Paeds · gastroenterology-hepatology-and-nutrition
Gastrointestinal bleeding
Also known as GI bleed · Haematemesis · Melaena · Haematochezia · Rectal bleeding in children · Upper gastrointestinal bleeding · Lower gastrointestinal bleeding · Meckel diverticulum bleed · Intussusception · Variceal bleeding
Fellowship guide to gastrointestinal bleeding in children, built around the upper versus lower split at the ligament of Treitz and the way the differential shifts with age. The page works from haematemesis, coffee-ground vomit, melaena and haematochezia through resuscitation, the Apt test, Meckel scan and endoscopy, and the age-anchored causes from swallowed maternal blood and necrotising enterocolitis in the neonate to intussusception and Meckel diverticulum in the infant, juvenile polyps and varices in the child, and inflammatory bowel disease in the adolescent.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a toddler brought in screaming and clutching his belly, then passing a motion streaked with bright red blood, and a teenager who vomits what looks like coffee grounds. Both have gastrointestinal bleeding, yet the two stories point to completely different parts of the gut and demand different first moves. Gastrointestinal bleeding is any loss of blood from the alimentary tract from the mouth to the anus, and in children the colour of the blood, the age of the child and the stability of the circulation together set the direction of the whole assessment. [1] [3]
The single most useful anatomical fork is whether the bleeding lies above or below the ligament of Treitz, the fibromuscular band at the duodenojejunal flexure. Bleeding proximal to it is an upper gastrointestinal bleed and tends to appear as haematemesis, the vomiting of fresh red blood, or coffee-ground vomit, or as melaena, the black tarry stool produced when blood is digested as it transits the gut. Bleeding distal to the ligament is a lower gastrointestinal bleed and usually appears as haematochezia, bright red or maroon blood passed per rectum. [1] [4]
Most childhood gastrointestinal bleeding is minor and self-limiting, yet a small minority is life-threatening, so the discipline is to assess for haemodynamic compromise first in every case and only then reason about the likely cause. The age of the child narrows the differential powerfully, because a neonate, an infant, a school-age child and an adolescent each carry a recognisably different set of causes for the same symptom. Holding the upper versus lower split and the age band together is what turns a vague presenting complaint into a tractable clinical problem. [1] [2]
Classification
Begin every bleed by placing it on two axes at once: the anatomical level relative to the ligament of Treitz, and the age of the child. The level decides whether you expect haematemesis or melaena above the line, and haematochezia below it, while the age decides which causes are statistically likely within that level. The classification figure sets these axes out as a grid, with the typical causes for each age and level in the cells. [1] [3]
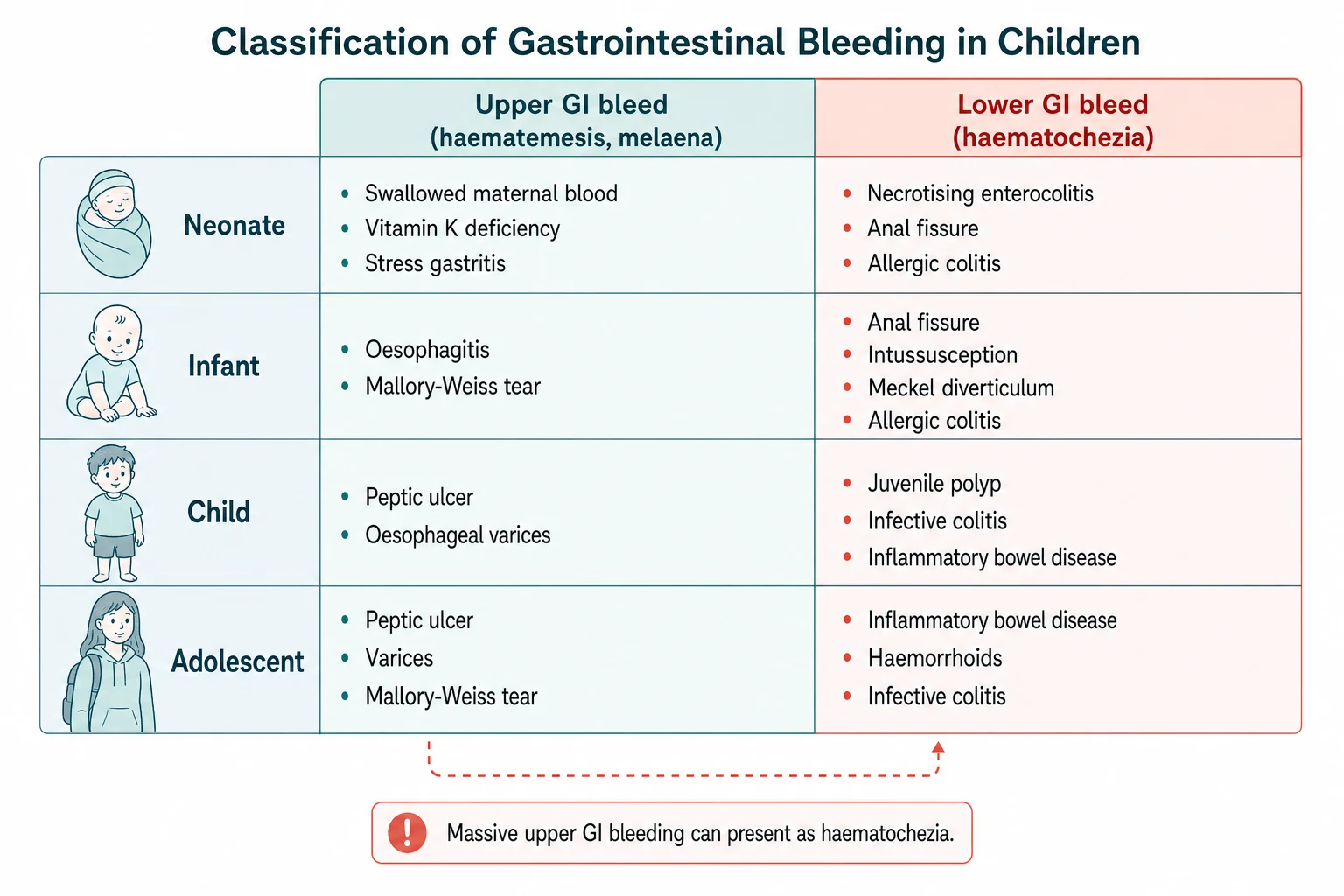
Within the upper tract the causes shift with age. In the neonate, swallowed maternal blood from delivery or a cracked nipple, stress gastritis and vitamin K deficiency bleeding dominate. In the infant and younger child, reflux oesophagitis and Mallory-Weiss tears from forceful vomiting appear, and in the older child and adolescent peptic ulcer disease, oesophageal varices from portal hypertension and NSAID-related gastritis take over. The age-specific review of upper gastrointestinal bleeding confirms this progression. [3] [12]
