Paeds · gastroenterology-hepatology-and-nutrition
Enteral feeding tubes and home enteral nutrition
Also known as Paediatric enteral feeding · Feeding tube management · Gastrostomy in children · Nasogastric feeding · Home enteral nutrition · Blenderised tube feeds
Fellowship guide to paediatric enteral feeding tubes and home enteral nutrition: the child with cerebral palsy who cannot swallow safely and needs a gastrostomy, the short-term nasogastric tube verified by gastric aspirate pH 5.5 or below, the percutaneous endoscopic gastrostomy and the low-profile balloon button, the post-pyloric jejunostomy for reflux and aspiration, the complications of granulation tissue, buried bumper syndrome, tube migration and stoma infection, blenderised versus commercial feeds, and the home enteral nutrition programme of caregiver training, supplies, monitoring and the emergency plan.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the four-year-old with severe cerebral palsy whose mealtimes last ninety minutes and end in a wet cough, the infant recovering from cardiac surgery who cannot yet take enough by mouth, and the adolescent with a metabolic disorder who needs precise overnight calories. Each needs nutrition the mouth cannot reliably deliver, and each will meet an enteral feeding tube. The clinician's job is to choose the right device, place and verify it safely, run the feeding regimen, and hand a workable plan to the family for home. [1] [8]
Enteral nutrition means delivering food into the gastrointestinal tract rather than into a vein, and whenever the gut works it is the route of choice, because it feeds the gut mucosa itself, preserves the intestinal barrier, avoids the line-infection and liver risks of parenteral nutrition, and costs far less. A feeding tube is simply the plumbing that gets nutrition into a stomach or small bowel that the child cannot fill by mouth. The choice between a tube through the nose, a tube through the abdominal wall, and a tube placed beyond the stomach follows the expected length of feeding and the child's reflux and aspiration status. [1] [3]
Home enteral nutrition is where this topic meets real life. Most tube-fed children live at home, fed by parents who must learn to pass a nasogastric tube, run a feed pump, look after a stoma, recognise a blocked or dislodged tube, and know when to come in. The medical role shifts from bedside doctor to designer of a safe, sustainable home programme, with the dietitian, the specialist nurse and the family at its centre. [8] [1]
Classification
The most useful way to hold the devices is by where the tube ends and how long it will stay there, because those two facts drive every later decision. A tube that ends in the stomach is gastric feeding, and a tube that ends in the jejunum is post-pyloric feeding, which matters when reflux or aspiration make the stomach an unsafe reservoir. A tube that stays for days to weeks is usually a nasogastric tube, while one that stays for months to years is a gastrostomy through the abdominal wall. [1] [3]
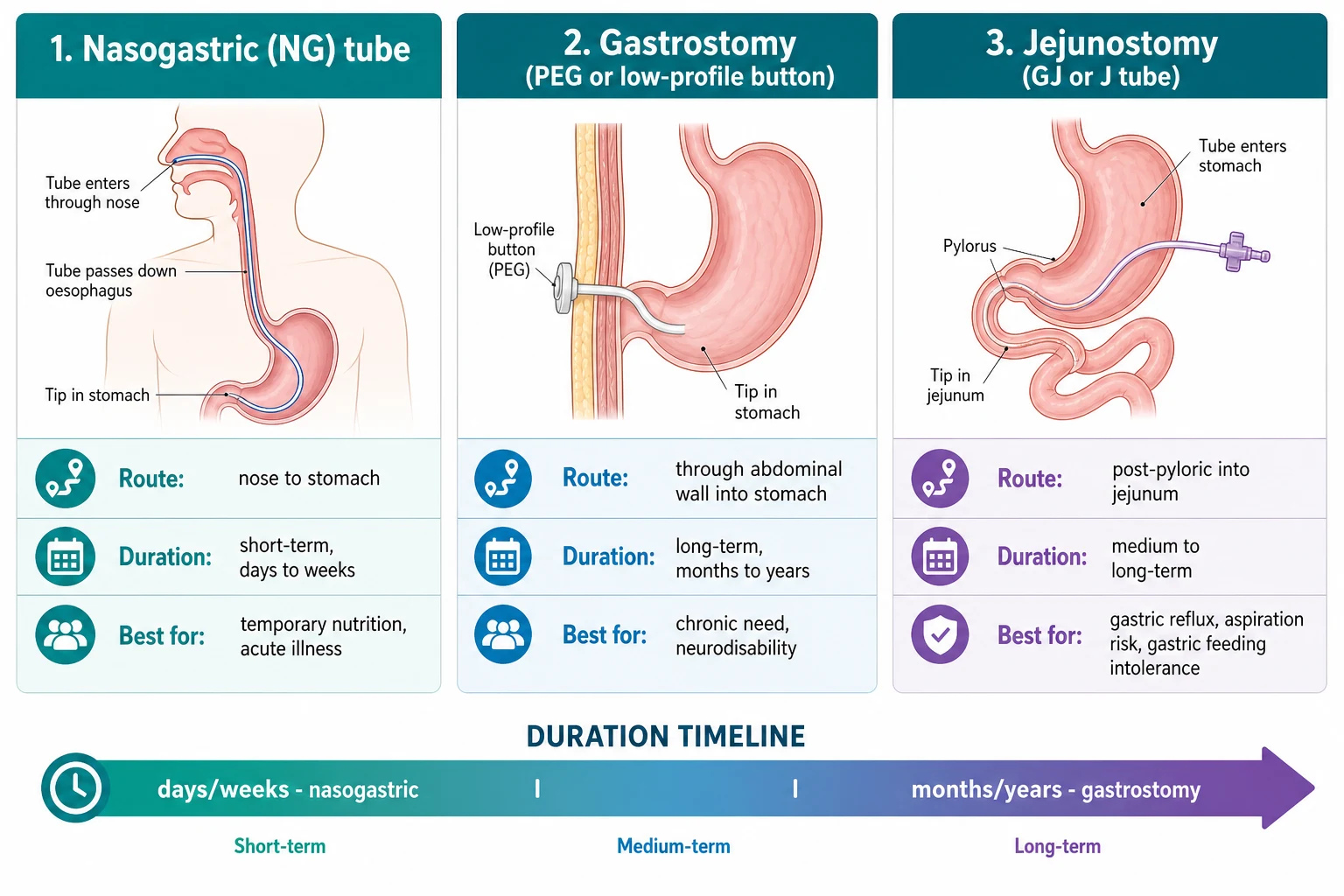
