Paeds · gastroenterology-hepatology-and-nutrition
Feeding assessment and paediatric dysphagia
Also known as Paediatric dysphagia · Swallowing disorder in children · Feeding difficulty · Feeding assessment · Oropharyngeal dysphagia · Paediatric feeding and swallowing disorder
Fellowship guide to feeding assessment and paediatric dysphagia: the child who coughs, chokes or turns blue with feeds, the wet-voice and prolonged mealtimes of oropharyngeal dysphagia, the four phases of swallowing and where each can fail, the high-risk child with cerebral palsy or airway anomaly, why aspiration is often silent in neurodisability, the bedside clinical feeding evaluation followed by the videofluoroscopic swallow study and fibreoptic endoscopic evaluation of swallowing, the penetration-aspiration scale, the IDDSI texture ladder, the Eating and Drinking Ability Classification System, and the multidisciplinary plan from texture modification and positioning to enteral feeding.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the child who splutters, coughs and goes red in the face at every meal, the infant who arches, gags and turns blue around the mouth during a bottle feed, and the withdrawn, underweight child with cerebral palsy whose mealtimes last an hour and end in a wet, rattly cough. These are the faces of paediatric dysphagia, and the clinician's task is to work out where in the swallow the problem lies, how dangerous it is, and how to feed the child safely while the cause is addressed. [1] [2]
Dysphagia means difficulty swallowing, and in a child it is never a single disease but a symptom that can arise anywhere from the mouth to the stomach. The swallow moves food and liquid from the oral cavity through the pharynx and into the oesophagus while protecting the airway, and when that coordination fails, feed or saliva spills toward the lungs. The clinical question is always whether the child is aspirating, because aspiration drives the pneumonia, the chronic lung disease, the faltering growth and the distress that bring these children to harm. [1] [6]
Feeding is far more than swallowing. It is a developmental skill that matures from the suckle of the newborn through the purees of weaning to the chewed solids and cup-drinking of the toddler, and it depends on intact anatomy, coordinated muscle, a functioning gut, an alert brain and a responsive feeder. A feeding assessment therefore covers intake and growth, oromotor skill, sensory tolerance, mealtime behaviour and swallow safety, because a child can be unsafe at the table for any one of these reasons, and the right intervention depends on which. [2] [8]
Classification
The most useful clinical way to hold paediatric dysphagia is by where in the swallow the failure occurs, because the site predicts the cause and the test. The oral preparatory and oral phases are voluntary, governed by sucking, chewing and moving the bolus back with the tongue; the pharyngeal phase is the split-second reflex that closes the airway and opens the oesophagus; and the oesophageal phase moves the bolus down to the stomach. Most aspiration happens in the pharyngeal phase, when the airway is not protected in time. [1] [2]
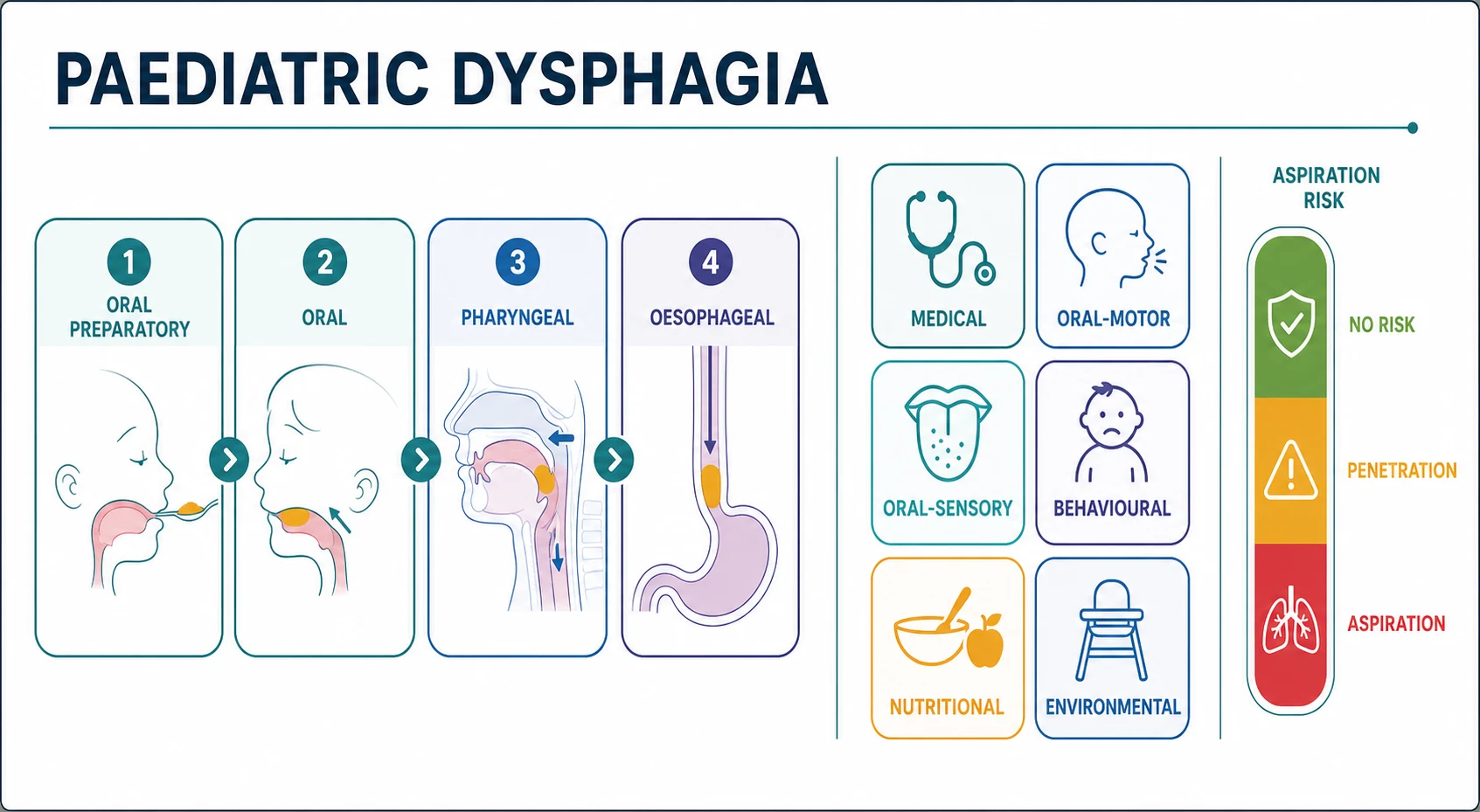
A second axis is the driver of the feeding difficulty, which a multidisciplinary team sorts into medical, oral-motor, oral-sensory, behavioural, nutritional and environmental causes. A child rarely has just one driver, and the severely neurologically impaired child may have oromotor weakness, oral sensory aversion, gastro-oesophageal reflux and an unsafe swallow all at once, so the team assesses each domain rather than assuming a single cause. [8] [2]
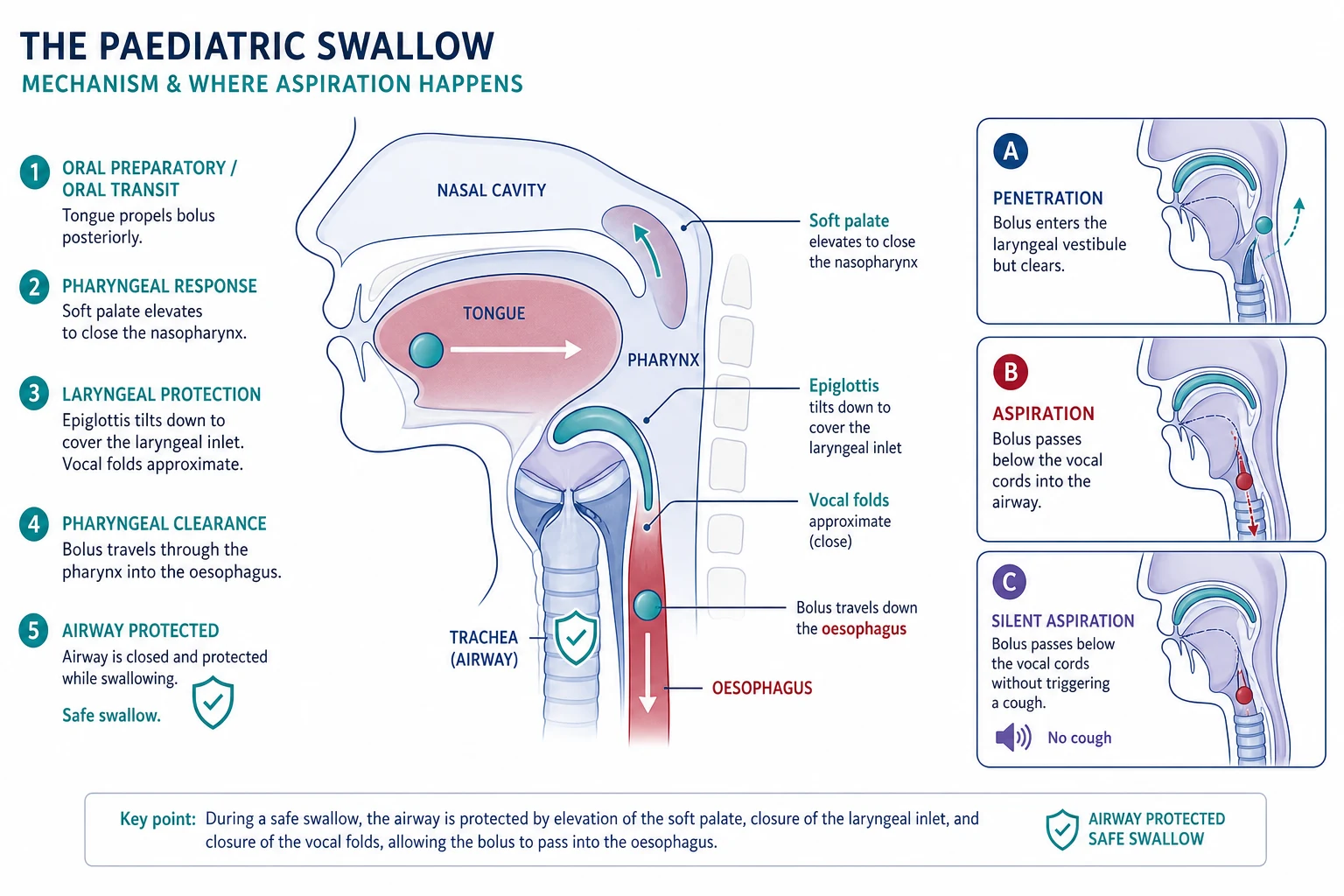
A third axis is the severity of airway compromise, graded by what happens to the bolus. Penetration is feed entering the laryngeal vestibule above the vocal cords but clearing again, aspiration is feed passing below the vocal cords into the trachea, and silent aspiration is aspiration that draws no cough. The penetration-aspiration scale scores the depth of bolus entry and whether it is cleared, and it is the standard way an instrumental study reports the danger of a given consistency. [1] [6]
