Paeds · gastroenterology-hepatology-and-nutrition
Gastro-oesophageal reflux and reflux disease
Also known as GOR and GORD · Gastro-oesophageal reflux disease in children · Infant reflux and posseting · Paediatric acid reflux · Reflux oesophagitis in children
Fellowship guide to paediatric gastro-oesophageal reflux and reflux disease — how to separate the physiologic reflux of the happy spitter from the disease that harms, the transient-sphincter-relaxation pathophysiology, the conservative-first stepwise ladder that keeps children off unnecessary acid suppression, and the red flags that turn reflux into a surgical or allergic emergency.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Few paediatric labels are applied as loosely, or as often, as "reflux". Every posset, every unsettled evening, and every back-arch after a feed attracts the word, and much of the time the word is wrong. The discipline this topic teaches is judgement: telling the common, harmless, self-limiting reflux of a thriving baby from the disease that genuinely harms, and refusing the reflex prescription of an acid-suppressing drug the evidence does not support. [1]
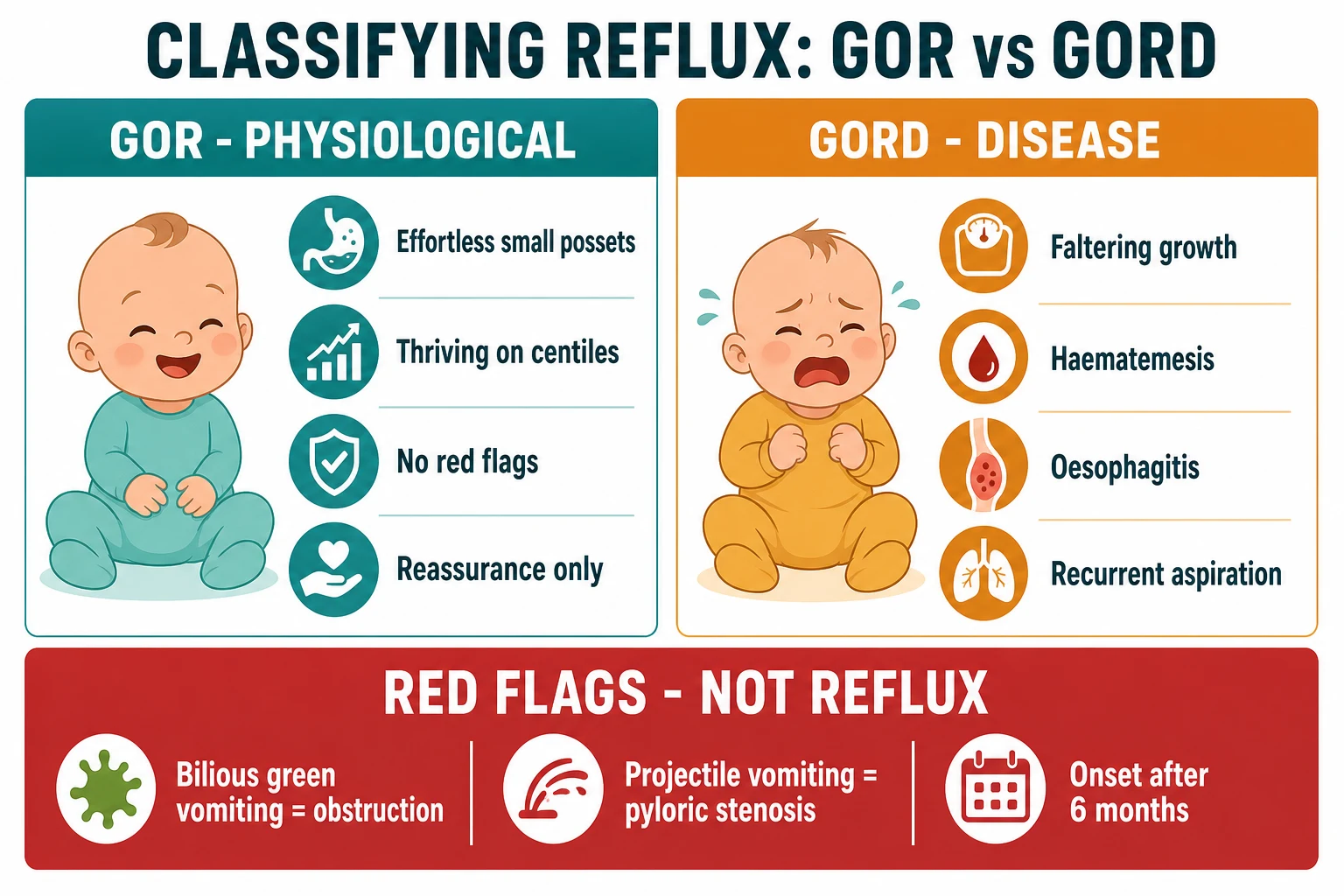
Gastro-oesophageal reflux, or GOR, is the effortless retrograde movement of gastric contents into the oesophagus, with or without regurgitation into the mouth. In infants it is the physiological norm rather than the exception, driven by an immature anti-reflux barrier and a liquid diet, and it resolves as the child sits, walks, and moves to solid food. Gastro-oesophageal reflux disease, GORD, is the term reserved for reflux that produces troublesome symptoms or complications, and separating the two is the single most important judgement you make at the cot-side and in clinic. [1]
The vocabulary matters because examiners test it. Regurgitation is the visible return of gastric contents into the pharynx or mouth, and posseting is the small, effortless bringing up of milk. Vomiting is different — it is forceful and involves coordinated muscular effort, and a forceful or projectile vomit is a surgical symptom until proven otherwise. Rumination and cyclical vomiting are distinct entities that masquerade as reflux and must be recognised on their own terms. [1]
Classification
The classification that changes management is the split between physiologic reflux and disease, and it rests entirely on whether reflux causes trouble. Physiologic GOR is effortless regurgitation in a child who is thriving, feeding well, and free of red flags, and it needs reassurance alone. GORD is reflux accompanied by troublesome symptoms or complications — faltering growth, oesophagitis, haematemesis, anaemia, recurrent aspiration, or distress that impairs feeding and quality of life — and it needs targeted assessment and treatment. [1]
A second, clinically useful axis separates the patterns of disease. Oesophageal GORD produces heartburn, epigastric or retrosternal pain, regurgitation, and, in older children, the adult picture of dyspepsia. Extra-oesophageal GORD is the harder group — chronic cough, wheeze, recurrent pneumonia, dental erosion, and hoarseness — where the causal link to reflux is frequently overstated and rarely proven. Naming which pattern you are treating keeps the investigation and the prescription honest. [1]
Epidemiology & Risk Factors
