Paeds · gastroenterology-hepatology-and-nutrition
Functional abdominal pain and irritable bowel syndrome
Also known as Functional abdominal pain disorders · Irritable bowel syndrome in children · Paediatric IBS · Functional abdominal pain not otherwise specified · Disorders of gut-brain interaction · Rome IV functional gastrointestinal disorders
Fellowship guide to paediatric functional abdominal pain and irritable bowel syndrome as disorders of gut-brain interaction: the Rome IV criteria that define functional abdominal pain-NOS and the IBS subtypes (IBS-C, IBS-D, IBS-M, IBS-U), the visceral hypersensitivity mechanism, the alarm features that separate functional from organic disease, a targeted rather than exhaustive workup, and stepwise biopsychosocial management from explanation and reassurance through cognitive behavioural therapy, gut-directed hypnotherapy, low-FODMAP diet, peppermint oil, and selective pharmacology.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child who has months of tummy pain, whose bowels swing between loose and hard, who looks well and grows normally, and in whom every routine test comes back clear is describing one of the commonest problems in paediatric gastroenterology. In most such children the pain is not caused by damaged tissue but by a disordered conversation between the gut and the brain. Functional abdominal pain and irritable bowel syndrome are the two headline members of this family of disorders of gut-brain interaction. [1]
Both are now defined positively by the Rome IV criteria rather than by ruling out every possible organic cause. Functional abdominal pain-NOS describes recurrent or continuous abdominal pain that does not fit a more specific pattern, while irritable bowel syndrome is the disorder in which the pain is tied to defecation and to a change in stool form or frequency. The distinction between them rests almost entirely on the relationship between the pain and the bowels. [1]
The clinical skill that this topic trains is twofold: to recognise the positive pattern of a functional disorder or IBS so a confident diagnosis can be made after a short targeted workup, and to detect the alarm features that flag the minority with organic disease. Getting this balance right spares the child the harm of endless investigation while keeping serious disease from being missed. [11]
Classification
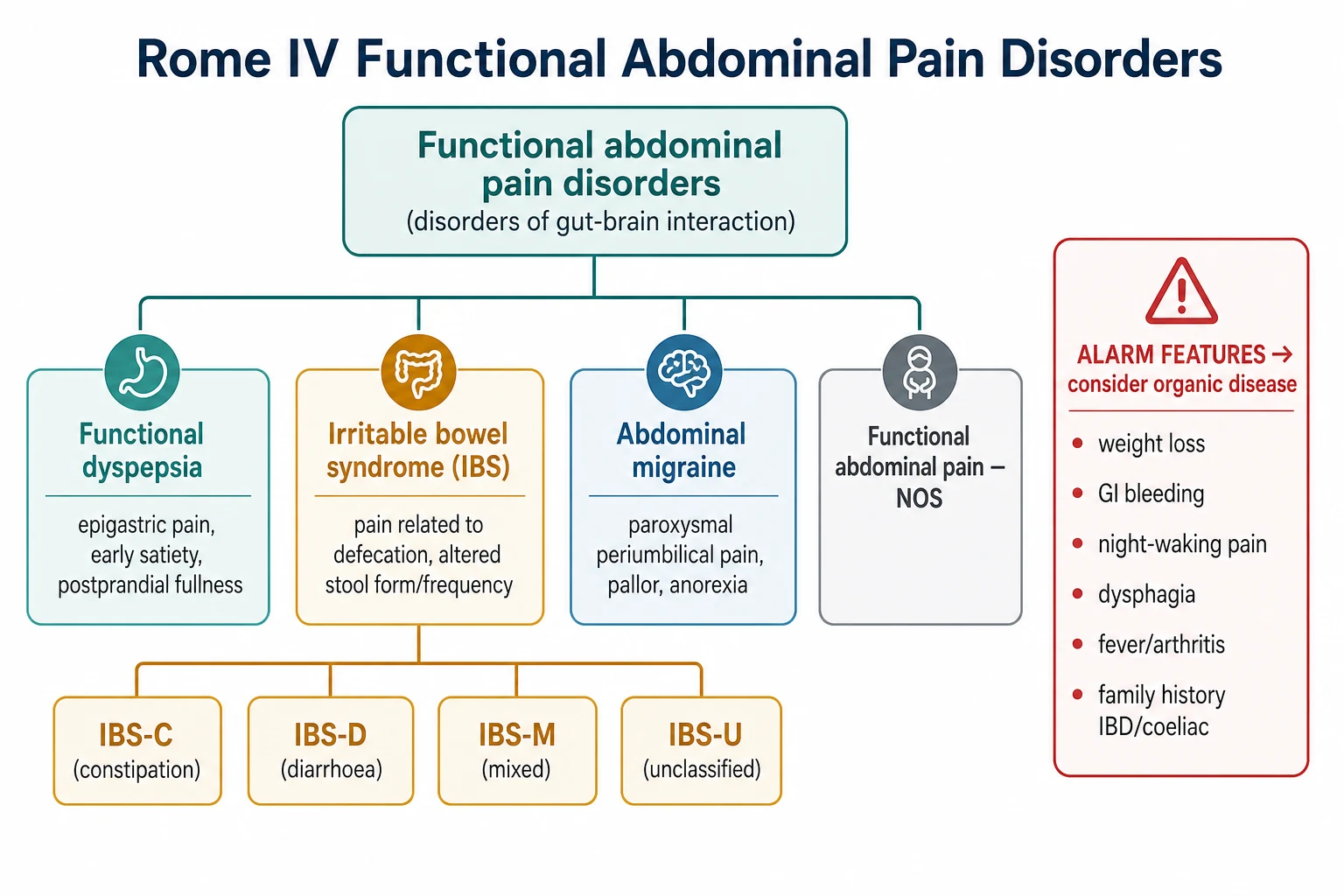
The first and most useful division separates functional from organic causes, because it steers the whole approach. Functional disorders share a well child, normal growth, a normal examination, and an absence of alarm features, whereas organic disease tends to declare itself through weight loss, bleeding, or systemic signs. Within the functional group, Rome IV then names four abdominal pain-related disorders that a candidate must be able to distinguish. [1]
[1]Irritable bowel syndrome is itself divided by the predominant stool pattern, and this subtyping guides treatment. IBS with constipation, IBS with diarrhoea, and mixed IBS are the three practical subtypes, with an unclassified group for children who do not fit neatly. The subtype is judged from the abnormal stools using the Bristol stool scale, and it can shift over time, so it is reassessed rather than fixed at diagnosis. [1]