[1] [2]Epidemiology & Risk Factors
Feeding and swallowing difficulty is among the commonest problems brought to a general paediatric clinic, and it is the single most frequent reason a child with neurodisability sees a speech-language therapist. Up to a quarter of typically developing children show some feeding difficulty in the preschool years, usually picky eating or oral sensory aversion that is benign, while serious dysphagia with aspiration clusters in defined high-risk groups. [2] [8]
The highest-risk child is the child with cerebral palsy, in whom oropharyngeal dysphagia is nearly universal in the severe forms. Across cerebral palsy cohorts roughly half to three-quarters of children have clinically significant feeding and swallowing difficulty, and those with the most severe motor impairment carry the greatest aspiration risk. The systematic evidence ties oropharyngeal dysphagia in cerebral palsy directly to malnutrition, faltering growth, recurrent chest infection and reduced survival, which is why every child with cerebral palsy deserves a structured feeding assessment. [7] [10]
The other high-risk groups share an immature, damaged or anatomically abnormal swallow. Premature and low-birthweight infants in the neonatal unit, children with airway anomalies such as laryngeal cleft, tracheo-oesophageal fistula and vocal cord palsy, those with syndromes such as Down syndrome and Pierre Robin sequence, and children with acquired brain injury or neuromuscular disease all carry a high burden of aspiration. The shared feature is either an uncoordinated pharyngeal reflex or an airway that cannot be protected. [1] [6]
Pathophysiology
A safe swallow is a precisely timed race between food moving backward and the airway shutting down. As the tongue strips the bolus toward the pharynx, the soft palate rises to seal the nose, the hyoid and larynx pull up and forward, the epiglottis tilts down, and the vocal folds approximate, so that for the instant the bolus passes, the laryngeal inlet is closed and the upper oesophageal sphincter opens. When any of these movements is slow, weak or discoordinated, feed spills into the laryngeal inlet and onward into the trachea. [1] [2]
In the neurologically impaired child the problem is usually a delayed, weak or discoordinated pharyngeal trigger. The bolus reaches the pharynx before the airway has closed, the swallow is fragmented, and residue pools in the valleculae and piriform sinuses, then trickles into the airway after the swallow. Because the sensory feedback that should trigger a protective cough is also blunted in these children, the aspiration draws no cough, and this silent aspiration is the mechanism behind the recurrent pneumonia and bronchiectasis that characterise chronic pulmonary aspiration. [6] [7]
In the anatomically abnormal child the problem is a structural gap between the airway and foodway. A laryngeal cleft leaves an opening between the posterior larynx and the oesophagus through which feed and saliva pass directly into the trachea, a tracheo-oesophageal fistula connects the two tubes, and a paralysed vocal cord cannot adduct to close the glottis. These children aspirate regardless of swallow skill, and the fix is surgical or structural rather than behavioural. [1] [6]
The downstream injury is repeated chemical and infective damage to the lung. Aspirated feed and acid inflame the bronchial tree, bacteria seed the damaged tissue, and the cycle of recurrent pneumonia, bronchiolar obliteration and bronchiectasis sets in over months to years. Malnutrition compounds the lung disease, because the child who cannot feed safely eats too little and burns too many calories with the work of breathing and of a prolonged, inefficient swallow. [6] [10]
Clinical Presentation
