Paeds · gastroenterology-hepatology-and-nutrition
Breastfeeding medicine and lactation support
Also known as Breastfeeding · Lactation · Breastfeeding difficulties · Lactation support · Mastitis · Low milk supply · Breast engorgement · Human milk · Relactation · Donor breast milk
Fellowship guide to breastfeeding medicine and lactation support: the care of the breastfeeding mother-infant dyad from the physiology of prolactin-driven milk synthesis and the oxytocin let-down reflex to the WHO recommendation of exclusive breastfeeding for about six months and continued breastfeeding to two years and beyond. The page covers the infant and maternal benefits, the few true contraindications, the disciplined assessment of latch and milk transfer with WHO growth standards, and the layered management of the common problems of engorgement, the mastitis spectrum, nipple trauma and perceived low supply. It addresses the safe use of medications in the lactating mother, the support of the late-preterm and preterm infant with pasteurised donor human milk, relactation, the Baby-Friendly Hospital Initiative and the equity gap for Indigenous, migrant and disadvantaged families.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Breastfeeding medicine is the clinical care of the mother-infant dyad. As a paediatric clinician your job is to protect, promote and support breastfeeding, to recognise and treat the common problems, and to know the few situations in which breastfeeding is contraindicated or needs modification. The evidence base is unusually strong and consistent across the World Health Organization, the Australian National Health and Medical Research Council, the American Academy of Pediatrics and the Academy of Breastfeeding Medicine. [1] [3]
Overview & Definition
Breastfeeding is far more than nutrition. Human milk provides immunoglobulins, antimicrobial proteins, growth factors and stem cells that shape the infant gut and immune system, and it lowers the risk of infant infections, sudden infant death syndrome, necrotising enterocolitis, leukaemia, obesity and diabetes. The mother benefits too, with reduced breast and ovarian cancer, longer inter-pregnancy intervals and a lower risk of type 2 diabetes. [1] [4]
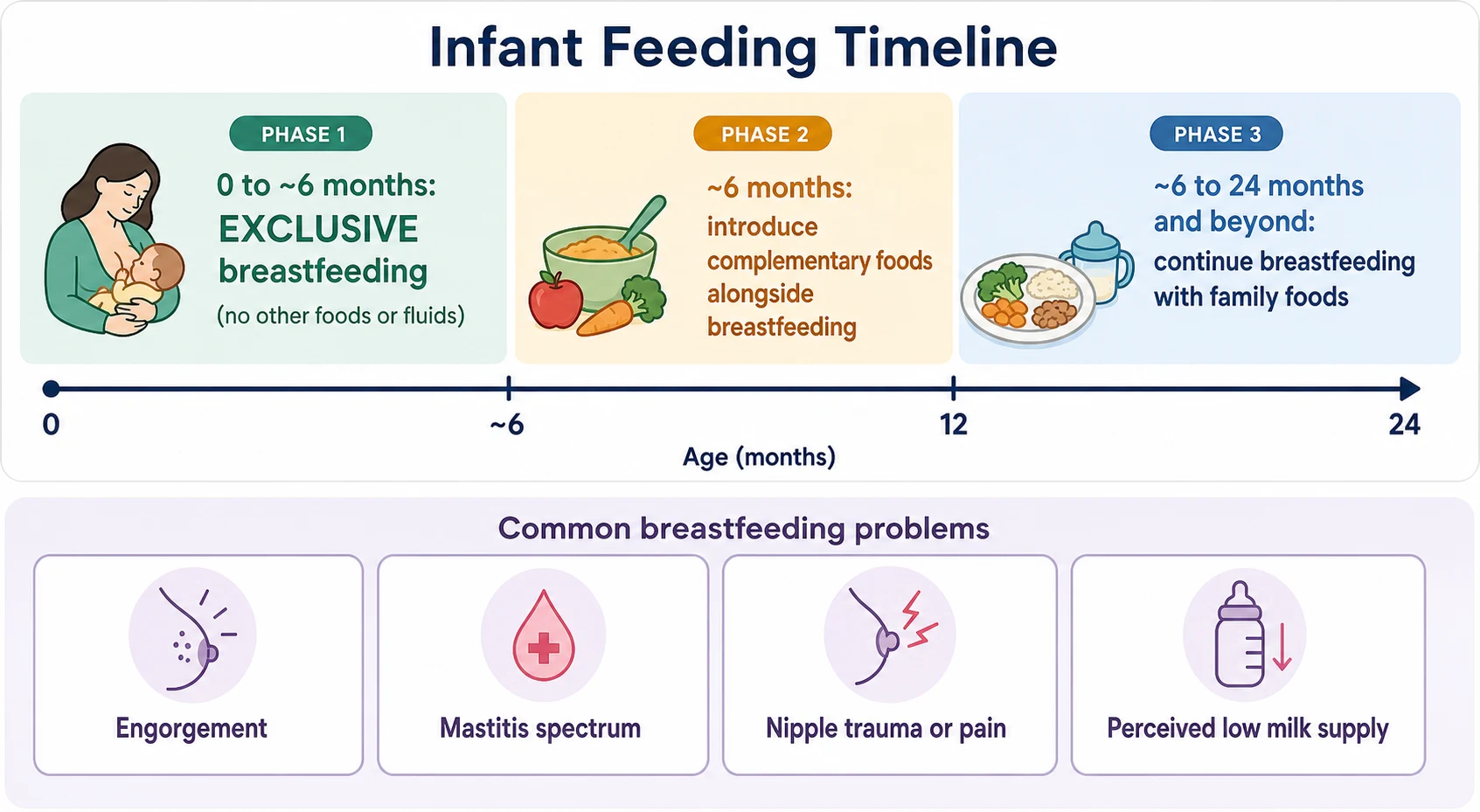
The global recommendation, affirmed by the 2016 Lancet Breastfeeding Series and adopted in Australia, is exclusive breastfeeding for about the first six months of life, introduction of nutritionally adequate and safe complementary foods from around six months, and continued breastfeeding to two years and beyond. [1] [2] The 2022 American Academy of Pediatrics policy supports continued breastfeeding to two years and beyond, depending on the mutual desires of mother and infant. [3]
