Paeds · gastroenterology-hepatology-and-nutrition
Formula feeding and complementary feeding
Also known as Infant formula feeding · Bottle feeding · Complementary feeding · Weaning · Introduction of solids · Complementary foods
Fellowship guide to formula feeding and complementary feeding: the classification and compositional standard for infant formula, why cow's milk is unsuitable before twelve months, the developmental and physiological reasons solids begin at around six months, safe formula preparation and the approximate 150 mL per kg daily volume, the texture and allergen ladder from iron-rich first foods to family meals, the never-before-twelve-months hazards of honey, added salt and sugar, whole cow's milk and choking foods, and the ESPGHAN, WHO, NHMRC and AAP regional guidance informed by the LEAP and EAT early-allergen trials.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
When breast milk is not available, not enough, or not chosen, the question for the clinician is deceptively simple: what do you feed the baby, how do you make it safely, and when do you start real food? Infant formula is a manufactured feed designed to be nutritionally complete for the first months of life, regulated to a strict compositional standard so that a healthy infant can grow on it alone [7]. Complementary feeding — the older term is weaning — is the progressive introduction of foods other than milk from around six months, building toward a child who eats the family diet by their first birthday [1].
The two halves of this topic share one goal: to supply enough energy, protein, iron, zinc and micronutrients for rapid infant growth without overwhelming an immature gut and kidney. Breastfeeding remains the reference standard and is recommended as the sole milk source for the first six months, continuing alongside foods to twelve months and beyond [3][4]. Where formula is used, the principles of choice, volume, preparation and progression are the everyday work of a general paediatrician, and the source of most parental questions in the first year [1][2].
Classification
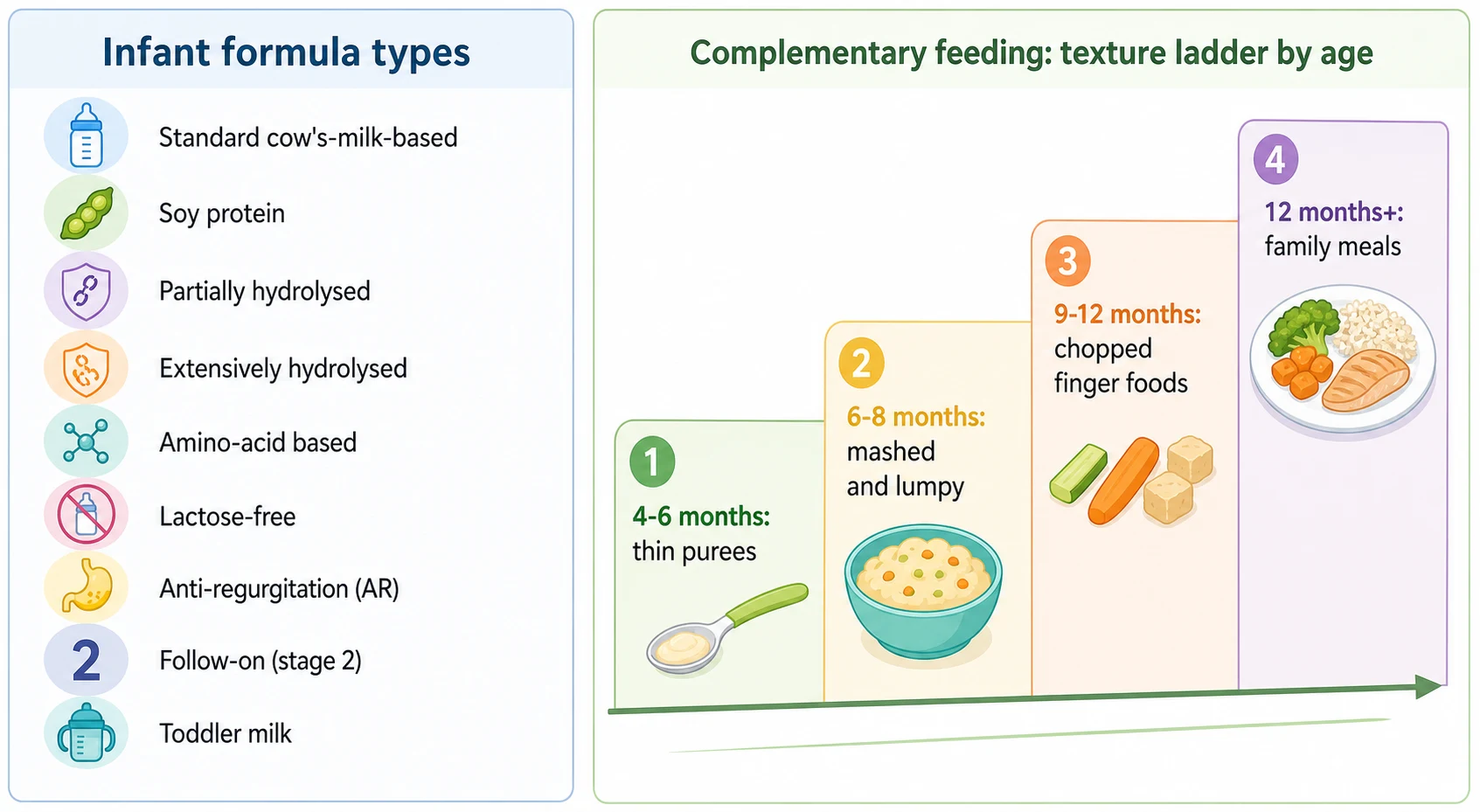
Infant formulas are grouped by their protein source and their intended use. The workhorse for almost every healthy infant is a standard first infant formula based on modified cow's milk, nutritionally complete from birth to twelve months [7]. Specialised formulas are reserved for specific medical indications rather than parental preference, and choosing the wrong formula — or switching without reason — is a common source of confusion and cost [1][2].
- Modified cow's-milk protein (whey-dominant for young infants)
- Nutritionally complete from birth to 12 months
- First choice for a healthy formula-fed infant
- No need to change brand or 'step up' to follow-on
- Plant protein isolate, lactose-free
- Not a first-line formula; use only for galactosaemia or strict vegan preference