Regurgitation is one of the most common concerns parents raise in the first months of life, and the prevalence alone explains why over-treatment is the rule. In a pediatric practice-based survey, daily regurgitation peaked at around half of infants at four months of age, and the symptom resolved in the vast majority by the end of the first year. This natural history — near-universal, benign, and self-limiting — is the epidemiological backbone of the conservative approach. [8] [9]
The children who tip from physiologic reflux into disease sit at recognisable ends of a gradient. Prematurity, neurological impairment such as cerebral palsy, oesophageal atresia after repair, hiatus hernia, chronic lung disease including cystic fibrosis, and obesity in older children all raise both the frequency of reflux and the chance that it will cause harm. A thriving term infant who possets is at the benign end; a child with severe neurodisability on gastrostomy feeds is at the dangerous end. [1] [7]
Age itself is a powerful risk marker. Reflux that starts in the first weeks and eases through infancy follows the physiologic pattern, whereas reflux that begins after six months, persists beyond the first birthday, or first appears in an older child is atypical and should prompt a search for another diagnosis. Timing, therefore, is not a detail but a discriminator that steers the whole assessment. [1]
Pathophysiology
The anti-reflux barrier is a team of structures, and in the young child several members of that team are still developing. The lower oesophageal sphincter sits at the gastro-oesophageal junction, and its resting tone normally keeps the junction closed between swallows. The angle of His and the crural diaphragm add a mechanical valve, and the intra-abdominal segment of oesophagus is compressed shut by abdominal pressure. Weakness anywhere in this system lets gastric contents ascend. [1]
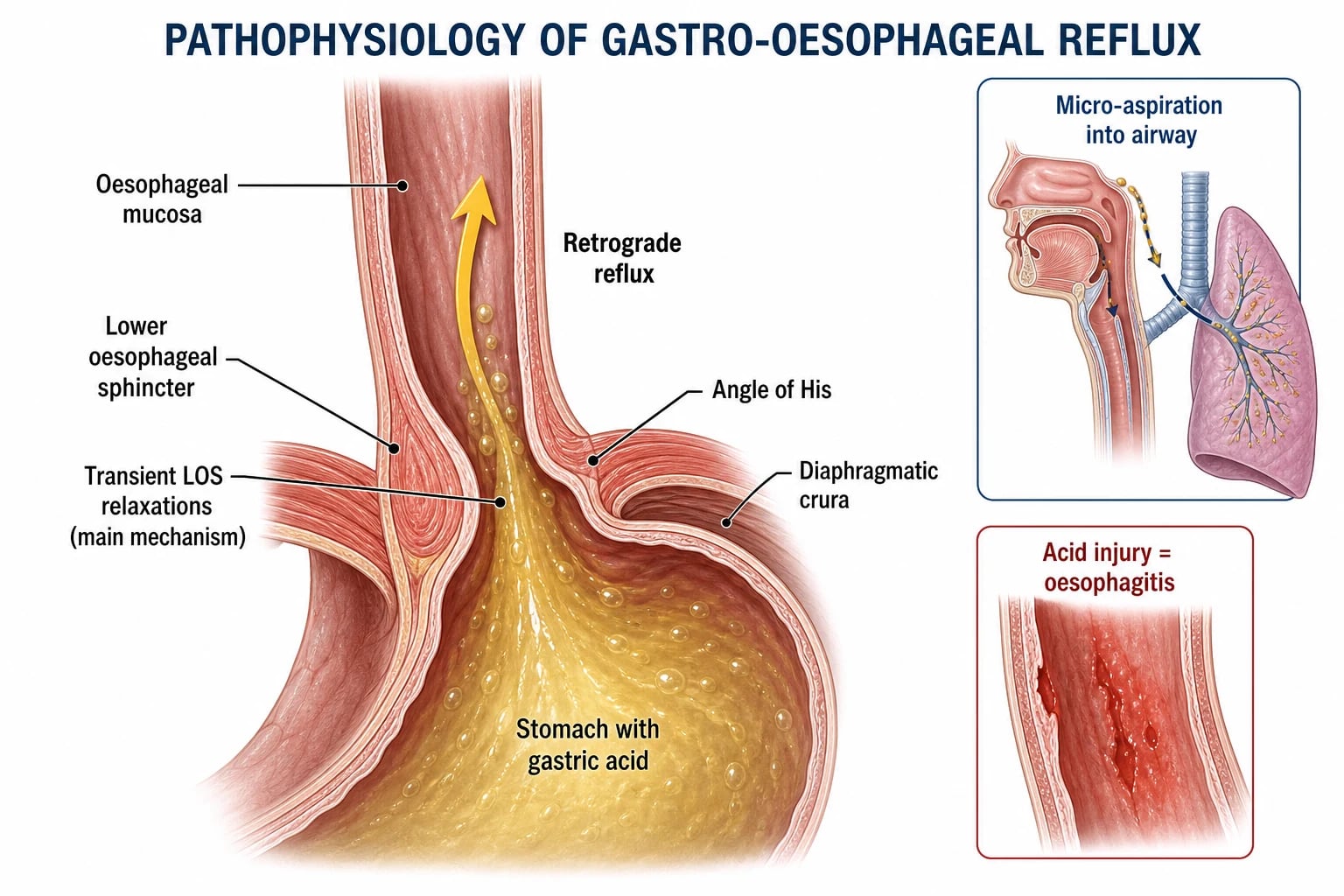
The dominant mechanism is not a chronically weak sphincter but the transient lower-oesophageal-sphincter relaxation. These are brief, inappropriate openings of the sphincter that occur independent of swallowing, most often triggered by gastric distension after a feed, and they account for the majority of reflux events. Layered onto this are a small, easily distended stomach, delayed gastric emptying, a predominantly liquid diet, and prolonged time spent lying flat, so reflux becomes almost inevitable in early infancy. [1]
Whether reflux harms depends on what happens to the refluxed material and how the oesophagus defends itself. Prolonged acid contact overwhelms mucosal defence and produces oesophagitis, pain, bleeding, and, over years, stricture. The more feared pathway is aspiration, where refluxed fluid breaches the larynx and seeds the airway, driving recurrent pneumonia or worsening chronic lung disease — a risk that is greatest in children with impaired airway protection from neurological injury. [1] [7]
Clinical Presentation
The classic infant presentation is one every parent recognises: a well, thriving baby who brings up small amounts of milk after feeds, often without any distress and sometimes looking entirely content afterwards. The regurgitation is effortless, the feeding is normal, the weight tracks the centiles, and there are no red flags. This is physiologic reflux, and recognising it confidently is the first and most valuable skill. [1] [8]