The child with oropharyngeal dysphagia usually presents through one of three doors. The first is the mealtime itself, with coughing, choking, gagging, spluttering or going blue during or just after feeds, nasal regurgitation, a wet or gurgly voice, and mealtimes that drag on beyond thirty to forty minutes. The second is the chest, with recurrent pneumonia, a chronic productive cough, wheeze that does not respond to asthma therapy, or bronchiectasis. The third is the growth chart, with faltering growth, weight loss or dehydration traced back to a child who simply cannot take enough in safely. [2] [6]
The infant adds a specific set of signs. Arching, irritability and crying with feeds, turning blue or stopping breathing during a bottle feed, poor latch and weak or incoordinated suck, and a child who tires before finishing the expected volume are the infant equivalents of an unsafe swallow. Premature infants in particular may demonstrate an immature suck-swallow-breathe pattern that desaturates them with each feed, and a feed that repeatedly drops the oxygen saturation is a feed that needs assessing. [12] [2]
The older neurologically impaired child often presents late, through the lung or the growth chart rather than the mealtime. The parents report mealtimes that last over an hour, food refusal, drooling and poor chewing, and the chart shows faltering weight, while the chest holds a recurrent or persistent problem that has been labelled asthma, recurrent viral wheeze or recurrent infection without anyone asking whether the child is aspirating. The recognition move is to ask about swallowing whenever a high-risk child has a chronic wet cough or unexplained faltering growth. [7] [10]
[6] [7]Differential Diagnosis
The differential depends on which door the child comes through. For the coughing, choking child the competitors are gastro-oesophageal reflux disease, eosinophilic oesophagitis, an upper airway cause such as laryngomalacia or tracheomalacia, a food allergy, and behavioural food refusal, and the discriminator is whether the symptoms are swallow-related and posture-related, which points toward the swallow, rather than purely post-prandial and reflux-like. [2] [6]
For the child with recurrent chest infections the differential is the whole list of chronic cough in children, including protracted bacterial bronchitis, post-viral cough, asthma, cystic fibrosis, an inhaled foreign body, primary ciliary dyskinesia, immunodeficiency and congenital lung malformation. The features that should pull aspiration to the top are a high-risk background such as cerebral palsy or an airway anomaly, a wet rather than dry cough, recurrent same-lobe pneumonia, and a clear temporal link between feeds and symptoms or a wet voice after drinking thin liquids. [6] [10]
For the faltering-growth child the differential spans inadequate intake, malabsorption, increased requirement and increased losses, and dysphagia sits firmly in the inadequate-intake arm. The clue to an unsafe or inefficient swallow is a child in a high-risk group whose intake is limited by mealtime distress, fatigue or prolonged feeding rather than by appetite or supply, and whose growth falters despite an apparently adequate offered volume. The must-not-miss trap is labelling the growth failure as neglect or behavioural when the child cannot swallow safely. [8] [7]
High-risk groups for aspiration — 'NEURO-AIRWAY'
Clinical & Bedside Assessment
Assessment begins with the growth chart and the mealtime history. Plot the weight, height and head circumference, ask exactly what and how much the child eats and drinks, how long a meal takes, and whether the child coughs, chokes, gags, goes blue, or has a wet voice during or after feeds. Ask about nasal regurgitation, food refusal, drooling, pocketing of food, and any chest symptoms, and establish the background of prematurity, cerebral palsy, airway surgery or syndrome. [2] [7]
The oromotor and clinical feeding evaluation is the core bedside skill, usually led by the speech-language therapist. It inspects the oral structures and tone, watches the child take age-appropriate consistencies, and looks for the signs of an unsafe swallow such as coughing, a delayed pharyngeal trigger, a wet voice, multiple swallows per bolus, and residue. It is the screening test that decides whether an instrumental study is needed and which consistencies are most dangerous. [3] [2]
