Paeds · gastroenterology-hepatology-and-nutrition
Food protein-induced enterocolitis and enteropathy
Also known as Food protein-induced enterocolitis syndrome · FPIES · Food protein-induced enterocolitis and enteropathy · Food protein-induced enteropathy · Non-IgE-mediated food allergy with delayed vomiting · Dietary protein enterocolitis
Fellowship guide to food protein-induced enterocolitis syndrome (FPIES): a non-IgE-mediated food allergy of infancy in which a trigger protein produces delayed, repetitive vomiting one to four hours after ingestion with lethargy, pallor and watery diarrhoea, the 2017 international consensus diagnostic criteria that separate acute from chronic FPIES, the distinction from sepsis and surgical abdomen, the absence of any validated diagnostic test and the central role of supervised oral food challenge, the resuscitation of the acute reaction with intravenous fluids and ondansetron, and the avoidance diet, the action plan and the natural history of tolerance that most children outgrow.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Food protein-induced enterocolitis syndrome is the non-IgE-mediated food allergy that every paediatric trainee must be able to pull out of the differential of a suddenly pale, vomiting infant. The child looks septic, the septic screen is negative, and the whole story unlocks the moment you realise the collapse is timed one to four hours after a specific food. That delayed, repetitive vomiting with lethargy, pallor and watery diarrhoea, in the absence of any hive, wheeze or swelling, is the signature, and recognising it changes the child from a case of recurrent sepsis into a case of a avoidable food trigger. [1]
The mechanism is cell-mediated rather than antibody-mediated, which is why skin-prick tests and specific immunoglobulin E are unhelpful and why the reaction is delayed rather than immediate. There is no validated laboratory test, so the diagnosis is clinical, built on the consensus criteria, and confirmed by resolution on elimination and recurrence on a medically supervised oral food challenge. The companion syndrome is food protein-induced enteropathy, a chronic, malabsorptive pattern with diarrhoea, vomiting and faltering growth from ongoing ingestion, which sits on the same non-IgE spectrum and resolves on removal of the trigger. [1] [2]
Classification
The most useful way to classify food protein-induced enterocolitis syndrome is by the tempo of the reaction to the trigger food, because the two patterns demand different recognition and a different workup. Acute FPIES appears with intermittent ingestion, as on first exposure to a new food: a delayed, dramatic reaction one to four hours later. Chronic FPIES appears with regular, ongoing ingestion, as in a young infant fed cow's-milk or soy formula around the clock: a smouldering illness of intermittent vomiting, diarrhoea and poor weight gain that clears only when the food is withdrawn. [1]
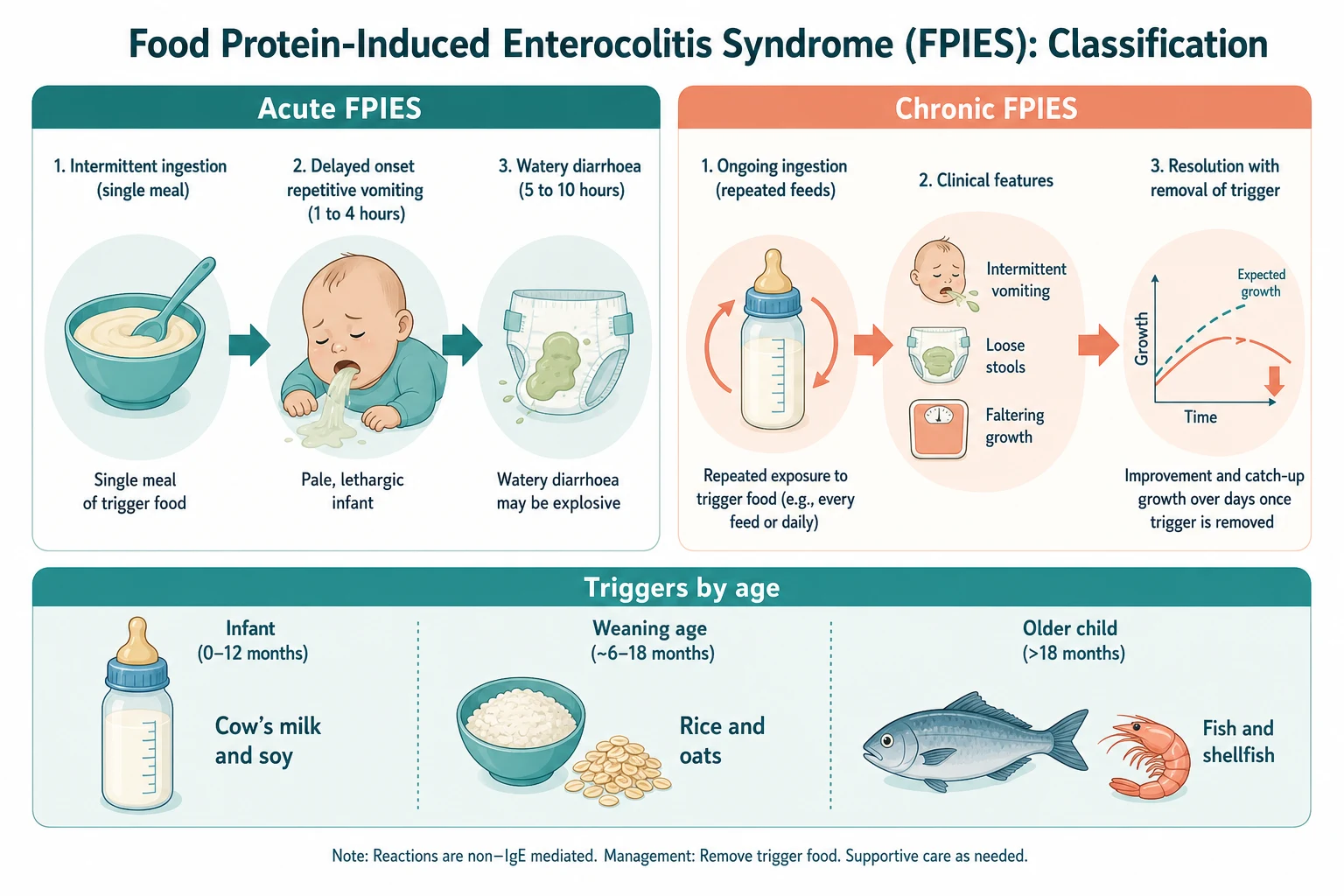
The trigger food usually tracks the child's age and the feeding milestone. Cow's milk and soy dominate in the formula-fed young infant, rice and oats dominate among the first cereals at weaning, and fish and shellfish become the common culprits in older children, with regional variation — fish is a leading trigger in Mediterranean and some Asian cohorts. Breast-milk-triggered FPIES is described but rare, so an exclusively breastfed infant who is thriving should prompt a search for another cause before FPIES is blamed on the breast milk. [1] [7] [9]