The features that signal disease are the ones that should change your plan. In infants these include faltering growth despite adequate intake, feed refusal or distressed feeding, haematemesis or occult blood with anaemia, and recurrent respiratory events. In older children the picture shifts toward the adult symptoms of heartburn, epigastric pain, regurgitation, and, occasionally, dysphagia. Any one of these moves the child from the reassure column to the assess-and-treat column. [1]
Reflux is over-blamed for two symptom clusters in particular, and both deserve scepticism. Unexplained crying, irritability, and back-arching in an otherwise well infant are rarely caused by acid reflux, and randomised trials show they do not respond to acid suppression. Apparent life-threatening events, apnoea, and cough are similarly attributed to reflux far more often than the evidence supports. Naming reflux as the cause of these symptoms without proof is the commonest route to inappropriate treatment. [5] [2]
Differential Diagnosis
The differential of the vomiting or regurgitating child is long, and the discipline is to hold the dangerous causes in mind before settling on reflux. The most urgent mimic is intestinal obstruction, whose signature is bilious vomiting — malrotation with volvulus, atresia, intussusception, and incarcerated hernia can all present this way, and missing them courts catastrophe. Pyloric stenosis, with projectile vomiting and hypochloraemic hypokalaemic alkalosis, is the classic surgical mimic of the first weeks. [1]
The medical mimics are just as important. Cow's milk protein allergy is the great imitator, producing regurgitation, vomiting, irritability, eczema, and blood or mucus in the stool, and it responds to an extensively hydrolysed or amino-acid formula. Eosinophilic oesophagitis presents with dysphagia, food impaction, and reflux-like symptoms that fail to respond to acid suppression. Sepsis, raised intracranial pressure, urinary tract infection, and inborn errors of metabolism all cause vomiting and must not be labelled reflux. [1]
The rule that keeps children safe is simple: in any child who is not thriving, or who has bilious, projectile, or bloody vomit, or whose symptoms start late or persist beyond infancy, reflux is a diagnosis of exclusion rather than the default. The commonest error in paediatric gastroenterology is treating one of these mimics as reflux and delaying the real diagnosis. [1]
Clinical & Bedside Assessment
Begin with the growth chart, because it is the single most powerful discriminator between physiologic reflux and disease. A child whose weight, length, and head circumference track the centiles, who feeds with enthusiasm and develops normally, almost certainly has physiologic reflux. Faltering growth changes everything — it is a red flag that mandates assessment and shifts the child into the GORD category regardless of how effortless the regurgitation appears. [1]
Take a focused history of the reflux itself. Ask about the frequency, volume, force, timing, and colour of the vomit, and specifically whether it is ever green, which is obstruction. Probe for pain, feed refusal, and arching, and ask directly about respiratory symptoms — cough, wheeze, recurrent pneumonia — and about the timing of any events relative to feeds. A history of a contented, growing baby with small effortless possets describes physiologic reflux; a history of distress, weight loss, or breathing trouble describes disease. [1] [8]