- Do not use for cow's-milk allergy prevention or 'colic'
- Contains phytoestrogens — avoid in preterm infants
- Cow's-milk protein broken into smaller peptides
- Marketed as 'gentle' or hypoallergenic
- Not appropriate for confirmed cow's-milk protein allergy
- No convincing benefit for allergy prevention over standard formula
- Cow's-milk protein fully broken down to peptides
- First-line specialised formula for cow's-milk protein allergy in most infants
- Examples: casein-based or whey-based eHF
- 100 percent free amino acids, non-allergenic
- For severe or multiple allergy, eosinophilic disease, or when eHF fails
- Also used in food protein-induced enterocolitis syndrome
- Cow's-milk protein with glucose polymers replacing lactose
- For post-gastroenteritis lactose intolerance or galactosaemia (soy also an option)
- Not needed for healthy infants or routine reflux
- Thickened with starch or carob bean gum to reduce posseting
- For troublesome regurgitation only after a review of feeding technique
- Never use a home-thickened feed or added cereal in a bottle
- Marketed from 6 months (follow-on) and from 12 months (toddler)
- Not necessary: a first infant formula or whole cow's milk (after 12 months) suffices
- Higher protein and sugar; poor value; driven by marketing
The single most important distinction in clinic is between a marketing category and a clinical one. Follow-on and toddler milks exist largely to extend brand loyalty and permit advertising in jurisdictions that restrict infant-formula promotion; they are not a nutritional requirement, and a first infant formula continues to be appropriate right through the first year [1][2]. Whole cow's milk becomes the main drink only after twelve months, never before [1].
Epidemiology & Risk Factors
In high-income settings a large share of infants receive some formula in the first six months, whether by choice, perceived insufficient milk, return to work, or a medical reason [4]. Formula feeding is more common among infants of younger mothers, smokers, those with earlier return to work, and families who received inconsistent feeding advice or free formula samples [4]. None of these is a judgement; each is a risk factor for suboptimal feeding practice that a clinician can address with clear, non-stigmatising guidance.
The timing of starting solids varies widely despite consistent guidance. Solids introduced before four completed months are commonest where families believe solids help sleep, reflux or weight gain, and where commercial baby food is marketed for young infants [8]. Late introduction after six months is seen with anxiety about allergy or choking, or with cultural beliefs about weaning age. Both ends of the spectrum carry risks: early solids raise the chance of later obesity and replace milk intake, while late solids risk iron deficiency and delay the developmental and allergen-tolerance benefits of timely weaning [1][8][10].