The gastric devices come in two long-term shapes. A percutaneous endoscopic gastrostomy, placed endoscopically, is held by an internal bumper against the gastric wall and an external flange against the skin; it is the workhorse device when feeding is first established. A low-profile balloon gastrostomy button sits flush on the abdominal wall, retained by a water-filled balloon inside the stomach, and is exchanged at the bedside; families and children usually prefer it for cosmesis and concealment, and it is increasingly placed as the primary device. The two are interchangeable across the life of a long-term feeding programme. [10] [1]
Post-pyloric feeding splits into a jejunostomy, a tube ending directly in the jejunum, and a gastrojejunostomy, a tube that enters through a gastric stoma but passes on to deliver feed into the jejunum. Both are reserved for the child whose reflux, aspiration or gastric emptying failure makes the stomach unsafe, and both demand continuous rather than bolus feeding because the jejunum cannot store a meal. They displace and block more often than gastric tubes, which is part of their cost. [9] [8]
[1] [9]Epidemiology & Risk Factors
Tube feeding sits at the heart of paediatric complex chronic disease. The children who need it are those whose intake is unsafe, insufficient or both: the child with cerebral palsy whose swallow risks aspiration, the cardiac infant whose breathlessness exhausts feeding, the extremely premature baby whose gut and suck are immature, and the child with a metabolic or neuromuscular disease whose demand outstrips what the mouth can deliver. Neurodisability is the single commonest thread, and the neurologically impaired child is the patient around whom most of this topic is built. [8] [12]
A dysphagic child who still aspirates despite texture modification, a child whose growth keeps faltering despite maximised oral feeding, and a child whose illness drives energy demand beyond what can be swallowed — these are the three situations that make tube feeding necessary. Named plainly, they are unsafe intake, insufficient intake and increased requirement. A fourth practical use is reliable delivery of medication, fluid or electrolyte when swallowing is unreliable. [8] [1]
Home enteral nutrition is a growing service as survival from prematurity, congenital heart disease and complex neurodisability improves. The burden it places on families is real and unequal: the cost of formula and consumables, the logistics of pumps and giving sets, the lost sleep of overnight feeds, and the anxiety of a dislodged tube at midnight fall hardest on families far from a specialist centre, on Indigenous and migrant families, and on those with the least support. Designing a programme that survives at home is as much a social as a clinical task. [8] [1]
Pathophysiology
Why feed the gut at all? The intestinal mucosa is not a passive pipe; it is a metabolically hungry surface that atrophies when it rests, and the luminal nutrients from enteral feeding directly nourish the enterocytes and preserve the tight junctions that keep bacteria and endotoxin out of the bloodstream. Enteral feeding therefore protects the gut barrier in a way parenteral nutrition cannot, which is the physiological reason it is the default route whenever the gut works. [1] [3]