The limitation the examiner expects you to name is that the bedside evaluation cannot reliably detect aspiration, and especially silent aspiration. A systematic review of the clinical feeding evaluation found it has limited and variable accuracy for detecting aspiration in children, because it cannot see the bolus in the pharynx and cannot register aspiration that draws no cough. A reassuring bedside evaluation therefore never closes the question in a high-risk child, and the instrumental study is the arbiter. [3] [1]
Examination extends to the systems that travel with dysphagia. Look for the stigmata of cerebral palsy, the airway noise of stridor, the chest signs of consolidation or bronchiectasis, the nutritional signs of wasting, drooling and poor dentition, and the tone and posture that will guide positioning and feeding technique. The examination frames the whole multidisciplinary plan, because posture, tone, reflux, chest status and growth all change what is safe to feed and how. [7] [8]
Investigations
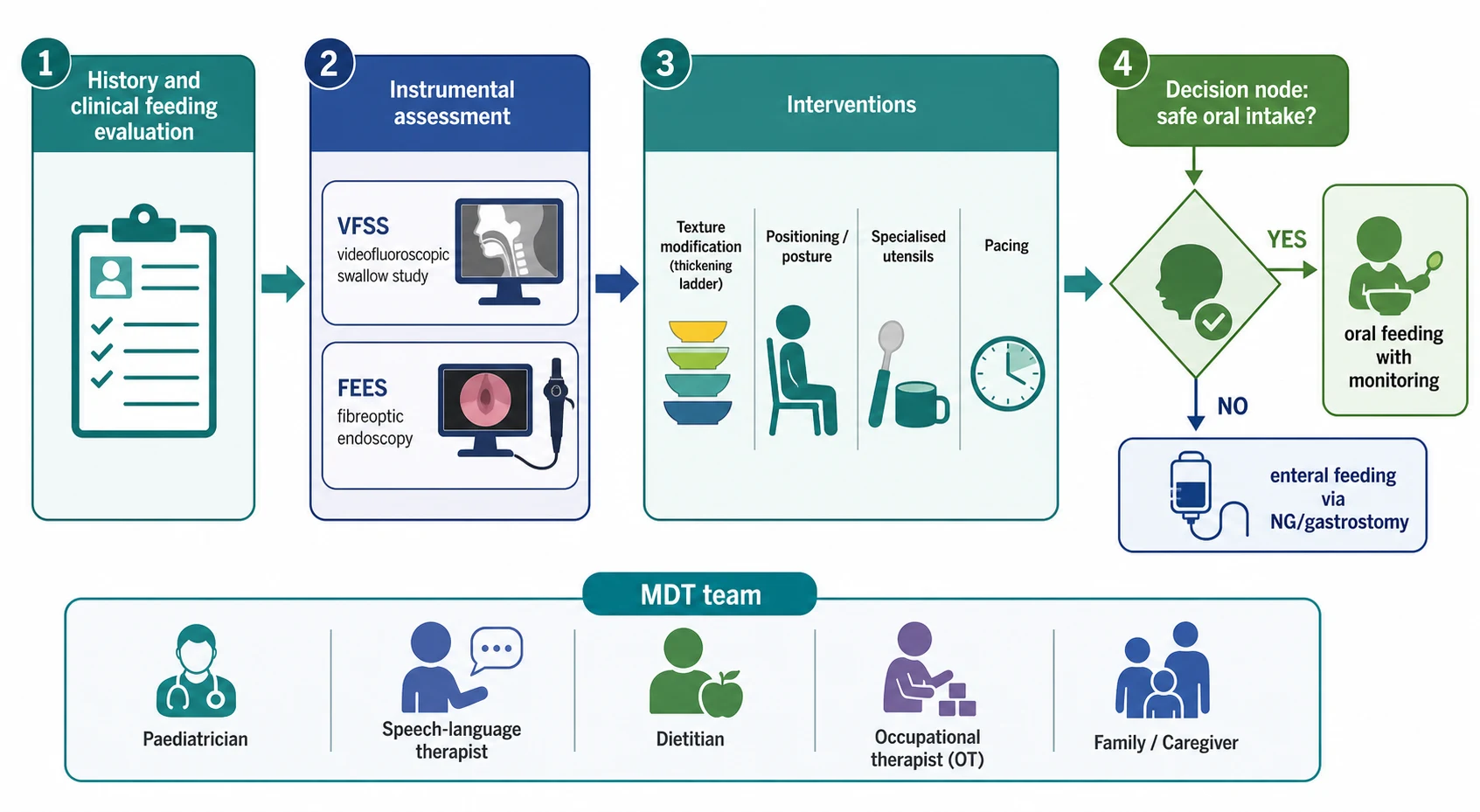
Investigation rests on two instrumental tests that see what the bedside cannot, and the choice between them depends on the question. The videofluoroscopic swallow study, sometimes called a modified barium swallow, is the gold standard for the oral and pharyngeal phases. It images the child swallowing barium of several consistencies under X-ray in real time, shows the timing and coordination of the swallow, and directly visualises penetration, aspiration and residue, including aspiration that is clinically silent. [1] [2]
The fibreoptic endoscopic evaluation of swallowing, known as FEES, passes a thin flexible scope through the nose to view the pharynx and larynx before and after the swallow. It shows the anatomy, the pooling of residue, penetration and aspiration, and it can be done at the bedside including in the neonatal unit, repeated readily, and used to test real food without barium. Its limitation is the white-out during the swallow itself, so it cannot see the moment of bolus transit through the pharynx, and it cannot assess the oral phase. [4] [5]
Both tests are safe in experienced paediatric hands, and FEES in particular has been shown to be well tolerated across the age spectrum from premature infants to adolescents, with a low complication rate over decades of use. The two are complementary rather than rivals, and many centres use the videofluoroscopic study to assess the dynamic swallow and FEES to assess anatomy, secretion management and residue, especially in the child who cannot travel to radiology. [4] [5]
Adjunct investigations address the company dysphagia keeps. A chest X-ray and, where indicated, a chest computed tomography look for aspiration-related consolidation and bronchiectasis. Reflux is assessed clinically and, when needed, with pH or impedance studies, because reflux compounds aspiration and may itself be treated. A flexible laryngoscopy or bronchoscopy defines structural causes such as a laryngeal cleft, vocal cord palsy or a recurrent tracheo-oesophageal fistula, and nutritional bloods stage the deficit that the unsafe swallow has produced. [1] [6]
VFSS or FEES — how to choose
Choose the videofluoroscopic swallow study when the question is about the dynamics of the swallow itself, because it shows the oral and pharyngeal phases in real time and is the most sensitive test for aspiration during the swallow. Choose FEES when the question is about anatomy, secretion management and residue, when the child cannot be moved to radiology, or when repeat bedside testing of real food is needed, including in the neonatal unit. The two are complementary, and a combined or sequential approach is common in complex children. Neither test replaces the other, and both depend on an experienced paediatric swallowing team to interpret. [4] [11] [12]
Management — Resuscitation
