Paeds · gastroenterology-hepatology-and-nutrition
Constipation and faecal incontinence
Also known as Functional constipation · Childhood constipation · Faecal soiling · Encopresis · Overflow incontinence · Non-retentive faecal incontinence · Chronic idiopathic constipation
Fellowship guide to childhood constipation and faecal incontinence: the Rome IV diagnosis of functional constipation, the withholding vicious cycle that drives megarectum and overflow soiling, the red flags that flag Hirschsprung disease and other organic causes, and the disimpaction-then-maintenance polyethylene glycol regimen with behavioural support that underpins evidence-based management.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A toddler who screams and clenches on the potty, a preschooler who stains their underwear several times a day, and a school-aged child who has not opened their bowels for a week and now has a palpable abdominal mass are all showing the same condition from different angles. Constipation in childhood is common, distressing, and in the great majority of children has no underlying disease. Most of these children have functional constipation, a positive Rome IV diagnosis rather than a label of exclusion. [1]
Constipation means infrequent or painful passage of hard stool, and the child may also have large-diameter stools, withholding behaviour, and a palpable rectal or abdominal faecal mass. Faecal incontinence is the involuntary passage of stool in a child old enough to be toilet trained, usually beyond four years of age. In most children the two problems are linked, because retained stool overflows around a rectal impaction, but a minority soil without any constipation at all. [2]
The core clinical skill is to make a confident functional diagnosis, treat early and adequately, and stay alert for the small number of children whose constipation signals organic disease such as Hirschsprung disease. Early, effective treatment matters because an established withholding cycle with a stretched rectum is far harder to reverse than a new problem. Families need to understand from the outset that treatment is measured in months, not days. [1]
Classification
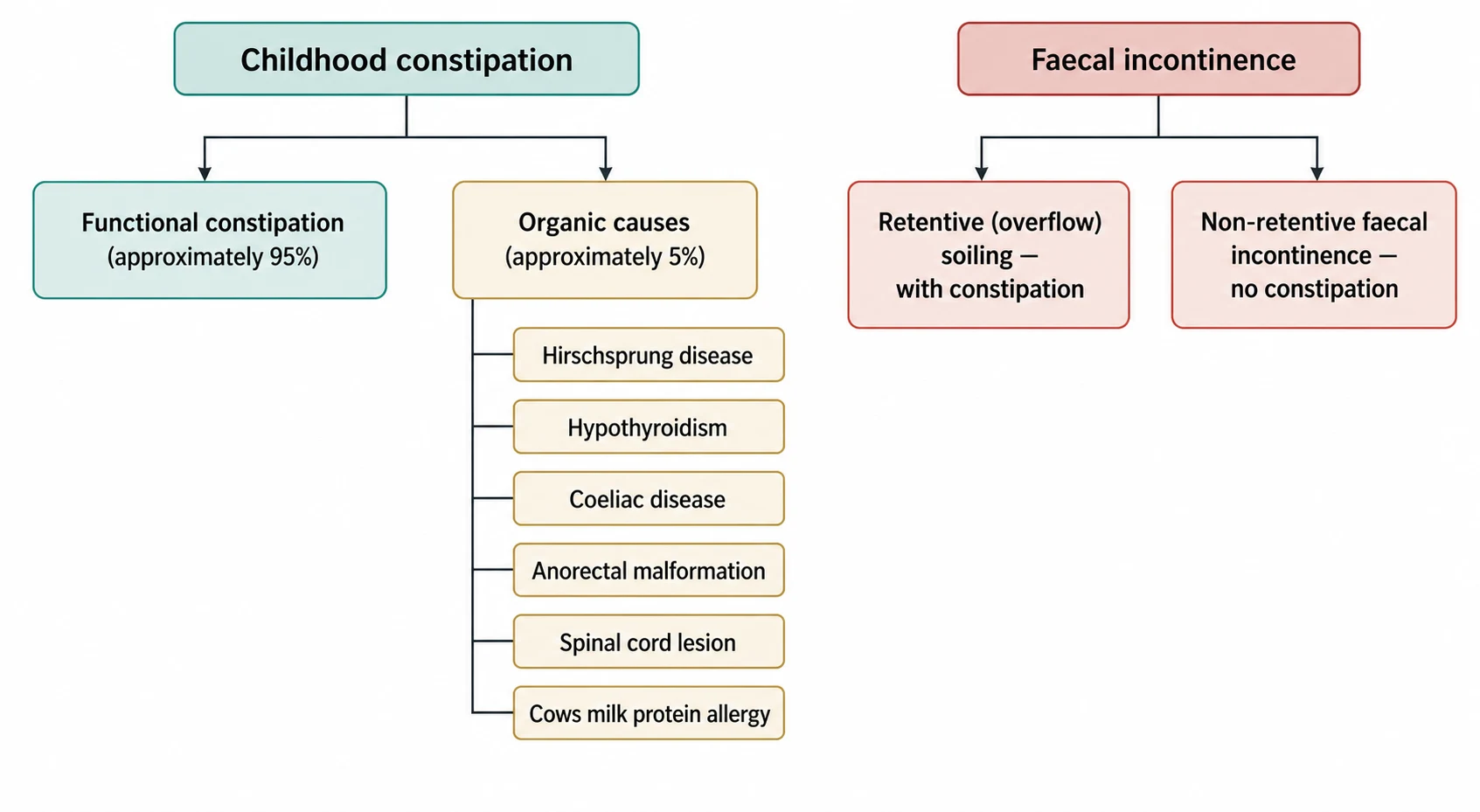
The most useful first division is between functional and organic constipation, because it decides whether the child needs treatment or a hunt for disease. Around ninety-five per cent of children have functional constipation, with a normal examination, no red flags, and a typical withholding story. Organic causes account for the remaining small minority and announce themselves through red flags such as delayed meconium, ribbon stools, or abnormal neurology. [1]
[1]Faecal incontinence divides along a second axis that changes management entirely. Retentive incontinence, the far more common type, is overflow soiling around a rectal impaction and resolves when the constipation is treated. Non-retentive faecal incontinence is soiling in a child with no constipation and an empty rectum, and it is closely linked to behavioural and emotional factors rather than to retained stool. [11]
