Paeds · gastroenterology-hepatology-and-nutrition
Inflammatory bowel disease
Also known as Paediatric inflammatory bowel disease · Crohn disease in children · Ulcerative colitis in children · Paediatric IBD · Crohn's disease
Fellowship guide to inflammatory bowel disease in children and adolescents: the ESPGHAN revised Porto criteria for diagnosis, the distinction between Crohn disease and ulcerative colitis, the growth-centred clinical presentation, a pan-endoscopy diagnostic strategy, the paediatric activity indices (PCDAI and PUCAI), induction with exclusive enteral nutrition and corticosteroids, maintenance with immunomodulators and anti-TNF biologics, and the evidence-based management of acute severe colitis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A school-age child or teenager who presents with months of diarrhoea, abdominal pain, weight loss, and a fall in their growth centiles is the classic picture of paediatric inflammatory bowel disease. This is a group of chronic, relapsing, immune-mediated disorders of the gastrointestinal tract in which an inappropriate inflammatory response damages the gut, and in children the consequences for growth, puberty, and psychosocial development are as important as the bowel symptoms themselves. [1]
The two main subtypes are Crohn disease, which can affect any segment from mouth to anus with transmural and patchy inflammation, and ulcerative colitis, which is confined to the colonic mucosa in continuous fashion from the rectum. A third group, IBD-unclassified, is reserved for colitis that cannot be definitively categorised as either at the time of diagnosis. In children the distinction matters because it drives the choice of induction and maintenance therapy and shapes the long-term risk of surgery, cancer, and growth failure. [1]
What sets paediatric IBD apart from the adult disease is growth. Up to half of children with Crohn disease have impaired growth at presentation, driven by a combination of chronic inflammation, malnutrition, and prolonged corticosteroid exposure. This is why every management plan, regardless of the drug chosen, must protect and ideally restore linear growth, and why growth-centred induction strategies such as exclusive enteral nutrition are preferred where evidence supports them. [2]
Classification
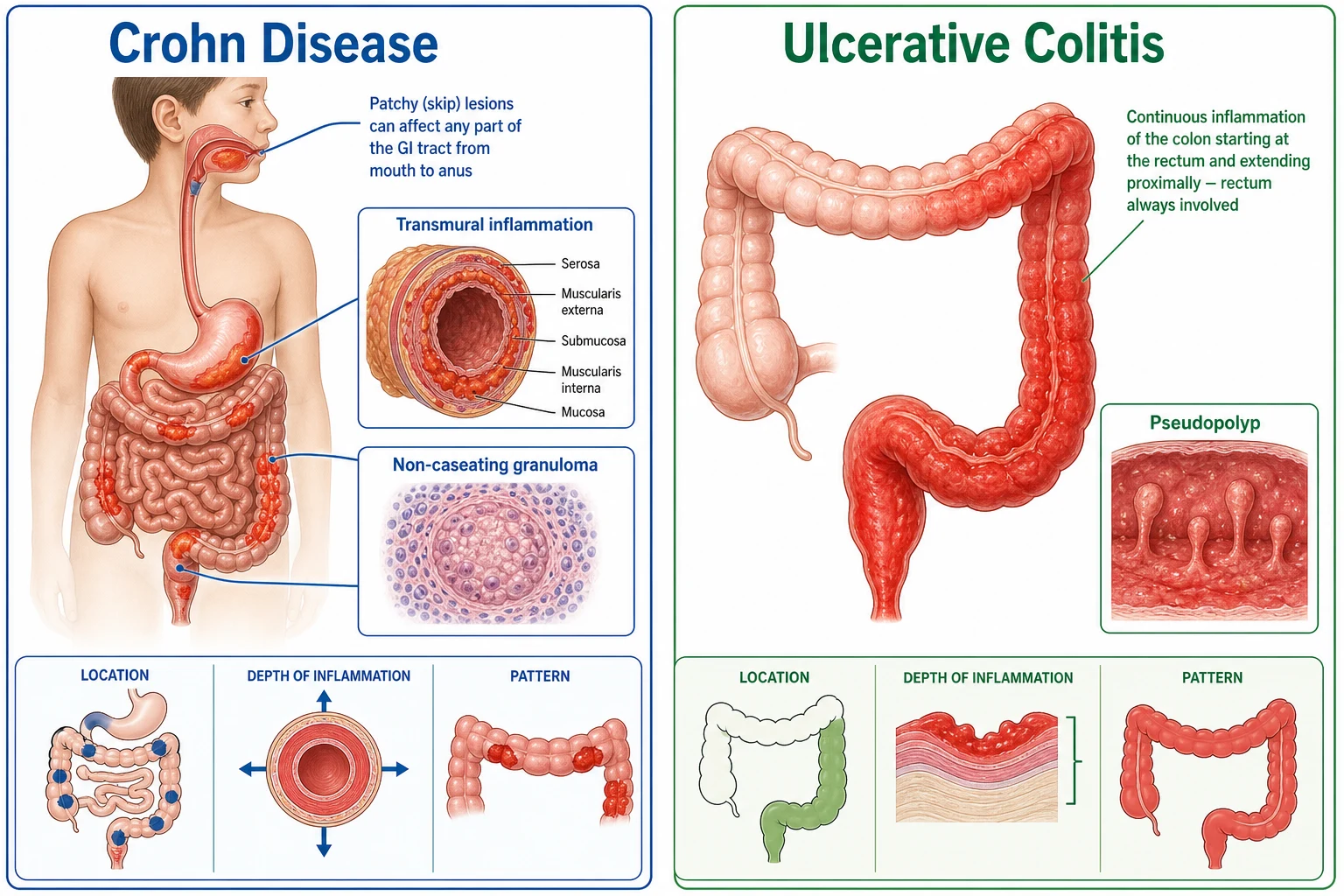
The first task is to separate Crohn disease from ulcerative colitis, because the distribution, depth, and behaviour of the inflammation differ in ways that determine treatment. Crohn disease is transmural, patchy, and can appear anywhere from the mouth to the anus, often with skip lesions separated by normal bowel. Ulcerative colitis is confined to the mucosa of the colon and rectum, spreads continuously and proximally from the rectum, and never involves the small intestine beyond the terminal ileum. [1]
[1]A substantial proportion of children, especially younger ones, present with colitis that cannot be confidently assigned to either category after full endoscopic and histologic evaluation. These children are labelled IBD-unclassified rather than indeterminate colitis, and many declare themselves as Crohn disease or ulcerative colitis over time as the disease evolves and deeper imaging or repeat endoscopy reveals upper-gut or perianal involvement. Keeping this category in mind prevents forcing an uncertain diagnosis into the wrong treatment pathway. [2]