[1]Epidemiology & Risk Factors
Functional abdominal pain disorders are among the most common complaints in paediatric practice. A meta-analysis of worldwide studies estimated a pooled prevalence of about 13.5 per cent in children and adolescents, with irritable bowel syndrome the single most frequent subtype at roughly 8 to 9 per cent. Girls are affected more often than boys, and presentation peaks across the school-age and early adolescent years. [2]
Several factors raise the risk of developing and maintaining functional pain and IBS. Anxiety, depression, and a history of stressful life events are consistently associated, as are parental anxiety and a family pattern of somatic symptoms and healthcare seeking. An episode of acute gastroenteritis can trigger a post-infectious IBS. Early-life stress, bullying, and school difficulties all feed the disorder through the gut-brain axis. [1]
The way parents and clinicians respond can either settle or entrench the pain. Excessive attention to symptoms, repeated investigation, and withdrawal from school tend to reinforce the illness behaviour, whereas calm reassurance and a return to normal activity promote recovery. Children with IBS and functional abdominal pain share high rates of anxiety and depression, which is why the psychosocial history is a core part of assessment rather than an optional extra. [12]
Pathophysiology
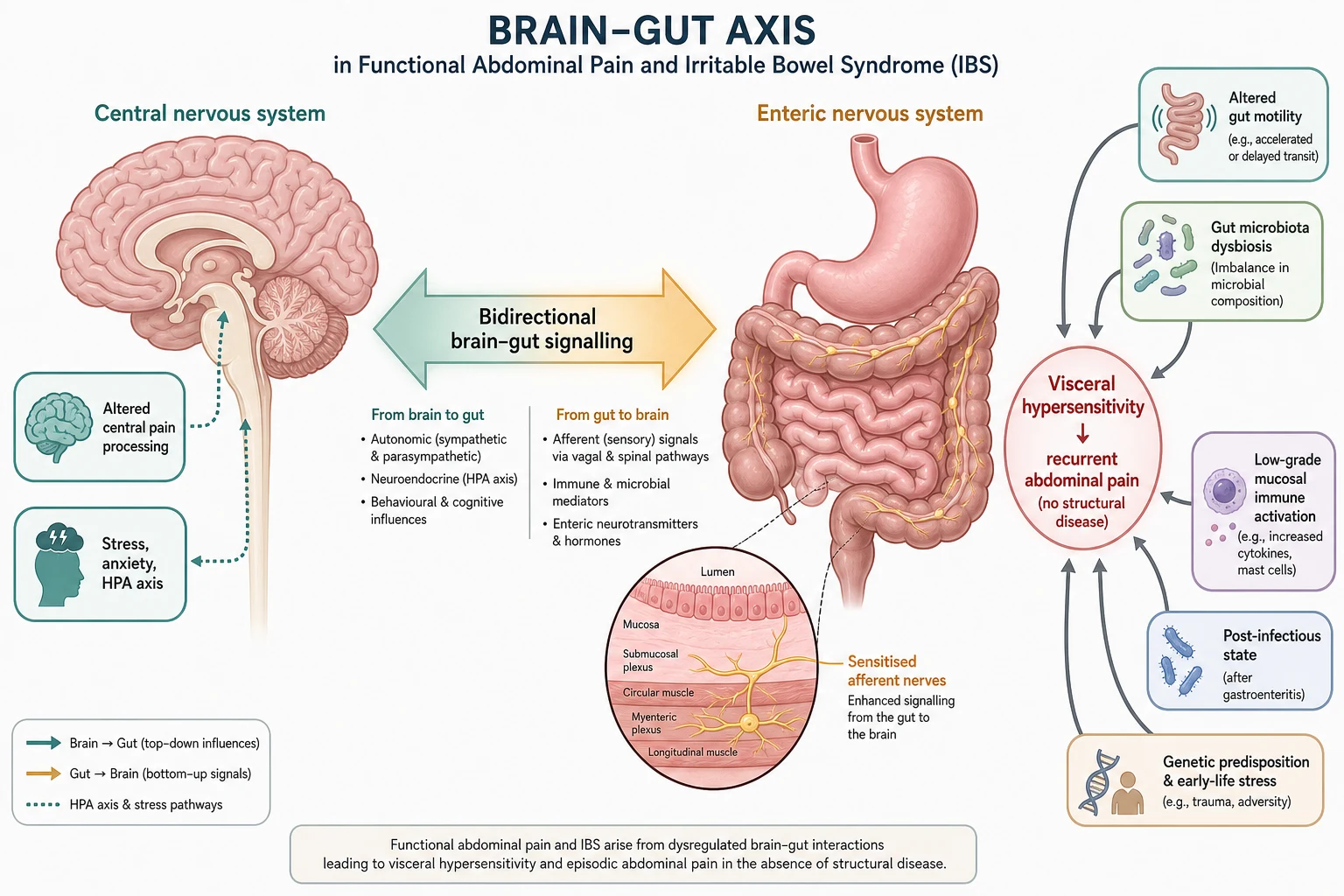
Functional abdominal pain and IBS arise from disordered communication along the gut-brain axis rather than from tissue damage. Signals pass in both directions between the central nervous system and the enteric nervous system, modulated by the autonomic nerves, the hypothalamic-pituitary-adrenal stress axis, and the gut microbiota. When this signalling is dysregulated, normal gut events such as filling and peristalsis are perceived as painful. [1]
The core mechanism is visceral hypersensitivity, a lowered threshold at which gut stimuli are registered as pain. Sensitised afferent nerves in the gut wall and altered central pain processing mean that ordinary distension or contraction produces discomfort that a child without the disorder would never notice. Stress, anxiety, and negative expectation amplify this central sensitisation, which explains the tight link between symptoms and emotional state. [1]
Several biological contributors feed into this final common pathway, and in IBS they help explain the altered bowel habit. Changed gut motility drives the swing between constipation and diarrhoea, while low-grade mucosal immune activation, shifts in the intestinal microbiota, and a post-infectious state after gastroenteritis all sensitise the gut. Genetic predisposition and early-life adversity set the background sensitivity, and diet, sleep, and psychosocial stress act as day-to-day triggers. No single lesion is responsible, which is why no single test can confirm the diagnosis. [10]
Clinical Presentation