Epidemiology & Risk Factors
Constipation is one of the most common problems in paediatric practice and accounts for a large share of general paediatric and gastroenterology referrals. A systematic review estimated the worldwide prevalence of childhood constipation at around three per cent, with wide variation between studies and populations. It affects boys and girls roughly equally in childhood, and the peak onset clusters around three predictable transitions. [6]
Those transitions are the introduction of solids, toilet training in the toddler years, and the start of school. Each brings a change in diet, routine, or the availability of a comfortable toilet, and each can be the setting for a first painful stool that triggers withholding. A family history of constipation, low dietary fibre and fluid intake, reduced physical activity, and a single frightening or painful defaecation all raise the risk. [1]
Psychosocial and developmental factors shape both onset and persistence. Anxiety, difficult toilet training, and stressful life events can trigger withholding, and children with autism spectrum disorder or intellectual disability are affected more often and can be harder to treat. Painful anal conditions such as a fissure, and coercive or punitive toileting, feed the fear that keeps the cycle turning. [2]
Pathophysiology
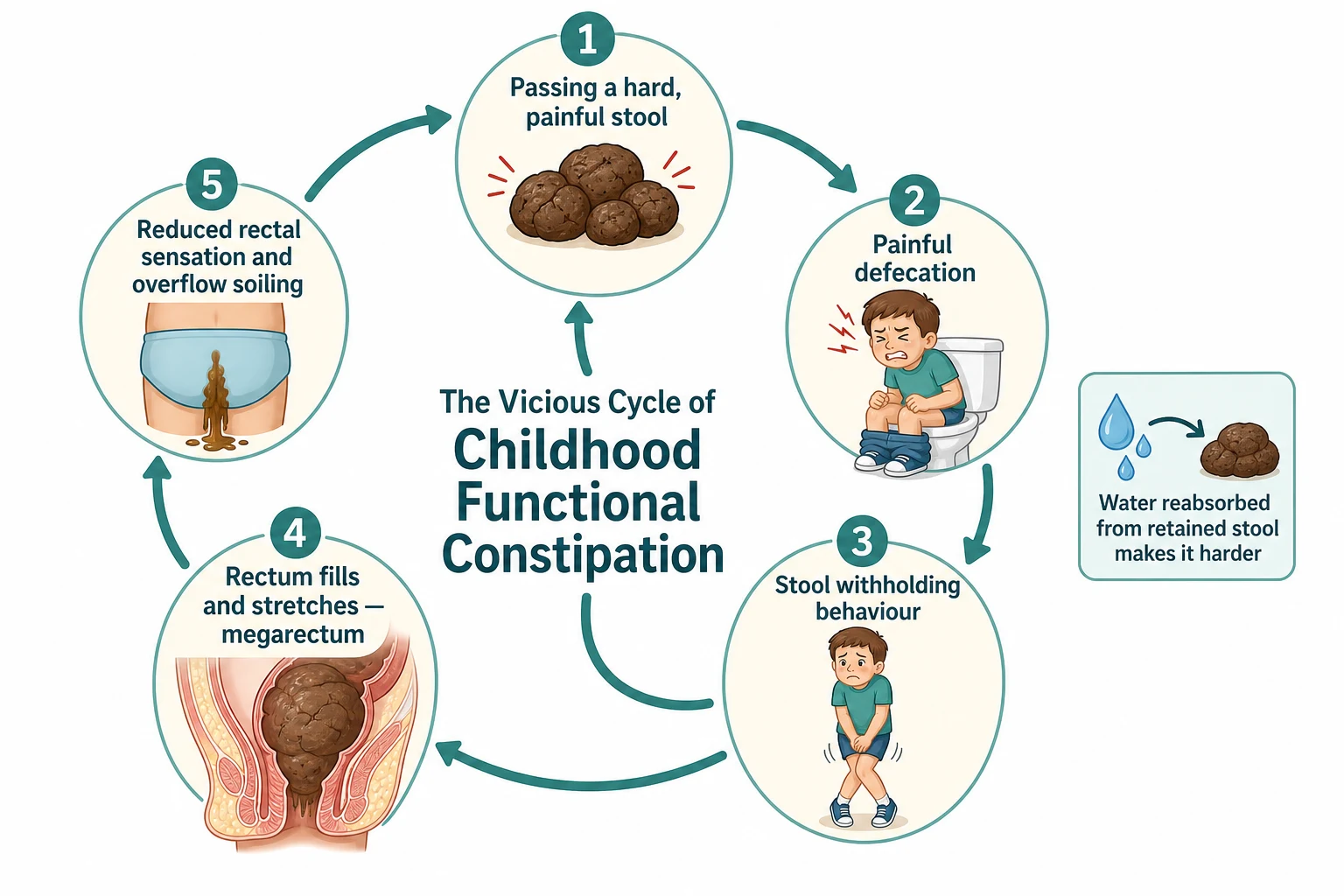
Functional constipation is driven by a self-reinforcing cycle rather than by any structural fault. It usually starts when a child passes a hard or painful stool, often at a time of dietary or routine change. The pain teaches the child to associate defaecation with distress, so they begin to withhold, clenching the buttocks and pelvic floor to hold stool in and avoid the feared event. [1]
Withheld stool sits in the rectum, where the colon continues to reabsorb water from it. The retained stool becomes larger, harder, and more painful, so the next attempt hurts more and the withholding deepens. Over weeks to months the rectum stretches to accommodate the growing mass, producing a dilated, low-tone megarectum that no longer generates a strong urge to defaecate. [2]
As the rectum enlarges and its wall stretches, the child loses the normal sensation that signals a full rectum. Fresh liquid or soft stool then tracks down and leaks around the hard impaction, escaping through an anus the child can no longer keep fully closed. This overflow is the mechanism of retentive faecal incontinence, and the child is genuinely unaware of it. Breaking this cycle requires both emptying the rectum and keeping it empty long enough for tone and sensation to recover. [1]
Clinical Presentation
The presentation shifts with age but the underlying story is consistent. Infants may strain, arch, and pass hard pellets, sometimes with a small anal fissure and blood-streaked stool. Toddlers show the classic withholding posture: standing on tiptoe, stiffening the legs, crossing the ankles, hiding in a corner, and going red in the face while parents mistake the effort for straining to pass rather than to hold. [2]