Examine the child with the differential in mind. Plot the growth, feel the abdomen for masses and hernias, inspect any vomit for bile or blood, assess hydration and perfusion, and look for the atopic features and neurological signs that point to a mimic. A structured symptom diary or a validated questionnaire adds objectivity, but no scoring tool reliably distinguishes GOR from GORD, so clinical judgement remains the arbiter. [1]
Investigations
The governing principle is that most reflux needs no tests at all. The diagnosis of physiologic reflux is clinical — a thriving infant with effortless regurgitation and no red flags is diagnosed at the bedside and reassured, not scoped or imaged. Investigation is reserved for the child with red flags, with atypical or extra-oesophageal features, or in whom the diagnosis is genuinely uncertain, and it is always targeted to a specific question. [1]
When investigation is warranted, each test answers a defined question. Upper gastrointestinal contrast series is not a test for reflux itself but the study that excludes anatomical obstruction and malrotation, and it is the first test in any bilious or projectile vomiter. Upper endoscopy with oesophageal biopsy is the test that confirms oesophagitis, diagnoses eosinophilic oesophagitis, and justifies long-term acid suppression, and it should precede committing a child to indefinite treatment. [1]
Oesophageal pH monitoring and combined pH-impedance quantify the burden of acid and non-acid reflux and can establish a temporal association with symptoms, but they are specialist tools for complex, refractory, or extra-oesophageal cases rather than routine practice. High-resolution manometry adds value when a motility disorder or achalasia is suspected. An empirical proton-pump-inhibitor trial is not a valid diagnostic test in infants and should not be used to prove that reflux is causing crying or apnoea. [1] [2]
Management — Resuscitation
True emergencies in reflux are uncommon, and when they occur they are surgical, respiratory, or metabolic rather than problems of acid. A child who presents with bilious vomiting, abdominal distension, or signs of obstruction needs intravenous access, fluid resuscitation, a nasogastric tube on free drainage, and urgent surgical review with contrast imaging — not anti-reflux therapy. Malrotation with volvulus can infarct the midgut within hours, so time spent assuming reflux is time the bowel is ischaemic. [1]
The child who has aspirated and presents with respiratory distress needs the airway supported, oxygen titrated to saturation, and a chest radiograph to define the infiltrate. Treat aspiration pneumonitis supportively and add antibiotics only when bacterial pneumonia or sepsis is suspected. Once the child is stable the reflux question returns, but resuscitation and the search for the precipitant come first. [1] [7]
The child with severe dehydration or electrolyte derangement from persistent vomiting needs fluid and electrolyte correction before the cause is pursued. Correct hypoglycaemia, restore intravascular volume, and check the gas and electrolytes — pyloric stenosis hides in the hypochloraemic hypokalaemic alkalosis, and an inborn error of metabolism hides in an unexplained acidosis. Stabilise first, then diagnose. [1]
Management — Definitive & Stepwise