The typical child is of school age, presents with weeks to months of recurrent central abdominal pain, and looks well between episodes. Growth is normal, the physical examination is unremarkable, and the child is not systemically unwell. Pain often clusters around stressful times such as school mornings and eases at weekends and during holidays, a pattern that supports a functional origin. [11]
Irritable bowel syndrome adds a bowel-habit signature to this picture. The pain is relieved or sometimes provoked by defecation, and it is accompanied by a change in how often the child opens the bowels or in the form of the stool. Bloating, a sense of incomplete evacuation, urgency, and mucus in the stool are common, and the predominant stool pattern defines whether the child has the constipation, diarrhoea, or mixed subtype. [1]
The other Rome IV disorders each carry their own colour. Functional dyspepsia brings upper abdominal pain, early satiety, and postprandial fullness. Abdominal migraine produces stereotyped, incapacitating attacks of periumbilical pain with pallor, nausea, and anorexia, separated by weeks of complete wellness. Functional abdominal pain-NOS is recurrent or continuous pain without the defecation link of IBS or the meal link of dyspepsia. [1]
Features that point toward functional pain or IBS
Recurrent central or periumbilical pain over weeks to months
Well appearance and normal growth between episodes
Normal physical examination with no alarm features
In IBS, pain relieved or triggered by defecation
In IBS, change in stool form or frequency, bloating, or urgency
Emotional or school-related stressors in the background
Differential Diagnosis
The differential is broad, so the disciplined approach uses alarm features to decide who needs investigation rather than testing every child. When alarm features are absent, growth is normal, and the examination is clear, functional abdominal pain or IBS is the most likely diagnosis and can be made positively. When alarm features are present, the workup is directed at the organs and diseases they suggest. [11]
Gastrointestinal organic causes to keep in mind include coeliac disease, inflammatory bowel disease, peptic ulcer and Helicobacter pylori, chronic constipation, lactose and carbohydrate malabsorption, and giardiasis and other infections. In a child whose main symptom is diarrhoea, coeliac disease, inflammatory bowel disease, and giardiasis are especially important to exclude before settling on IBS with diarrhoea. Acutely, appendicitis, intussusception, and malrotation with volvulus must not be overlooked when the story shifts. [10]
Extra-intestinal mimics complete the picture. Urinary tract infection and renal disease, gynaecological causes such as dysmenorrhoea and ovarian pathology in adolescents, diabetic ketoacidosis, lower lobe pneumonia, and abdominal migraine all deserve consideration. In every case the aim is to weigh the clinical pattern rather than reflexively order a panel of tests, because over-investigation reinforces illness behaviour and rarely changes the diagnosis. [11]
Clinical & Bedside Assessment