Older children present with infrequent bowel motions, large-diameter stools that can block the toilet, abdominal pain, poor appetite, and faecal soiling of the underwear. The soiling is often the reason for referral and is a major source of distress, bullying, and low self-esteem. A palpable, non-tender abdominal faecal mass and a loaded rectum are common findings that confirm the retentive picture. [1]
Non-retentive faecal incontinence looks different and must be separated from overflow. These children soil, usually in the afternoon or evening, but pass normal-calibre stools, have no palpable faecal mass, and show no withholding. The problem sits at the interface of bowel function and emotional or behavioural regulation, and it does not respond to laxatives. Recognising it prevents the futile escalation of osmotic treatment. [11]
Age-related clues to functional constipation
Infant: hard pellets, straining, anal fissure with blood streaks
Toddler: tiptoe withholding posture, ankle crossing, red face
Preschool: refusal of the toilet after toilet training begins
School-age: infrequent large stools, abdominal pain, soiling
Any age: palpable abdominal faecal mass and loaded rectum
Overflow soiling that parents may report as diarrhoea
Differential Diagnosis
The overriding question is whether this is functional constipation or one of the uncommon organic causes, and red flags decide it. When the story is typical, the examination is normal apart from faecal loading, and no red flags are present, functional constipation can be diagnosed positively. When red flags appear, the differential opens up and directed assessment follows. [1]
Hirschsprung disease is the classic organic mimic and must be considered whenever constipation dates from birth, meconium was delayed beyond forty-eight hours, or the child has failure to thrive and abdominal distension. Other organic causes include hypothyroidism, coeliac disease, cows milk protein allergy, hypercalcaemia, anorectal malformation, and spinal cord problems such as tethered cord or spina bifida occulta. Some medications, including opioids and certain anticonvulsants, also cause constipation. [1]
For faecal incontinence specifically, the differential is between retentive overflow, which accompanies constipation, and non-retentive incontinence, which does not. It is also essential to consider sexual abuse in any child with unexplained soiling, anal signs, or behavioural change, and to keep an open mind about neurological and structural anorectal disease. A careful history and examination usually distinguish these without extensive testing. [11]
Clinical & Bedside Assessment
A focused history is the highest-yield tool and should map the whole story of the bowels. Ask about the age of onset and any link to meconium delay, weaning, toilet training, or a painful stool. Characterise stool frequency, size, and consistency, the presence of withholding behaviour, blood, and pain, and ask specifically about soiling, its timing, and whether the child seems aware of it. Screen directly for red flags at every visit. [1]