The lower tract has its own age fingerprint. The neonate brings necrotising enterocolitis, allergic colitis and anal fissure. The infant adds intussusception, Meckel diverticulum and cow's milk allergic colitis. The school-age child most often bleeds from a solitary juvenile polyp, infective colitis or the onset of inflammatory bowel disease, and the adolescent adds haemorrhoids to the inflammatory and infectious causes. The lower gastrointestinal bleeding review details this distribution. [4] [7]
Upper GI bleed
- Proximal to the ligament of Treitz
- Haematemesis (fresh red or coffee-ground) and melaena
- Neonate: swallowed maternal blood, vitamin K deficiency, stress gastritis
- Older child: peptic ulcer, varices, oesophagitis
Lower GI bleed
- Distal to the ligament of Treitz
- Haematochezia, bright red or maroon blood per rectum
- Infant: intussusception, Meckel diverticulum, anal fissure
- Child and adolescent: juvenile polyp, IBD, infective colitis
Obscure bleed
- Persistent bleeding with negative endoscopy and colonoscopy
- Small bowel source such as Meckel diverticulum or vascular malformation
- Capsule endoscopy and tagged red cell study localise the site
- May require angiography or surgery for refractory haemorrhage
Epidemiology & Risk Factors
Gastrointestinal bleeding is a common reason for paediatric presentation, and the reassuring fact is that the majority of episodes are small and self-limiting. Anal fissure alone accounts for a large share of lower tract bleeding in infants and toddlers, and swallowed maternal blood explains many apparently alarming neonatal bleeds. The danger lies in the minority who bleed from a surgical or vascular cause, so epidemiology is used to raise pre-test probability rather than to lower vigilance. [1] [4]
Age is the strongest epidemiological lever. Intussusception peaks between six months and two years of age, with a classic presentation around five to nine months, and Meckel diverticulum most often declares itself before the age of two. Juvenile polyps cluster between two and five years, while inflammatory bowel disease and peptic ulcer disease rise through the school-age years into adolescence. Knowing the age band therefore sharpens the differential before any test returns. [4] [7]
Specific risk factors mark out the higher-risk child. Liver disease, prior umbilical catheterisation or neonatal thrombosis point to portal hypertension and varices, while NSAID or corticosteroid use, anticoagulation and a bleeding diathesis raise the chance of upper tract haemorrhage. A family history of inflammatory bowel disease, polyposis or bleeding disorders, and immunocompromise, all shift the differential and should be asked for directly. [2] [8]
Pathophysiology
The appearance of blood is not arbitrary, it is a record of what the blood has travelled through. When blood pools in the stomach, gastric acid and pepsin denature it into the dark granular coffee-ground appearance. When it transits the length of the gut, digestive enzymes and bacterial action turn it into the black, sticky, foul-smelling melaena, which means the source is high even though it exits low. Fresh red blood per rectum, by contrast, has spent little time in the gut and usually signals a lower tract source, unless a massive upper bleed has rushed through too quickly to be digested. [1] [3]
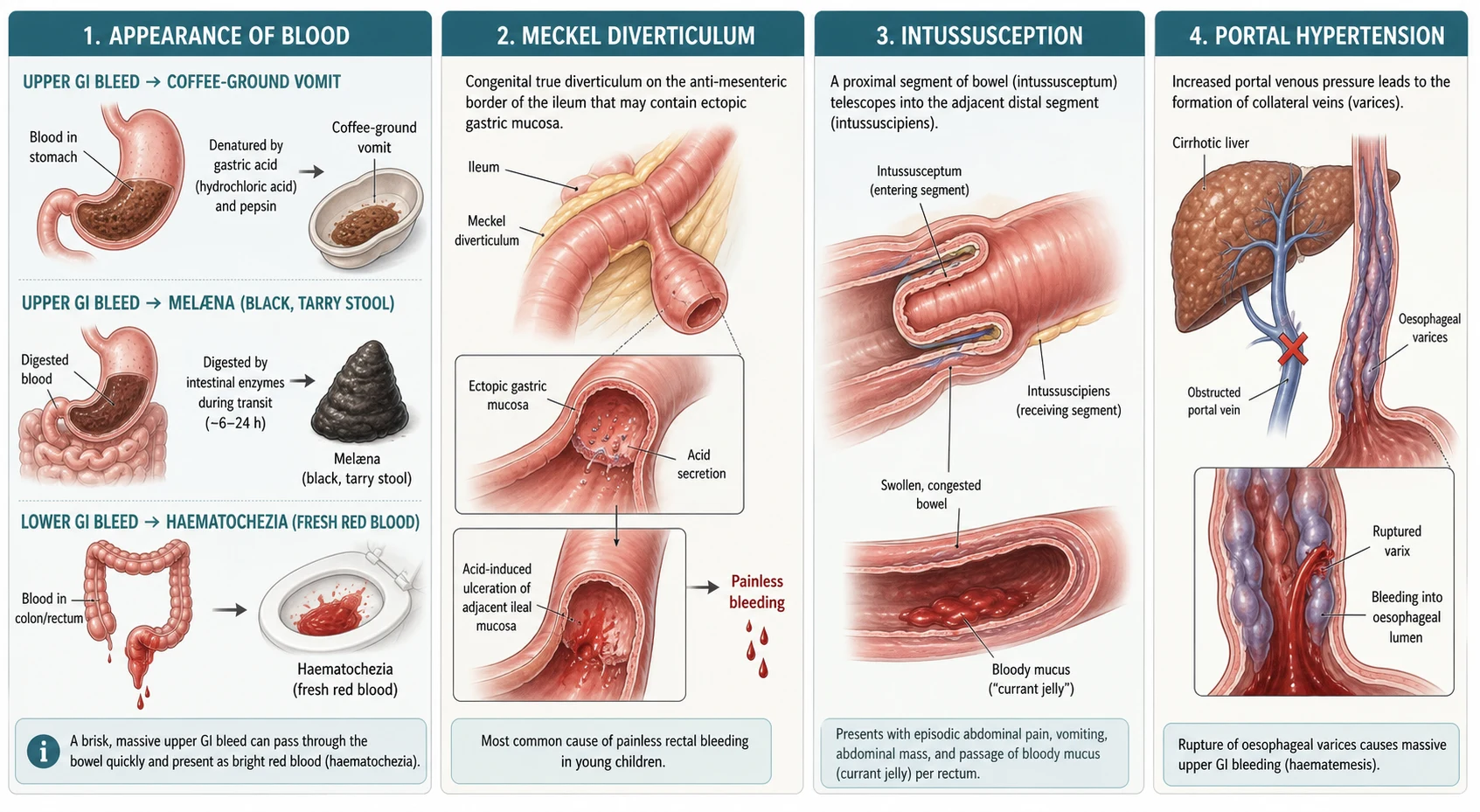
Several specific mechanisms recur in the paediatric differential and deserve to be held as mental models. A Meckel diverticulum is a congenital true diverticulum on the anti-mesenteric border of the ileum, a remnant of the vitelline or omphalomesenteric duct, and when it harbours ectopic gastric mucosa that mucosa secretes acid, ulcerates the adjacent ileal wall and produces painless, often massive bleeding. Intussusception telescopes a proximal segment into a distal one, venous congestion and then ischaemia follow, and the bowel weeps bloody mucus into the lumen. Portal hypertension, whether from extrahepatic portal vein obstruction or cirrhosis, opens collateral oesophageal and gastric varices that can rupture and bleed catastrophically. [5] [8]