Clinical phenotyping also matters for Crohn disease, where the Montreal or Paris classification describes the location (L1 ileal, L2 colonic, L3 ileocolonic, L4 upper) and behaviour (inflammatory, stricturing, penetrating) of the disease. The Paris modification adds growth retardation as a modifier, recognising that growth failure is itself a phenotype-defining feature in children. Together these distinctions guide prognostic discussion and the threshold for biologic therapy. [2]
Epidemiology & Risk Factors
Paediatric inflammatory bowel disease is rising in incidence worldwide, and the steepest increases are seen in newly industrialised countries adopting a Western lifestyle. Roughly a quarter of all IBD is diagnosed before the age of 18 years, and within paediatric cohorts the onset peaks in early to mid-adolescence, though a significant minority present in early childhood. Crohn disease is now more common than ulcerative colitis in children in most Western populations. [2]
The risk reflects an interaction between genetic susceptibility, the gut microbiota, and environmental triggers. A family history of IBD is the strongest single risk factor, and the condition is more common in people of Ashkenazi Jewish descent. Early antibiotic exposure, frequent infections, a low-fibre processed diet, and possibly a lack of breastfeeding have all been linked, while growing up in an environment with higher microbial exposure appears protective. Smoking raises the risk and severity of Crohn disease but, paradoxically, may protect against ulcerative colitis. [2]
The rising incidence in children is the subject of intense research. Leading hypotheses point to a changing microbiome shaped by diet, antibiotics, and sanitation, which in a genetically susceptible child tilts the mucosal immune system toward a sustained inflammatory response. Understanding that IBD is neither purely genetic nor purely environmental helps families grasp why there is no single cause and no single cure. [11]
Pathophysiology
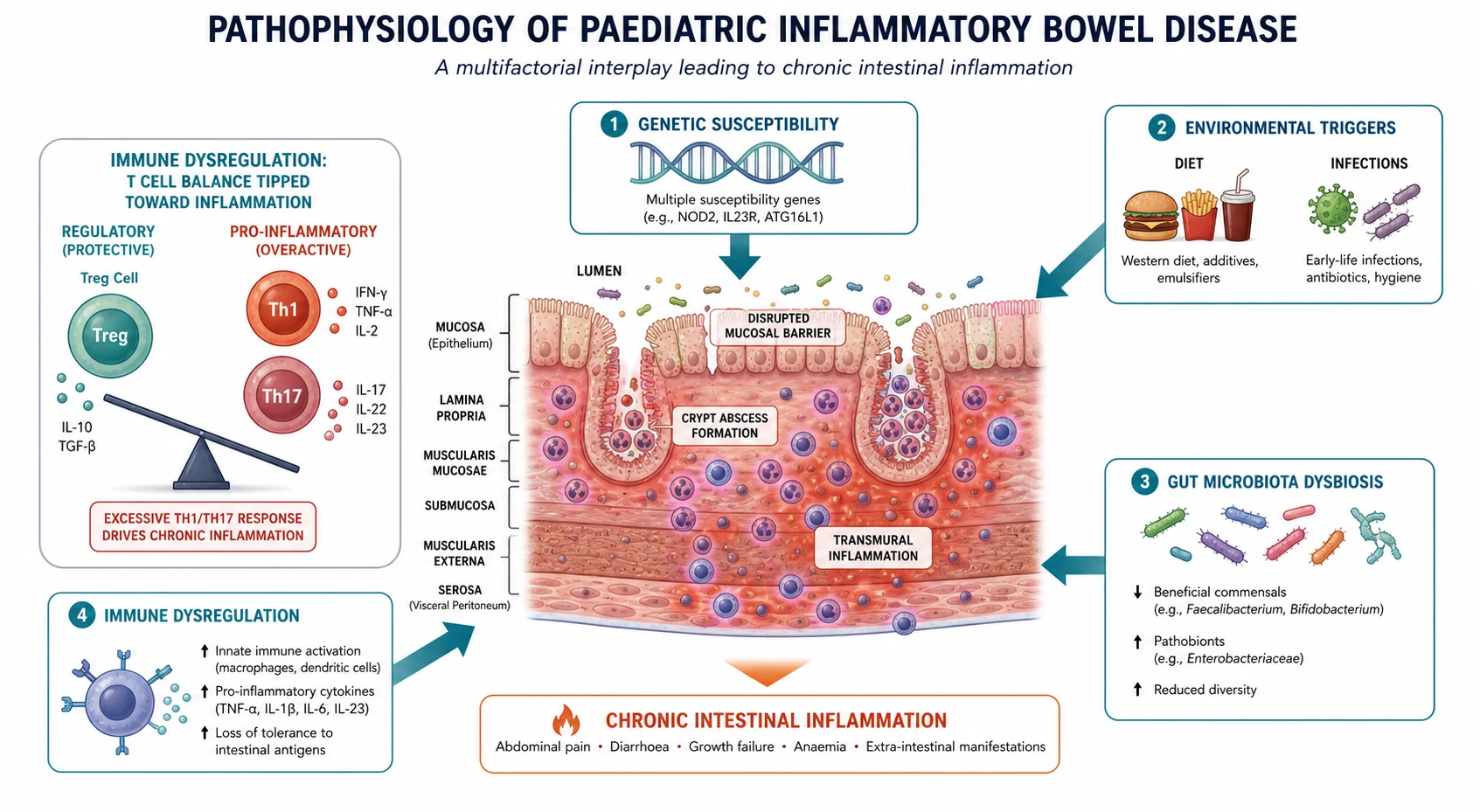
Inflammatory bowel disease arises when the delicate balance between the intestinal immune system, the commensal microbiota, and the epithelial barrier breaks down. In a healthy child the gut immune system tolerates trillions of commensal organisms while remaining alert to pathogens. In IBD this tolerance fails, and an inappropriately sustained inflammatory response damages the very tissue it is meant to protect. [11]
The response is driven by an overactive T-helper-1 and T-helper-17 immune axis in Crohn disease and a more T-helper-2 and humoral pattern in ulcerative colitis. Pro-inflammatory cytokines, chief among them tumour necrosis factor alpha, amplify and perpetuate the inflammation, recruiting further immune cells and producing the tissue injury seen on histology. This is precisely why anti-TNF biologic therapy is so effective: it interrupts the central amplifier of the inflammatory loop. [3]
Several contributing factors set the stage. Genetic susceptibility plays a clear role, with NOD2 among the best-characterised Crohn disease risk genes, and monogenic IBD syndromes such as IL-10 receptor deficiency causing very-early-onset disease in infants. Dysbiosis of the gut microbiota, a disrupted epithelial barrier with increased permeability, and environmental triggers such as antibiotic use and dietary change all converge on the final common pathway of chronic mucosal and transmural inflammation. [2]
Clinical Presentation
The presentation ranges from an indolent decline over months to an acute severe colitis, and in children the extraintestinal and growth features are often as prominent as the bowel symptoms. Chronic diarrhoea, abdominal pain, weight loss, and fatigue are the core gastrointestinal complaints, while growth faltering, delayed puberty, and perianal disease may be the features that first bring the child to medical attention. [1]