The complications each have their own mechanism, and knowing them explains the bedside signs. Granulation tissue is the foreign-body response to a tube sitting through the skin: the stoma stays chronically inflamed, the body tries to wall off the tube, and a friable, beefy, bleeding mound of tissue grows up around the exit site. It is benign but distressing, and it weeps and bleeds and leaks. Buried bumper syndrome is its dangerous cousin: the internal bumper of a percutaneous endoscopic gastrostomy slowly migrates and erodes into the gastric wall, becoming buried in the wall itself, so feed can no longer pass and the child has abdominal pain with a tube that will not run. [7] [1]
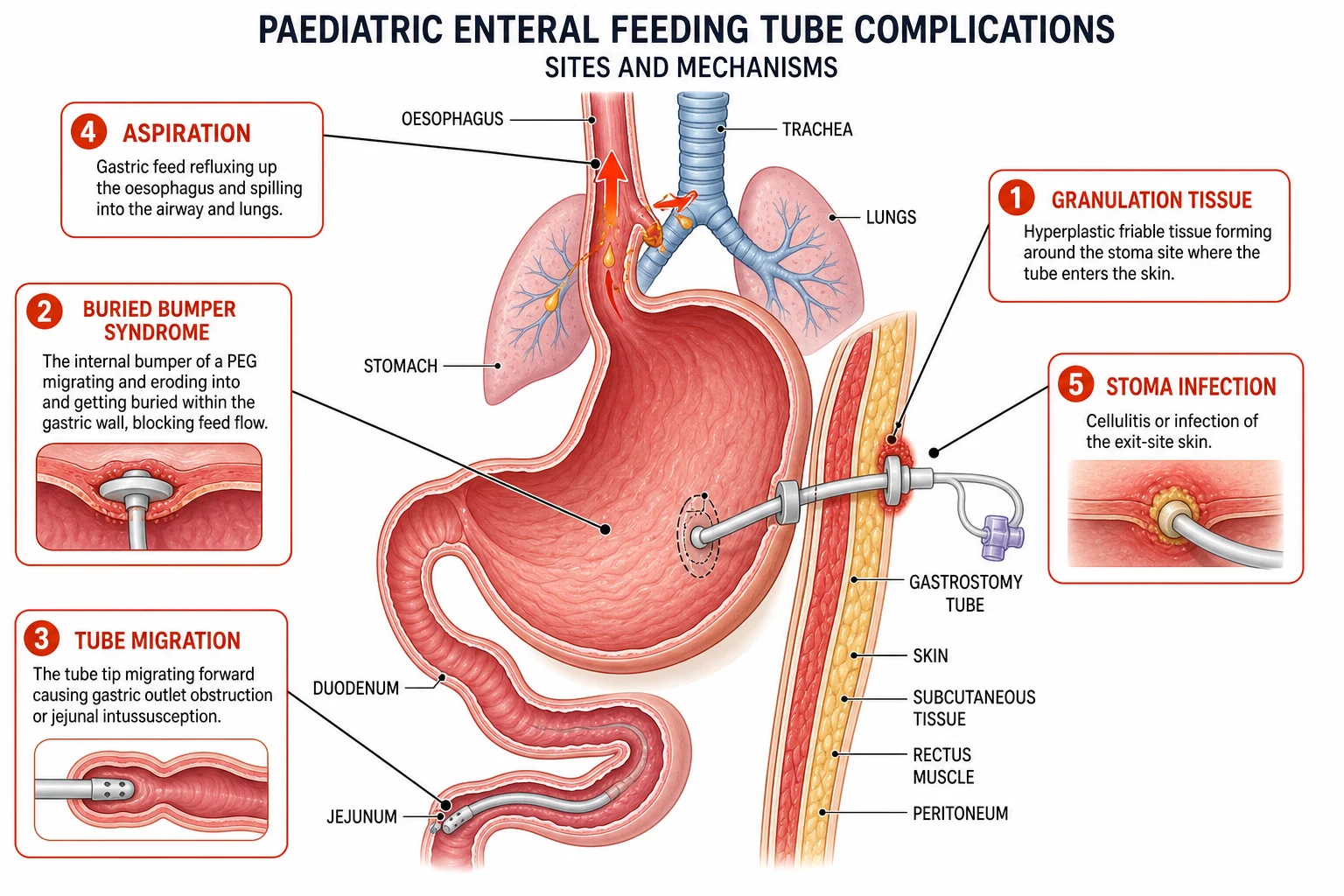
Aspiration in a tube-fed child is usually reflux of gastric feed up the oesophagus and over into the airway, and the risk climbs with recumbency, large bolus volumes and delayed gastric emptying. A post-pyloric tube reduces the reservoir that can reflux, but it does not abolish aspiration, because oral secretions and refluxed jejunal contents can still reach the airway. Tube migration is the fourth mechanism to hold: a tube that slips forward can obstruct the gastric outlet or intussuscept the bowel, presenting as vomiting, feed intolerance or obstruction. [7] [9]
Finally, the refeeding mechanism is the one that catches the unwary. A starved child who suddenly receives carbohydrate drives insulin release, which shifts phosphate, potassium and magnesium into cells and drops their serum levels, while the thiamine-dependent metabolism of glucose can precipitate acute thiamine deficiency. The malnourished child starting tube feeding is precisely the child at risk, which is why refeeding is a planned, monitored process and not a free run of feed. [8] [1]
Clinical Presentation
The child who needs a feeding tube usually arrives through one of three doors. The first is the swallow: a child with neurodisability whose mealtimes are prolonged, distressing or unsafe, with coughing, choking or a wet voice, has an oropharyngeal dysphagia that puts the lung at risk. The second is the growth chart: a child whose weight or length is falling despite maximised oral intake and fortification is failing to thrive on what the mouth can deliver. The third is the acute illness: a cardiac or surgical infant, or a metabolically decompensated child, who needs reliable nutrition the gut can absorb while the body recovers. [8] [12]
The complications present themselves, and recognising them early keeps children out of hospital. A nasogastric tube that has migrated into the airway or curled in the oesophagus causes coughing, respiratory distress or feed that makes the child splutter, and feeding it is the error to avoid. A dislodged gastrostomy presents as a tube lying on the bedclothes or a stoma that is open, and the urgency is replacement before the tract closes. Granulation tissue presents as a bleeding, weeping mound at the stoma, and stoma infection as spreading erythema, pain, discharge or fever. [7] [1]
The home-enteral presentations that bring a family back are practical and often preventable. A blocked tube that will not flush, a split balloon that lets the button fall out, feeding intolerance with vomiting or diarrhoea, a leaking stoma that excoriates the skin, and the malnourished child who, days into feeding, develops the lethargy and electrolyte disturbance of refeeding. The best defence against these returns is a family trained to manage the routine and a clear written plan for the emergency, because a confident carer resolves most problems at home. [1] [8]