The rule of twos anchors the Meckel mental model and is a favourite exam fact. A Meckel diverticulum is present in about two per cent of the population, sits roughly two feet from the ileocaecal valve, is around two inches long, tends to present clinically before the age of two, and contains two common types of ectopic tissue, gastric and pancreatic. Holding this rule lets a candidate predict the diagnosis from a painless bleed in a young child and request the right scan. [5] [6]
Clinical Presentation
The presentation divides first by stability and then by site. A child with major haemorrhage shows tachycardia, pallor, cool peripheries, prolonged capillary refill, oliguria and altered consciousness, and these signs demand resuscitation ahead of diagnosis. A child with minor bleeding is typically well and the bleed is found on the nappy, the toilet paper or in vomit, and the task is to localise the source safely. Distinguishing these two groups in the first minute is the most important triage decision in the topic. [1] [2]
Haematemesis presents as the vomiting of bright red blood or dark coffee-ground material, and points to an upper tract source. Melaena is the passage of black, tarry, foul-smelling stool and similarly indicates bleeding proximal to the ligament of Treitz, though a right-sided colonic bleed can occasionally mimic it. Haematochezia is bright red or maroon blood passed per rectum, with or without stool, and most often signals a lower tract source, with the caveat that a very brisk upper bleed can present the same way. [1] [3]
The accompanying symptoms refine the cause. Colicky abdominal pain, vomiting and a palpable sausage-shaped mass in an infant point to intussusception. Painless bright bleeding in a well toddler points to a juvenile polyp or Meckel diverticulum. Fever, diarrhoea and abdominal pain suggest infective or inflammatory colitis. A palpable purpuric rash on the lower limbs and buttocks with abdominal pain marks IgA vasculitis, formerly Henoch-Schönlein purpura, and a child with known liver disease who vomits blood has presumed variceal bleeding. [4] [11]
Differential Diagnosis
Build the differential from the site and the age together, because either alone is too broad to be useful. For an upper tract bleed in a neonate, think first of swallowed maternal blood, then stress gastritis and vitamin K deficiency bleeding. In an older child or adolescent, weigh peptic ulcer disease, oesophagitis, Mallory-Weiss tear and oesophageal varices. For a lower tract bleed in an infant, intussusception, Meckel diverticulum, anal fissure and allergic colitis lead the list, while in a school-age child a juvenile polyp, infective colitis and inflammatory bowel disease come to the fore. [1] [3]
Painless bright bleed
- Juvenile polyp in a two to five year old
- Meckel diverticulum in a toddler
- Often well-looking child with red blood on stool
- Endoscopy or Meckel scan to localise
Painful bleed with colic
- Intussusception in an infant
- Drawing up legs, vomiting, sausage mass
- Currant-jelly stool is a late ischaemic sign
- Ultrasound target sign, urgent enema reduction
Bleed with systemic illness
- Infective colitis with fever and diarrhoea
- Inflammatory bowel disease with weight loss
- IgA vasculitis with palpable purpura
- Haemolytic uraemic syndrome with oliguria
