Paeds · gastroenterology-hepatology-and-nutrition
Intussusception
Also known as Intussusception · Ileocolic intussusception · Telescoping bowel · Redcurrant jelly stool · Target sign · Pseudokidney sign · Air enema reduction · Pathological lead point · Idiopathic intussusception · Intussusceptum
Fellowship guide to intussusception in children, built around the single rule that a previously well infant with intermittent colicky screaming, vomiting and a sausage-shaped mass has intussusception until proven otherwise. The page covers the idiopathic-versus-pathological-lead-point split, the telescoping mechanism that drags the mesentery and ischaemes the bowel, the bedside ultrasound target sign, the resuscitation that precedes imaging, and the air enema as first-line reduction with surgery reserved for failure, peritonitis and pathological lead points.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a seven-month-old who was perfectly well, then begins to scream, draw his knees to his chest and go pale, settles into an exhausted sleep, and twenty minutes later does it again. That rhythm is the signature of intussusception. It is the telescoping of one segment of bowel into the next, the proximal intussusceptum invaginating into the distal intussuscipiens, and it is the commonest cause of intestinal obstruction in an infant between three months and three years of age. [1] [2]
The danger is mechanical and vascular at once. As the proximal bowel is driven forward it drags its mesentery with it, and the trapped mesentery is steadily strangulated, so the bowel wall swells, becomes ischaemic and bleeds, producing the blood-and-mucus redcurrant-jelly stool that is a late and ominous sign. The art of the diagnosis is to recognise the colicky pattern and act before that late stage arrives. [2] [6]
The governing principle is therefore speed coupled with a clear decision rule. You resuscitate the child, confirm the diagnosis with ultrasound, and attempt non-operative air enema reduction as first-line treatment, reserving surgery for failure, for signs of peritonitis or ischaemia, and for the older or very young child who is likely to harbour a pathological lead point. Most infants are reduced without an operation and do well, which is exactly why recognising the early pattern matters. [3] [6]
Classification
Sort intussusception first by whether a lead point can be found, because that single distinction governs both the suspicion and the surgery. The overwhelming majority in young infants are idiopathic, where hypertrophied lymphoid tissue in the terminal ileum, the Peyer patches swollen after a viral illness, forms the lead point that peristalsis drives forward. A smaller but important minority have a pathological lead point, a discrete lesion that must be found and removed. [1] [2]