Definitive management is a ladder, and the first rung is the one most often skipped — reassurance and conservative measures. For the thriving infant with physiologic reflux, explain to the family that reflux is normal, expected, and self-limiting, and that it resolves as the child sits, walks, and takes solids. Over-investigation and over-treatment cause more harm than the reflux itself, and a confident, calm explanation is genuinely the treatment. [1] [6]
The conservative measures form the foundation and are supported by systematic review. Feed the infant smaller volumes more frequently to reduce gastric distension, wind carefully, and keep the child upright after feeds; avoid overfeeding, which is common and easily corrected. In the breastfed infant support continued breastfeeding, and in the formula-fed infant review the volume and preparation. These simple measures move the needle for most families without any drug at all. [6] [1]
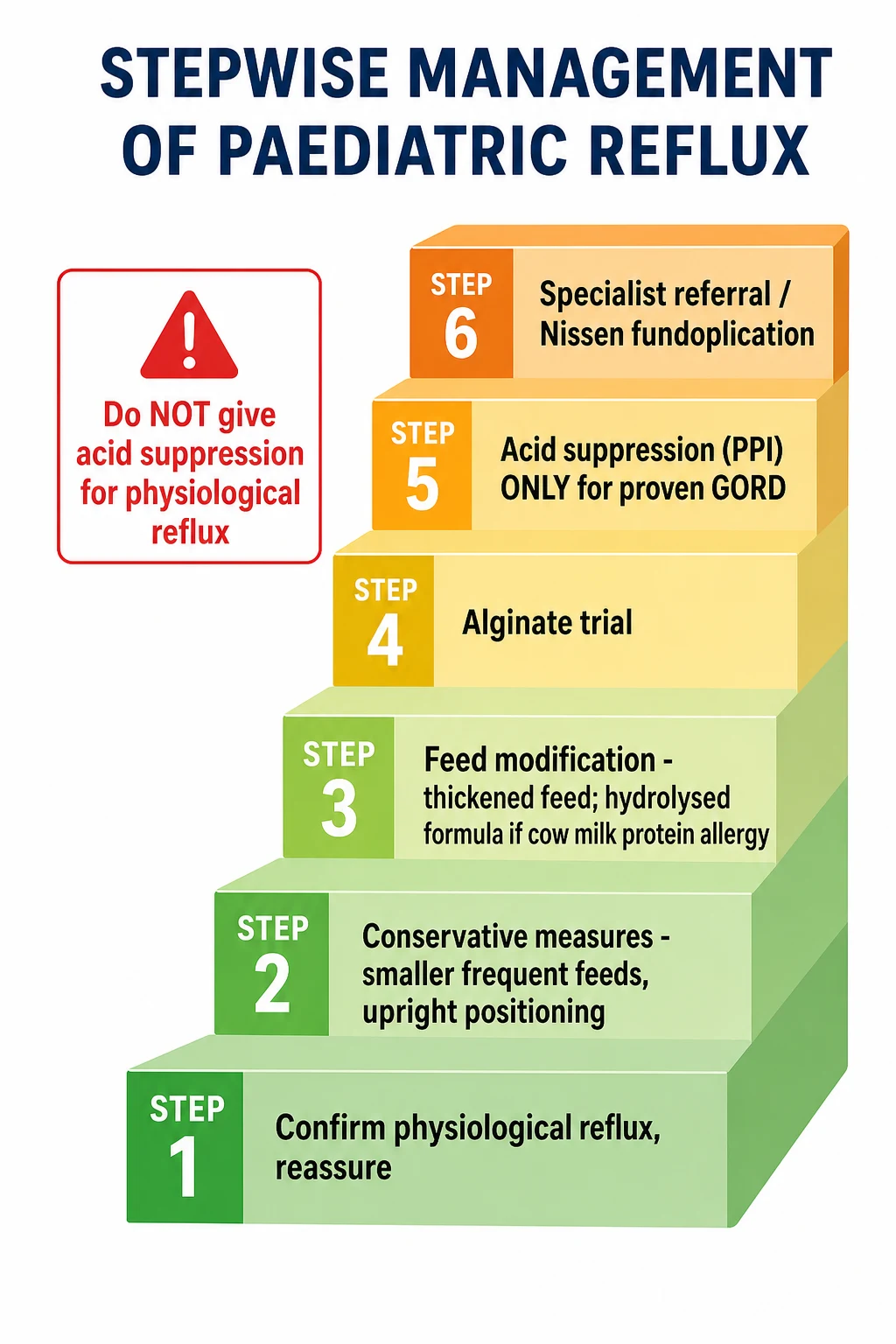
Stepwise management of paediatric reflux
Confirm physiologic reflux versus disease — exclude red flags and mimics; reassure if thriving
Conservative measures — smaller frequent feeds, avoid overfeeding, upright positioning, careful winding
Feed modification — thickened or anti-regurgitation feed; a 2 to 4 week trial of extensively hydrolysed formula if cow milk protein allergy is suspected
Alginate trial for persistent troublesome symptoms — reassess response and stop if ineffective
Acid suppression (PPI first line, H2-receptor antagonist alternative) for proven oesophagitis or a time-limited trial in older children with typical GORD
Refer to paediatric gastroenterology or surgery for red flags, refractory disease, or consideration of Nissen fundoplication
Feed modification is the next step when conservative measures fall short. A thickened or anti-regurgitation feed reduces visible regurgitation, though its effect on distress and complications is modest. Where cow's milk protein allergy is plausible, a two-to-four-week trial of an extensively hydrolysed formula, or an amino-acid formula if symptoms persist, is both diagnostic and therapeutic and should be tried before any acid-suppressing drug in the vomiting, atopic, or unsettled infant. [1] [6]
Pharmacotherapy is the step that demands the most restraint. Alginates, which form a raft over the gastric contents, are the one agent with a reasonable evidence base for short-term symptom relief and are worth a defined trial when conservative measures fail. Proton-pump inhibitors and H2-receptor antagonists heal oesophagitis and relieve typical heartburn, so they are appropriate for proven GORD and for a time-limited trial in older children with classic symptoms. They should not be prescribed for infant crying, arching, or apnoea, where placebo-controlled trials show no benefit and real harm. Prokinetics such as domperidone lack a favourable balance of efficacy and cardiac safety and are not recommended for routine use. [5] [3] [10]
Surgery, almost always a Nissen fundoplication, is reserved for the child with severe, refractory GORD — recurrent aspiration, life-threatening events, oesophagitis unresponsive to maximal medical therapy, or dependence that cannot be weaned — most often in the context of neurodisability or repaired oesophageal atresia. It is a specialist decision that follows a thorough work-up, not a treatment for physiologic reflux, and it carries its own morbidity of dysphagia, gas-bloat, and recurrence. [1]
Specific Subtypes & Scenarios