A few red-flag diagnoses must never be missed because they progress quickly. In the neonate, necrotising enterocolitis and malrotation with midgut volvulus can present with blood in the stool and deteriorate to shock and perforation within hours. In any age group, variceal bleeding from portal hypertension can be torrential, and a coagulopathic or anticoagulated child can bleed from a trivial lesion. The discipline is to actively exclude these dangerous causes rather than to settle on a benign label first. [2] [8]
The minor causes still need to be named and distinguished. An anal fissure produces a small streak of bright blood on the outside of a hard stool and is the commonest cause of minor rectal bleeding in infants. Swallowed maternal blood in a neonate is benign but must be confirmed, not assumed. Allergic, cow's milk protein colitis gives blood-streaked stool in an otherwise well infant and settles with dietary elimination. Each benign cause is a diagnosis of reassessment, reached only after the dangerous ones have been considered. [4] [10]
Clinical & Bedside Assessment
Run the assessment in parallel with resuscitation, because a bleeding child may need fluid while the history is taken. Begin with the airway, breathing and circulation, and judge the haemodynamic status from the heart rate, capillary refill, skin temperature, pulse volume and conscious level, remembering that blood pressure is a late and unreliable sign in children. Only once the child is stable, or resuscitation is under way, turn to the focused history and examination. [1] [2]
The history should capture the colour, volume and frequency of the bleeding, any associated abdominal pain, vomiting, diarrhoea or fever, and the child's weight trajectory. Ask specifically about NSAID or steroid use, anticoagulation, known liver disease, prior surgery, umbilical catheterisation in the neonatal period, and a family history of inflammatory bowel disease, polyposis or bleeding disorders. In a neonate, ask about vitamin K administration at birth and any maternal cracked nipples, since swallowed maternal blood is a key benign mimic. [3] [8]
Examine the abdomen for distension, tenderness, guarding and masses, checking every hernial orifice, and look for the sausage-shaped mass of intussusception in the right upper quadrant. Search for signs of chronic liver disease such as jaundice, spider naevi, palmar erythema and splenomegaly, and examine the skin for the palpable purpura of IgA vasculitis or the bruising of a coagulopathy. A gentle perianal and rectal inspection completes the bedside picture and often reveals a fissure immediately. [4] [11]
Investigations
Choose investigations by the suspected site and the stability of the child, and never let a test delay resuscitation in an unstable patient. The baseline bloods in any significant bleed are a full blood count, group and crossmatch, coagulation screen with prothrombin time and activated partial thromboplastin time, urea and electrolytes, liver function tests and a CRP. A raised urea relative to creatinine can hint at an upper tract source from digested blood, and a low haemoglobin with a high white count and acidosis signals major haemorrhage. [1] [2]
In the neonate with rectal bleeding, the Apt test is a quick and decisive first step when swallowed maternal blood is suspected. It distinguishes fetal from adult haemoglobin by alkali denaturation, because fetal haemoglobin resists alkali and stays pink while adult haemoglobin turns brown. A positive Apt test confirms maternal blood and closes a benign case, while a negative test sends the neonate down the surgical and haematological pathway. [1] [3]
Endoscopy is both diagnostic and therapeutic and is the reference test for upper gastrointestinal bleeding once the child is stable. Upper endoscopy identifies and treats oesophagitis, ulcers, Mallory-Weiss tears and varices through band ligation, sclerotherapy, adrenaline injection or clips. Colonoscopy evaluates lower tract bleeding when the child is stable and prepared, and capsule endoscopy and tagged red blood cell studies localise obscure small bowel sources. In a actively and massively bleeding unstable child, CT angiography can localise the site when endoscopy is not feasible, and surgery is reserved for refractory haemorrhage. [2] [6]