A structured history is the highest-yield tool. Characterise the pain by its site, timing, radiation, relationship to meals and defecation, and pattern over time, and in a suspected IBS establish the stool form and frequency using the Bristol stool scale. Ask directly about alarm features: weight loss, blood in stool or vomit, night waking with pain, nocturnal diarrhoea, dysphagia, fever, joint symptoms, and mouth or perianal disease. Explore the family history of coeliac disease and inflammatory bowel disease. [10]
Give equal weight to the psychosocial history. Ask about school attendance and performance, friendships and bullying, sleep, mood and anxiety, recent life events, and how the family responds to the pain. Understanding the child's daily function and the reinforcing behaviours around the symptom guides both the diagnosis and the management plan, and framing these questions as routine keeps the family from feeling accused. [12]
The examination should be thorough and, when normal, reassuring to both clinician and family. Plot height and weight on a growth chart and review the trajectory, assess pubertal stage in adolescents, and examine the abdomen for masses, organomegaly, and localised tenderness. Inspect the perianal area when inflammatory bowel disease is suspected, and perform a general examination for pallor, clubbing, rashes, and joint signs. [10]
Investigations
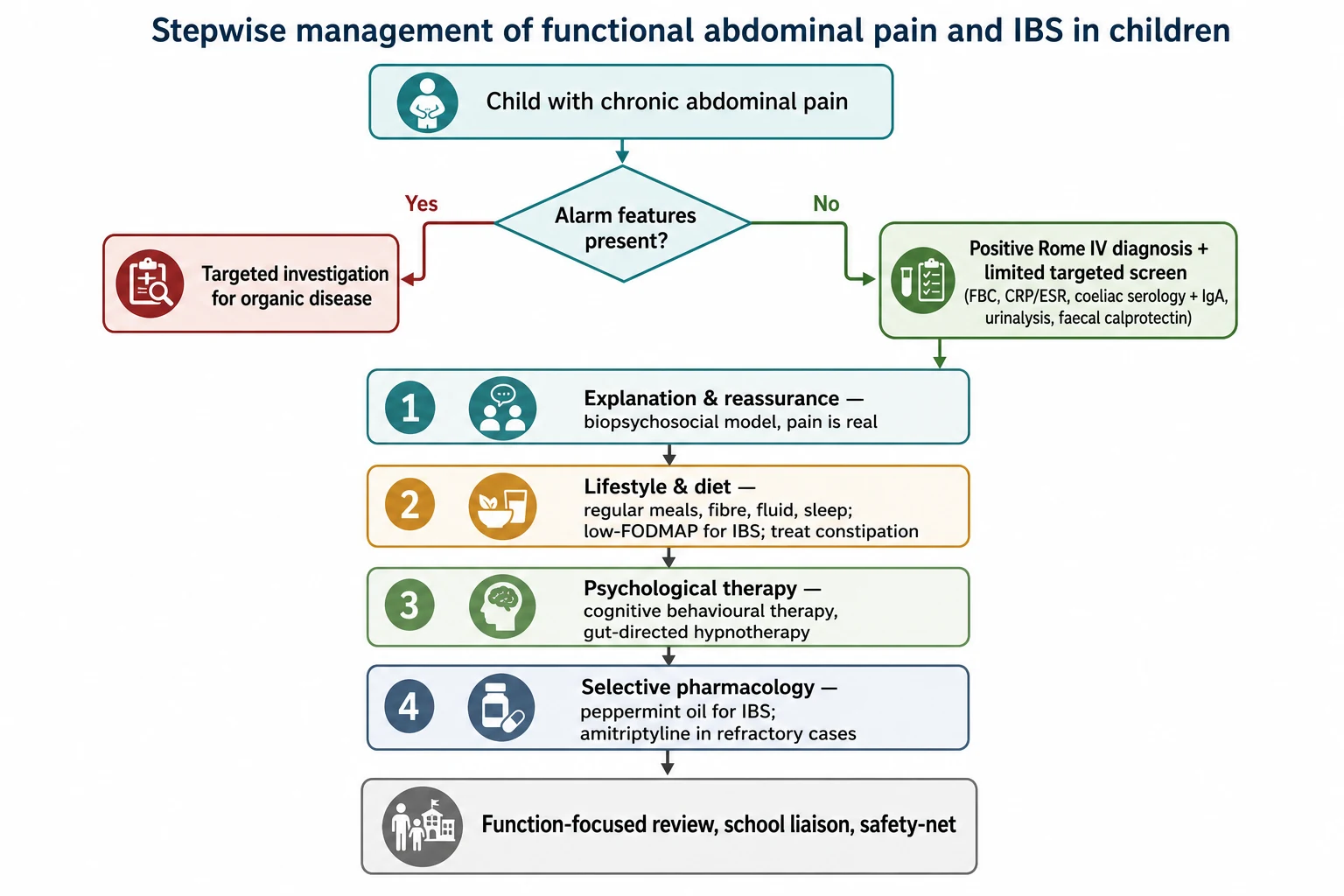
Investigation should be targeted, not reflexive. In a well child with a typical functional or IBS pattern, no alarm features, and normal growth and examination, extensive testing is unnecessary and can be harmful by reinforcing the search for disease. A limited first-line screen reassures the family, excludes the common treatable organic mimics, and supports a confident positive diagnosis. [11]
A reasonable baseline in most children includes a full blood count, inflammatory markers such as C-reactive protein and erythrocyte sedimentation rate, coeliac serology with total immunoglobulin A, and a urinalysis. A faecal calprotectin is particularly valuable in a child with diarrhoea because it helps separate inflammatory bowel disease from IBS, and stool testing for giardia or Helicobacter pylori antigen is added when the history suggests them. Normal results in a well child strongly favour a functional disorder. [10]
Second-line tests are reserved for children with alarm features or an abnormal screen. Abdominal ultrasound helps when pain is focal, right-sided, or suggests biliary, renal, or gynaecological disease, though it is low-yield in typical central functional pain. Upper endoscopy is appropriate for persistent dyspeptic symptoms or suspected ulcer, and colonoscopy for suspected inflammatory bowel disease, especially where calprotectin is raised. Order each test to answer a specific question rather than as a routine sweep. [10]
Management — Resuscitation
Most functional abdominal pain and IBS needs no resuscitation, but the clinician must stay alert to the child who presents acutely unwell or with a surgical abdomen superimposed on chronic symptoms. Bilious vomiting, severe localised pain with guarding, signs of obstruction, gastrointestinal bleeding, or shock demand immediate assessment along airway, breathing, and circulation lines and urgent surgical review. [10]