Give real attention to diet, fluids, activity, and the toileting environment, and to the psychosocial context. Ask how toilet training went, whether toileting has ever been punitive or frightening, how the family and school respond to soiling, and how the problem affects the child's mood and friendships. In any child with unexplained soiling, keep the possibility of maltreatment in mind and ask sensitively. [2]
The examination should be gentle, thorough, and reassuring. Plot growth, examine the abdomen for a faecal mass, and inspect the perianal area, the lower spine for a dimple, sinus, or hair tuft, and the lower limbs for tone, power, reflexes, and the anal wink. A digital rectal examination is not routinely required to diagnose functional constipation and should be reserved for specific indications and performed by an experienced clinician. [1]
Investigations
Functional constipation is a clinical diagnosis and needs no routine investigation in a well child with a typical history and normal examination. Blood tests, plain abdominal radiographs, and transit studies do not add to a confident clinical picture and can mislead or delay treatment. A plain abdominal film in particular is neither sensitive nor specific for faecal loading and should not be used to confirm constipation. [1]
Targeted tests are reserved for atypical features, red flags, or treatment failure. Coeliac serology with total immunoglobulin A, thyroid function, and calcium are reasonable when growth faltering or an atypical course raises concern about an organic cause. A trial of removing cows milk protein can help selected infants whose constipation resists standard treatment, undertaken in a structured, time-limited way. [1]
When Hirschsprung disease is suspected, specialist referral for a rectal suction biopsy is the definitive step, sometimes preceded by anorectal manometry or a contrast enema. Spinal imaging is indicated when the examination suggests a cord lesion. The guiding principle is to investigate the child whose story or examination is atypical, and to treat rather than test the far larger group with clear functional constipation. [1]
Management — Resuscitation
Most constipation is managed in the community and needs no acute intervention, but a few presentations demand urgent attention. A neonate with delayed meconium, bilious vomiting, and abdominal distension may have Hirschsprung disease with enterocolitis, a surgical emergency requiring resuscitation, decompression, antibiotics, and urgent surgical review. Any child with signs of obstruction or peritonism needs the same immediate assessment. [3]
In the acutely unwell child, assess airway, breathing, and circulation, secure intravenous access, correct dehydration and electrolyte disturbance, and keep the child fasted while a surgical cause is excluded. Severe faecal impaction can occasionally cause distension, vomiting, and overflow that prompts an acute presentation, and it may need in-hospital disimpaction when oral treatment at home has failed or is not tolerated. [5]