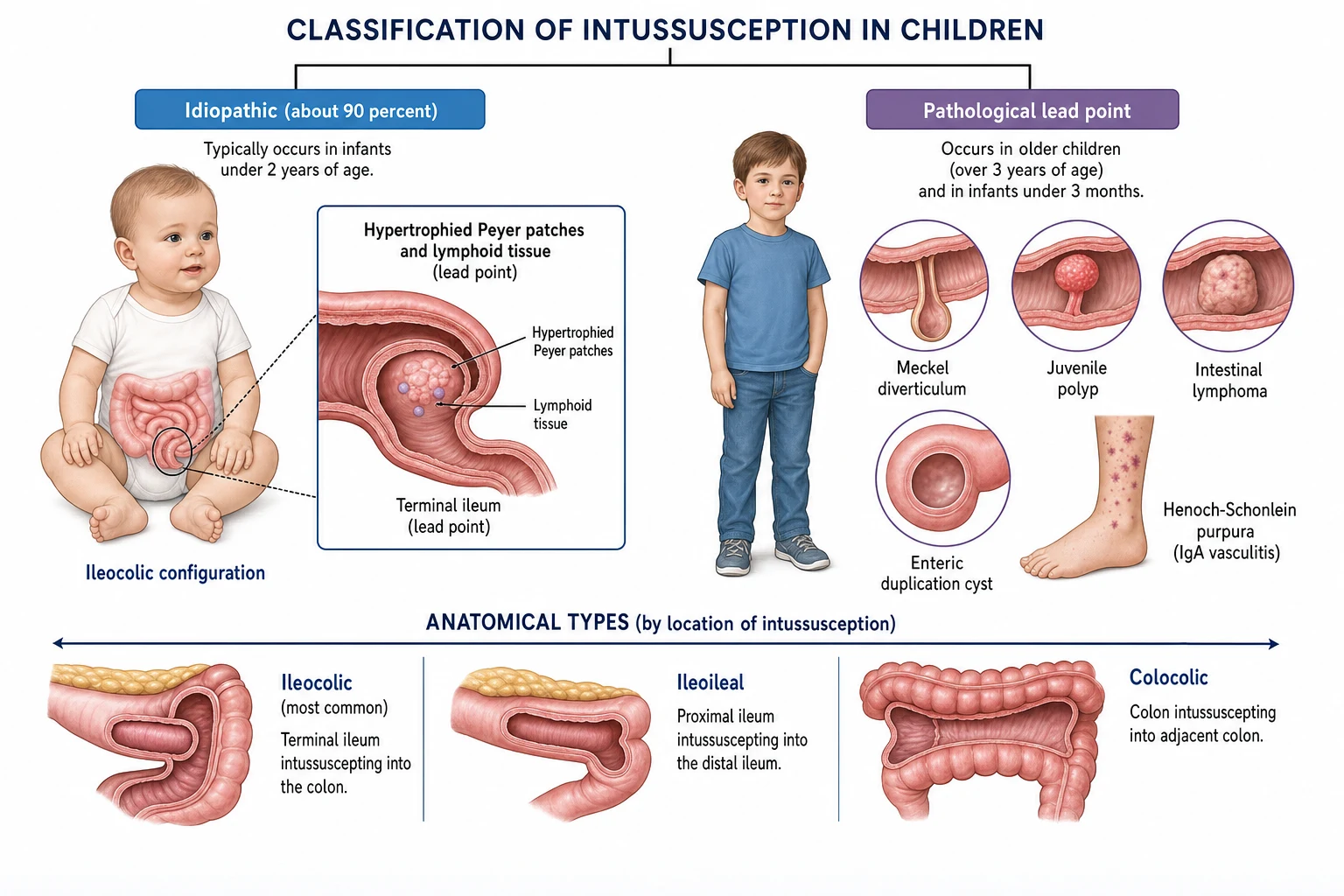
The second axis is anatomical, and it matters for imaging and for the conditions that mimic the disease. Ileocolic intussusception, where the terminal ileum prolapses into the ascending colon, is by far the commonest type and the one the classic mass and ultrasound signs describe. Ileoileal and jejunoileal forms are less common and are the patterns associated with Henoch-Schonlein purpura and with a pathological lead point, while a purely colocolic intussusception is rare and almost always pathological. [1] [4]
Idiopathic
- About ninety percent of cases in young infants
- Lead point is swollen Peyer patch and lymphoid tissue
- Typically three months to three years, peak five to nine months
- Reducible by enema in most, no lesion to resect
Pathological lead point
- More likely under three months or over three years
- Meckel diverticulum, juvenile polyp, lymphoma, duplication cyst
- Henoch-Schonlein purpura causes ileoileal intussusception
- Often needs surgery to remove the lead point
By location
- Ileocolic is the commonest and the classic pattern
- Ileoileal and jejunoileal less common, often pathological
- Colocolic is rare and usually has a lead point
- Location shapes the ultrasound findings and the operation
Epidemiology & Risk Factors
Intussusception is principally a disease of infancy. The peak incidence sits between five and nine months, around three-quarters of cases occur under two years of age, and the classic idiopathic form is concentrated in that window because the lymphoid tissue of the terminal ilean reaches its greatest bulk in the first year. Boys are affected slightly more often than girls. [1] [11]
Age shifts the aetiology in a predictable and exam-critical way. Under three months and over about three years, the chance of a pathological lead point rises sharply, so the very young baby and the older child with intussusception must be presumed to have a discrete lesion until imaging and surgery prove otherwise. A preceding viral respiratory or gastrointestinal illness is common, and the seasonal peaks mirror adenovirus and rotavirus activity, which is the thread that links the disease to its vaccine story. [1] [9]
