuity. A child with confirmed or suspected volvulus needs a paediatric surgical centre and often retrieval from a smaller hospital, with resuscitation and decompression continued throughout transfer. After surgery the child needs monitoring for anastomotic and feeding progress, nutritional support where bowel has been lost, and, for the specific diagnoses, enrolment in cystic fibrosis or Hirschsprung follow-up. Clear safety-netting is given to families whenever bilious vomiting is assessed and a benign cause is accepted. [1] [3]
Special Populations
The preterm and the sick neonate blur the picture in both directions. In a preterm baby, necrotising enterocolitis causes an ileus with bilious aspirates, distension and blood in the stool that can mimic mechanical obstruction, and it is managed medically unless it perforates. Conversely, a term baby cooled for hypoxic-ischaemic encephalopathy can have benign bilious aspirates from a slow gut, but this remains a diagnosis of exclusion reached only after a surgical cause has been considered and, where doubt remains, imaged. [11] [6]
Children with syndromes and complex anatomy carry a higher baseline risk. Malrotation is almost universal alongside anterior abdominal wall defects and congenital diaphragmatic hernia and common in heterotaxy, so these children warrant a low threshold for investigating bilious vomiting and often screening for rotational anomaly. Trisomy 21 raises the odds of both duodenal atresia and Hirschsprung disease, so a baby with trisomy 21 and obstruction deserves particular vigilance for these two diagnoses. [4] [7]
Geography shapes safety for many families. In Australia and New Zealand a neonate with bilious vomiting in a rural, remote or Indigenous community may be hours from a paediatric surgical centre, so early recognition, resuscitation, nasogastric decompression and prompt discussion with a retrieval service are what protect the midgut. Building the reflex to treat bilious vomiting as an emergency into every rural and general setting is therefore an equity issue as much as a clinical one. [1] [3]
Evidence, Guidelines & Regional Differences
The evidence base blends classic clinical series with modern imaging and surgical reviews. The observation that only a minority of newborns with bilious vomiting have a surgical cause, yet that the surgical causes are dangerous, comes from clinical series and underpins the safe default of treating every episode as an emergency. Historical and contemporary reviews of malrotation establish the upper gastrointestinal contrast study as the reference test and the Ladd procedure as the definitive operation. [1] [2]
Where evidence is softer, controversy remains. The management of incidentally discovered asymptomatic malrotation is debated, with a systematic review supporting an individualised approach that weighs the real risk of volvulus against operative risk rather than mandating surgery for all. The identification of malrotation in older children, whose intermittent symptoms are easily mislabelled, is an area where a higher index of suspicion and readier contrast imaging are advocated. [4] [5]
Regional practice is consistent in principle and variable in logistics. The rule that bilious vomiting in a neonate is a surgical emergency until proven otherwise is universal, but access to paediatric surgery, interventional radiology for enema reduction and rapid retrieval differs between and within countries. Cause-specific guidance, such as the ERNICA recommendations for Hirschsprung disease and cystic fibrosis pathways for meconium ileus, standardises the definitive care once the acute obstruction is addressed. [8] [9]
Exam Pearls
Hold one sentence above all others: bilious vomiting in a neonate is malrotation with midgut volvulus until proven otherwise. State the reflex that follows without hesitation, which is resuscitate, keep nil by mouth, pass a nasogastric tube, call the surgeon, and arrange an urgent upper gastrointestinal contrast study, going straight to laparotomy if the child is unstable or peritonitic. This is the answer that saves both marks and midguts. [1] [2]
Get the frequently tested facts exactly right. The diagnostic imaging sign of malrotation is an abnormally placed duodenojejunal flexure low and to the right, with a corkscrew appearance in volvulus, and the ultrasound clue is inversion of the superior mesenteric artery and vein with a whirlpool sign. A double bubble on plain film means duodenal obstruction and links to trisomy 21, while meconium ileus points to cystic fibrosis. [6] [7]
The high-yield pairings do the work in a viva. A previously well neonate with sudden bilious vomiting needs a Ladd procedure for midgut volvulus; a baby vomiting from birth with a double bubble has duodenal atresia; a term baby who does not pass meconium and then distends has Hirschsprung disease; and an infant with colicky pain, a sausage-shaped mass and redcurrant-jelly stool has an intussusception that is usually reduced by air enema. Always resuscitate and decompress before you image. [8] [10]
References
- [1]Godbole P; Stringer MD Bilious vomiting in the newborn: How often is it pathologic? J Pediatr Surg, 2002.PMID 12037761
- [2]Lampl B; Levin TL; Berdon WE; et al Malrotation and midgut volvulus: a historical review and current controversies in diagnosis and management. Pediatr Radiol, 2009.PMID 19241073
- [3]Salehi Karlslätt K; Husberg B; Ullberg U; et al Intestinal Malrotation in Children: Clinical Presentation and Outcomes. Eur J Pediatr Surg, 2024.PMID 36882104
- [4]Graziano K; Islam S; Dasgupta R; et al Asymptomatic malrotation: Diagnosis and surgical management: An American Pediatric Surgical Association outcomes and evidence based practice committee systematic review. J Pediatr Surg, 2015.PMID 26205079
- [5]Dekonenko C; Sujka JA; Weaver K; et al The identification and treatment of intestinal malrotation in older children. Pediatr Surg Int, 2019.PMID 30810798
- [6]Choi G; Je BK; Kim YJ Gastrointestinal Emergency in Neonates and Infants: A Pictorial Essay. Korean J Radiol, 2022.PMID 34983099
- [7]Rich BS; Bornstein E; Dolgin SE Intestinal Atresias. Pediatr Rev, 2022.PMID 35490204
- [8]Kyrklund K; Sloots CEJ; de Blaauw I; et al ERNICA guidelines for the management of rectosigmoid Hirschsprung's disease. Orphanet J Rare Dis, 2020.PMID 32586397
- [9]Sathe M; Houwen R Meconium ileus in Cystic Fibrosis. J Cyst Fibros, 2017.PMID 28986020
- [10]Sadigh G; Zou KH; Razavi SA; et al Meta-analysis of Air Versus Liquid Enema for Intussusception Reduction in Children. AJR Am J Roentgenol, 2015.PMID 26496576
- [11]Hukui J; Jones S; Coughlin K; et al Non-pathological bilious vomiting complicating therapeutic hypothermia for hypoxic ischaemic encephalopathy in neonates: a retrospective cohort study. BMJ Paediatr Open, 2017.PMID 29637099
- [12]Ingoe R; Lange P The Ladd's procedure for correction of intestinal malrotation with volvulus in children. AORN J, 2007.PMID 17292689