The heart of the matter is the dyad. A problem on one side is usually a problem on both: a poor latch causes maternal nipple trauma and infant poor transfer, which causes low supply, which causes more supplementation, which lowers supply further. Your task is to find the break in the loop and close it early. [3]
Classification
Breastfeeding problems sort themselves into four practical groups, and naming the group drives the management. [3] [5] The first is milk-supply problems — engorgement in the early days, and perceived or true low supply. The second is the mastitis spectrum, a single continuous process running from inflammatory mastitis through bacterial mastitis to phlegmon, abscess and galactocele. The third is mechanical problems: poor latch and positioning, nipple trauma and ankyloglossia. The fourth is infant factors such as jaundice, reflux and late prematurity that interfere with feeding. [5] [12]
The numbers matter because they frame the gap between recommendation and reality. Most infants are ever breastfed, but exclusive breastfeeding to six months falls far short of the World Health Organization target of at least fifty percent, and the lost benefits are measurable in infections, deaths and maternal cancer. [1] [2]
Epidemiology & Risk Factors
Breastfeeding rates tell a story of support, not of biology. In Australia and similar high-income settings most infants start breastfeeding, but exclusive rates fall steeply in the first weeks and months as problems go unmanaged. [1] [6] The fall is steepest where support is weakest: among young, first-time, socially disadvantaged, Indigenous and migrant mothers, and those returning to work. [2]
The risk factors for early problems cluster around the birth and the early days. Caesarean and instrumental delivery, a complicated or painful labour, separation of mother and infant, and a late-preterm or preterm infant all raise the risk of delayed establishment. [12] [9] Poor latch and positioning, primiparity, smoking and limited skilled support then compound the difficulty. [2]
The equity dimension is inescapable. The structural interventions that work — paid maternity leave, the Baby-Friendly Hospital Initiative, skilled lactation support and workplace accommodation — are least available to the families who need them most, widening rather than narrowing the gap. [2] [6]
Pathophysiology
To understand any breastfeeding problem you first need the two hormones that run lactation. [1] [3] Prolactin, released from the anterior pituitary in response to suckling, binds receptors on the alveolar lactocytes and drives milk synthesis. Oxytocin, released from the posterior pituitary, contracts the myoepithelial cells around the alveoli and produces the let-down reflex that ejects milk toward the nipple.