For the common non-acute presentation, the immediate priority is different. It is to explain the diagnosis clearly, remove blame, and begin adequate treatment without delay. A confident, non-punitive explanation of the withholding cycle and overflow soiling is itself therapeutic, because it changes how the family and child approach the toilet and improves adherence to the treatment that follows. [1]
When constipation becomes an emergency
Neonate with delayed meconium, bilious vomiting, distension
Assess ABC, resuscitate, and correct fluids and electrolytes
Suspect Hirschsprung enterocolitis and start antibiotics
Keep fasted and obtain urgent surgical and specialist review
Exclude obstruction and peritonism before attributing to stool
Admit for disimpaction if home oral treatment has failed
Management — Definitive & Stepwise
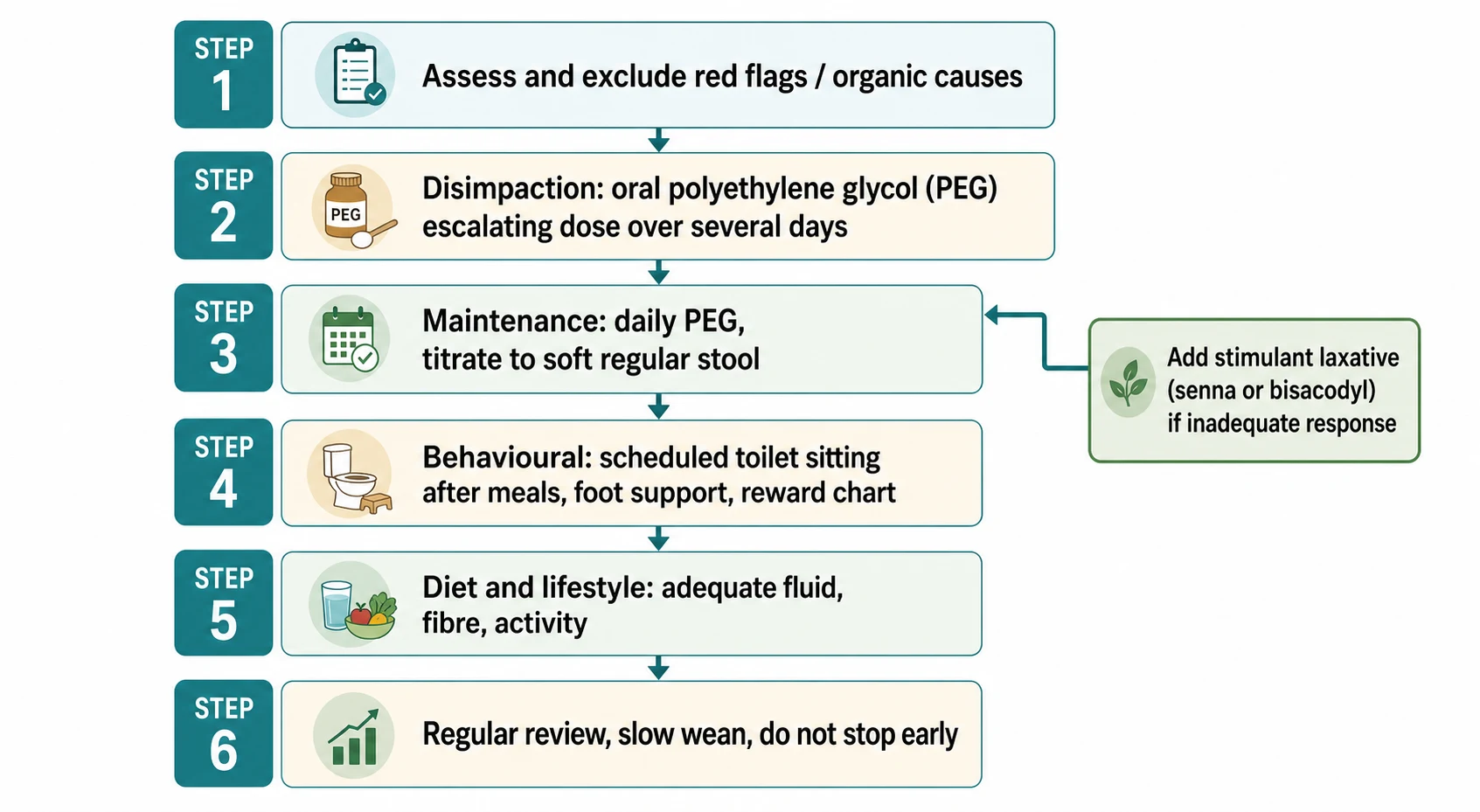
Treatment follows a clear sequence that the whole team should understand: disimpact, maintain, support behaviour, and review over months. Once red flags are excluded, the first step in a child with a significant faecal mass is disimpaction, because starting maintenance-dose laxatives on top of a large impaction increases soiling and undermines confidence. Oral polyethylene glycol is the first-line agent for both phases. [1]
Disimpaction uses an escalating high dose of oral polyethylene glycol over several days. In a randomised trial, high-dose oral polyethylene glycol was as effective as enemas for rectal disimpaction and was better tolerated, which supports an oral-first approach in most children. Enemas are reserved for children who cannot tolerate or do not respond to oral treatment. [5]
Polyethylene glycol 3350 — disimpaction
Dose
1 to 1.5 g/kg/day orally for 3 to 6 consecutive days (an escalating sachet regimen is an alternative, increasing over about a week)
Maintenance begins as soon as the rectum is cleared and continues for months to allow the stretched rectum to recover tone and sensation. A placebo-controlled trial confirmed that polyethylene glycol is effective and safe for maintenance in children. The dose is titrated to produce a soft, regular, painless stool, and the commonest mistake is stopping too soon, which allows the impaction and cycle to return. [7]
Polyethylene glycol 3350 — maintenance
Dose
Start about 0.4 g/kg/day orally (usual range 0.2 to 0.8 g/kg/day), titrated to one soft painless stool daily
Behavioural and lifestyle measures are woven through the whole plan. Encourage regular, unhurried toilet sitting for a few minutes after meals to use the gastrocolic reflex, with proper foot support so the child can brace, and a simple reward chart for sitting rather than for producing stool. Advise adequate fluid, a normal balanced diet with fruit, vegetables, and fibre, and physical activity, while being clear that diet alone will not clear an established impaction. [1]
[4]When an osmotic laxative alone does not maintain regular soft stools, a stimulant laxative such as senna or bisacodyl is added. A Cochrane review found osmotic and stimulant laxatives effective in childhood constipation, with polyethylene glycol outperforming placebo, lactulose, and milk of magnesia, though the overall evidence quality was limited. The combination of adequate dosing, behavioural support, and persistence, rather than any single drug, delivers the best results. [4]