[7] [1]Differential Diagnosis
The question of whether a child needs a tube is itself a differential, and the trap is inserting one when the problem is better solved another way. For the child failing oral feeding, separate the causes that genuinely need enteral access from those that respond to medical or behavioural management. Oral sensory aversion, uncontrolled reflux, untreated constipation and behavioural food refusal can all masquerade as feeding failure, and each has a better first answer than a tube. The tube is the answer when the swallow is unsafe, when the intake is absolutely insufficient despite optimised oral management, or when the metabolic demand is unreachable by mouth. [8] [1]
Feed intolerance has its own differential, and the temptation is to blame the formula when the tube is the culprit. Vomiting, diarrhoea and abdominal pain in a tube-fed child can reflect feed osmolarity or rate, but they can equally reflect a tube that has migrated to obstruct the pylorus, a jejunal tube that has curled back into the stomach, or an intercurrent gastroenteritis or constipation. Reading the problem means checking the tube position and the bowel pattern before changing the feed. [9] [7]
A leaking stoma is a differential that frustrates families, and the causes run from the trivial to the serious. A stoma that is still settling in the first weeks after insertion may leak a little as it matures. A tube that is too small for the tract, or a balloon that has deflated or ruptured, lets the tube slide and widens the gap. Granulation tissue and infection both impair healing and worsen leak. Buried bumper syndrome, the serious end, presents with leak alongside feed that will not run and abdominal pain. Sorting these out determines whether the answer is a dressing change, a new tube, or an operation. [7] [1]
Why is this tube-fed child not growing — 'FEED'
Clinical & Bedside Assessment
Assessment begins before any tube is passed. Establish the indication and the expected duration, because these fix the device. Plot the weight, height and head circumference to quantify the nutritional deficit, and assess the reflux and aspiration status that will decide between gastric and post-pyloric feeding. Check the coagulation and the anatomy that might complicate placement, take consent, and make sure the child and family understand what the tube means for daily life. The assessment frames the whole plan, from device to regimen to home support. [1] [3]
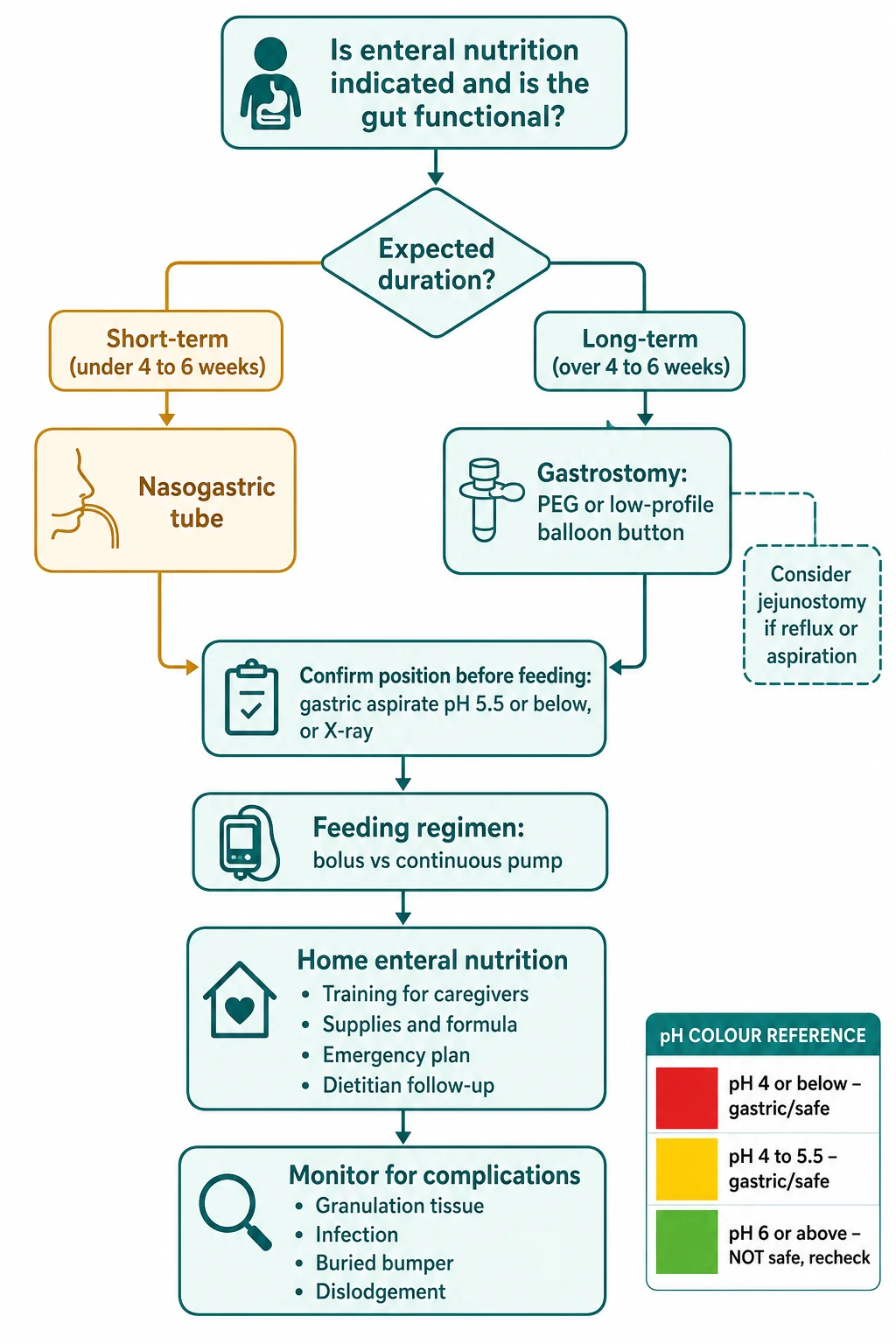
The bedside skill that every paediatric trainee must own is nasogastric tube verification, and the standard comes from the NOVEL Project. Before every feed, confirm the tube is at its documented insertion length, aspirate gastric contents, and test the pH. A pH of 5.5 or below is accepted as gastric and safe to feed. When aspirate cannot be obtained, or the pH is above 5.5, or the child is at high risk, confirm the position by X-ray, reading the tube tip below the diaphragm and curving toward the pylorus within the stomach. Verification is not optional and it is not a one-off: it belongs before every feed. [4] [5]