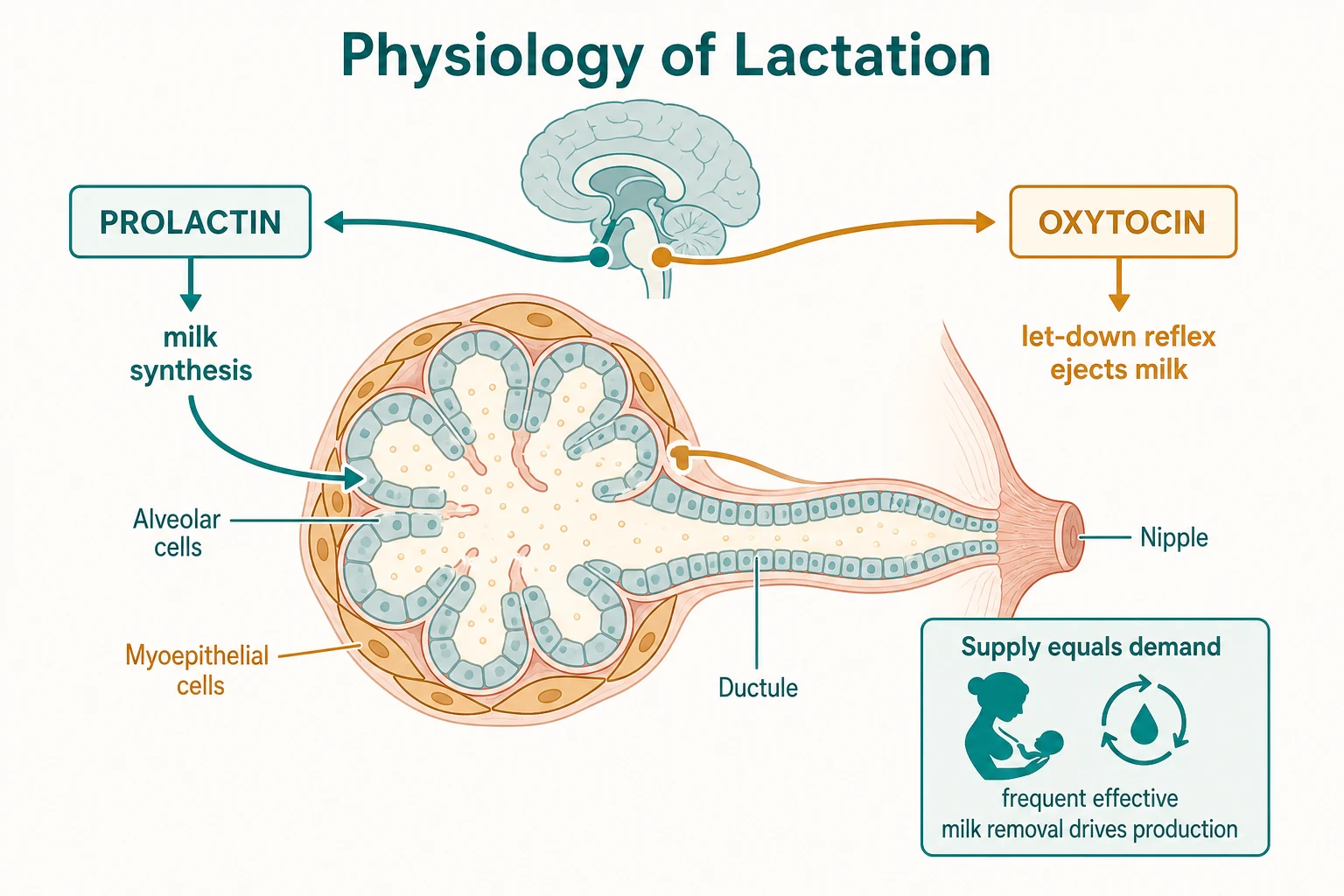
The clinical consequence is the single most useful idea in breastfeeding medicine: supply equals demand. [3] Frequent, effective milk removal is the dominant determinant of supply. Infrequent feeds, a poor latch that fails to transfer milk, engorgement that blocks removal, and unnecessary supplementation all reduce removal and so suppress production. Almost every problem you see can be traced to a break in this feedback loop, and almost every fix works by restoring effective removal.