[1]Epidemiology & Risk Factors
Food protein-induced enterocolitis syndrome is among the commonest of the non-IgE-mediated food allergies of infancy, yet it remains under-recognised. Reported incidence from a large Israeli population cohort placed cow's-milk FPIES at about 0.34 per cent of infants, with overall figures higher once all triggers are counted, and most cases declare themselves within the first year of life. The under-recognition is itself a risk factor for harm: surveys show limited knowledge among general paediatricians, so children are repeatedly investigated for sepsis or surgery before the dietary pattern is identified. [11] [1]
The risk profile points to an atopic, early-life disease. Most children present in infancy, often at the introduction of formula or the first solids; there is a slight male predominance; and affected children frequently have a personal or family history of atopy. Cow's milk and soy are the leading triggers in infants, with a meaningful minority of cow's-milk-FPIES children also reacting to soy, which shapes the choice of a substitute feed. Solid-food FPIES tends to present slightly later, at weaning, and grains such as rice and oats are over-represented among the cereal triggers. [1] [7]
Pathophysiology
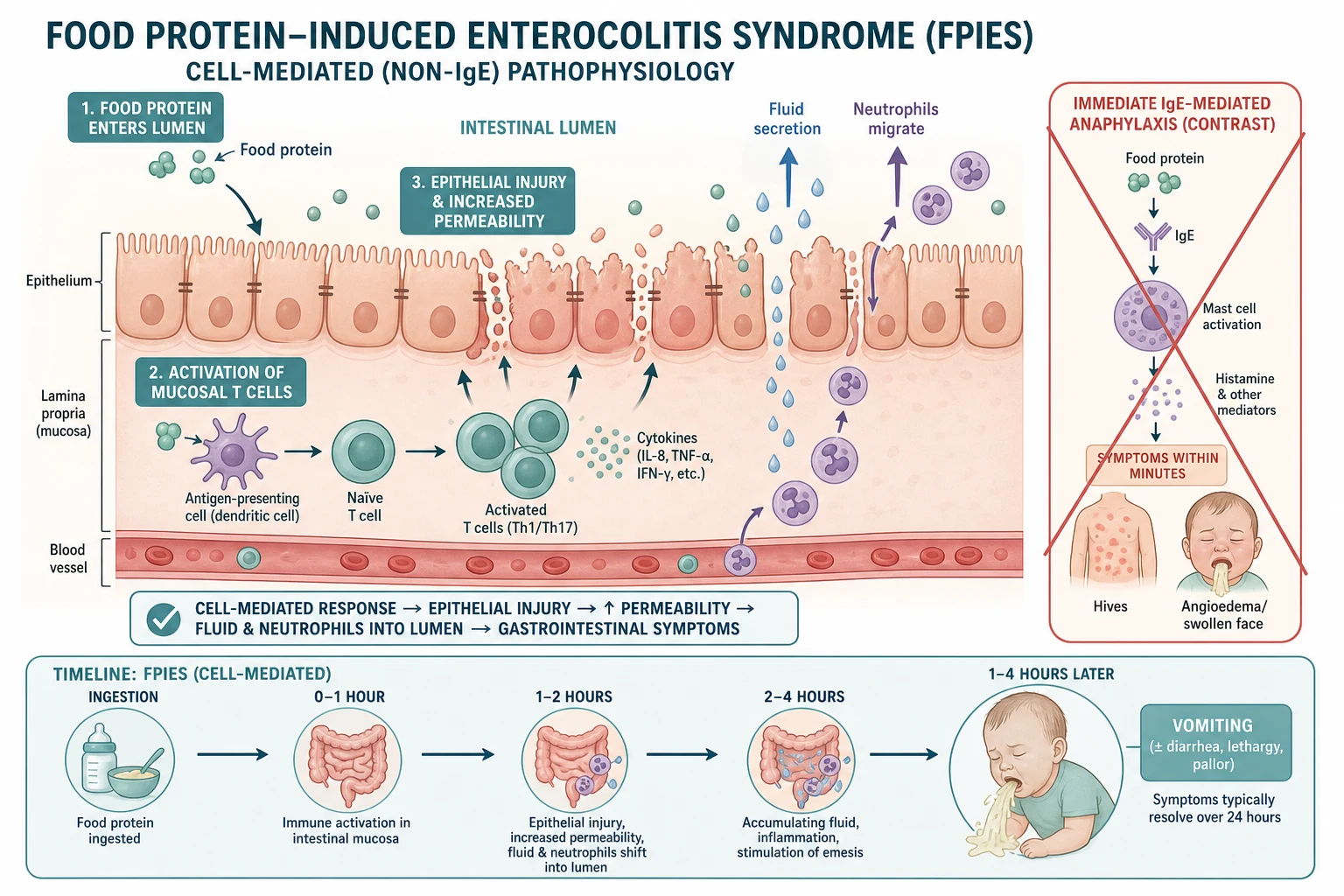
The mechanism of food protein-induced enterocolitis syndrome is a cell-mediated, delayed hypersensitivity of the gut, quite different from the immediate, antibody-driven release of histamine that produces anaphylaxis. When the trigger protein reaches the intestinal mucosa it drives a T-cell-led inflammatory response that injures the epithelium, increases mucosal permeability, and shifts fluid and inflammatory cells into the gut lumen. The delay between ingestion and symptoms reflects the time this cell-mediated injury and fluid shift take to develop, which is why the vomiting appears at one to four hours rather than within minutes. [1] [3]
The downstream effect is a sudden loss of fluid and electrolyte into the gut and a systemic inflammatory response that produces the striking pallor, lethargy and floppiness of an acute reaction. In severe cases this progresses to dehydration, metabolic acidosis, hypotension and, occasionally, methaemoglobinaemia. The chronic form reflects sustained mucosal injury from ongoing ingestion, producing malabsorption, protein loss and the smouldering diarrhoea and faltering growth that mimic a primary enteropathy. The pathophysiology explains both the clinical picture and the management: stop the trigger to stop the injury, and resuscitate the volume and acid-base deficit in the acute reaction. [3] [8]
Clinical Presentation
The classic acute presentation is the infant who becomes pale, floppy and lethargic with repetitive vomiting one to four hours after eating a food. The vomiting is profuse and repetitive, the child looks grey and unwell rather than merely miserable, and many parents describe a frightening change in their child's colour and tone. Watery diarrhoea, sometimes with blood, follows some hours later, and the episode settles over twelve to twenty-four hours once the trigger has passed through the gut. Between episodes the child is usually entirely well, which is why a single dramatic reaction is so easily labelled a one-off infection. [1] [2]