The auscultatory whoosh test, listening over the stomach while pushing air down the tube, is the verification method to name and discard. Studies of tube verification in hospitalised infants and children show it is unreliable and cannot distinguish a gastric from an oesophageal or airway position. Judging position by the colour or appearance of the aspirate is no better. The reliable methods are pH and radiography, and the disciplined practice is to use pH first and escalate to X-ray when pH is equivocal or unavailable. [5] [4]
For the child with a gastrostomy, the bedside assessment centres on the stoma and the device. Inspect for erythema, discharge, granulation and skin excoriation, check that the external flange sits comfortably against the wall without being too tight, and verify the balloon volume of a button. Test that feed and water flush freely, and feel the stoma for the subtle firmness of a bumper burying itself. The stoma tells the story of the device, and a careful weekly look catches problems long before they become admissions. [7] [1]
Investigations
Investigation in this topic is mostly the verification of tube position and the monitoring of nutrition, rather than a battery of tests. The first-line bedside confirmation of a nasogastric tube is gastric aspirate pH, with a reading of 5.5 or below accepted as gastric by the NOVEL Project. The practical limits are real: acid-suppression therapy raises gastric pH and can give a falsely reassuring high reading, neonates and small infants may yield too little aspirate to test, and colour-based reading of pH strips is prone to error, so a confirmed reading needs care and sometimes a second method. [4] [5]
Chest or abdominal X-ray is the gold-standard confirmatory test when pH is equivocal, when aspirate cannot be obtained, or in high-risk situations such as the first feed after insertion. The film is read for the tube tip lying below the diaphragm and curving toward the pylorus within the stomach, not tracking up the oesophagus or into the bronchial tree. Knowing when to request it is part of the discipline: after first insertion, after any suspected dislodgement, and whenever the pH method has failed to confirm position. [4] [5]
Before a gastrostomy is placed, the workup addresses the child as much as the device. A nutritional assessment and growth plotting quantify the deficit the tube will correct, and a consideration of upper endoscopy or a contrast study defines anatomy that may be uncertain, particularly after previous abdominal surgery. Reflux is assessed clinically and, when needed, with pH or impedance studies, because uncontrolled reflux may change the choice from a gastric to a post-pyloric device or prompt an anti-reflux procedure. Coagulation and a full blood count are checked before any procedure that breaches the abdominal wall. [8] [1]
Ongoing monitoring is where the tube-fed child is kept well over time. Weight, height and head circumference are plotted regularly to confirm the feed is meeting growth. Fluid balance and electrolytes are tracked, particularly during illness or when feeding is being established. The micronutrients that tube-fed children are prone to lose or lack, iron, vitamin D, zinc and vitamin B12, are checked periodically, and bone health is watched in the child on a restricted or long-term feed. The prescription is reviewed against the child's changing weight and requirement, because a feed that was right at six kilograms is wrong at sixteen. [8] [1]
When does pH verification need an X-ray instead?