The bleeding child — the mnemonic SITE
Management — Resuscitation
Resuscitation follows one rule, stabilise the child before you chase the diagnosis, and never let imaging or endoscopy wait on a patient who is still bleeding and shocked. Keep the child nil by mouth, secure two large-bore intravenous cannulae, and take blood for a full count, group and crossmatch, coagulation and electrolytes at the moment of cannulation. Give oxygen to any child with shock or major blood loss, and warn the anaesthetic and surgical teams early. [1] [2]
Isotonic crystalloid bolus
Dose
10 to 20 mL per kg
Restore the circulation with aliquots of isotonic crystalloid, giving 10 to 20 mL per kg and reassessing the perfusion, heart rate and conscious level after each bolus. In ongoing major haemorrhage, move early to blood products, transfusing packed red cells when the child remains unstable after crystalloid or when the haemoglobin falls below 70 g/L in a stable child, with a higher threshold in the unstable or comorbid child. Correct any coagulopathy with vitamin K and fresh frozen plasma or platelets as guided by the coagulation screen, since a bleeding child who cannot clot will not stop bleeding. [2] [8]
For suspected variceal bleeding, start specific therapy during resuscitation. Give an intravenous proton-pump inhibitor, and use an octreotide infusion to reduce splanchnic and portal blood flow, since pharmacological control buys time for urgent endoscopic band ligation. In a child with chronic liver disease, give prophylactic broad-spectrum antibiotics, because infection worsens portal pressure and outcomes in cirrhotic bleeding. A Sengstaken-Blakemore or similar balloon tamponade is a temporary bridge to definitive endoscopy in uncontrolled variceal haemorrhage. [8] [2]
Management — Definitive & Stepwise
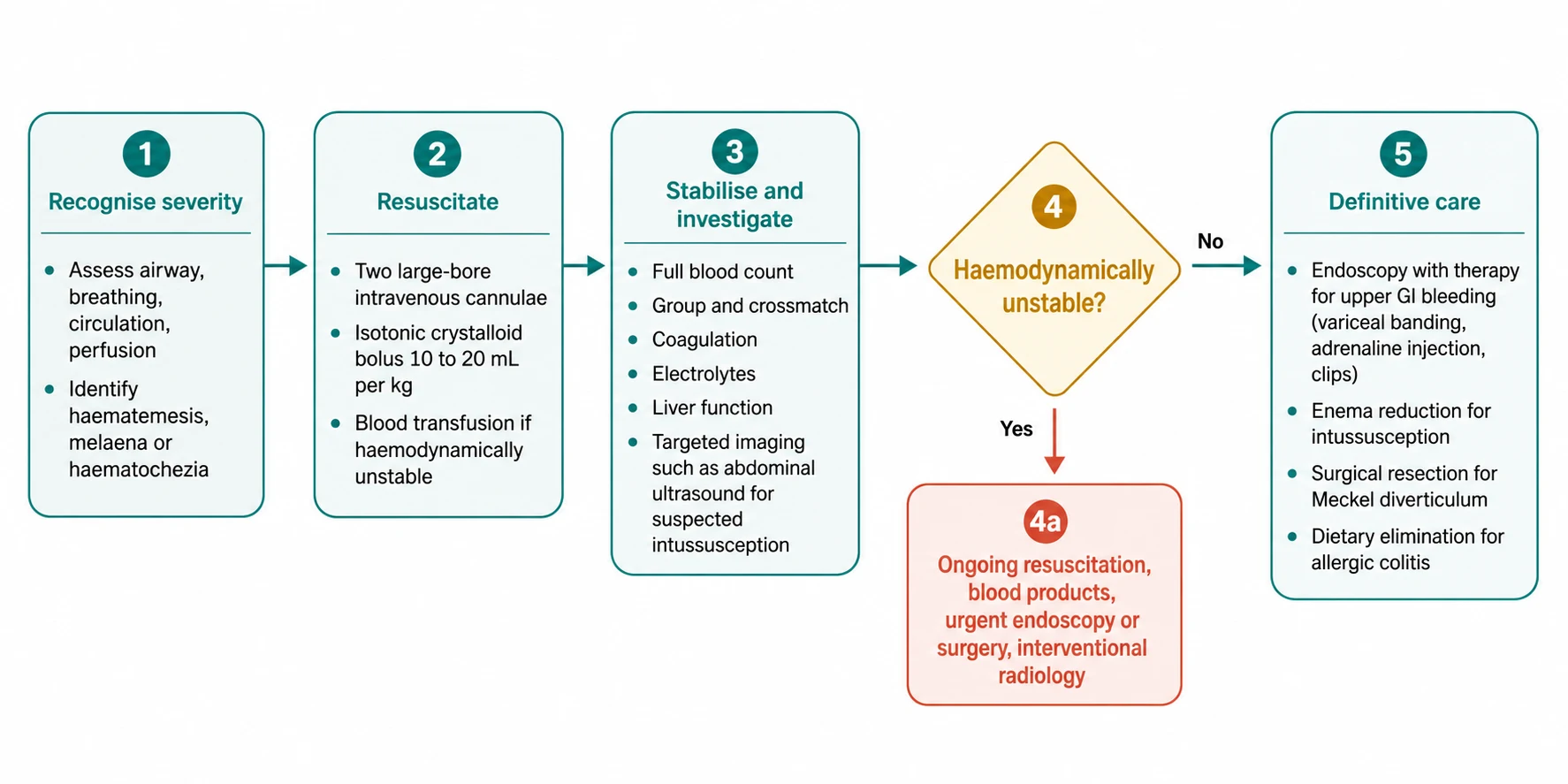
Once the child is stable, definitive care follows the suspected cause down a disciplined pathway. The management figure sets out the route from recognition and resuscitation, through stabilisation and investigation, to the decision point on stability and the definitive intervention for each cause. The principle is to resuscitate and localise in parallel, and to escalate to endoscopy, radiology or surgery the moment the bleeding is severe or refractory. [1] [2]
Upper tract bleeding is managed endoscopically wherever possible. Varices undergo band ligation or sclerotherapy, bleeding ulcers receive adrenaline injection with thermal or mechanical therapy, and oesophagitis is treated with acid suppression. Colonoscopy manages lower tract bleeding from polyps by snare polypectomy and diagnoses colitis, with the bowel prepared unless the bleed is too brisk to wait. Capsule endoscopy and double-balloon enteroscopy reach the small bowel for obscure sources, and refractory or unlocalised massive bleeding may need intra-arterial embolisation or surgery. [2] [7]
Cause-specific definitive treatment completes the picture. Intussusception is reduced by ultrasound-guided pneumatic or hydrostatic enema, with surgery for failed reduction, perforation or peritonitis. A bleeding Meckel diverticulum is resected surgically, with the segment of ileum bearing the diverticulum removed. Allergic colitis in the infant is treated by eliminating cow's milk protein from the diet, with resolution of the bleeding. Juvenile polyps are removed endoscopically, and inflammatory bowel disease is managed by the paediatric gastroenterology team with the appropriate medical therapy. [9] [10]