Pathophysiology
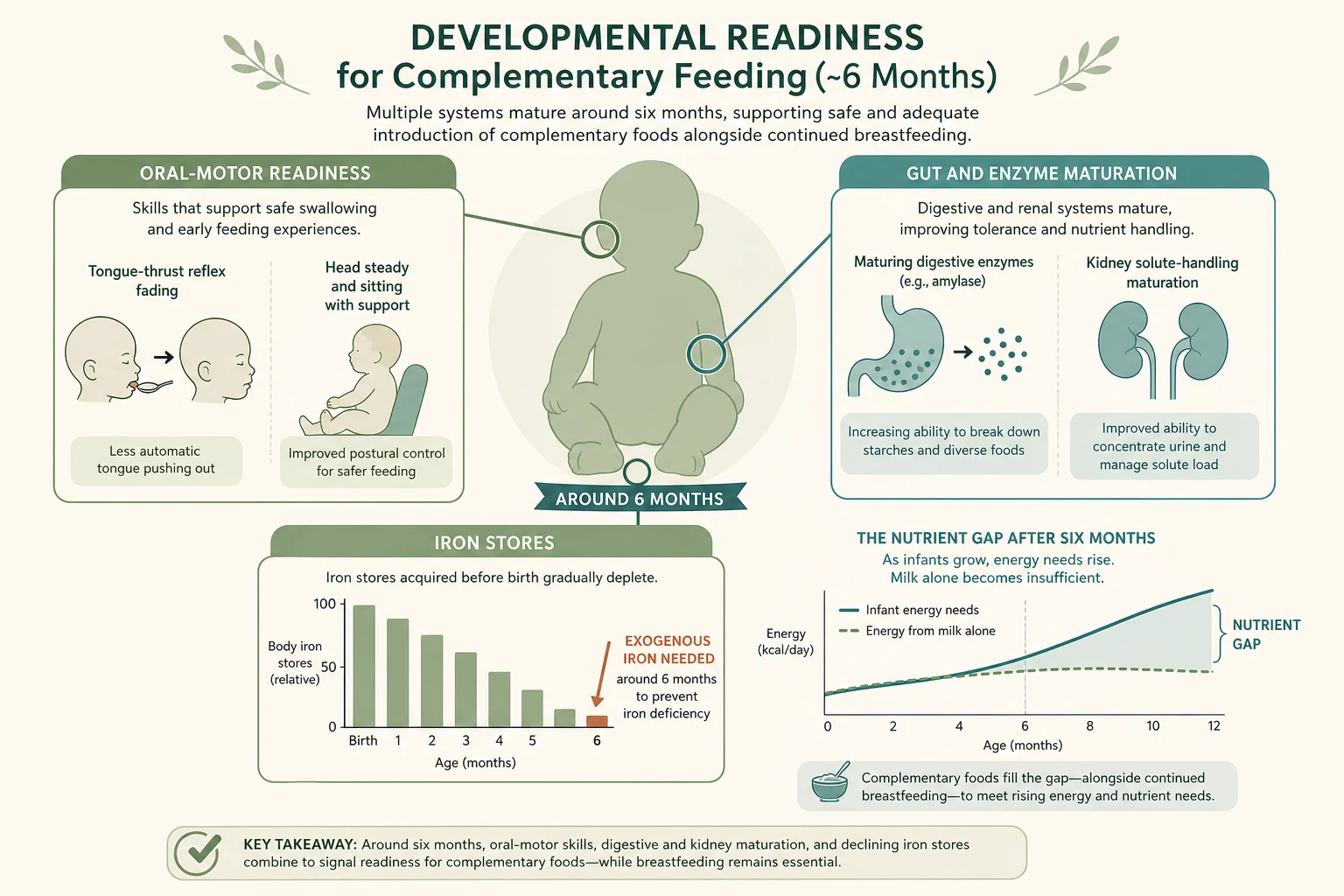
The timing of complementary feeding is not arbitrary. Around six months, four changes converge to make solids both possible and necessary. The infant gains head control and trunk stability, sits with support, and the extrusion (tongue-thrust) reflex fades so a spoon can move food backwards rather than pushing it out [1]. The gut and pancreas mature enough to digest starches and complex foods, and the kidney handles the higher solute load of mixed foods [2].
At the same time a genuine nutrient gap appears. Iron stores laid down in late pregnancy are largely depleted by six months, so the infant needs a dietary iron source — which is why iron-rich foods are recommended as first foods [1][10]. Milk alone, whether breast or formula, becomes insufficient for total energy and micronutrient needs as growth and activity accelerate [1]. Before four months these systems are not ready, which is why solids before four months are discouraged; after about six months the iron deficit and missed developmental window become the concern [2][3].