In this acute setting, secure intravenous access, take bloods, give analgesia, and keep the child fasted while a surgical cause such as appendicitis, intussusception, or malrotation with volvulus is excluded. Correct dehydration with isotonic fluid and check glucose, electrolytes, and, in an unwell adolescent, a pregnancy test and ketones. The presence of a longstanding functional disorder or IBS never removes the duty to exclude a new acute organic emergency. [10]
For the far more common non-acute presentation, the immediate priority is different: it is to provide effective explanation, validate the pain, and prevent the harm of over-investigation. Reassurance delivered with a clear model of why the pain occurs is itself a therapeutic intervention and often reduces symptom severity before any specific treatment begins. [1]
Red-flag acute presentation priorities
Assess airway, breathing, circulation in the acutely unwell child
Exclude surgical abdomen: appendicitis, intussusception, volvulus
Keep fasted, secure IV access, give analgesia, take bloods
Correct dehydration; check glucose, electrolytes, ketones
Pregnancy test in adolescent girls with acute pain
Urgent surgical review for guarding, obstruction, or bleeding
Management — Definitive & Stepwise
The foundation of treatment is a positive diagnosis delivered with a clear biopsychosocial explanation. Explain that the pain is real, that it comes from an oversensitive gut-brain connection rather than damage, and that the goal is to restore normal function while the symptoms settle. Set expectations that improvement is gradual and that a return to school and activity is part of the treatment, not something to wait for. [1]
Lifestyle and dietary measures come next, and in IBS the diet is more central than in undifferentiated functional pain. Encourage regular meals, adequate fibre and fluid, good sleep, and physical activity, and treat any constipation in the IBS-C subtype. A supervised low-FODMAP trial can reduce pain and bloating in IBS, but restrictive diets must be time-limited and dietitian-supervised to avoid nutritional harm, and a symptom diary helps identify individual triggers. [8]
Psychological therapies have the strongest evidence for functional abdominal pain and IBS. Gut-directed hypnotherapy produced markedly better pain relief than standard care in a randomised trial, with benefit sustained years later, and cognitive behavioural therapy delivered to the child and parents also reduces pain and improves function. These are not a signal that the pain is imaginary but a direct treatment of the gut-brain mechanism, and framing them this way improves uptake. [3]
[8]Pharmacology is reserved for children with severe or refractory symptoms and is used alongside, not instead of, the measures above. Peppermint oil reduced pain in a small randomised trial of children with irritable bowel syndrome and is a reasonable option for IBS-type symptoms. Amitriptyline is sometimes used for severe functional pain, but a multicentre randomised trial found no significant benefit over placebo, which itself produced a large response, so any trial of a tricyclic should be time-limited and carefully reviewed. [5]
Amitriptyline (selected severe or refractory functional pain or IBS)