The child with neurodisability is the scenario where GORD does most of its harm. Impaired airway protection, spasticity, scoliosis, and gastrostomy feeding make reflux frequent, aspiration silent, and oesophagitis severe, so these children genuinely need investigation, often need long-term acid suppression, and are the group most likely to come to fundoplication. Their reflux is disease, not physiology, and their care belongs with a multidisciplinary team. [1]
The unsettled, crying infant is the scenario that generates the most reflexive prescribing. Persistent crying, back-arching, and feed-time distress are attributed to acid reflux, yet a placebo-controlled trial of lansoprazole in symptomatic infants showed no benefit over placebo and more lower respiratory infections in the treated group. The correct response is to reassure, exclude cow's milk protein allergy, optimise feeding, and resist the drug. [5] [2]
The preterm infant is a distinct group with its own evidence. Reflux is frequent, aspiration risk is real, and the temptation to blame apnoea on reflux is strong, but a Cochrane review found insufficient evidence that proton-pump inhibitors are safe and effective in preterm infants with GORD. Management is conservative and feeding-focused, and acid suppression is reserved for proven oesophagitis given the heightened infection and necrotising-enterocolitis concerns in this population. [11] [7]
The older child and adolescent presenting with heartburn, epigastric pain, and regurgitation approach the adult pattern of GORD. Here a time-limited trial of a proton-pump inhibitor alongside lifestyle advice — weight management, avoiding late meals, and reducing caffeine — is reasonable, with endoscopy for alarm features, dysphagia, or failure to respond, and always with a plan to reassess and stop. [1]
Complications & Pitfalls
The complications of untreated GORD are the reason the diagnosis matters. Persistent acid contact produces oesophagitis, stricture, anaemia from occult bleeding, and, very rarely in children, Barrett's oesophagus. Recurrent aspiration causes pneumonia, worsens chronic lung disease, and in the extreme leads to bronchiectasis. Feed refusal and the resulting faltering growth compound all of these, as the child avoids feeding to escape the pain. [1]
The greater harm in ordinary practice, however, comes from over-treatment, and modern evidence has made it prominent. Proton-pump inhibitors in children are associated with an increased risk of gastrointestinal and respiratory infection, with a signal toward necrotising enterocolitis in preterm infants, and with a small increase in fracture risk on prolonged use. None of this harm buys any benefit in physiologic reflux, which is why every guideline urges restraint. [2] [11]
The pitfalls cluster around a failure to distinguish. The first is calling a surgical emergency reflux — the bilious or projectile vomiter sent home with an antacid who returns in shock. The second is attributing crying, apnoea, or cough to reflux and prescribing acid suppression instead of finding the real cause. The third is the reflexive proton-pump inhibitor for physiologic posseting, which trades no benefit for real harm. The fourth is starting acid suppression and never stopping it, so a self-limiting condition becomes years of unnecessary medication. [1] [2]
Prognosis & Disposition
The prognosis for physiologic reflux is excellent, and saying so with conviction is part of the treatment. The great majority of infants resolve by twelve to eighteen months as they adopt upright posture, take solid food, and the anti-reflux barrier matures, and one-year follow-up of symptomatic infants confirms this benign trajectory. Parents who understand that reflux is developmental and self-limiting are far less likely to seek unnecessary investigation and treatment. [9] [1]