Most feeding assessment is elective, but a small number of children present acutely and need the feed stopped and the airway protected first. An infant who chokes, desaturates, becomes apnoeic or turns blue during a feed has an acutely unsafe swallow, and the immediate action is to pause oral feeds, maintain the airway and oxygenation, and secure hydration and nutrition by another route while the swallow is assessed. Suction the airway if feed or secretions have pooled, and treat any aspiration event with supportive care. [6] [2]
The child who aspirates and develops pneumonia needs the pneumonia treated as well as the feed made safe. Assess the work of breathing, give oxygen and respiratory support as needed, and treat the infection with antibiotics guided by severity and local policy, recognising that aspiration pneumonia favours the dependent lobes. The pivotal step is to stop the ongoing aspiration, which means pausing or modifying oral feeding until an instrumental swallow study defines what is safe, because treating the pneumonia without fixing the swallow guarantees recurrence. [6] [10]
The severely malnourished child who presents through faltering growth needs safe nutrition established without delay. Where the swallow is acutely unsafe, begin fluid and nutrition via a nasogastric tube while the assessment proceeds, and watch for refeeding risk if the malnutrition is severe. The resuscitation phase is a bridge to the instrumental study and the definitive multidisciplinary feeding plan, and its goal is to stabilise the airway, the chest and the hydration while the swallow is worked out. [8] [1]
Immediate management of the child with an acutely unsafe swallow
Stop oral feeding and protect the airway; suction pooled feed and secretions
Give oxygen and respiratory support for any aspiration event or pneumonia
Secure hydration and nutrition by nasogastric tube while the swallow is assessed
Treat aspiration pneumonia with antibiotics guided by severity and local policy
Address reflux if it is compounding the aspiration
Arrange an instrumental swallow study to define which consistencies, if any, are safe
Plan the definitive multidisciplinary feeding and airway-protection strategy
Management — Definitive & Stepwise
The definitive plan is built by a multidisciplinary team around the child and family. The paediatrician coordinates the medical care and the investigations, the speech-language therapist leads the swallow assessment and the texture and feeding technique, the dietitian secures the nutrition and growth, the occupational therapist addresses posture, seating and utensils, the physiotherapist manages tone and chest clearance, and the family carries the plan at every meal. No single discipline owns the problem, because the unsafe swallow, the tone, the reflux, the nutrition and the mealtime behaviour all interact. [1] [8]
When aspiration is confirmed, the first lever is to modify what the child swallows. Thickened liquids flow more slowly and give a delayed pharyngeal reflex more time to close the airway, so many children who aspirate thin liquids can drink safely once the liquid is thickened, while pureed or soft solids are safer than mixed or hard textures for the child with poor chewing. The texture ladder is standardised by the International Dysphagia Diet Standardisation Initiative, which grades liquids and foods from level zero thin through to level seven regular, so that the safe consistency is prescribed precisely and reproducibly. [1] [2]
The second lever is to change how the child is fed. Upright positioning, head and trunk support, chin-tuck or head-neutral posture, a controlled pace with small volumes, and specialised bottles, teats, cups and utensils all reduce the risk that the bolus outruns the airway closure. The speech-language therapist and occupational therapist tailor these to the individual child, and a carefully positioned, paced feed can convert an unsafe swallow into a safe one for selected consistencies. [2] [7]
When the swallow cannot be made safe for enough intake, enteral feeding secures nutrition while protecting the lung. A nasogastric tube is the short-term option, and a gastrostomy is the long-term option for the child who will need non-oral feeding for months or years, placed in concert with reflux control when reflux is contributing. The decision is individualised, balances quality of life and lung protection, and should preserve some safe oral feeding for pleasure where any consistency is safe, because complete oral removal carries its own developmental and emotional cost. [8] [1]