Dose
Low dose, for example 10 mg at night in older children, titrated cautiously
Specific Subtypes & Scenarios
Irritable bowel syndrome is managed according to its predominant stool pattern. In IBS with constipation, treat the constipation directly and optimise fibre and fluid; in IBS with diarrhoea, focus on trigger avoidance, a supervised low-FODMAP trial, and confident exclusion of inflammatory bowel disease and coeliac disease using faecal calprotectin and serology. Across all subtypes, reassurance that IBS is a genuine but benign disorder that does not lead to serious bowel disease is central to reducing anxiety. [1]
Functional dyspepsia centres on upper abdominal symptoms: epigastric pain or burning, early satiety, and postprandial fullness. Management follows the same biopsychosocial base, with attention to meal patterns and avoidance of triggers. A trial of acid suppression is reasonable for pain-predominant symptoms, and testing for Helicobacter pylori is guided by history, with eradication offered when infection is confirmed. [1]
Abdominal migraine produces stereotyped, severe attacks of periumbilical pain with pallor, nausea, and anorexia, and complete wellness between episodes, often in a child with a personal or family history of migraine. Management mirrors that of migraine: identify and avoid triggers, treat acute attacks supportively, and consider prophylaxis such as pizotifen for frequent, disabling episodes. Recognising the pattern spares the child repeated acute workups. [1]
[8]Complications & Pitfalls
The main complications of functional abdominal pain and IBS are those of the disability rather than the disease. Prolonged school absence, social withdrawal, disrupted sleep, and secondary anxiety and low mood can entrench a cycle of pain and avoidance that is harder to reverse the longer it persists. Early, function-focused treatment prevents this downward spiral and is the reason not to delay management while awaiting more tests. [1]
Iatrogenic harm is a real and avoidable complication. Repeated blood tests, imaging, endoscopy, and specialist referrals in a child without alarm features rarely change the diagnosis but heighten family anxiety, expose the child to procedures, and reinforce the belief that serious disease is being missed. Restraint in testing is an active clinical skill, not a failure to act. [11]
The classic pitfalls are twofold and opposite. The first is over-investigation and failure to make a positive diagnosis, leaving the child in limbo without treatment. The second is complacency: labelling pain as functional or IBS and dismissing it, then missing evolving organic disease such as inflammatory bowel disease, which nocturnal diarrhoea or a rising calprotectin should flag. Safety-netting with clear review and a low threshold to re-examine when the pattern changes guards against both errors. [10]
Prognosis & Disposition
The outlook is generally good, and most children improve with explanation, reassurance, and time. A substantial proportion become pain-free within months to a year, particularly when treatment begins early and the family engages with a function-focused plan. Clear communication that recovery is expected is itself a positive prognostic factor. [1]