The chronic presentation is subtler and is the trap in the outpatient clinic. The young infant on cow's-milk or soy formula has intermittent vomiting, loose or bloody stools and poor weight gain, and may be worked up for recurrent sepsis, cow's-milk protein allergy of the IgE type, or a primary malabsorptive disorder. The clue is that the symptoms are locked to ongoing ingestion and resolve within a few days of changing the feed. Solid-food FPIES presents at weaning with the same delayed vomiting pattern after rice cereal, oats or another new food, and a careful diet-and-symptom diary often exposes the link that the history alone missed. [3] [7]
The severity spectrum is wide, and this is what makes FPIES a genuine emergency at one end. Most reactions settle with oral or intravenous rehydration, but a minority progress to hypovolaemic shock, profound metabolic acidosis and, rarely, methaemoglobinaemia. Reassuringly, anaphylaxis with cardiovascular collapse is uncommon, but the acutely pale, lethargic, vomiting infant must always be assessed for dehydration and shock, because the cell-mediated fluid loss can be large. [1] [8]
Differential Diagnosis
The differential diagnosis is built around the two presentations. For an acute, delayed vomiting collapse in an infant, the dangerous mimics are sepsis and an acute surgical abdomen, and the task is to avoid both anchoring on sepsis and missing a surgical emergency. Sterile, recurrent, food-timed episodes with negative cultures point to FPIES, but a first episode still warrants a septic screen and careful surgical assessment, because intussusception, appendicitis and, in the very young or premature infant, necrotising enterocolitis can look identical. [1] [11]
For the chronic, faltering-growth infant, the differential is the chronic diarrhoea and malabsorption list. Cow's-milk protein allergy of the IgE or mixed type can coexist and confuse, but its classic picture includes eczema, immediate reactions and blood with mucus in an otherwise well breastfed infant, rather than delayed pallid vomiting. Coeliac disease, cystic fibrosis with pancreatic insufficiency, congenital enteropathies and persistent post-enteritis diarrhoea all produce chronic diarrhoea with faltering growth and are excluded by their own targeted workup. The discriminating feature for FPIES is resolution on elimination of a single trigger with recurrence on reintroduction. [3] [6]
Differential of an acute delayed vomiting collapse in infancy — 'SAFE VOMIT'
Clinical & Bedside Assessment
Assessment begins with the trigger and the timing, because the diagnosis lives in the history rather than the bedside or the laboratory. Establish exactly what the child ate, when the symptoms began, and how long after the food the vomiting started: the one-to-four-hour window is the signature of acute FPIES. Quantify the reaction — repetitive vomiting, pallor, lethargy or floppiness, diarrhoea, and any change in colour or consciousness — and ask whether the same food has produced the same pattern before, because stereotyped recurrence is the strongest single clue. A three-day diet-and-symptom diary is invaluable for the chronic or weaning presentation, where the link between a new cereal and the reaction is easily missed. [1] [5]
Examination in the acute reaction is a resuscitation assessment first and a search for clues second. Assess the airway, breathing and circulation, grade the dehydration, look for pallor, reduced perfusion and altered tone, and identify shock early. Then look for what FPIES is not: the absence of urticaria, angio-oedema, stridor and wheeze argues against immediate IgE-mediated allergy and supports the cell-mediated picture. Between episodes the child is usually well and growing, so a thriving inter-episode infant is consistent with FPIES, whereas persistent faltering growth between reactions points to the chronic form or an alternative diagnosis. [8] [1]