[1] [2]Specific Subtypes & Scenarios
The child with cerebral palsy is the central scenario, because dysphagia is common, often silent, and tightly linked to survival. Every child with cerebral palsy should have a structured feeding and swallowing assessment, and the severity is usefully captured by the Eating and Drinking Ability Classification System, a five-level scale that grades how safely and efficiently a child eats and drinks in everyday life. A validation study confirmed that the higher levels of this scale track closely with aspiration risk, so it is both a communication tool and a triage instrument. [9] [10]
The premature infant in the neonatal unit is the second scenario. Preterm infants must coordinate suck, swallow and breathe, and an immature or discoordinated pattern causes desaturation, bradycardia and aspiration with feeds. A bedside clinical evaluation, increasingly supplemented by fibreoptic endoscopic evaluation of swallowing, defines the safe feeding strategy and the rate of progression, and the goal is to advance oral feeding as the infant matures while protecting the airway. [12] [4]
The child with a structural airway anomaly is the third. A laryngeal cleft, a repaired tracheo-oesophageal fistula, a vocal cord palsy after cardiac or airway surgery, and laryngomalacia all aspirate through a structural gap rather than a discoordinated swallow, and the evaluation combines the instrumental swallow study with airway endoscopy. The fix is surgical or structural where possible, with feeding and airway protection held in the meantime. [1] [6]
The child who aspirates saliva is the fourth. Some neurologically impaired children cannot manage their own secretions and chronically aspirate saliva regardless of feeding, presenting with a constant wet cough and recurrent pneumonia. The management ladder runs from positioning, suction and medications that reduce secretory flow, through to surgical options such as salivary duct ligation or botulinum toxin to the salivary glands, and the multidisciplinary team weighs lung protection against comfort and quality of life. [6] [7]
Across Australia, New Zealand and the United Kingdom, feeding and swallowing assessment is delivered by a multidisciplinary team built around the speech-language therapist or speech pathologist, the dietitian and the paediatrician, with videofluoroscopic swallow studies and fibreoptic endoscopic evaluation of swallowing available through regional paediatric and ear-nose-throat services. The International Dysphagia Diet Standardisation Initiative texture framework is the shared language for prescribed consistencies. In many low-resource, rural and remote settings the instrumental tests are distant or unavailable, the burden of untreated aspiration falls on Indigenous and disadvantaged children, and telehealth-supported shared care with the local team is what makes safe feeding plans achievable far from a specialist centre. [1] [8]
Complications & Pitfalls
The complications of untreated dysphagia run through the lung, the growth chart and the family. Recurrent aspiration pneumonia is the acute threat, and the chronic consequences are bronchiolitis obliterans and bronchiectasis that permanently damage the child's lungs. Malnutrition and faltering growth follow from an inefficient, unsafe or prolonged swallow that delivers too few calories, and dehydration compounds the picture when thin liquids are unsafe. Mealtime distress, food refusal and family exhaustion carry their own developmental and emotional cost. [6] [10]
The diagnostic pitfalls are the failures the examiner rewards for naming. The first is relying on the bedside evaluation to exclude aspiration, which it cannot do, because silent aspiration is invisible at the bedside. The second is attributing the chronic wet cough or recurrent pneumonia of a neurologically impaired child to asthma or recurrent infection without ever asking about the swallow. The third is labelling faltering growth in a high-risk child as behavioural or neglect while the child silently aspirates. [3] [7]