Specific Subtypes & Scenarios
Intussusception is the subtype every candidate must own. The classic infant is between six months and two years, presenting with episodic, drawing-up colicky pain, vomiting and eventually the passage of currant-jelly stool, though the bloody stool is a late sign of ischaemia and its absence never excludes the diagnosis. Ultrasound shows the target sign, and the first-line treatment is ultrasound-guided pneumatic or hydrostatic enema reduction, which succeeds in most stable children, with surgery reserved for failure or peritonitis. [9] [4]
The bleeding Meckel diverticulum is the classic cause of painless, often massive lower gastrointestinal bleeding in a young child. The diverticulum contains ectopic gastric mucosa that secretes acid and ulcerates the adjacent ileum, and the technetium-99m pertechnetate Meckel scan is the investigation of choice, though high-frequency ultrasound can help when the scan is negative. Definitive treatment is surgical resection of the diverticulum and the affected ileal segment. [5] [6]
Variceal bleeding in portal hypertension is the subtype where preparation saves lives. In children, extrahepatic portal vein obstruction is the commonest cause of portal hypertension and varices, more so than cirrhosis, so a child with variceal bleeding may have no chronic liver disease at all. Resuscitate, give an octreotide infusion and an intravenous proton-pump inhibitor, give antibiotics if cirrhotic, and arrange urgent endoscopy for band ligation, with balloon tamponade as a bridge in uncontrolled bleeding and a shunt or surgery for refractory cases. [8] [2]
IgA vasculitis, formerly Henoch-Schönlein purpura, is the systemic subtype to remember. A child with palpable purpura on the lower limbs and buttocks, abdominal pain and arthritis may develop gastrointestinal bleeding from submucosal haemorrhage, and rarely intussusception, which is typically ileoileal rather than ileocolic. Severe abdominal pain or a falling haemoglobin in a child with IgA vasculitis warrants urgent imaging, since intussusception in this setting often needs surgical rather than enema reduction. [11] [4]
Complications & Pitfalls
The complications flow from blood loss and from delay. Major haemorrhage causes hypovolaemic shock, tissue hypoperfusion and, if uncorrected, multiorgan failure and death. Chronic or recurrent bleeding causes iron deficiency anaemia and faltering growth, particularly in inflammatory bowel disease and allergic colitis. Intussusception that is not reduced in time progresses to bowel ischaemia, perforation and peritonitis, and a missed volvulus or necrotising enterocolitis in a bleeding neonate can cost the midgut. [1] [9]
The pitfalls cluster around underestimation and mislocalisation. The classic error is to be reassured by a normal early blood pressure and to under-resuscitate a tachycardic child who is still bleeding. A second is to attribute bright red rectal bleeding to a benign cause without a perianal exam or without considering a Meckel diverticulum or intussusception. A third is to assume that haematochezia always means a lower source, forgetting that a brisk upper bleed can present with red blood per rectum. A fourth is to accept swallowed maternal blood in a neonate without an Apt test, missing a surgical or haematological cause. [2] [3]
Prognosis & Disposition
Outcome depends on the cause and on the speed of resuscitation. Most childhood gastrointestinal bleeding is minor and resolves with the cause treated, and conditions such as anal fissure, allergic colitis and juvenile polyps have an excellent prognosis once identified. The dangerous causes, intussusception, volvulus, necrotising enterocolitis and variceal haemorrhage, carry a prognosis tied directly to the time to definitive treatment, so early recognition and transfer drive the outcome. [1] [9]