Crohn disease often declares itself with a more insidious and deceptive course. A child may present with fatigue, pallor from iron deficiency, poor weight gain, and periumbilical or right lower quadrant pain that has been attributed to stress or constipation for months. Perianal disease, including skin tags, fissures, and fistulae, is a distinctive clue that should prompt urgent referral, and prominent oral ulcers or aphthous stomatitis support an upper-gut or Crohn phenotype. [2]
Ulcerative colitis more often presents with bloody diarrhoea, urgency, tenesmus, and cramping lower abdominal pain. The bleeding and stool frequency are usually more overt than in Crohn disease, which brings these children to attention earlier, though the distinction is never made on symptoms alone and always confirmed endoscopically. [7]
Extraintestinal manifestations can precede or accompany the bowel disease and broaden the differential considerably. These include peripheral arthritis, erythema nodosum, pyoderma gangrenosum, oral aphthous ulcers, episcleritis or uveitis, and primary sclerosing cholangitis. Recognising these as part of IBD rather than separate problems prevents diagnostic delay and ensures the whole child, not just the colon, is managed. [1]
Presenting features that should trigger an IBD workup
Chronic diarrhoea, especially bloody or nocturnal, beyond four weeks
Growth faltering, weight loss, or delayed puberty
Persistent abdominal pain, particularly right lower quadrant
Perianal disease: skin tags, fissures, fistulae, or abscesses
Unexplained iron deficiency anaemia or elevated inflammatory markers
Extraintestinal signs: arthritis, oral ulcers, erythema nodosum
Differential Diagnosis
The differential for chronic diarrhoea with inflammation is broad, and the disciplined approach uses the history, examination, and a targeted laboratory and endoscopic workup to separate IBD from its mimics. Infection remains the first consideration, because infectious colitis can produce bloody diarrhoea and raised inflammatory markers that closely resemble ulcerative colitis. Stool culture, Clostridioides difficile testing, and parasitic studies are part of the initial screen. [1]
Coeliac disease is a common and treatable mimic that presents with diarrhoea, weight loss, and faltering growth, and it is excluded by coeliac serology with total immunoglobulin A rather than endoscopy alone. Other enteropathies, including eosinophilic gastroenteritis, food-protein-induced enterocolitis, and immunodeficiency-related enteropathy, enter the differential in younger children and those with atypical features. [1]
Functional abdominal pain disorders and irritable bowel syndrome cause chronic pain and altered bowel habit but are distinguished by normal growth, normal inflammatory markers, normal faecal calprotectin, and the absence of alarm features. The clinician must be alert to the child with a prior functional label who develops new alarm features, because a functional diagnosis never immunises against later organic disease. The table below contrasts the highest-yield discriminators. [1]
[1]Clinical & Bedside Assessment
A structured history and examination remain the highest-yield tools and should actively seek the features that separate IBD from its mimics. Characterise the stool frequency, consistency, urgency, and the presence of blood or mucus, and ask directly about nocturnal diarrhoea and pain that wakes the child from sleep, both of which argue strongly for organic disease. Document the duration of symptoms and any preceding gastroenteritis or antibiotic course. [1]