Specific Subtypes & Scenarios
Infant constipation deserves a tailored approach because the differential and the treatments differ from older children. Simple functional constipation in a bottle-fed infant may respond to correcting feed preparation and adding extra water or a lactulose. A structured, time-limited trial of a cows milk protein-free diet can help selected infants with resistant constipation, and delayed meconium in a neonate should prompt evaluation for Hirschsprung disease. [3]
Retentive faecal incontinence is managed by treating the underlying constipation, and the soiling resolves as the impaction clears and the rectum recovers. Families need to be warned that soiling can worsen transiently during disimpaction, so they do not abandon treatment. Non-retentive faecal incontinence is a separate problem that does not respond to laxatives and is managed with toileting routines, reassurance, and psychological or behavioural support. [11]
Refractory constipation that fails optimal medical treatment warrants specialist review to reconsider the diagnosis, check adherence and dosing, and consider further options. These can include anorectal manometry, transanal irrigation, and, in a small minority, antegrade continence enemas through an appendicostomy. Reassessing for a missed organic cause and for unaddressed behavioural or safeguarding factors is essential before escalating invasive treatment. [9]
[1]Complications & Pitfalls
The main complications flow from an established, undertreated cycle. Chronic pain, anal fissures, rectal bleeding, and recurrent urinary tract infections or enuresis from a distended rectum pressing on the bladder are common. The most damaging complications are psychosocial: the shame, bullying, and low self-esteem that accompany soiling, and the family conflict that grows when the child is wrongly blamed. [1]
The classic treatment pitfalls are avoidable and heavily examined. The commonest is inadequate treatment: starting maintenance without disimpacting, using too low a dose, or stopping too soon at the first improvement, all of which allow relapse. A second is misreading overflow soiling as diarrhoea and treating it as such, and a third is over-investigating a straightforward functional case, particularly with unhelpful abdominal radiographs. [8]
The final pitfall is complacency in the face of red flags. Attributing constipation from birth, growth faltering, or abnormal neurology to a simple functional cause risks missing Hirschsprung disease, a spinal lesion, or maltreatment. Safety-netting with clear review, and a willingness to reassess when the pattern does not fit or treatment fails, guards against both undertreatment and missed organic disease. [1]
Prognosis & Disposition