Investigations
There is no validated diagnostic test for food protein-induced enterocolitis syndrome, and the single most important point for the exam is that skin-prick tests and specific immunoglobulin E are negative in classic disease and cannot be used to confirm or to exclude it. The diagnosis is clinical, built on the 2017 international consensus criteria, and where confirmation is needed it rests on resolution of symptoms when the trigger is removed and recurrence on a medically supervised oral food challenge. Ordering a battery of allergy panels not only wastes resources but misleads, because a positive immunoglobulin E to the same food represents sensitisation, not the mechanism of the reaction. [1] [6]
Investigations during an acute episode support resuscitation and exclude mimics rather than confirm the diagnosis. A full blood count may show a neutrophil leukocytosis, which is itself a minor consensus criterion; a blood gas may show metabolic acidosis; and electrolytes, glucose and renal function guide fluid therapy. Stool studies, inflammatory markers and cultures help exclude infectious enterocolitis and surgical causes. Rare but important findings in severe reactions include methaemoglobinaemia and endoscopic evidence of mucosal oedema, friability and colitis with eosinophils or neutrophils, but endoscopy is not routine and is reserved for the atypical or chronic case where the diagnosis is in doubt. [1] [8]
Management — Resuscitation
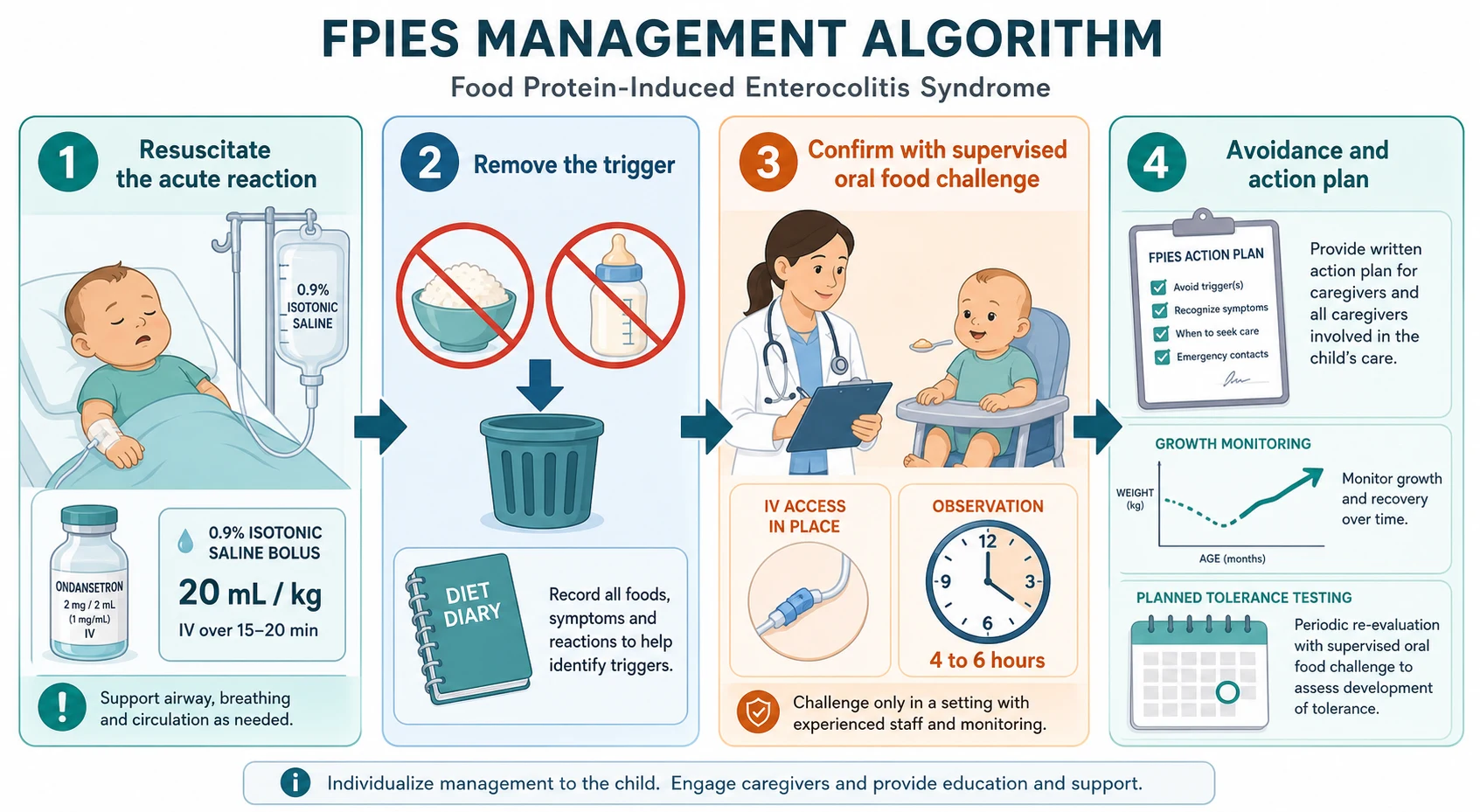
The acute reaction is managed as a volume-depleting, acidotic collapse, and the first move is to resuscitate the child as for any shocked infant. Assess the airway, breathing and circulation, grade the dehydration, secure intravenous access, and give repeated boluses of twenty millilitres per kilogramme of isotonic crystalloid until perfusion is restored. Correct the electrolyte and acid-base disturbance, check the glucose, and treat any methaemoglobinaemia. For the child with ongoing repetitive vomiting, intravenous ondansetron is used to control the vomiting, and a single dose of a systemic corticosteroid such as methylprednisolone is often given to blunt the cell-mediated response, although the evidence for steroids is limited. [1] [8]
Mild reactions can be managed with oral rehydration solution under observation, provided the child is drinking, not shocked and not continuing to vomit. The principle is to match the severity: a well, drinking child who has stopped vomiting can be observed, whereas a pale, lethargic, persistently vomiting child needs intravenous fluids and monitoring. Antidiarrhoeal agents have no role. Once the acute episode has settled, the child is admitted to an avoidance and prevention pathway, because the long-term management is what prevents the next reaction. [1] [3]
Intravenous fluid resuscitation for an acute FPIES reaction
Loading dose
20 mL/kg boluses of isotonic crystalloid (0.9% saline), repeated to restore perfusion
Maintenance dose
ongoing intravenous fluids guided by continuing losses, perfusion, electrolytes and acid-base status
Immediate management of the acute FPIES reaction
Assess airway, breathing and circulation; grade dehydration and look for shock, pallor and altered tone