Escalate to X-ray confirmation of a nasogastric tube when the aspirate pH is above 5.5 and cannot be brought down by repositioning, when no aspirate can be obtained despite repositioning and a small flush, when the child is on acid-suppression therapy that invalidates the pH reading, after the first insertion of a new tube, after any suspected dislodgement or significant coughing episode, and before the first feed in a high-risk child such as an infant or a child with an unsafe swallow. In these situations pH alone is not enough, and a film that shows the tube tip below the diaphragm within the stomach is the safe confirmation before feeding. [4] [5]
Management — Resuscitation
Most tube feeding is planned, but a small number of situations are emergencies, and the trainee must know them cold. A misplaced or migrated nasogastric tube that has fed into the airway or lung causes coughing and respiratory distress, and the immediate action is to stop feeding, withdraw the tube, assess and support the airway and breathing, and treat any aspiration event with oxygen and respiratory support. The chest film confirms the injury, and the lesson is that the feed should never have started without verified position. [4] [1]
The acutely dislodged gastrostomy is the second emergency, and the principle is speed. A mature stoma can close within hours, so the tube must be replaced promptly with a suitable Foley catheter or a spare device to keep the tract patent, even if the definitive device is fitted later. If the tube cannot be replaced, if there is peritonism, or if the dislodgement happened soon after insertion before the tract matured, the concern is intraperitoneal leak of feed, which is a surgical emergency. The child is kept nil by mouth, given intravenous fluids and antibiotics, imaged urgently, and reviewed by surgery. [1] [3]
A previously malnourished child starting enteral feeding carries the third resuscitation problem, refeeding syndrome. The sudden delivery of carbohydrate drives phosphate, potassium and magnesium into cells and can precipitate acute thiamine deficiency. The safe approach is to start with conservative calories, give thiamine before and during the first days of feeding, and monitor and correct phosphate, potassium and magnesium closely, advancing the feed only as the child tolerates and the biochemistry stays safe. [8] [1]
Immediate management of the tube-feeding emergency
Misplaced nasogastric tube in the airway: stop feeding, withdraw the tube, support the airway and breathing, treat aspiration with oxygen and a chest film
Acutely dislodged gastrostomy: replace promptly with a suitable catheter to keep the tract patent before it closes
Suspected intraperitoneal leak or peritonism: nil by mouth, intravenous fluids and antibiotics, urgent imaging and surgical review
Refeeding risk in the malnourished child: conservative starting calories, thiamine, and monitor and correct phosphate, potassium and magnesium
Stoma infection or cellulitis: swab the site, topical or systemic antibiotics guided by severity, and review device fit
Management — Definitive & Stepwise
The definitive plan follows a sequence, and the first step is always the same: confirm the gut is functional, because enteral feeding is the route of choice whenever it is. The expected duration of feeding then fixes the device, with a nasogastric tube for the short term under four to six weeks and a gastrostomy for anything longer. Reflux, aspiration or gastric intolerance add a post-pyloric jejunostomy or gastrojejunostomy when the stomach is not the right reservoir, accepting the higher displacement and blockage rate of these tubes as the price of safer feeding. [1] [9]
The feeding regimen converts the child's needs into a written prescription. Daily fluid and calorie targets are calculated from weight-based and activity-adjusted estimates, and the dietitian owns this calculation. The delivery method is chosen for the child and the gut: bolus feeding mimics meals and suits the ambulant child, while continuous pump feeding suits the child with poor tolerance, high overnight requirements, or a post-pyloric tube that cannot take a bolus. The rate and volume are advanced gradually to tolerance, watching for reflux, diarrhoea and refeeding signs as the feed builds. [1] [8]
The nasogastric pathway is the short-term workhorse. The tube is measured from nose to ear to xiphisternum, passed to the measured length, secured to the cheek or nose, and verified by pH before the first feed and before every feed thereafter. Daily care checks the nose for pressure, re-secures the tube, and watches for the subtle dislodgement that the family will learn to recognise at home. When feeding extends beyond the expected few weeks, the decision point for converting to a gastrostomy arrives, and delaying it leaves a child and family managing an increasingly inconvenient nasogastric tube. [4] [1]
The gastrostomy pathway is the long-term commitment. The device is placed percutaneously and endoscopically or at operation, the tract is allowed to mature over the first weeks, and the percutaneous endoscopic gastrostomy is often later converted to a low-profile balloon button for comfort and cosmesis, commonly around six to twelve weeks after insertion. Ongoing care addresses the balloon volume, the flange fit, the stoma skin and the elective device exchange, and the home programme is built around trained carers, reliable supplies, regular growth and micronutrient monitoring, and a written emergency plan for the blocked, dislodged or infected tube. [1] [10]
[1] [8]Specific Subtypes & Scenarios
The child with cerebral palsy and neurodisability is the central scenario, because this is the patient most likely to move from an unsafe swallow to a long-term gastrostomy. The swallow is often unsafe and always inefficient, reflux and constipation compound the feeding difficulty, and the ESPGHAN guideline on gastrointestinal and nutritional complications in neurologically impaired children frames the evaluation that should precede tube placement. A well-chosen gastrostomy in this child improves nutrition, growth, carer quality of life and mealtime distress, while the open questions of fundoplication and post-pyloric feeding are weighed against the child's reflux and aspiration. [8] [12]
The nasogastric tube as a short-term bridge is the second scenario. It is the default for acute illness, for post-operative recovery, and for the infant whose feeding is expected to recover within weeks. The technique is bedside, the verification is pH before every feed, and the daily reality for families is the management of a tube that dislodges, irritates the nose, and must be re-passed. The decision point is the duration: when feeding extends beyond four to six weeks, the balance tips toward a gastrostomy, and naming that moment prevents a child lingering on a nasogastric tube longer than serves them. [4] [1]