The protein story is the second physiological lesson. Infant formula contains more protein per litre than breast milk, and the protein content falls and self-regulates in breast milk over the feed. Higher protein intake in infancy has been linked to faster early weight gain and a higher body mass index in childhood, which is why modern formulas are formulated toward the lower end of the permitted range — the so-called "early protein hypothesis" of later obesity [9].
The third mechanism underpins modern allergy advice. The old dogma of delaying allergenic foods to prevent allergy was overturned by trials showing that early, regular exposure to allergens such as peanut during infancy induces tolerance rather than sensitisation [5][6]. This is why complementary feeding now deliberately includes common allergens from around six months rather than excluding them.
Clinical Presentation
A well-fed infant gains weight steadily along their centiles, is settled between feeds, has at least four to six wet nappies a day, and develops normally. The signs that an infant is ready to begin solids are the developmental milestones that confirm the gut and oral-motor physiology above: good head control, sitting with support, watching and reaching for food, and the loss of the tongue-thrust reflex, usually appearing around six months [1][2].
Problems declare themselves through growth and feeding behaviour. Faltering growth — weight crossing centiles downward — is the cardinal sign of inadequate intake, malabsorption, or underlying disease, and is the single most important thing to detect in a feeding review [10]. Persistent vomiting, blood or mucus in the stool, eczema, irritability with feeds, or chronic diarrhoea point toward cow's-milk protein allergy or another food intolerance rather than simple feeding variation [1]. Pallor and lethargy in a milk-fed older infant raise iron deficiency anaemia, which is commonest in infants given whole cow's milk too early or weaned onto low-iron foods [10].
Differential Diagnosis
Most "feeding problems" in the first year are normal variation that needs reassurance and a feeding review rather than investigation [1]. Mild spilling (posseting), a slow start with textures, and intermittent food refusal are expected; the task is to separate these from the pathological patterns that change management [1].
- Urticaria, vomiting, angio-oedema within minutes to 2 hours of cow's-milk exposure
- Positive skin-prick or specific IgE
- Switch to extensively hydrolysed or amino-acid formula; refer to allergy
- Delayed symptoms: blood-mucus stool, eczema, reflux, persistent diarrhoea
- Skin-prick and IgE negative; diagnosis by elimination and rechallenge
- Trial extensively hydrolysed formula; may need amino-acid formula
- Effortless regurgitation in a thriving, happy infant
- Reassure; review feeding technique and volume
- Reserve thickeners or AR formula for troublesome reflux in a thriving infant
- Watery, acidic diarrhoea with perianal excoriation
- Usually transient post-gastroenteritis in infants
- Lactose-free formula for a short defined trial
- Weight crossing centiles down; few wet nappies
- Check prepared formula dilution, volume, and feeding frequency
- Often a preparation or intake error rather than disease
- Pallor, lethargy, pallor in an older milk-fed infant
- Early whole cow's milk or low-iron weaning diet
- Confirm with ferritin; treat with iron and dietary review
The discriminator that matters most is the weight centile. A thriving, settled infant with posseting almost never needs a formula change, whereas a child crossing centiles downward or with red-flag symptoms needs the underlying cause found, not a trial of a different formula [10].
Clinical & Bedside Assessment
A feeding review begins with a precise history of what the infant actually receives. Ask the exact formula brand and stage, how it is prepared (the number of scoops and the volume of water), the total daily volume, the number and timing of feeds, and any solids already introduced with their textures and allergens [1]. The commonest preparation error — adding extra scoops or packing them tightly — is found only by asking how the family makes up a feed, and it is the cause of both hypernatraemic dehydration and faltering growth [7].
Examination centres on growth and hydration. Measure weight, length and head circumference on the same growth charts each visit, plot them, and look for centile crossing [4]. Assess hydration (mucous membranes, capillary refill, wet nappies), look for signs of allergy (eczema, perioral rash) and anaemia (pallor), and observe feeding — oral-motor coordination, swallowing, and whether the infant manages the offered texture [1]. Confirm the developmental milestones of feeding readiness: head control, supported sitting, and interest in food [2].
Investigations
Most formula-fed and weaning infants need no investigation; a careful history and growth review resolve the question. Investigations are reserved for the child with faltering growth, persistent symptoms, or signs of deficiency [1].