Engorgement is the early-days result of vascular congestion and milk stasis as lactogenesis kicks in, and it softens with frequent feeding. [5] The mastitis spectrum begins when milk stasis and duct narrowing trigger inflammation; if stasis persists, bacterial overgrowth follows, and a collection may form. [5] Stress and pain inhibit the oxytocin-driven let-down, which is why a calm, supported mother and a good latch are therapeutic in themselves. [1]
Clinical Presentation
The well breastfed infant feeds eight to twelve times in twenty-four hours, swallows audibly, settles after feeds, has at least six heavy wet nappies and several soft stools a day by day five, and regains birth weight by two weeks with steady gain thereafter. [3] When these signs falter, feeding is failing and you need to find out why.
Engorgement presents in the first week as firm, swollen, tender and often bilateral breasts that feel heavy and warm. [5] Mastitis, by contrast, is usually unilateral: a hot, tender, wedge-shaped area of induration with overlying erythema, accompanied by fever, malaise and flu-like aches. [5]
The red flags within mastitis are the signs of abscess formation: a fluctuant or exquisitely tender mass, persistent fever, and failure to improve after forty-eight hours of appropriate antibiotics. [5] Ankyloglossia presents through the mother as nipple pain, trauma, a compressed or blanched nipple after feeds, and poor weight gain or clicking in the infant — though many ties are asymptomatic and need no treatment. [10]
Differential Diagnosis
The first fork is true low supply versus perceived low supply. A fussy, frequently-feeding but thriving infant with good output and weight gain has perceived low supply, not genuine insufficiency, and the fix is reassurance and feeding on cue. [3] True low supply shows as inadequate output, persistent weight loss, dehydration or hypernatraemia, and signals a real failure of transfer that needs investigation and supplementation. [12]
Inflammatory mastitis
- Local heat, induration, mild systemic upset
- No or low-grade fever
- Improves with milk removal and anti-inflammatories in 24-48 hours
- Antibiotics not yet indicated
Bacterial mastitis
- Fever, malaise, wedge of erythema and induration
- Usually unilateral
- No improvement or worsening on conservative care
- Needs antibiotics such as flucloxacillin or cephalexin
Breast abscess
- Fluctuant, exquisitely tender mass
- Persistent fever despite antibiotics
- Failure to improve at 48 hours
- Needs ultrasound and drainage
Nipple pain is most often mechanical, from a shallow latch, and is fixed by repositioning. [3] Burning, shooting, stabbing pain between feeds that persists despite a good latch raises candidiasis or vasospasm, while dermatitis presents with visible skin change. A posterior tongue-tie can cause both infant transfer problems and maternal pain. [10]
Poor weight gain in a breastfed infant should prompt you to look beyond feeding mechanics. Cardiac, metabolic and endocrine disease in the infant, and retained products, anaemia, hypothyroidism or inadequate nutrition in the mother, can all present as a failing-to-thrive baby. [3] [12]
Clinical & Bedside Assessment
Assessment rests on three things: a focused history, observation of a full feed, and serial weights on the WHO child growth standards. [3] Ask about feed frequency and duration, latch, swallowing, maternal pain, any supplementation, and the infant's output and weight trajectory. Then watch a feed from start to finish.
Good attachment is visible: the infant takes a deep mouthful of breast, the chin touches the breast, the lower lip is everted, and more areola shows above the top lip than below. [9] [3] Sucking is rhythmic, with pauses that correspond to audible swallows. A clicking sound, cheeks drawing in, or a nipple that is pinched or blanched on release all signal a poor latch.
GOODLATCH
Examine the mother for engorgement, mastitis, nipple trauma and candidiasis, and the infant for ankyloglossia, tone, oral anatomy and any sign of illness. [5] [10] Plot weight on the WHO standards; normal early gain is about 150 to 200 grams per week, and failure to regain birth weight by two weeks is a flag. [3]
Investigations
Most breastfeeding problems are clinical and need no investigations at all. [3] The diagnosis comes from the history and the observed feed, and the response to management is itself the test of whether you were right.