Plot height and weight on an appropriate growth chart and review the trajectory carefully, because crossing down through centiles, delayed puberty, or a fall in height velocity may be the only clue to Crohn disease in a child whose bowel symptoms are subtle. Ask about fever, fatigue, mouth ulcers, joint pain or swelling, rash, and eye symptoms to capture extraintestinal disease, and take a careful family history of IBD, coeliac disease, and other autoimmune conditions. [1]
The examination must include a thorough abdominal assessment and inspection of the perianal area, which is frequently overlooked yet reveals the skin tags, fissures, and fistulae that point to Crohn disease. Look for pallor, clubbing, aphthous oral ulcers, erythema nodosum, pyoderma gangrenosum, and joint swelling, and assess pubertal staging. A complete examination is essential because extraintestinal findings change the differential and the urgency of referral. [2]
Investigations
Diagnosis follows the ESPGHAN revised Porto criteria, which require ileocolonoscopy with biopsies from all segments, including the terminal ileum, at a minimum. Upper gastrointestinal endoscopy is recommended at diagnosis in all suspected paediatric IBD even without upper-gut symptoms, because isolated upper-gut Crohn disease is common in children and is missed by colonoscopy alone. Upper endoscopy may be omitted only when both endoscopy and histology of the ileum and colon are completely normal and IBD is thereby excluded. [1]
Blood and stool tests support but never replace endoscopy. A full blood count, C-reactive protein, erythrocyte sedimentation rate, ferritin, and albumin assess anaemia, inflammation, and nutritional status, while coeliac serology with total immunoglobulin A excludes a common mimic. Faecal calprotectin is the most sensitive non-invasive marker of intestinal inflammation and guides the threshold for endoscopy. Stool studies exclude infection, and thiopurine methyltransferase activity or genotyping is checked early if azathioprine is contemplated. [1]
Cross-sectional imaging complements endoscopy rather than replacing it. Magnetic resonance enterography is the preferred modality for evaluating small-bowel Crohn disease, strictures, fistulae, and abscesses, and avoids the radiation of computed tomography. Abdominal ultrasound is a useful bedside adjunct for assessing bowel wall thickening and is increasingly used for monitoring in experienced centres. Capsule endoscopy has a role when small-bowel disease is suspected and other imaging is negative, but only after a stricture is excluded. [2]
Two validated activity indices quantify disease severity and guide treatment. The Paediatric Crohn Disease Activity Index scores symptoms, examination, growth, and laboratory values, while the Paediatric Ulcerative Colitis Activity Index is built around stool pattern, bleeding, and global well-being. Both are central to trial endpoints and to clinical decisions about induction, escalation, and rescue therapy. [5]
Management — Resuscitation
Most newly diagnosed IBD presents as a chronic outpatient problem rather than an emergency, but acute severe colitis is a medical emergency that demands prompt recognition and resuscitation. A child with profuse bloody diarrhoea, fever, tachycardia, dehydration, abdominal distension, or signs of toxicity must be assessed immediately for airway, breathing, and circulation, and a paediatric gastroenterologist and surgeon involved early. [8]