Secure intravenous access and send a blood gas, full blood count, electrolytes, glucose and renal function
Give repeated 20 mL/kg boluses of isotonic crystalloid until perfusion is restored
Give intravenous ondansetron for ongoing vomiting and consider a single dose of methylprednisolone
Correct electrolyte and acid-base disturbance; treat methaemoglobinaemia if present
Observe until the child is rehydrated, no longer vomiting and clinically stable
Plan the avoidance pathway and provide a written FPIES action plan before discharge
Management — Definitive & Stepwise
Definitive management is the strict avoidance of the trigger food, delivered with dietetic support and a written action plan, and it is the single most effective intervention available. The family must know how to read food labels, avoid the trigger and its cross-reactive relatives, and manage a reaction; in Australia and New Zealand this is delivered through an Australasian Society of Clinical Immunology and Allergy action plan for FPIES. For the formula-fed infant with cow's-milk FPIES, an extensively hydrolysed formula is first-line, escalating to an amino-acid formula if symptoms persist, and soy is used with caution in young infants because of the meaningful cross-reactivity with cow's milk. [1] [6]
Confirmation and tolerance testing both rely on the medically supervised oral food challenge, which is the gold standard for both diagnosis and reassessment. The challenge is performed in a setting able to manage severe vomiting and dehydration, with intravenous access or the immediate capacity to establish it, graded dosing of the suspect food over about thirty minutes, and observation for four to six hours afterwards. When the challenge is negative, the food can be introduced at home under guidance; when it is positive, the typical delayed vomiting confirms the diagnosis and the child continues on the avoidance pathway. [1] [8]
[1] [6]The oral food challenge — the detail examiners probe
The oral food challenge for FPIES is not the same as for IgE-mediated allergy: it is done for a delayed reaction, so observation extends over four to six hours rather than the usual hour, and the setting must be able to resuscitate a child with severe vomiting and dehydration rather than anaphylaxis. Intravenous access is established or immediately available, the food is given in graded doses, and a positive challenge reproduces the delayed, repetitive vomiting with pallor and lethargy. A negative challenge permits home introduction of the food, while a positive challenge confirms FPIES and continues avoidance until the next assessment. Recent work has questioned whether the traditional conservative protein limit is always necessary, but the standard remains a cautious, supervised, monitored challenge. [1] [12]
Specific Subtypes & Scenarios
Cow's-milk and soy FPIES is the infant scenario an examiner most often tests, because it presents in the first months of life with the formula-fed young child. The chronic pattern dominates here: intermittent vomiting, diarrhoea and faltering growth on regular cow's-milk or soy formula, with the diagnosis emerging when the feed is changed and the symptoms clear over several days. A first acute reaction can also occur on a new formula. Because a meaningful proportion of cow's-milk-FPIES infants also react to soy, an extensively hydrolysed formula is preferred over soy as the substitute, with an amino-acid formula in reserve. [1] [4]