The low-profile balloon gastrostomy button is the third scenario, and it has changed the experience of long-term feeding for families and children. It sits flush on the abdominal wall, it is concealed under clothes, it does not catch on furniture, and families report better cosmesis and quality of life. It can be placed primarily or converted from a percutaneous endoscopic gastrostomy once the tract has matured, and it is exchanged at the bedside when the balloon fails or the child outgrows the stem length. The balloon volume is checked and topped up at routine intervals, and a split balloon with a tube that falls out is one of the home emergencies a family must be ready for. [10] [1]
The jejunostomy and gastrojejunostomy tube is the fourth, reserved for the child whose reflux, aspiration or gastric emptying failure makes the stomach an unsafe reservoir. A gastrojejunostomy tube enters through a gastric stoma but delivers feed into the jejunum, while a jejunostomy ends directly in the jejunum. Both demand continuous rather than bolus feeding, because the jejunum cannot store a meal, and both displace and block more often than gastric tubes, which is the recognised cost of safer feeding. The systematic evidence shows gastrojejunostomy complications are common and demand a team ready to manage them. [9] [7]
Across Australia, Aotearoa New Zealand and the United Kingdom, paediatric enteral feeding is delivered by a multidisciplinary nutrition team built around the paediatrician, the dietitian, the specialist nurse and the speech-language therapist, with surgical and gastroenterology services for device insertion and complications. Home enteral nutrition programmes fund formula and consumables through national schemes, though the detail and the reach of funding differ. The blenderised tube feed movement has grown across these regions, supported by the systematic evidence that it can improve upper gastrointestinal symptoms when carefully prescribed. In many low-resource, rural and remote settings the specialist teams and the funded supplies are distant, the burden of complex tube feeding falls on Indigenous and disadvantaged families, and telehealth-supported shared care with a locally trained carer network is what makes a home programme achievable. [8] [6]
Complications & Pitfalls
The complications divide by device, and the trainee should hold the common and the dangerous separately. Nasogastric tubes cause respiratory misplacement and aspiration when fed unverified, dislodgement and migration, nasal and pharyngeal irritation, and occasional oesophageal trauma from repeated passage. Gastrostomy and gastrojejunostomy tubes cause stoma infection, granulation tissue, leakage, buried bumper syndrome, tube migration with intussusception or pyloric obstruction, and the surgical emergency of peritonism from intraperitoneal leak. Jejunal tubes add the higher rates of displacement and blockage that come with a longer, finer lumen. [7] [9]
The prevalence evidence is sobering and useful for the viva. Studies of gastrostomy and gastrojejunostomy complications in children report that the majority of devices cause at least one complication over their life, with stoma infection, granulation and leakage the most frequent and buried bumper and peritonism the most serious. Gastrojejunostomy tubes carry a particular burden of displacement and blockage that often leads to repeated radiological or surgical interventions. Knowing this keeps the clinician vigilant rather than reassured, because a complication-free long-term tube is the exception, not the rule. [7] [1]
The diagnostic pitfalls are the errors the examiner rewards for naming. The first is feeding from a nasogastric tube without confirming position, which delivers feed into the lung. The second is trusting the auscultatory whoosh test or the appearance of aspirate rather than pH and radiography. The third is missing buried bumper syndrome in a child whose feed will not run, by repeatedly flushing and re-flushing a tube whose bumper is buried in the gastric wall. The fourth is failing to replace a dislodged gastrostomy before the tract closes, turning a bedside problem into a surgical one. [4] [7]
The management pitfalls cut both ways. Over-investigating a stoma leak that is settling in the first weeks wastes family time and worry, while under-recognising the peritonism of an intraperitoneal leak endangers the child. Under-treating granulation tissue leaves a bleeding, weeping site that distresses the family, while over-tightening the external flange in an attempt to stop a leak drives the bumper into the wall and causes the buried bumper the clinician was trying to prevent. The discipline is to read each complication against its mechanism and to keep the flange comfortably loose. [1] [7]
Prognosis & Disposition
The outcome of tube feeding is governed by the underlying condition, the adequacy of the nutritional prescription, and the avoidance of complications. A well-run gastrostomy programme in carefully selected children with cerebral palsy and neurodisability improves nutrition, growth, carer quality of life and mealtime distress, and the systematic evidence supports this benefit. The tube does not cure the underlying disease, but it removes the daily failure of insufficient or unsafe intake and lets the child and family live around nutrition rather than be consumed by it. [12] [8]
Complications are common but mostly manageable. Stoma infection and granulation are the most frequent and respond to topical care, antibiotics and device adjustment. Buried bumper and intraperitoneal leak are the most serious and need endoscopic or surgical intervention. Early recognition and a clear home emergency plan keep most children out of hospital, and a family confident in managing the routine and the common problems is the single best protection against repeated admissions. The prognosis of the device, in other words, depends heavily on the quality of the home programme. [7] [1]
Disposition follows the multidisciplinary team. The general paediatrician coordinates care with the dietitian, the speech-language therapist and the specialist nurse in the community or outpatient clinic. Tertiary paediatric gastroenterology and surgery manage device insertion and the serious complications, and a planned transition supports the adolescent moving to adult services, with handover of the feeding history, the device detail and the prescription. The straightforward, stable child is a community patient; the complex or newly-inserted child is a tertiary patient until stable. [1] [8]
Special Populations