Acute severe colitis in children is defined by a PUCAI score of 65 or greater and warrants admission for intravenous corticosteroids, fluid and electrolyte correction, thromboprophylaxis, and close monitoring for deterioration. Blood tests track haemoglobin, C-reactive protein, albumin, and electrolytes, and a plain abdominal radiograph excludes toxic megacolon. The child is reviewed daily, with the PUCAI recalculated to guide the timing of rescue therapy. [8]
Nutritional resuscitation is part of the initial care in both acute and chronic presentations, because malnutrition and micronutrient deficiency are common and impair healing and growth. Iron deficiency is treated, electrolytes corrected, and exclusive enteral nutrition considered both as therapy and as nutritional rehabilitation in Crohn disease. A dietitian is involved from the outset to support the child through induction. [2]
Management — Definitive & Stepwise
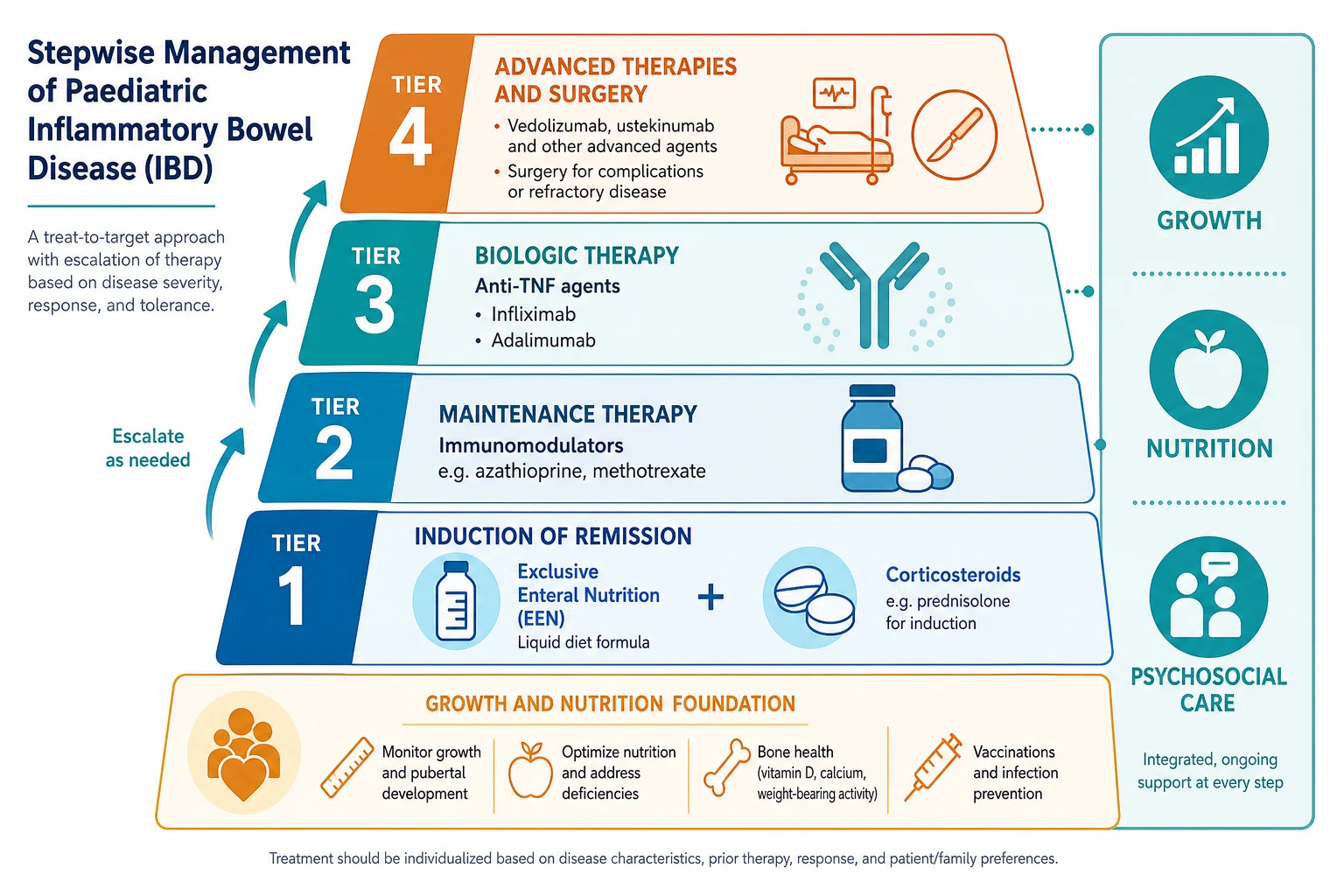
The goal of therapy is steroid-free remission with normal growth and mucosal healing, not merely symptom control. Achieving mucosal healing is now a recognised treatment target because it predicts a more durable remission and a lower risk of complications and surgery. Every step of the ladder must be weighed against its effect on growth, bone health, infection risk, and the child's quality of life. [11]
For induction of remission in Crohn disease, exclusive enteral nutrition is the preferred first-line therapy in many paediatric centres. A nutritionally complete liquid formula is given as the sole nutrition for six to eight weeks, inducing remission in a high proportion of children while simultaneously correcting malnutrition and avoiding the growth-suppressing effects of corticosteroids. Corticosteroids remain an effective alternative for induction where enteral nutrition fails or is refused, but are never used for maintenance because of their effects on growth, bone, and adrenal function. [2]
Maintenance therapy relies on immunomodulators and biologics. Azathioprine or its active metabolite 6-mercaptopurine is the mainstay for steroid-dependent or frequently relapsing disease, and a multicentre trial in newly diagnosed Crohn disease showed that adding 6-mercaptopurine to corticosteroids improved the maintenance of remission. Methotrexate is an alternative for thiopurine-intolerant children. [10]
Azathioprine (maintenance immunomodulation in paediatric IBD)
Dose
Typically 2 to 3 mg per kg per day orally, guided by thiopurine methyltransferase status and metabolite monitoring
Anti-TNF biologic therapy is reserved for moderate to severe disease that is refractory to, or dependent on, corticosteroids and immunomodulators, and is increasingly used earlier to achieve mucosal healing and protect growth. The REACH trial established infliximab for induction and maintenance of moderate-to-severe paediatric Crohn disease, and adalimumab was shown in the IMAgINE studies to be safe and effective in the same population. Both agents have transformed the outlook for children with severe disease. [3]
Infliximab (anti-TNF biologic, induction and maintenance)
Dose
5 mg per kg per dose intravenously at weeks 0, 2, and 6, then every 8 weeks for maintenance
Adalimumab (anti-TNF biologic, induction and maintenance)
Dose
Weight-based subcutaneous induction followed by maintenance dosing on alternate weeks, per local paediatric protocol