Solid-food FPIES is the weaning scenario. Rice and oats are over-represented among the cereal triggers, and the presentation is the delayed, pallid vomiting one to four hours after a new food, often at the first or second exposure. The history and a diet diary are diagnostic, and management is avoidance of the trigger, with attention to grains that may cross-react. Fish and shellfish FPIES presents more often in older children and carries a regional pattern — fish is a leading trigger in Mediterranean and some Asian cohorts — and it tends to persist longer than cow's-milk FPIES. [7] [9]
Chronic FPIES with faltering growth is the scenario that tests whether the candidate can move from the acute collapse to the outpatient malabsorption picture. The young infant on regular trigger feeding has ongoing mucosal injury, malabsorption and protein loss, and the growth chart drifts downward. Removal of the trigger resolves the diarrhoea and vomiting and allows catch-up growth, which both confirms the diagnosis and reverses the harm. The key is to include FPIES in the differential of every faltering infant on a cow's-milk or soy formula. [3] [6]
In Australia and Aotearoa New Zealand, the Australasian Society of Clinical Immunology and Allergy provides a dedicated guide and a written action plan for FPIES, which standardise the avoidance advice, the substitute-feed choice and the acute-reaction response across primary care and emergency departments; the large Australian cohort of Mehr and colleagues anchors local epidemiology. In the United Kingdom, the Ludman cohort and the standard allergy pathways drive similar practice. Globally, the 2017 international consensus criteria are the common diagnostic standard, with regional variation in triggers — fish and shellfish are more prominent in Mediterranean and Asian populations — and in access to supervised oral food challenge, which is the limiting step in many services. [5] [10] [1]
Complications & Pitfalls
The dominant acute complication is fluid and acid-base loss: dehydration, metabolic acidosis, electrolyte disturbance and, in severe reactions, hypovolaemic shock and methaemoglobinaemia. These are preventable with early intravenous fluid resuscitation, and the child who arrives pale, lethargic and acidotic after a trigger food should be resuscitated first and investigated second. Chronic FPIES adds malabsorption and faltering growth from ongoing mucosal injury, which reverse on removal of the trigger. The psychosocial burden on the family — repeated emergency visits, anxiety about feeding and the restrictive diet — is substantial and is best addressed with a clear action plan and dietetic support. [1] [8]
The pitfalls are mainly diagnostic. The first is anchoring on sepsis: a recurring, food-timed, culture-negative collapse should prompt the dietary question rather than another septic screen. The second is over-investigating with IgE panels: skin-prick tests and specific immunoglobulin E are negative in classic FPIES and cannot confirm it, and a positive result represents sensitisation, not the mechanism. The third is confusing FPIES with cow's-milk protein allergy of the IgE or mixed type, which has a different picture and a different management pathway. The fourth is the mirror error of reassuring a faltering infant as simply colicky or intolerant when chronic FPIES is quietly driving the poor weight gain. [1] [11]
Prognosis & Disposition