Where milk transfer is uncertain, a test weigh before and after a feed can estimate intake, though routine test weighing is unnecessary and anxiety-provoking. [3] Mastitis that fails to improve, or that presents with a mass, warrants ultrasound to exclude or guide drainage of an abscess; milk culture is reserved for recurrent, severe or atypical disease. [5]
In the late-preterm or preterm infant, pre-feed glucose monitoring and close growth surveillance guide the balance between feeding support and supplementation, because these infants are at real risk of hypoglycaemia and poor transfer. [12]
Management — Resuscitation
The breastfed infant who is dehydrated, hypoglycaemic, losing excessive weight or failing to thrive needs urgent assessment and treatment, not patience. Rehydrate or supplement with expressed breast milk or formula, check electrolytes and glucose, and search for the cause of the failure. [12] [3] Hypernatraemic dehydration from poor intake is the feared complication of missed low supply.
A suspected breast abscess is a surgical urgency. It needs antibiotics and prompt drainage — usually ultrasound-guided aspiration or incision and drainage — with continued expression or feeding from the affected side to maintain removal. [5] Severe bilateral nipple trauma with cracked, bleeding skin requires a pause from direct feeding on the damaged nipples: express to maintain supply, feed expressed milk, and resume once healed. [3]
Note that infant jaundice requiring phototherapy does not, by itself, demand stopping or supplementing breastfeeding. Continued breastfeeding with adequate hydration is supported, and interruption risks lowering supply. [3]
Management — Definitive & Stepwise
The foundation of all support is preventive and structural: early skin-to-skin contact, rooming-in, demand feeding, correct latch and positioning, and avoidance of unnecessary supplementation, delivered through the Baby-Friendly Hospital Initiative. [9] [6] Early skin-to-skin contact improves breastfeeding at one to four months and cardiorespiratory stability, and the Baby-Friendly Hospital Initiative measurably improves initiation and duration. [9] [6]
Moore 2016 — Early skin-to-skin contact (Cochrane)
PMID 27885658
Key finding
Skin-to-skin soon after birth increased breastfeeding at 1-4 months and improved cardiorespiratory stability and maternal attachment behaviour.
Practice change
Make early, uninterrupted skin-to-skin a default in the delivery room and the ward.
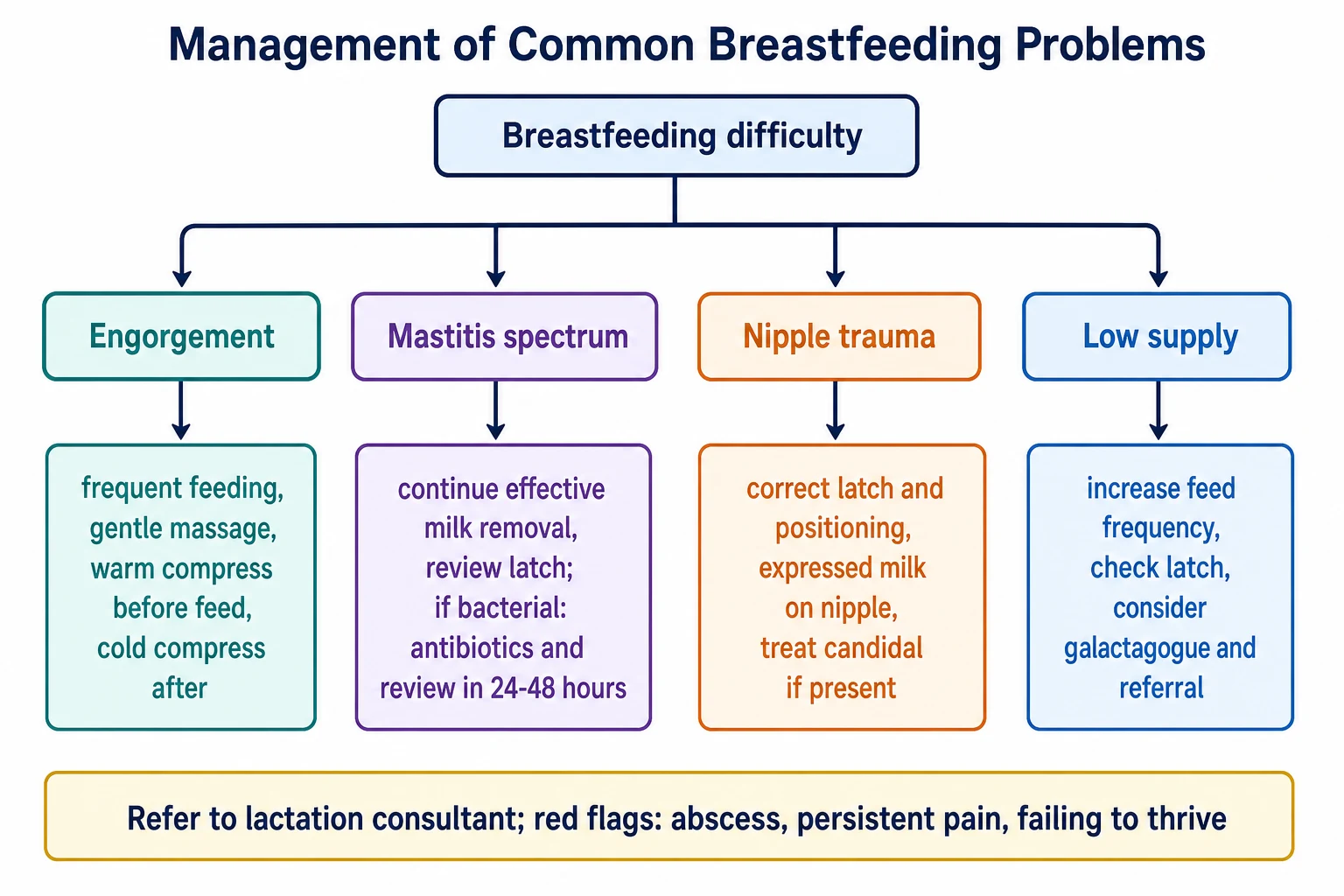
Engorgement is managed by frequent feeding, a good latch, gentle massage and reverse-pressure softening, a warm compress before and a cold compress after feeds, and anti-inflammatory measures; antibiotics play no part. [5]
The mastitis spectrum is managed first and always by continued effective milk removal and improved latch, with anti-inflammatory measures and a review at twenty-four to forty-eight hours. [5] The 2022 Academy of Breastfeeding Medicine protocol #36 reframes mastitis as a spectrum in which over-aggressive pumping and deep massage worsen inflammation, so the emphasis shifts to gentle, frequent feeding rather than forceful emptying. Antibiotics are added for bacterial mastitis.