Surgery is never a failure of medical therapy but a defined part of the treatment pathway for complications such as strictures, fistulae, abscesses, and medically refractory disease. Bowel-sparing resection is the goal in Crohn disease to preserve absorptive capacity and avoid short-bowel syndrome, while in ulcerative colitis colectomy is curative for the colonic disease though extraintestinal manifestations may persist. Growth often improves dramatically after surgery in Crohn disease. [2]
Specific Subtypes & Scenarios
Acute severe colitis deserves specific attention as the most dangerous scenario in paediatric IBD. After intravenous corticosteroids, the daily PUCAI guides decisions: a persistently high score by day three to five triggers second-line rescue therapy with infliximab or ciclosporin, and a colectomy rate that rises steeply with delay means the surgical team is involved from admission. The aim is to rescue the colon without compromising safety. [6]
Perianal Crohn disease is a distinct and challenging subtype that requires combined medical and surgical management. Exam under anaesthetic, cross-sectional imaging with pelvic magnetic resonance imaging, and a combination of antibiotics, anti-TNF therapy, and surgical drainage of abscesses and seton placement for fistulae form the standard approach. Perianal disease often precedes the intestinal diagnosis and should always prompt endoscopic evaluation. [2]
Very-early-onset IBD, presenting before the age of six years, behaves differently from older-child disease and frequently reflects an underlying monogenic immune defect. Infants and young children with severe, refractory, or atypical colitis warrant specialised immunologic and genetic evaluation, including testing for IL-10 receptor deficiency and other monogenic causes, because the diagnosis can change management decisively, including the consideration of haematopoietic stem cell transplantation. [11]
[6]Complications & Pitfalls
The complications of paediatric IBD span the disease itself and its treatment. Stricturing, penetrating, and perianal disease in Crohn disease may require surgery, while longstanding ulcerative colitis carries a cumulative risk of colorectal cancer that rises with disease duration and extent, particularly with co-existing primary sclerosing cholangitis. Growth failure, delayed puberty, osteoporosis, and impaired quality of life are chronic complications that drive the push for steroid-free remission. [2]
Treatment carries its own risks. Corticosteroids suppress growth, bone health, and adrenal function and increase infection risk, which is why they are reserved for induction and never for maintenance. Thiopurines carry risks of myelosuppression, pancreatitis, hepatotoxicity, and a small increase in lymphoma risk, and require thiopurine methyltransferase testing and regular blood monitoring. Anti-TNF agents carry risks of serious infection, reactivation of tuberculosis, and infusion or injection reactions, all of which demand pre-treatment screening and ongoing vigilance. [3]
The classic pitfalls are diagnostic delay and treatment inertia. Because children may present with growth failure or extraintestinal symptoms rather than overt bloody diarrhoea, months can pass before IBD is considered, particularly in Crohn disease. Conversely, once diagnosed, prolonged reliance on corticosteroids without an effective steroid-sparing strategy remains a common and avoidable source of harm. A proactive, growth-centred plan with early escalation to effective maintenance therapy avoids both errors. [11]
Prognosis & Disposition