For the child with genuine GORD the outlook depends on the underlying condition. A previously well older child with reflux oesophagitis usually responds to a defined course of acid suppression and lifestyle change, whereas the child with neurodisability or repaired oesophageal atresia may need long-term management and occasionally surgery. The disposition is to treat for a defined period, monitor growth and symptoms, and escalate only when red flags or refractory disease appear. [1]
Most children with reflux are managed entirely in primary care or general paediatric clinic and never need a specialist. Discharge or reassurance is appropriate for the thriving infant with a clear safety-net explanation of the red flags that should prompt review — bile-stained vomit, forceful or projectile vomiting, faltering growth, haematemesis, or respiratory distress. Any child started on an acid-suppressing drug needs a documented plan to review and wean it, because unmonitored, indefinite treatment is the avoidable harm. [1] [2]
Special Populations
Children with neurodisability carry the most severe and persistent GORD and the highest aspiration risk, and they are the population most likely to need endoscopy, long-term acid suppression, and fundoplication. Their care is shared with gastroenterology, surgery, respiratory, and feeding teams, and the general paediatrician's role is to recognise the severity, protect nutrition, and refer early rather than cycle through empirical drugs. [1]
Preterm infants and those with chronic lung disease or repaired oesophageal atresia are a second high-stakes group. Reflux is frequent, aspiration risk is real, and the evidence for acid suppression is weak, so management is conservative and feeding-focused with acid suppression reserved for proven oesophagitis. The heightened infection and necrotising-enterocolitis concerns in the preterm make restraint especially important. [11] [7]
The atopic infant is the population most often mislabelled as reflux. The combination of vomiting, eczema, irritability, and blood or mucus in the stool warrants a trial of extensively hydrolysed or amino-acid formula, which is both diagnostic and therapeutic. Recognising cow's milk protein allergy prevents months of ineffective acid suppression and treats the real cause. [1]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric reflux has moved decisively toward restraint. The joint NASPGHAN and ESPGHAN 2018 clinical practice guidelines remain the international standard: they define GORD by troublesome symptoms and complications, place conservative measures first, restrict acid suppression to proven or strongly suspected disease, and explicitly discourage empirical proton-pump-inhibitor trials in infants. [1]
The pharmacological trial data are sobering for those who prescribe freely. A large multicentre, placebo-controlled trial of lansoprazole in symptomatic infants found no benefit over placebo and a signal of harm, a systematic review concluded that proton-pump-inhibitor efficacy for infant GORD is unproven, and a Cochrane review of pharmacological treatment reached the same conclusion. A separate Cochrane review found insufficient evidence for the safety and efficacy of proton-pump inhibitors in preterm infants. [5] [3] [2] [11]