Bacterial mastitis (ABM Protocol #36, 2022)
Low supply is a stepwise problem. Increase feed frequency and skin-to-skin contact, correct the latch and confirm transfer, address reversible causes, and only then consider a galactagogue such as domperidone where approved, alongside referral to a lactation consultant. [3] [8]
Stepwise management of perceived or true low supply
Confirm whether supply is truly low: check infant output, growth on WHO charts and transfer at a feed
Increase feed frequency (8-12 in 24 hours) and skin-to-skin contact; feed on cue, including overnight
Correct the latch and positioning; observe swallowing and a softened breast after feeds
Build supply by expressing after feeds to increase removal; minimise non-essential supplementation
Consider a galactagogue such as domperidone where approved, after reversible causes are addressed
Refer to a lactation consultant; review growth and feeding to confirm resolution
Specific Subtypes & Scenarios
The late-preterm infant — born at thirty-four plus zero to thirty-six plus six weeks — looks like a term baby but feeds like a preterm one. They are sleepy, tire easily, latch poorly, and are at high risk of hypoglycaemia, jaundice, suboptimal weight gain and re-feeding. [12] They need intensified lactation support, a feeding plan from birth to discharge, monitoring of glucose and bilirubin, and a low threshold to supplement with expressed milk.
For the preterm or low-birth-weight infant, the mother's own milk is the clear first choice. When it is unavailable, pasteurised donor human milk is preferred over formula, because it lowers the risk of necrotising enterocolitis, accepting somewhat slower early growth. [7]
The World Health Organization and the Australian National Health and Medical Research Council recommend exclusive breastfeeding for about six months and complementary foods from around six months, with continued breastfeeding to two years and beyond. The 2022 American Academy of Pediatrics policy likewise supports continued breastfeeding to two years and beyond. Regional practice differs on HIV: in settings with safe formula and clean water, replacement feeding is recommended to eliminate transmission; in many low- and middle-income settings, breastfeeding with effective maternal antiretroviral therapy is recommended. [1] [3]
Ankyloglossia causing breastfeeding difficulty is managed first by conservative lactation support. Frenotomy is reserved for significant maternal nipple pain or poor transfer, and the best evidence shows it reduces maternal nipple pain, though broader benefit is less certain. [10] Relactation — re-establishing milk supply after stopping or when it never built — is achievable for many mothers through frequent stimulation by hand expression, pumping and putting the infant to the breast, sometimes aided by a galactagogue. [3] [8]
Complications & Pitfalls
When breastfeeding problems are missed, the consequences are real. The infant can develop dehydration, hypernatraemia, failure to thrive and re-admission, and the mother can develop an abscess needing drainage. [12] [5] The most dangerous pitfall is the reassured dyad: a fussy but actually under-transferring infant sent home to return sicker.