The outlook for paediatric IBD has improved dramatically with the move to early effective therapy targeting mucosal healing. Most children achieve remission with induction and maintain it with immunomodulators or biologics, attend school, and grow normally, and early treatment of inflammation is the single most important determinant of growth recovery. The disease remains chronic and relapsing, so ongoing surveillance and a therapeutic partnership with the family are lifelong. [11]
Surgery plays a defined role in both subtypes. In Crohn disease, resection or strictureplasty addresses complications and is followed by maintenance therapy to prevent recurrence, while in ulcerative colitis, colectomy is curative for the colonic disease and is offered for medically refractory disease or dysplasia. Growth typically improves markedly after surgery in Crohn disease, which reinforces that the inflammation, not the calories alone, was driving the growth failure. [2]
All children with IBD are managed by a paediatric gastroenterology service with multidisciplinary input from dietitians, specialist nurses, psychologists, and surgeons. Transition to adult care is a structured process that begins in early adolescence, building the young person's knowledge, self-management, and independence so that continuity of care is preserved into adulthood. Poor transition is a recognised cause of relapse and disengagement in young adulthood. [11]
Special Populations
Adolescents are the largest affected group and carry unique needs. Puberty, identity, body image, school performance, mental health, adherence, and risk behaviours all shape the disease experience, and a non-judgemental, confidential, adolescent-friendly approach is essential. Transition to adult care must be planned and gradual, because the years immediately after transfer carry the highest risk of disengagement and relapse. [11]
Children from socioeconomically disadvantaged backgrounds and those in rural or remote areas face barriers to diagnosis and to the costly biologic therapies that define modern care. Practical support with travel, telehealth monitoring, school liaison, and subsidised access to treatment helps close this gap, and a named coordinator can prevent the fragmentation that disproportionately affects vulnerable families. [6]
Younger children and those with very-early-onset disease warrant particular care because the differential widens to include monogenic and immune-deficiency syndromes. These children may have refractory disease, failure to thrive, and atypical infections, and they benefit from referral to a specialist centre with access to genetic testing, advanced immunomodulation, and consideration of haematopoietic stem cell transplantation for defined monogenic causes. [11]
[2]Evidence, Guidelines & Regional Differences
The ESPGHAN revised Porto criteria, published in 2014, remain the diagnostic foundation for paediatric IBD and mandate ileocolonoscopy with biopsies and, in most cases, upper endoscopy at diagnosis. They shifted practice toward earlier and more complete endoscopic evaluation, recognising that isolated upper-gut Crohn disease is common in children and is missed by colonoscopy alone. The PUCAI, developed and validated in 2007, provides the activity index that defines and guides acute severe colitis management. [1]
The ECCO and ESPGHAN consensus guidelines codify the medical management of paediatric Crohn disease, endorsing exclusive enteral nutrition as first-line induction, corticosteroids as an alternative, and azathioprine and anti-TNF agents for maintenance. The paired ambulatory and acute severe colitis guidelines for paediatric ulcerative colitis provide the evidence base for the PUCAI-driven approach to rescue therapy, defining clear thresholds for infliximab, ciclosporin, and surgery. [7]