A minority follow a more persistent course, with pain continuing into adolescence or adulthood or evolving into other functional syndromes, and childhood IBS raises the risk of adult IBS. Persistence is more likely with high baseline anxiety or depression, greater symptom severity and disability at presentation, and unhelpful parental responses that reinforce the illness. These children benefit most from structured psychological therapy and coordinated care. [4]
Most children can be managed entirely in primary care or general paediatrics, with follow-up focused on function, school attendance, mood, and bowel habit rather than on repeated testing. Referral to paediatric gastroenterology is appropriate for alarm features, an abnormal screen, or failure to respond to first-line treatment, and referral to psychology is appropriate for significant anxiety, depression, or disability. Set review dates and safety-net clearly. [11]
Special Populations
Children with anxiety, depression, or neurodevelopmental conditions such as autism spectrum disorder are over-represented among those with functional abdominal pain and IBS, and their pain can be harder to characterise. Assessment must adapt to communication needs, and management should be tightly coordinated with mental health services, because treating the co-existing emotional disorder often improves the pain. [12]
Socioeconomic disadvantage and limited access to psychological therapy, dietitians, and paediatric gastroenterology can worsen outcomes by delaying diagnosis and restricting evidence-based treatment. Practical, low-cost interventions such as clear explanation, primary care follow-up, school liaison, and telehealth-delivered psychological support help close this gap for families who cannot easily reach specialist centres. [8]
Adolescents warrant particular attention to menstrual history, mental health, and the transition toward self-management. Dysmenorrhoea and gynaecological causes enter the differential, the risk of depression and self-harm rises, and disordered eating can complicate dietary interventions such as the low-FODMAP diet. Building the young person's own understanding and coping skills prepares them for adult care and reduces long-term healthcare dependence. [1]
[2]Evidence, Guidelines & Regional Differences
The Rome IV criteria, published in 2016, define the paediatric functional abdominal pain disorders and underpin current diagnosis. They deliberately promote a positive, symptom-based diagnosis with limited testing rather than a diagnosis of exclusion, and they separate functional dyspepsia, irritable bowel syndrome with its subtypes, abdominal migraine, and functional abdominal pain-NOS. This framework is the reference standard for both examinations and practice. [1]
The AAP and NASPGHAN clinical and technical reports on chronic abdominal pain established that, in the absence of alarm features, extensive testing is low-yield and that a functional diagnosis can be made confidently. Systematic reviews since then have clarified treatment: nonpharmacological therapies, especially gut-directed hypnotherapy and cognitive behavioural therapy, have the best evidence, while the pharmacological evidence base remains limited. [8]