Disposition reflects the severity and the likely cause. A haemodynamically unstable child or one with suspected variceal or surgical bleeding needs a paediatric centre with gastroenterology, surgery and interventional radiology, often through a retrieval service with resuscitation continued throughout transfer. A stable child with a clearly benign cause, such as an anal fissure or a confirmed swallowed maternal blood, can be managed with clear safety-netting in the community. Any child with ongoing or recurrent bleeding, uncertain diagnosis or systemic illness needs admission and observation. [2] [8]
Special Populations
The neonate is the population where the differential is most distinct and most time-critical. A neonate with blood in the stool may have necrotising enterocolitis, malrotation with midgut volvulus, Hirschsprung-associated enterocolitis, allergic colitis, anal fissure or vitamin K deficiency bleeding, and several of these deteriorate within hours. The Apt test, an abdominal radiograph, a careful surgical review and a coagulation screen are the early tools, and a well-looking neonate with rectal bleeding is still an emergency until these are complete. [1] [3]
Children with chronic liver disease and portal hypertension are at recurrent risk of variceal bleeding. They need primary prophylaxis with non-selective beta-blockers where tolerated, surveillance endoscopy, and a clear action plan for the family for any bleed. After a variceal bleed, secondary prophylaxis with band ligation and beta-blockade reduces recurrence, and a child with refractory bleeding may need a surgical or interventional shunt and assessment for transplant. [8] [2]
Immunocompromised children, including those on chemotherapy or after transplant, bleed from a different spectrum that includes neutropenic enterocolitis, graft-versus-host disease of the gut and opportunistic infection. They need early involvement of oncology or transplant teams alongside gastroenterology and surgery, and a low threshold for broad antimicrobial cover. Geography matters too, since a bleeding child in a rural or remote community may be hours from endoscopy or paediatric surgery, so early recognition, resuscitation and retrieval discussion are what protect the child during transfer. [1] [2]
Evidence, Guidelines & Regional Differences
The evidence base blends age-specific clinical reviews with imaging and endoscopic series. The diagnostic approach to gastrointestinal bleeding in children, the age-specific causes of upper bleeding and the lower gastrointestinal bleeding review together establish the age-anchored differential and the upper versus lower split. Management reviews detail the endoscopic and pharmacological options, while focused series refine the Meckel scan, ultrasound for intussusception and the treatment of portal hypertension. [1] [3]
Where evidence is softer, practice varies. The choice between pneumatic and hydrostatic enema reduction for intussusception, the role of capsule endoscopy in obscure bleeding, and the thresholds for transfusion in the stable child all show regional variation, though the principles of resuscitation first and endoscopic therapy for upper bleeding are consistent. The management of juvenile polyposis syndrome, including surveillance intensity and the threshold for colectomy, is guided by specialist protocols that weigh cancer risk against operative morbidity. [7] [9]