The management pitfalls cut both ways. Over-treating a child whose swallow can be made safe with thickening and positioning, by moving straight to a gastrostomy, imposes an unnecessary and stigmatising intervention, while under-treating a child who aspirates silently, by reassuring the family on a normal bedside evaluation, condemns the lung to progressive damage. The safeguard is always the instrumental study in the high-risk or unclear child, and a team that balances lung protection against quality of life. [1] [8]
Prognosis & Disposition
The prognosis depends on the underlying cause, the severity of the dysphagia, and how early and how completely the airway is protected. The typically developing infant with an immature suck-swallow-breathe pattern matures out of the problem as the brain develops, and the child with a surgically correctable structural lesion improves once the anatomy is fixed. The child with severe, permanent neurodisability carries a chronic or progressive problem in which the goal shifts from cure to protecting the lung, securing nutrition and preserving as much safe oral feeding and quality of life as possible. [1] [10]
In cerebral palsy the feeding and swallowing outcome tracks the motor severity. Children with milder motor impairment often manage safe oral feeding with minor modification, while those with the most severe impairment have a high risk of aspiration, malnutrition and chest disease, and dysphagia and malnutrition are recognised contributors to reduced survival in the most severely affected. Early gastrostomy in carefully selected severely affected children improves nutrition and carer quality of life and reduces mealtime distress. [7] [8]
Disposition follows the cause and the risk. The straightforward case is managed jointly by the general paediatrician, the speech-language therapist and the dietitian in the community or outpatient clinic, with instrumental studies as needed and the general practitioner supporting ongoing care. The child with an acutely unsafe swallow, aspiration pneumonia, severe malnutrition or a complex structural or neurological problem is managed in a tertiary centre with paediatric gastroenterology, ear-nose-throat and respiratory services, and a planned transition of care through childhood and adolescence. [1] [8]
Special Populations
The child with cerebral palsy is the first special population, because the burden of dysphagia is greatest here. A structured feeding assessment, the Eating and Drinking Ability Classification System grade, the instrumental swallow study when the bedside is uncertain, and a multidisciplinary plan for texture, posture, nutrition and reflux are the standard of care, and early gastrostomy is considered when oral intake cannot be made safe or sufficient. [7] [9]
The premature and technology-dependent infant is the second. Coordinated suck-swallow-breathe matures with postmenstrual age, and a structured oral feeding pathway, often using fibreoptic evaluation in the neonatal unit, advances feeding while protecting the airway. The technology-dependent child with a tracheostomy or long-term ventilation adds anatomical and secretory challenges that demand a specialist airway and feeding team. [12] [4]
The Indigenous, remote and migrant child is the third. In many settings the burden of untreated neurodisability and aspiration falls unevenly on these children, the instrumental tests and the specialist teams are distant, and the cost and logistics of modified feeding and enteral nutrition are harder to sustain. Culturally safe shared-care pathways, telehealth support for the local team, and attention to the practicalities of feeding equipment and supplies are what make a safe feeding plan achievable for families far from a specialist centre. [1] [8]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric dysphagia is built on a body of specialist reviews and systematic studies rather than a single guideline cycle. The Lawlor and Choi review frames the diagnosis and management of paediatric dysphagia for the generalist, and the Duffy review sets out the swallow phases, the clinical presentation and the approach to the child with a feeding difficulty, together giving the clinician the structural backbone of the topic. [1] [2]