The outlook is good for most children when treatment is early, adequate, and sustained, and the majority recover with polyethylene glycol and behavioural support. Recovery is gradual, and relapses are common, so families should expect a fluctuating course over months rather than a quick cure. Clear expectations at the outset improve adherence and reduce the disappointment that drives families to abandon treatment. [1]
A significant minority follow a more persistent course, and long-term follow-up shows that a proportion of children continue to have symptoms into adolescence and adulthood. Persistence is more likely with later presentation, a longer duration before treatment, and greater severity at the start, which is a powerful argument for treating early and well. Ongoing symptoms in adulthood, though a minority outcome, underline that this is not always a self-limiting problem. [8]
Most children are managed entirely in primary care and general paediatrics, with follow-up focused on stool pattern, soiling, adherence, and the child's wellbeing. Referral to paediatric gastroenterology or surgery is appropriate for red flags, suspected Hirschsprung disease, or failure of optimal treatment, and referral to psychology helps where behavioural or emotional factors dominate. Regular review and slow, supervised weaning prevent early relapse. [9]
Special Populations
Children with neurodevelopmental conditions such as autism spectrum disorder, cerebral palsy, and intellectual disability have higher rates of constipation and are often harder to treat. Sensory sensitivities, communication difficulties, reduced mobility, restricted diets, and medication side effects all contribute, and management must adapt with visual supports, structured routines, and close coordination with families and carers. Treatment thresholds should be low, and reviews frequent. [2]
Faecal incontinence in any child raises the need to consider maltreatment, and unexplained soiling, anal injury, or associated behavioural change must be assessed sensitively with safeguarding in mind. Soiling also carries a heavy social cost, and children may face bullying and exclusion, so involving the school in a supportive, non-punitive plan is an important part of care. [11]
Socioeconomic disadvantage and limited access to continence services, dietitians, and psychology can delay diagnosis and worsen outcomes. Practical, low-cost measures such as clear explanation, a well-titrated polyethylene glycol regimen, primary care follow-up, school liaison, and telehealth support help families who cannot easily reach specialist centres. Cultural attitudes to toileting and soiling also shape how families engage and should be explored respectfully. [9]
[6]Evidence, Guidelines & Regional Differences
The joint ESPGHAN and NASPGHAN evidence-based guideline is the reference standard for evaluation and treatment of functional constipation in infants and children. It supports a positive clinical diagnosis using the Rome criteria, discourages routine abdominal radiographs, and recommends polyethylene glycol as first-line for both disimpaction and maintenance. Its stepwise, family-centred approach underpins both practice and examinations. [1]