When iron deficiency is suspected — pallor, lethargy, or an infant weaned onto whole cow's milk or low-iron foods — a full blood count and ferritin confirm the diagnosis and guide treatment [10]. Suspected IgE-mediated cow's-milk protein allergy may warrant skin-prick testing or specific immunoglobulin E, ideally after referral, though non-IgE-mediated allergy has no reliable test and is diagnosed by elimination and supervised rechallenge [1]. A dietitian's nutritional analysis is itself an investigation when faltering growth or a restricted diet raises concern about adequate energy, iron, or micronutrient intake [10].
Management — Resuscitation
Feeding-related emergencies are uncommon but time-critical, and they almost always arise from an error in formula preparation or from a first allergen exposure. Over-concentrated formula (too much powder, too little water) drives hypernatraemia with irritability, seizures and dehydration; under-concentrated formula causes hyponatraemia, faltering growth and, rarely, water intoxication [7]. Recognise the dehydrated or encephalopathic infant, stop the incorrect feed, and treat the electrolyte disturbance with intravenous rehydration guided by measured sodium, not a standard formula [7].
A first exposure to a common allergen can trigger IgE-mediated anaphylaxis within minutes. The infant who develops urticaria, angio-oedema, wheeze, pallor or collapse after a new food needs intramuscular adrenaline by weight, airway and circulatory support, and observation for the biphasic reaction [5][6]. Honey exposure in an infant under twelve months is a separate, insidious emergency: Clostridium botulinum spores germinate in the immature gut to produce infant botulism with descending flaccid paralysis, poor feeding, weak cry and respiratory failure — a diagnosis to raise and confirm with stool toxin testing, with supportive ventilation as the mainstay [1].
Management — Definitive & Stepwise
Definitive management is preventive and educational, and it follows two parallel ladders — one for formula, one for solids — that run together from birth to the first birthday [1].
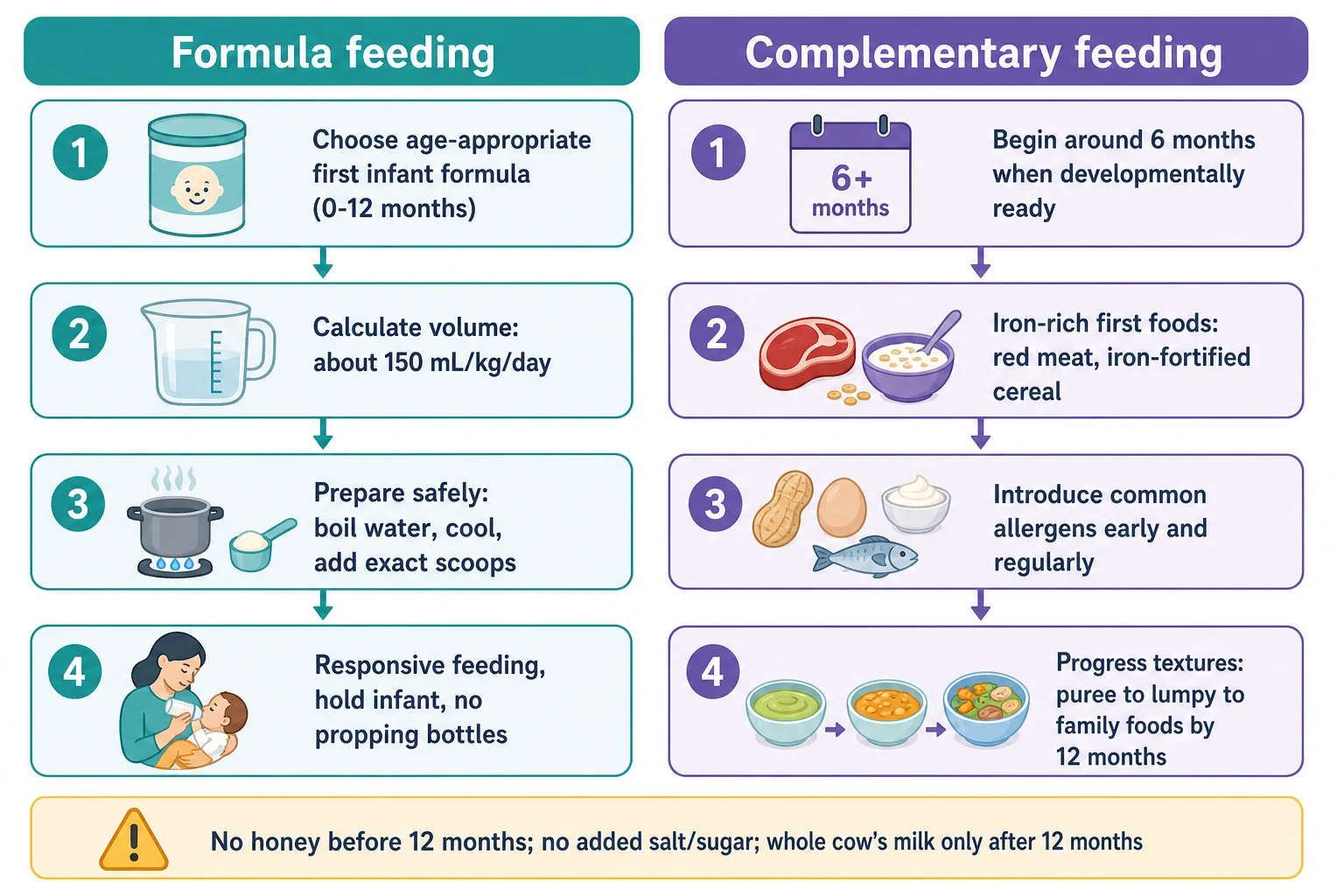
Safe formula feeding
Choose a standard first infant formula (stage 1) for a healthy infant from birth to 12 months; do not switch brands or step up to follow-on without reason.
Guide volume by appetite and growth — a working figure is about 150 mL per kg per day in early infancy, tapering as solids take over; never force a set amount.
Prepare each feed safely: boil fresh water and let it cool to no less than 70 degrees Celsius, add the exact number of level, unpacked scoops, and use or refrigerate immediately.
Feed responsively: hold the infant, keep the bottle horizontal to control flow, watch for fullness cues, and never prop a bottle or put the infant to bed with one.