Regional practice is consistent in principle and variable in logistics. The rule that a bleeding child is assessed for haemodynamic compromise first, then localised by site and age, is universal, but access to paediatric endoscopy, interventional radiology and rapid retrieval differs between and within countries. In Australia and New Zealand, a child with major bleeding in a rural or Indigenous community may be far from a tertiary centre, so early resuscitation, nasogastric decompression where appropriate and prompt retrieval discussion are equity issues as much as clinical ones. [1] [2]
Exam Pearls
Hold one sentence above all others, the colour of the blood and the age of the child set the differential, and the stability of the circulation sets the urgency. State the reflex that follows, which is to resuscitate the unstable child with two large-bore cannulae and crystalloid boluses of 10 to 20 mL per kg before any imaging, then localise the bleeding by site and age, and escalate to endoscopy, radiology or surgery for the severe or refractory case. This answer covers both the marks and the patient. [1] [2]
Get the frequently tested facts exactly right. The ligament of Treitz divides upper from lower bleeding, melaena means a source proximal to it, and haematochezia usually means a lower source unless the upper bleed is brisk and massive. The Meckel scan uses technetium-99m pertechnetate to detect ectopic gastric mucosa, the rule of twos describes the Meckel diverticulum, and the target sign on ultrasound diagnoses intussusception. [5] [9]
The high-yield pairings do the work in a viva. An infant with colicky pain, vomiting and currant-jelly stool has intussusception reduced by enema. A toddler with painless bright rectal bleeding has a Meckel diverticulum shown on a Meckel scan. A school-age child with painless bleeding on the stool has a juvenile polyp removed at colonoscopy. A child with liver disease who vomits blood has variceal bleeding controlled by octreotide and band ligation. Always resuscitate before you image. [7] [8]
References
- [1]Piccirillo M; Pucinischi V; Mennini M; Strisciuglio C; et al Gastrointestinal bleeding in children: diagnostic approach. Ital J Pediatr, 2024.PMID 38263189
- [2]Novak I; Bass LM Gastrointestinal Bleeding in Children: Current Management, Controversies, and Advances. Gastrointest Endosc Clin N Am, 2023.PMID 36948753
- [3]Kocic M; Rasic P; Marusic V; Prokic D; et al Age-specific causes of upper gastrointestinal bleeding in children. World J Gastroenterol, 2023.PMID 38186684
- [4]Sahn B; Bitton S Lower Gastrointestinal Bleeding in Children. Gastrointest Endosc Clin N Am, 2016.PMID 26616898
- [5]Aboughalia HA; Cheeney SHE; Elojeimy S; Blacklock LC; et al Meckel diverticulum scintigraphy: technique, findings and diagnostic pitfalls. Pediatr Radiol, 2023.PMID 36323958
- [6]Hu Y; Wang X; Jia L; Wang Y; et al Diagnostic accuracy of high-frequency ultrasound in bleeding Meckel diverticulum in children. Pediatr Radiol, 2020.PMID 32076751
- [7]Dal Buono A; Gaiani F; Poliani L; Laghi L Juvenile polyposis syndrome: An overview. Best Pract Res Clin Gastroenterol, 2022.PMID 35988962
- [8]Grammatikopoulos T; McKiernan PJ; Dhawan A Portal hypertension and its management in children. Arch Dis Child, 2018.PMID 28814423
- [9]Vakaki M; Sfakiotaki R; Liasi S; Hountala A; et al Ultrasound-guided pneumatic reduction of intussusception in children: 15-year experience in a tertiary children's hospital. Pediatr Radiol, 2023.PMID 37665367
- [10]Yu MC; Tsai CL; Yang YJ; Yang SS; et al Allergic colitis in infants related to cow's milk: clinical characteristics, pathologic changes, and immunologic findings. Pediatr Neonatol, 2013.PMID 23445743
- [11]Su D; Yang M; Wang X; Li G; et al Risk factors for gastrointestinal bleeding in children with Henoch-Schönlein purpura. Front Pediatr, 2025.PMID 40336803
- [12]Ozdogan E; Caglayan LD; Mizikoglu O; Arikan C Upper Gastrointestinal Bleeding as the First Presentation of Eosinophilic Gastrointestinal Disease. JPGN Rep, 2020.PMID 37206599