[8]Controversies and regional differences persist. The pharmacological evidence is weak, with a striking placebo response in trials, so drug use varies widely between centres. The role and intensity of the low-FODMAP diet in children is debated given the risk of nutritional harm, and access to psychological therapies and specialist dietitians differs markedly between and within countries. The consistent theme across guidelines is confident positive diagnosis and biopsychosocial treatment. [9]
Exam Pearls
ALARMS for red flags in functional pain and IBS
References
- [1]Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, van Tilburg M Functional Disorders: Children and Adolescents. Gastroenterology, 2016.PMID 27144632
- [2]Korterink JJ, Diederen K, Benninga MA, Tabbers MM Epidemiology of pediatric functional abdominal pain disorders: a meta-analysis. PLoS One, 2015.PMID 25992621
- [3]Vlieger AM, Menko-Frankenhuis C, Wolfkamp SC, Tromp E, Benninga MA Hypnotherapy for children with functional abdominal pain or irritable bowel syndrome: a randomized controlled trial. Gastroenterology, 2007.PMID 17919634
- [4]Vlieger AM, Rutten JM, Govers AM, Frankenhuis C, Benninga MA Long-term follow-up of gut-directed hypnotherapy vs. standard care in children with functional abdominal pain or irritable bowel syndrome. Am J Gastroenterol, 2012.PMID 22310221
- [5]Kline RM, Kline JJ, Di Palma J, Barbero GJ Enteric-coated, pH-dependent peppermint oil capsules for the treatment of irritable bowel syndrome in children. J Pediatr, 2001.PMID 11148527
- [6]Saps M, Youssef N, Miranda A, Nurko S, Hyman P, Cocjin J, Di Lorenzo C Multicenter, randomized, placebo-controlled trial of amitriptyline in children with functional gastrointestinal disorders. Gastroenterology, 2009.PMID 19596010
- [7]Levy RL, Langer SL, Walker LS, Romano JM, Christie DL, Youssef N, DuPen MM, Feld AD, Ballard SA, Welsh EM, Jeffery RW, Young M, Coffey MJ, Whitehead WE Cognitive-behavioral therapy for children with functional abdominal pain and their parents decreases pain and other symptoms. Am J Gastroenterol, 2010.PMID 20216531
- [8]Rutten JM, Korterink JJ, Venmans LM, Benninga MA, Tabbers MM Nonpharmacologic treatment of functional abdominal pain disorders: a systematic review. Pediatrics, 2015.PMID 25667239
- [9]Korterink JJ, Rutten JM, Venmans L, Benninga MA, Tabbers MM Pharmacologic treatment in pediatric functional abdominal pain disorders: a systematic review. J Pediatr, 2015.PMID 25449223
- [10]Di Lorenzo C, Colletti RB, Lehmann HP, Boyle JT, Gerson WT, Hyams JS, Squires RH Jr, Walker LS, Kanda PT Chronic Abdominal Pain In Children: a Technical Report of the American Academy of Pediatrics and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr, 2005.PMID 15735476
- [11]American Academy of Pediatrics Subcommittee on Chronic Abdominal Pain Chronic abdominal pain in children. Pediatrics, 2005.PMID 15741394
- [12]Rutten JM, Benninga MA, Vlieger AM IBS and FAPS in children: a comparison of psychological and clinical characteristics. J Pediatr Gastroenterol Nutr, 2014.PMID 24897168