The volume figure of about 150 mL per kg per day is a starting estimate for the early months, not a prescription; by around six months total milk intake often settles near 600 mL per day and falls as solids increase, and from twelve months a child needs roughly 400 to 600 mL of milk or dairy equivalents daily alongside food [1][7]. Safe preparation is the part that prevents harm: boiling and cooling water to at least 70 degrees Celsius kills any Cronobacter or Salmonella in powder, and exact scoop measurement prevents concentration errors [1][7].
The complementary feeding ladder
Begin at around six months, when the infant shows developmental readiness (head control, supported sitting, interest in food, reduced tongue thrust).
Offer iron-rich first foods: pureed red meat, lentils, beans, or iron-fortified infant cereal, since iron stores are low by six months.
Introduce common allergens — egg, peanut, tree nuts, dairy as food (not as the main milk), wheat, fish and shellfish — early and keep them in the diet regularly; do not delay them.
Progress texture quickly from smooth puree to mashed, lumpy and soft finger foods over weeks, so the infant chews rather than only swallows by around nine to twelve months.
Move toward family meals by twelve months: three meals plus snacks, eaten together, responsive to hunger and fullness, with milk as a drink rather than the main nutrient source.
The allergen ladder deserves emphasis because it is the part of modern advice that most contradicts what parents — and many clinicians — remember. The LEAP trial showed that early, regular peanut consumption in high-risk infants dramatically reduced peanut allergy, and the EAT trial supported the principle of early introduction in the general breast-fed population [5][6]. The practical message is to introduce allergens from around six months, one new food at a time in small amounts, and to keep them regularly in the diet rather than avoiding them [1].
Responsive feeding is the unifying principle across both ladders: feed the infant, not the clock or the bottle, and read the cues of hunger and fullness [1]. Practical guidance also covers cup use (introduce an open cup from around six months and phase out bottles by twelve months), family meals, and avoiding food as reward, bribe or comfort [1][2].
Specific Subtypes & Scenarios
The preterm or low-birth-weight infant needs particular care. Their iron stores are lower because most iron is transferred in the third trimester, so they often require iron supplementation and an earlier focus on iron-rich foods; their oral-motor maturation may lag their corrected age, so solids are usually started around four to six months corrected age, guided by readiness rather than chronology [1].