Several pitfalls deserve naming because they recur. Over-diagnosing low supply and supplementing unnecessarily reduces milk removal and suppresses the very supply you are trying to protect. [3] Aggressive pumping or deep massage to empty the breast worsens the mastitis spectrum rather than curing it. [5] Empirical treatment of nipple candidiasis when the pain is mechanical, and frenotomy for an asymptomatic tongue-tie, are interventions without an indication. [10]
The pacifier question is a common trap. Restricted pacifier use does not clearly change breastfeeding duration, and pacifiers reduce the risk of sudden infant death syndrome once feeding is established. [11] The balanced position is to avoid routine pacifier introduction before feeding is established, but not to forbid it where a family wishes to use one for sleep.
Prognosis & Disposition
With early, skilled support, most breastfeeding problems resolve and feeding continues. Early skin-to-skin contact and the Baby-Friendly Hospital Initiative improve both initiation and duration, and the common problems respond well to the measures above. [9] [6]
Disposition turns on the infant's hydration and weight, and the mother's confidence and support. A well, thriving infant with a manageable problem is managed in the community with lactation support and follow-up. [3] The indications for referral or admission are dehydration or hypernatraemia, failure to thrive, a suspected abscess, persistent pain despite correct management, and unsafe or unsupported home circumstances. [12] [5]
Follow-up after any intervention — a latch correction, frenotomy, antibiotics or a relactation plan — confirms resolution through reassessed growth and feeding, because the proof that management worked is the weight chart and the settled, well-hydrated infant. [3]
Special Populations
The late-preterm and preterm infant needs the most support and the closest surveillance: intensified lactation support, glucose and bilirubin monitoring, pasteurised donor human milk when maternal milk is short, and fortification for growth once demand feeding is established. [12] [7]
The mother returning to work is at high risk of early cessation and needs planning: a place and time to express, storage of expressed milk, and a supportive workplace. [2] Return to work is among the most common reasons breastfeeding stops earlier than intended, and anticipatory guidance is part of routine care.
The contraindications to breastfeeding are few but firm, and they are examinable. Classic galactosaemia in the infant is an absolute contraindication, because the infant cannot metabolise galactose. [3] Maternal HIV is a regional decision: replacement feeding is recommended where safe formula and clean water are available, while breastfeeding with effective antiretroviral therapy is recommended in many low- and middle-income settings. Active untreated tuberculosis requires separation until the mother is non-infectious, though expressed milk may be given. Active herpes simplex lesions on the breast, human T-lymphotropic virus type 1, certain cytotoxic and radioactive drugs, and illicit substance use are also contraindications. [3]
Which maternal medication should usually be avoided in breastfeeding?