The Rome IV criteria define functional constipation separately for infants and toddlers and for older children and adolescents, requiring a minimum set of features over a defined period. The trial and review evidence is consistent on the mainstays: high-dose oral polyethylene glycol matches enemas for disimpaction, polyethylene glycol is effective and safe for maintenance, and osmotic and stimulant laxatives are the core pharmacological tools. [2]
[4]Controversies and regional differences persist despite broad agreement on the framework. The optimal disimpaction regimen, the role of routine dietary fibre supplements, the place of newer agents, and the management of truly refractory constipation all remain debated, and the evidence base for many interventions is limited. Access to polyethylene glycol products, continence services, and psychology varies markedly between and within countries, which shapes what is achievable in practice. [9]
Exam Pearls
FLAGSS for red flags in childhood constipation
References
- [1]Tabbers MM, DiLorenzo C, Berger MY, Faure C, Langendam MW, Nurko S, Staiano A, Vandenplas Y, Benninga MA Evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN. J Pediatr Gastroenterol Nutr, 2014.PMID 24345831
- [2]Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, van Tilburg M Functional Disorders: Children and Adolescents. Gastroenterology, 2016.PMID 27144632
- [3]Benninga MA, Faure C, Hyman PE, St James Roberts I, Schechter NL, Nurko S Childhood Functional Gastrointestinal Disorders: Neonate/Toddler. Gastroenterology, 2016.PMID 27144631
- [4]Gordon M, MacDonald JK, Parker CE, Akobeng AK, Thomas AG Osmotic and stimulant laxatives for the management of childhood constipation. Cochrane Database Syst Rev, 2016.PMID 27531591
- [5]Bekkali NL, van den Berg MM, Dijkgraaf MG, van Wijk MP, Bongers ME, Liem O, Benninga MA Rectal fecal impaction treatment in childhood constipation: enemas versus high doses oral PEG. Pediatrics, 2009.PMID 19948614
- [6]Mugie SM, Benninga MA, Di Lorenzo C Epidemiology of constipation in children and adults: a systematic review. Best Pract Res Clin Gastroenterol, 2011.PMID 21382575
- [7]Nurko S, Youssef NN, Sabri M, Langseder A, McGowan J, Cleveland M, Di Lorenzo C PEG3350 in the treatment of childhood constipation: a multicenter, double-blinded, placebo-controlled trial. J Pediatr, 2008.PMID 18534221
- [8]Bongers ME, van Wijk MP, Reitsma JB, Benninga MA Long-term prognosis for childhood constipation: clinical outcomes in adulthood. Pediatrics, 2010.PMID 20530072
- [9]van Mill MJ, Koppen IJN, Benninga MA Controversies in the Management of Functional Constipation in Children. Curr Gastroenterol Rep, 2019.PMID 31025225
- [10]Koppen IJN, Vriesman MH, Saps M, Rajindrajith S, Shi X, van Etten-Jamaludin FS, Di Lorenzo C, Benninga MA, Tabbers MM Prevalence of Functional Defecation Disorders in Children: A Systematic Review and Meta-Analysis. J Pediatr, 2018.PMID 29656863
- [11]Rajindrajith S, Hathagoda W, Devanarayana NM, Benninga M Non-retentive fecal incontinence in children: current perspectives and future directions. Expert Rev Gastroenterol Hepatol, 2026.PMID 42090001