[7]Controversies and regional differences persist. The timing and choice of biologic therapy, the role of top-down early anti-TNF treatment versus step-up from immunomodulators, and the place of newer agents such as vedolizumab and ustekinumab in children are evolving. Access to biologics is governed by national funding criteria that differ between countries, and the practice of exclusive enteral nutrition as first-line induction for Crohn disease, though strongly supported in Europe and Australasia, is less uniform in North America. The consistent theme is steroid-free remission with mucosal healing and normal growth. [2]
Exam Pearls
CROHN for the defining features of Crohn disease
References
- [1]Levine A, Koletzko S, Turner D, Escher JC, Cucchiara S, de Ridder L, et al ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J Pediatr Gastroenterol Nutr, 2014.PMID 24231644
- [2]Ruemmele FM, Veres G, Kolho KL, Griffiths A, Levine A, Escher JC, et al Consensus guidelines of ECCO/ESPGHAN on the medical management of pediatric Crohn's disease. J Crohns Colitis, 2014.PMID 24909831
- [3]Hyams J, Crandall W, Kugathasan S, Griffiths A, Olson A, Johanns J, et al Induction and maintenance infliximab therapy for the treatment of moderate-to-severe Crohn's disease in children. Gastroenterology, 2007.PMID 17324398
- [4]Turner D, Otley AR, Mack D, Hyams J, de Bruijne J, Uusoue K, et al Development, validation, and evaluation of a pediatric ulcerative colitis activity index: a prospective multicenter study. Gastroenterology, 2007.PMID 17681163
- [5]Hyams JS, Ferry GD, Mandel FS, Gryboski JD, Kibort PM, Kirschner BS, et al Development and validation of a pediatric Crohn's disease activity index. J Pediatr Gastroenterol Nutr, 1991.PMID 1678008
- [6]Turner D, Ruemmele FM, Orlanski-Meyer E, Griffiths AM, de Carpi JM, Bronsky J, et al Management of Paediatric Ulcerative Colitis, Part 2: Acute Severe Colitis-An Evidence-based Consensus Guideline From the European Crohn's and Colitis Organization and the European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr, 2018.PMID 30044358
- [7]Turner D, Ruemmele FM, Orlanski-Meyer E, Griffiths AM, de Carpi JM, Bronsky J, et al Management of Paediatric Ulcerative Colitis, Part 1: Ambulatory Care-An Evidence-based Guideline From European Crohn's and Colitis Organization and European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr, 2018.PMID 30044357
- [8]Turner D, Travis SP, Griffiths AM, Ruemmele FM, Levine A, Benchimol EI, et al Consensus for managing acute severe ulcerative colitis in children: a systematic review and joint statement from ECCO, ESPGHAN, and the Porto IBD Working Group of ESPGHAN. Am J Gastroenterol, 2011.PMID 21224839
- [9]Hyams JS, Griffiths A, Markowitz J, Baldassano RN, Faubion WA Jr, Colletti RB, et al Safety and efficacy of adalimumab for moderate to severe Crohn's disease in children. Gastroenterology, 2012.PMID 22562021
- [10]Markowitz J, Grancher K, Kohn N, Lesser M, Daum F A multicenter trial of 6-mercaptopurine and prednisone in children with newly diagnosed Crohn's disease. Gastroenterology, 2000.PMID 11040176
- [11]Ruemmele FM, Hyams JS, Otley A, Griffiths A, Kolho KL, Dias JA, et al Outcome measures for clinical trials in paediatric IBD: an evidence-based, expert-driven practical statement paper of the paediatric ECCO committee. Gut, 2015.PMID 24821616
- [12]Faubion WA, Dubinsky M, Ruemmele FM, Escher J, Rosh J, Hyams JS, et al Long-term Efficacy and Safety of Adalimumab in Pediatric Patients with Crohn's Disease. Inflamm Bowel Dis, 2017.PMID 28129288