Codeine and tramadol are generally avoided in breastfeeding because a subset of mothers are CYP2D6 ultra-rapid metabolisers who convert the drug to high morphine concentrations, risking neonatal opioid toxicity. Most other medicines are compatible; assess using the relative infant dose and a current source such as LactMed, and consult rather than defaulting to stopping breastfeeding. [3]
Equity is the through-line for Indigenous, migrant, refugee and disadvantaged families, where culturally safe, peer-counsellor and community-based support, alongside the Baby-Friendly Hospital Initiative, measurably improve breastfeeding outcomes. [2] [6]
Evidence, Guidelines & Regional Differences
The guideline core is strikingly consistent across the World Health Organization, the National Health and Medical Research Council, the American Academy of Pediatrics and the Academy of Breastfeeding Medicine: exclusive breastfeeding for about six months, complementary foods from around six months, continued breastfeeding to two years and beyond, skin-to-skin contact, demand feeding and skilled support. [1] [3] [2]
The strongest evidence supports early skin-to-skin contact, the Baby-Friendly Hospital Initiative and donor human milk for preterm infants. Skin-to-skin improves breastfeeding and stability; the Baby-Friendly Hospital Initiative improves initiation and duration; and pasteurised donor human milk reduces necrotising enterocolitis compared with formula. [9] [6] [7]
Frenotomy for tongue-tie
- Reduces maternal nipple pain
- Broader benefit on supply or growth less certain
- Reserve for symptomatic tie
- Conservative support first
Domperidone as galactagogue
- Modest increase in milk volume
- Small QT-prolongation signal
- Not approved in all jurisdictions (e.g. US caution)
- Use after reversible causes addressed
Restricted pacifier use
- No clear change in breastfeeding duration
- Pacifiers reduce SIDS once feeding established
- Avoid routine introduction before feeding established
The controversies are honest ones. Frenotomy for tongue-tie is widely performed, but good evidence is limited to reducing nipple pain. [10] Domperidone as a galactagogue has a modest benefit on milk volume with a small QT-prolongation signal, and is not approved for this use in all jurisdictions. [8] Restricted pacifier use does not clearly change breastfeeding duration, yet pacifiers reduce sudden infant death syndrome risk. [11]
Exam Pearls
Exclusive breastfeeding means breast milk only — medicines, vitamins and minerals permitted — for about the first six months, then complementary foods with continued breastfeeding to two years and beyond. [1] [3]
Prolactin drives milk synthesis and oxytocin drives the let-down reflex; because supply equals demand, frequent effective milk removal governs supply. [1] [3] The mastitis spectrum is managed first by continued effective milk removal and anti-inflammatory measures, with antibiotics (flucloxacillin or dicloxacillin 500 mg four times daily for ten to fourteen days) reserved for bacterial mastitis. [5]
Classic galactosaemia in the infant is an absolute contraindication to breastfeeding; maternal HIV is a regional decision; and pasteurised donor human milk is preferred over formula for preterm and low-birth-weight infants. [3] [7] Name the Baby-Friendly Hospital Initiative and early skin-to-skin contact as the evidence-based structural supports, and remember that the proof of any intervention is the infant's growth on the WHO standards. [6] [9]
References
- [1]Victora CG; Bahl R; Barros AJ; et al Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet, 2016.PMID 26869575
- [2]Rollins NC; Bhandari N; Hajeebhoy N; et al Why invest, and what it will take to improve breastfeeding practices? Lancet, 2016.PMID 26869576
- [3]Meek JY; Noble L; Section on Breastfeeding Policy Statement: Breastfeeding and the Use of Human Milk. Pediatrics, 2022.PMID 35921640
- [4]Ip S; Chung M; Raman G; et al Breastfeeding and maternal and infant health outcomes in developed countries. Evid Rep Technol Assess (Full Rep), 2007.PMID 17764214
- [5]Mitchell KB; Johnson HM; Rodriguez JM; et al Academy of Breastfeeding Medicine Clinical Protocol #36: The Mastitis Spectrum, Revised 2022. Breastfeed Med, 2022.PMID 35576513
- [6]Perez-Escamilla R; Martinez JL; Segura-Perez S Impact of the Baby-friendly Hospital Initiative on breastfeeding and child health outcomes: a systematic review. Matern Child Nutr, 2016.PMID 26924775
- [7]Quigley M; Embleton ND; McGuire W Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst Rev, 2019.PMID 31322731
- [8]Paul C; Zenut M; Dorut A; et al Use of domperidone as a galactagogue drug: a systematic review of the benefit-risk ratio. J Hum Lact, 2015.PMID 25475074
- [9]Moore ER; Bergman N; Anderson GC; et al Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev, 2016.PMID 27885658
- [10]O'Shea JE; Foster JP; O'Donnell CP; et al Frenotomy for tongue-tie in newborn infants. Cochrane Database Syst Rev, 2017.PMID 28284020
- [11]Jaafar SH; Ho JJ; Jahanfar S; et al Effect of restricted pacifier use in breastfeeding term infants for increasing duration of breastfeeding. Cochrane Database Syst Rev, 2016.PMID 27572944
- [12]Busch DW; Silbert-Flagg J Breastfeeding Plan of Care for the Late Preterm Infant From Birth Through Discharge. J Perinat Neonatal Nurs, 2021.PMID 33900247