The prognosis is generally excellent, because most children outgrow food protein-induced enterocolitis syndrome, but the timeline depends on the trigger. Cow's-milk and soy FPIES resolve earliest, with tolerance developing in the majority within the first few years of life, whereas solid-food FPIES and fish or shellfish FPIES tend to persist longer. Resolution is assessed at intervals by a medically supervised oral food challenge, and a negative challenge permits home introduction of the food. Between challenges, the child thrives on the avoidance diet. [4] [5]
Disposition follows the presentation and the certainty of diagnosis. The acute reaction needs emergency assessment and resuscitation, with admission for the dehydrated or acidotic child. The child with suspected or confirmed FPIES is referred to a paediatric allergist or a paediatrician with an interest in food allergy for diagnostic confirmation by supervised oral food challenge, dietetic support for the avoidance diet, and a planned programme of tolerance testing. The well child with a confident clinical diagnosis and a clear action plan can be managed in shared care between primary care, the general paediatrician and the allergy service. [1] [6]
Special Populations
The young infant is the first special population, because FPIES is predominantly a disease of the first year and the chronic form can cause faltering growth before the trigger is identified. A formula-fed young infant with intermittent vomiting, diarrhoea and poor weight gain should prompt consideration of chronic cow's-milk or soy FPIES, with an extensively hydrolysed formula as the substitute. In the premature or very young infant, an acute reaction can mimic necrotising enterocolitis, and the two must be distinguished because both can present with pallor, lethargy, vomiting and acidosis; the food timing and the sterile, recurrent pattern point to FPIES. [1] [3]
The child in a disadvantaged or remote setting is the second. Access to a supervised oral food challenge and to specialist allergy and dietetic services is uneven, and in rural, remote, Indigenous, migrant and refugee families the burden of repeated emergency visits and a restrictive diet falls hardest on those with the least support. Shared-care pathways, telehealth allergy support and a clear written action plan are the tools that allow local teams to manage FPIES safely where specialist access is limited. [5] [1]
The older child with persistent solid-food or fish FPIES is the third. These children carry the allergy into the school years, where self-management, school staff education, label reading and an up-to-date action plan become central. Fish and shellfish FPIES in particular can persist into adolescence and adulthood in some populations, so tolerance testing is continued at intervals rather than assumed. [9] [7]
Evidence, Guidelines & Regional Differences
The evidence base is anchored on the 2017 international consensus guidelines of Nowak-Węgrzyn and the Adverse Reactions to Foods Committee, which set the diagnostic criteria and the management framework that current practice follows. The consensus formalises the major criterion of delayed vomiting one to four hours after ingestion without classic IgE features, the set of minor criteria, the distinction between acute and chronic FPIES, the role of the supervised oral food challenge, and the resuscitation of the acute reaction with intravenous fluids, ondansetron and corticosteroid. [1]