The non-pharmacological evidence points the other way. A systematic review of non-pharmacological interventions supports feed modification, positioning, and thickening as effective and safe first-line measures, and alginate has modest short-term benefit that earns it a place ahead of acid suppression. The consistent message is that the ladder should be climbed slowly, with drugs near the top rather than the bottom. [6] [4]
Exam Pearls
The facts that earn marks are few and worth memorising cold. Reflux is physiologic and effortless, GORD is reflux with troublesome symptoms or complications, and the discriminator is the thriving child versus the faltering one. Bilious vomiting is never reflux, management is conservative first, and acid suppression is reserved for proven disease and always time-limited. Cow's milk protein allergy is the mimic to exclude before any drug. [1] [6]
The pharmacology point that separates a pass from a distinction is the trial evidence: proton-pump inhibitors do not improve crying, arching, or apnoea in infants and carry real harm, alginate has modest short-term benefit, and prokinetics such as domperidone are not recommended for routine use. The natural-history data — daily regurgitation in roughly half of four-month-olds resolving in the great majority by one year — is the number examiners love and the reason restraint is right. [5] [8] [9]
References
- [1]Rosen R, Vandenplas Y, Singendonk M, et al Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr, 2018.PMID 29470322
- [2]Tighe MP, Andrews E, Einhorn C, et al Pharmacological treatment of gastro-oesophageal reflux in children. Cochrane Database Syst Rev, 2023.PMID 37635269
- [3]van der Pol RJ, Smits MJ, van Wijk MP, et al Efficacy of proton-pump inhibitors in children with gastroesophageal reflux disease: a systematic review. Pediatrics, 2011.PMID 21464183
- [4]Salvatore S, Ripepi A, Huysentruyt K, et al The Effect of Alginate in Gastroesophageal Reflux in Infants. Paediatr Drugs, 2018.PMID 30182358
- [5]Orenstein SR, Hassall E, Furmaga-Jablonska W, et al Multicenter, double-blind, randomized, placebo-controlled trial assessing the efficacy and safety of proton pump inhibitor lansoprazole in infants with symptoms of gastroesophageal reflux disease. J Pediatr, 2009.PMID 19054529
- [6]Banderali G, Mameli C, Bozzola E, et al Efficacy and safety of non-pharmacological interventions for gastroesophageal reflux and gastroesophageal reflux disease in children: a systematic review. Ital J Pediatr, 2026.PMID 42098776
- [7]Eichenwald EC, Committee on Fetus and Newborn Diagnosis and Management of Gastroesophageal Reflux in Preterm Infants. Pediatrics, 2018.PMID 29915158
- [8]Nelson SP, Chen EH, Syniar GM, et al Prevalence of symptoms of gastroesophageal reflux during infancy. A pediatric practice-based survey. Pediatric Practice Research Group. Arch Pediatr Adolesc Med, 1997.PMID 9193240
- [9]Nelson SP, Chen EH, Syniar GM, et al One-year follow-up of symptoms of gastroesophageal reflux during infancy. Pediatric Practice Research Group. Pediatrics, 1998.PMID 9832595
- [10]Puoti MG, Assa A, Benninga M, et al Drugs in Focus: Domperidone. J Pediatr Gastroenterol Nutr, 2023.PMID 37159421
- [11]King E, Horn D, Gluchowski N, et al Safety and efficacy of proton pump inhibitors in preterm infants with gastroesophageal reflux disease. Cochrane Database Syst Rev, 2025.PMID 40066936