Infants with cow's-milk protein allergy are the largest group needing a specialised feeding plan. An extensively hydrolysed formula is first-line for most, with an amino-acid formula reserved for severe, multiple, or non-responding allergy [1]. Weaning proceeds as for any infant, with dairy introduced as a food only if tolerated and under allergy guidance; calcium from non-dairy sources must be ensured [1]. Galactosaemia mandates a lactose- and galactose-free feed such as a soy formula or a specialised amino-acid formula, since breast milk and standard formula are excluded [7].
Infants with reflux, constipation, or lactose intolerance during weaning are usually managed with feeding review and simple measures rather than formula change. AR formula has a role only for troublesome regurgitation in a thriving infant after technique is reviewed; constipation responds to fluids, fibre and fruit rather than formula switching; and transient post-infectious lactose intolerance may justify a short trial of a lactose-free formula [1][2].
Complications & Pitfalls
A baby who is made ill by their feed is usually ill because of a preparation mistake, and the harm is immediate. Over-concentration — too many scoops or too little water — causes hypernatraemic dehydration and seizures, while under-concentration causes faltering growth and hyponatraemia; both are traced to how the feed is made rather than to the formula itself [7]. Reusing bottles, storing made-up feeds too long, or using unboiled water risk infection with Cronobacter or Salmonella [7].
- Replaces milk and reduces intake
- Associated with later obesity
- Gut and oral-motor systems not ready
- Excludes breast milk benefits
- Iron deficiency as stores deplete
- Missed window for allergen tolerance
- Delayed oral-motor development
- Energy gap as milk insufficient
- Faster early weight gain
- Higher childhood BMI (early protein hypothesis)
- Modern formulas lower in protein to match breast milk
- Occult gastrointestinal blood loss
- Iron deficiency anaemia
- High renal solute load
- Low iron, vitamin C and essential fatty acids
The never-before-twelve-months hazards are the high-yield facts an examiner tests. Honey carries botulism risk [1]; whole cow's milk as a drink causes iron deficiency and stresses the kidney [1][10]; added salt risks hypernatraemia and strains the immature kidney; added sugar establishes a sweet preference and dental caries; and choking foods — whole grapes, nuts, hard lumps, popcorn, hotdog rounds — must be modified or avoided, with the infant always upright and supervised while eating [1][2].
Prognosis & Disposition
With appropriate formula feeding and timely complementary feeding, an infant grows along their centiles, develops normal oral-motor skills, and transitions smoothly to the family diet by twelve months [1]. Progress is monitored through routine growth and developmental checks, and most families need only consistent, confident advice at each visit. Faltering growth, persistent symptoms, or a complex feeding situation prompt referral.
Referral to a dietitian is appropriate for faltering growth, restricted or specialised diets, and parental anxiety about feeding [10]. A speech pathologist or feeding clinic is warranted for oral-motor difficulty, swallowing problems, or persistent food refusal beyond normal variation [1]. An allergy clinic is needed for confirmed or suspected IgE-mediated food allergy before allergen reintroduction [5][6]. The safety-net is clear: any infant losing weight, becoming dehydrated, or developing new red-flag symptoms returns promptly for review [1].
Special Populations
In low- and middle-income settings and food-insecure households, the risks shift toward infection from unsafe formula preparation and toward growth faltering from dilution to save money [3]. Here breastfeeding is protected even more strongly, and where formula is necessary, education on safe water, clean preparation and correct dilution is lifesaving [3]. Fortified blended foods and locally appropriate iron-rich complementary foods are the foundation of safe weaning where commercial options are unaffordable [1].
Infants with complex needs — cleft palate, neurological impairment, congenital heart disease — often need a tailored feeding plan and may progress more slowly through textures, with input from a multidisciplinary feeding team [1]. Cultural, Indigenous and migrant feeding practices vary widely in weaning age, first foods, and the use of family foods; the clinician's role is to give evidence-based guidance that is also culturally safe, building on existing practices rather than dismissing them [1].
Evidence, Guidelines & Regional Differences
The international baseline is the World Health Organization, which recommends exclusive breastfeeding for six months with continued breastfeeding alongside complementary foods to two years and beyond [3]. ESPGHAN's position papers set the European and much of the global technical standard, recommending that complementary feeding begin no earlier than four months and not later than six months, that any food can be introduced from around six months, and that allergens be introduced early and kept in the diet [1][2]. The American Academy of Pediatrics likewise supports exclusive breastfeeding for about six months and continued breastfeeding to twelve months and beyond [4].