The cohort studies define the clinical features and the natural history. Sicherer's original clinical-features report established the delayed vomiting and pallor pattern, and the later case series of Sicherer, the ten-year cohort of Caubet and the sixteen-year Australian cohort of Mehr described the trigger profile, the severity spectrum and the resolution rates that underpin the prognosis. The solid-food report of Nowak-Węgrzyn established rice and oats as leading cereal triggers, the Italian fish-and-shellfish cohort of Miceli Sopo defined a regional trigger pattern, and the United Kingdom cohort of Ludman described referral characteristics and diagnostic delay. [2] [4] [5] [7] [9] [10]
[1] [6]The recognition gap and the contemporary debates round out the picture. The survey of Feuille and colleagues showed limited knowledge of FPIES among general paediatricians, which is the root cause of the sepsis-mimic diagnostic delay, and the Leonard review and the recent beyond-the-guidelines appraisal of Shah and colleagues summarise the consensus and its open questions, including the optimal challenge dosing and the role of ondansetron in the acute reaction. Across all settings the strategy is uniform: recognise the delayed food-timed pattern, resuscitate the acute reaction, remove the trigger, confirm with supervised challenge, and test tolerance at intervals. [11] [6] [12]
Exam Pearls
The 2017 consensus criteria — 'VOMIT PLUS'
References
- [1]Nowak-Węgrzyn A; Chehade M; Groetch ME; Spergel JM; Wood RA; Allen K International consensus guidelines for the diagnosis and management of food protein-induced enterocolitis syndrome: Executive summary-Workgroup Report of the Adverse Reactions to Foods Committee, American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol, 2017.PMID 28167094
- [2]Sicherer SH; Eigenmann PA; Sampson HA Clinical features of food protein-induced enterocolitis syndrome. J Pediatr, 1998.PMID 9709708
- [3]Sicherer SH Food protein-induced enterocolitis syndrome: case presentations and management lessons. J Allergy Clin Immunol, 2005.PMID 15637562
- [4]Caubet JC; Ford LS; Sickles L; Järvinen KM; Sicherer SH; Sampson HA; Nowak-Węgrzyn A Clinical features and resolution of food protein-induced enterocolitis syndrome: 10-year experience. J Allergy Clin Immunol, 2014.PMID 24880634
- [5]Mehr S; Kakakios A; Frith K; Kemp AS Food protein-induced enterocolitis syndrome: 16-year experience. Pediatrics, 2009.PMID 19188266
- [6]Leonard SA; Pecora V; Fiocchi AG; Nowak-Węgrzyn A Food protein-induced enterocolitis syndrome: a review of the new guidelines. World Allergy Organ J, 2018.PMID 29441147
- [7]Nowak-Węgrzyn A; Sampson HA; Wood RA; Sicherer SH Food protein-induced enterocolitis syndrome caused by solid food proteins. Pediatrics, 2003.PMID 12671120
- [8]Feuille E; Nowak-Węgrzyn A Medical Algorithms: Recognizing and treating food protein-induced enterocolitis syndrome. Allergy, 2019.PMID 31070799
- [9]Miceli Sopo S; Monaco S; Badina L; Barni S; Toscano A; Tripodi S; Meglio P Food protein-induced enterocolitis syndrome caused by fish and/or shellfish in Italy. Pediatr Allergy Immunol, 2015.PMID 26287446
- [10]Ludman S; Harmon M; Whiting D; du Toit G Clinical presentation and referral characteristics of food protein-induced enterocolitis syndrome in the United Kingdom. Ann Allergy Asthma Immunol, 2014.PMID 25065570
- [11]Feuille E; Menon NR; Huang F; Nowak-Węgrzyn A Knowledge of food protein-induced enterocolitis syndrome among general pediatricians. Ann Allergy Asthma Immunol, 2017.PMID 28890023
- [12]Shah S; Grohman R; Nowak-Węgrzyn A Food protein-induced enterocolitis syndrome (FPIES): Beyond the guidelines. J Food Allergy, 2023.PMID 39022754