The instrumental-assessment evidence is the part examiners probe. The Calvo systematic review established that the clinical feeding evaluation has limited accuracy for detecting aspiration in children and cannot be relied on to exclude it, which is the rationale for the instrumental study. The Miller papers on fibreoptic endoscopic evaluation of swallowing describe the protocol, safety and clinical efficacy across twenty-five years and across the age spectrum, and the Pazinatto and Reynolds studies confirm the role of FEES in children with suspected dysphagia and in the neonatal unit. [3] [4] [5] [11] [12]
The cerebral-palsy evidence defines the highest-risk group. The Erasmus clinical-practice paper and the Arvedson review set out the swallowing problems and the feeding approach in cerebral palsy, and the Calderone systematic review ties oropharyngeal dysphagia to its nutritional and health consequences. The Bykova validation study confirms that the Eating and Drinking Ability Classification System detects aspiration risk, giving the clinician a practical triage tool. The Tutor and Gosa review of dysphagia and aspiration in children frames the pulmonary consequences that bring these children to harm. [7] [8] [9] [10] [6]
Regional practice differs chiefly in access to the instrumental tests and the specialist teams rather than in the diagnostic principle. In well-resourced settings the videofluoroscopic swallow study and FEES are routinely available and the International Dysphagia Diet Standardisation Initiative texture ladder is the shared language, while in many low-resource, rural and remote settings the tests are distant, the burden of untreated aspiration is higher, and telehealth-supported shared care is the practical answer. [1] [8]
Exam Pearls
Paediatric dysphagia assessment — 'SWALLOW'
References
- [1]Lawlor CM; Choi S Diagnosis and Management of Pediatric Dysphagia: A Review. JAMA Otolaryngol Head Neck Surg, 2020.PMID 31774493
- [2]Duffy KL Dysphagia in Children. Curr Probl Pediatr Adolesc Health Care, 2018.PMID 29571543
- [3]Calvo I; Conway A; Henriques F Diagnostic accuracy of the clinical feeding evaluation in detecting aspiration in children: a systematic review. Dev Med Child Neurol, 2016.PMID 26862075
- [4]Miller CK; Willging JP Fiberoptic Endoscopic Evaluation of Swallowing in Infants and Children: Protocol, Safety, and Clinical Efficacy: 25 Years of Experience. Ann Otol Rhinol Laryngol, 2020.PMID 31845586
- [5]Miller CK; Schroeder JW Jr; Langmore S Fiberoptic Endoscopic Evaluation of Swallowing Across the Age Spectrum. Am J Speech Lang Pathol, 2020.PMID 32650653
- [6]Tutor JD; Gosa MM Dysphagia and aspiration in children. Pediatr Pulmonol, 2012.PMID 22009835
- [7]Erasmus CE; van Hulst K; Rotteveel JJ Clinical practice: swallowing problems in cerebral palsy. Eur J Pediatr, 2012.PMID 21932013
- [8]Arvedson JC Feeding children with cerebral palsy and swallowing difficulties. Eur J Clin Nutr, 2013.PMID 24301008
- [9]Bykova KM; Frank U; Girolami GL Eating and Drinking Ability Classification System to detect aspiration risk in children with cerebral palsy: a validation study. Eur J Pediatr, 2023.PMID 37184644
- [10]Calderone A; Militi D; Cardile D Swallowing disorders in cerebral palsy: a systematic review of oropharyngeal Dysphagia, nutritional impact, and health risks. Ital J Pediatr, 2025.PMID 39985076
- [11]Pazinatto DB; Brandão MAB; Costa FLP Role of fiberoptic endoscopic evaluation of swallowing (FEES) in children with suspected dysphagia. J Pediatr (Rio J), 2024.PMID 38679061
- [12]Reynolds J; Carroll S; Sturdivant C Fiberoptic Endoscopic Evaluation of Swallowing: A Multidisciplinary Alternative for Assessment of Infants With Dysphagia in the Neonatal Intensive Care Unit. Adv Neonatal Care, 2016.PMID 26709466