The child with severe neurodisability and cerebral palsy is the first special population, and the principal recipient of a gastrostomy. The ESPGHAN guideline frames the evaluation that should precede tube placement: the reflux, the constipation, the aspiration and the nutrition are assessed together, and the choice between a gastric device, a post-pyloric tube and an anti-reflux procedure follows that evaluation. The aim is to secure nutrition and protect the lung while preserving any safe oral feeding for pleasure, because removing all oral experience carries its own developmental and emotional cost. [8] [12]
The neonate and infant is the second. The nasogastric tube is the default short-term access in the neonatal unit, and the immature gut and the risk of necrotising enterocolitis in the premature infant dictate cautious advancement of feed volume and rate. The developmental importance of preserving non-nutritive sucking and safe oral feeding alongside tube feeding is part of the plan, so that the infant builds oral skill while the gut matures and the tube carries the nutrition. The decision to convert to a gastrostomy in infancy waits until the duration and the prognosis of feeding difficulty are clear. [1] [4]
The technology-dependent child with a tracheostomy or long-term ventilation is the third. The interplay of airway, secretion management and feeding is complex, and aspiration risk is high, so the feeding device and the airway are managed by a specialist team together. A post-pyloric tube is often chosen when the airway and the reflux make the stomach unsafe, and the family is trained across both the airway and the feeding emergency, because the two can present together. [9] [8]
The Indigenous, remote, migrant and disadvantaged child is the fourth. The burden of complex chronic disease and tube feeding falls unevenly on these children, the specialist teams and the funded supplies are distant, and the cost and logistics of formula, pumps and consumables are harder to sustain. Culturally safe shared-care pathways, telehealth support for the local team, a locally trained carer network, and attention to the practical realities of power, refrigeration and transport are what make a home feeding programme achievable for families far from a specialist centre. [8] [1]
Evidence, Guidelines & Regional Differences
The evidence base rests on the ESPGHAN position paper on percutaneous endoscopic gastrostomy in children, updated by Homan and colleagues, which is the central guideline for indications, technique and complications and the document to quote in the viva. The Romano ESPGHAN guideline on gastrointestinal and nutritional complications in neurologically impaired children extends this into the highest-risk population, framing the evaluation of reflux, constipation, aspiration and nutrition that should precede tube placement. [1] [8]
The technique evidence is the part examiners probe. The Cassaro systematic review and meta-analysis compares percutaneous endoscopic and laparoscopic gastrostomy in children, and the Baker systematic review of gastrostomy insertion techniques sets the broader comparison of percutaneous, laparoscopic and open surgical approaches. The Cortez study establishes that primary placement of a low-profile gastrostomy button is safe and associated with improved outcomes, supporting the shift toward the button as a first device in selected children. [2] [3] [10]
The nasogastric verification evidence is the high-yield set. The Irving NOVEL Project best-practice recommendations established aspirate pH of 5.5 or below as the bedside standard for confirming gastric position, and the Northington follow-up evaluated the methods actually used to verify nasogastric tube placement in hospitalised infants and children, reinforcing the move away from the unreliable whoosh test. These two papers are the defence for the verification practice the examiner will test. [4] [5]
[1] [4]The controversies are three. First, whether gastrostomy worsens or unmasks gastro-oesophageal reflux: the Noble systematic review found the relationship between percutaneous endoscopic gastrostomy and reflux in children is not straightforward, and reflux must be assessed before and after placement rather than assumed. Second, blenderised versus commercial formulae: the Delcourt systematic review found blenderised tube feeding may improve upper gastrointestinal symptoms such as reflux and retching, but it demands careful attention to nutritional adequacy and microbial safety, which is the current balance point of practice. Third, the higher complication rate of gastrojejunostomy tubes, documented by the Morse and Gestels studies, which tempers their use to genuine post-pyloric indications. [11] [6] [9]
Exam Pearls
Choosing enteral access — 'TUBE'
References
- [1]Homan M; Hauser B; Romano C Percutaneous Endoscopic Gastrostomy in Children: An Update to the ESPGHAN Position Paper. J Pediatr Gastroenterol Nutr, 2021.PMID 34155150
- [2]Cassaro F; Impellizzeri P; Bartolone A Percutaneous endoscopic gastrostomy versus laparoscopic gastrostomy in pediatric age: A systematic review and meta-analysis. J Pediatr Gastroenterol Nutr, 2026.PMID 41229146
- [3]Baker L; Beres AL; Baird R A systematic review and meta-analysis of gastrostomy insertion techniques in children. J Pediatr Surg, 2015.PMID 25783383
- [4]Irving SY; Rempel G; Lyman B Pediatric Nasogastric Tube Placement and Verification: Best Practice Recommendations From the NOVEL Project. Nutr Clin Pract, 2018.PMID 30187517
- [5]Northington L; Kemper C; Rempel G Evaluation of methods used to verify nasogastric feeding tube placement in hospitalized infants and children - A follow-up study. J Pediatr Nurs, 2022.PMID 34763985
- [6]Delcourt H; Van Den Eynde R; De Belder L Blenderized tube feeding for children: A systematic review of health outcomes and impact on upper gastrointestinal symptoms. J Pediatr Gastroenterol Nutr, 2025.PMID 41144871
- [7]Gestels T; Hauser B; Van de Vijver E Complications of Gastrostomy and Gastrojejunostomy: The Prevalence in Children. Pediatr Gastroenterol Hepatol Nutr, 2023.PMID 37214169
- [8]Romano C; van Wynckel M; Hulst J European Society for Paediatric Gastroenterology, Hepatology, and Nutrition Guidelines for the Evaluation and Treatment of Gastrointestinal and Nutritional Complications in Children With Neurological Impairment. J Pediatr Gastroenterol Nutr, 2017.PMID 28737572
- [9]Morse J; Baird R; Muchantef K Gastrojejunostomy tube complications - A single center experience and systematic review. J Pediatr Surg, 2017.PMID 28162764
- [10]Cortez AR; Warren PW; Goddard GR Primary Placement of a Low-Profile Gastrostomy Button Is Safe and Associated With Improved Outcomes in Children. J Surg Res, 2020.PMID 31958600
- [11]Noble LJ; Dalzell AM; El-Matary W The relationship between percutaneous endoscopic gastrostomy and gastro-oesophageal reflux disease in children: a systematic review. Surg Endosc, 2012.PMID 22437953
- [12]Sleigh G; Brocklehurst P Gastrostomy feeding in cerebral palsy: a systematic review. Arch Dis Child, 2004.PMID 15155398