The Australian NHMRC Infant Feeding Guidelines recommend exclusive breastfeeding to around six months, the introduction of solid foods at around six months (not before four months), continued breastfeeding to twelve months and beyond, iron-rich first foods, and no honey before twelve months. Whole cow's milk is introduced as the main drink from around twelve months. These align closely with WHO and ESPGHAN. [1]
WHO and UNICEF frame complementary feeding within the broader protection, promotion and support of breastfeeding, and emphasise safe preparation and age-appropriate, nutrient-dense complementary foods as a global child-survival priority, particularly in low-resource settings where unsafe formula and inadequate weaning foods drive malnutrition and mortality. [3]
The landmark trials that reshaped allergy advice are LEAP and EAT. LEAP randomised high-risk infants to early regular peanut consumption versus avoidance and showed a large reduction in peanut allergy, overturning decades of avoidance advice [5]. EAT tested early introduction of multiple allergenic foods in the general breast-fed population and supported the principle, though with challenges to adherence [6]. Together they established that early, regular allergen exposure induces tolerance. Controversies persist around the marketing and necessity of follow-on and toddler milks, the optimal protein content of infant formula, and whether puree-led or baby-led weaning approaches are superior — current evidence supports responsive feeding and texture progression over any rigid method [1][9].
Exam Pearls
The frequently misremembered facts are where marks are lost and won. Soy formula is not a first-line formula and does not prevent allergy [7]. Follow-on formula is not a nutritional requirement at six months [1]. Whole cow's milk as a drink is for after twelve months, not from six [1][10]. The tongue-thrust reflex usually fades around four to six months, marking feeding readiness rather than a fixed calendar date [1]. Early allergen introduction prevents allergy; delaying it does not [5][6]. And the single most common feeding error in clinic is a preparation mistake — the wrong number of scoops — so always ask how the family makes up a feed [7].
IRON-FED
The handful of one-liners an examiner rewards: complementary feeding begins at around six months; iron-rich foods first; allergens early and regularly; cow's milk as the main drink after twelve months; no honey before twelve months; and a first infant formula is appropriate for the whole first year [1][2][5][10].
References
- [1]Fewtrell M; Bronsky J; Campoy C; Domellöf M; Embleton N; Fidler Mis N; et al Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J Pediatr Gastroenterol Nutr, 2017.PMID 28027215
- [2]Agostoni C; Decsi T; Fewtrell M; Goulet O; Kolacek S; Koletzko B; et al Complementary feeding: a commentary by the ESPGHAN Committee on Nutrition. J Pediatr Gastroenterol Nutr, 2008.PMID 18162844
- [3]Kramer MS; Kakuma R Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev, 2012.PMID 22895934
- [4]Meek JY; Noble L; Section on Breastfeeding Policy Statement: Breastfeeding and the Use of Human Milk. Pediatrics, 2022.PMID 35921640
- [5]Du Toit G; Roberts G; Sayre PH; Bahnson HT; Radulovic S; Santos AF; et al Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med, 2015.PMID 25705822
- [6]Perkin MR; Logan K; Tseng A; Raji B; Ayis S; Peacock J; et al Randomized Trial of Introduction of Allergenic Foods in Breast-Fed Infants. N Engl J Med, 2016.PMID 26943128
- [7]Koletzko B; Baker S; Cleghorn G; Neto UF; Gopalan S; Hernell O; et al Global standard for the composition of infant formula: recommendations of an ESPGHAN coordinated international expert group. J Pediatr Gastroenterol Nutr, 2005.PMID 16254515
- [8]Huh SY; Rifas-Shiman SL; Taveras EM; Oken E; Gillman MW Timing of solid food introduction and risk of obesity in preschool-aged children. Pediatrics, 2011.PMID 21300681
- [9]Totzauer M; Escribano J; Closa-Monasterolo R; Luque V; Verduci E; ReDionigi A; et al Different protein intake in the first year and its effects on adiposity rebound and obesity throughout childhood: 11 years follow-up of a randomized controlled trial. Pediatr Obes, 2022.PMID 36355369
- [10]Tsai SF; Chen SJ; Yen HJ; Hung GY; Tsao PC; Jeng MJ; et al Iron deficiency anemia in predominantly breastfed young children. Pediatr Neonatol, 2014.PMID 24953965
- [11]Yadav B; Gupta N; Sasidharan R; Thanigainathan S; Purohit P; Singh K; et al 800 IU versus 400 IU per day of vitamin D(3) in term breastfed infants: a randomized controlled trial from an LMIC. Eur J Pediatr, 2022.PMID 35726033