The rotavirus vaccine association is the one epidemiological fact candidates must state accurately. Oral rotavirus vaccination carries a small, well-characterised excess risk of intussusception in the week after the first dose, but the absolute risk is tiny and the benefit in preventing severe dehydrating diarrhoea overwhelmingly outweighs it, so universal infant vaccination remains strongly recommended in Australia, New Zealand and worldwide. [9] [10]
Pathophysiology
The mechanism is one of peristalsis running away with a lead point. In the idiopathic form, swollen Peyer patches in the terminal ileum protrude into the lumen after a viral illness, and normal peristalsis pushes that nodule forward into the caecum and ascending colon. Once the intussusceptum has entered the intussuscipiens, peristalsis keeps driving it onward, and the segment telescopes deeper with each wave. [2] [4]
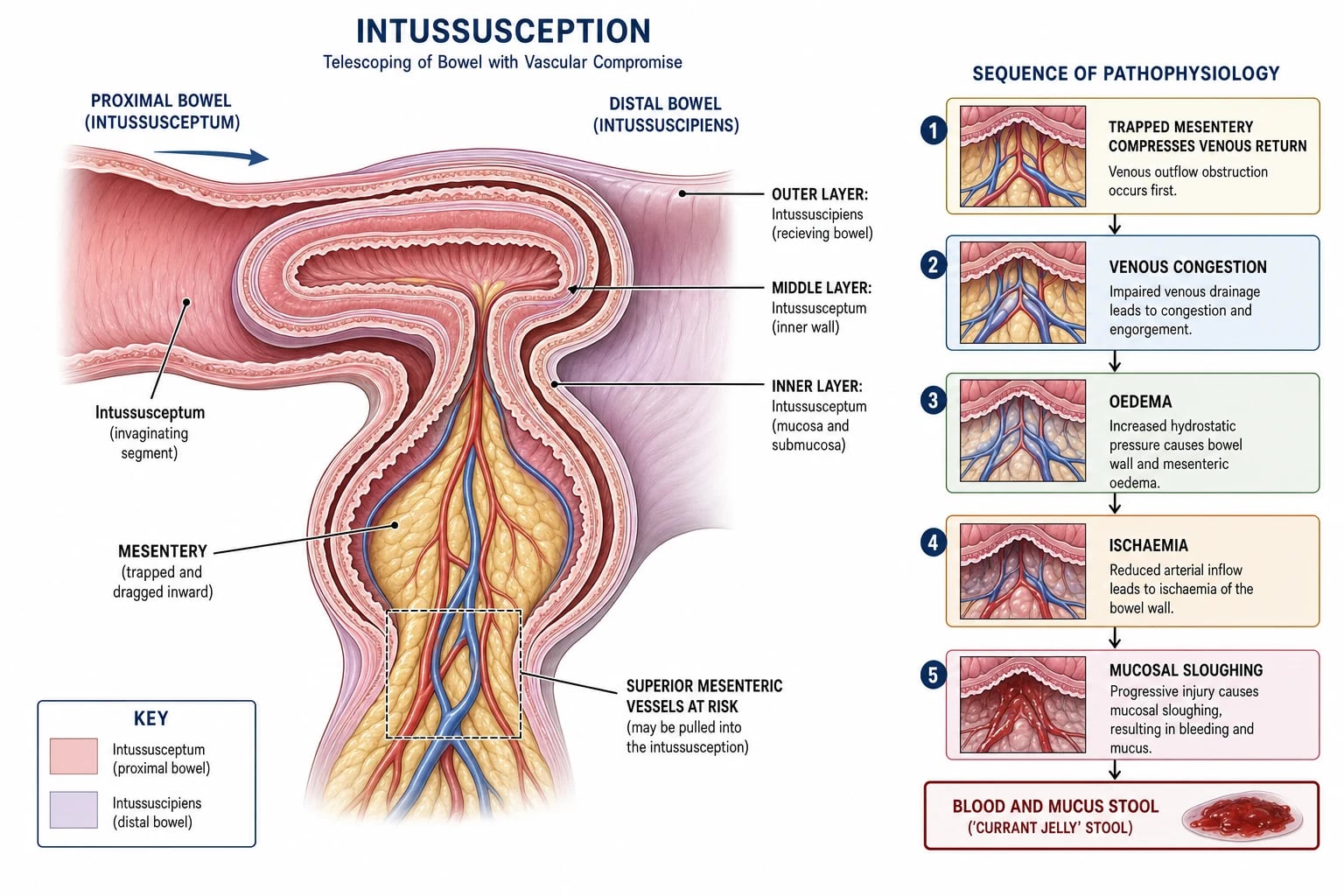
The trapped mesentery is what turns obstruction into ischaemia. Because the mesentery is pulled into the fold alongside the bowel, the veins and lymphatics, which are low-pressure and thin-walled, are compressed first, so the wall becomes oedematous and boggy. As the swelling tightens the fold, the arterial supply is eventually compromised, the mucosa sloughs, and blood and mucus weep into the lumen to form the redcurrant-jelly stool. Untreated, the segment infarcts and perforates. [2] [6]
The clinical rhythm follows directly from this anatomy. Each peristaltic wave drives the telescoping bowel forward and produces a wave of cramping pain, so the child screams and draws up the knees, then exhausts into a quiet interval until the next wave. Vomiting appears early from the obstructed proximal bowel, and as the cycle repeats the child dehydrates, becomes lethargic, and, if the ischaemia deepens, passes blood. Understanding that the pain is peristalsis-driven explains both the episodic pattern and the urgency. [1] [4]
Clinical Presentation
The presentation is rhythmic and distinctive, and recognising the rhythm is the whole skill. A previously well infant begins to have episodes of sudden, severe, colicky abdominal pain during which he screams, goes pale and draws the knees up to the chest, lasting a few minutes and followed by a quiet, drowsy or apparently pain-free interval before the next episode. Vomiting accompanies the early episodes and becomes bilious as the obstruction establishes. [1] [2]
Between episodes the abdomen holds the clues. A sausage-shaped mass is often palpable in the right upper quadrant, and the right lower quadrant may feel empty, the so-called sign of Dance, because the caecum has been displaced. The classic redcurrant-jelly stool, a mixture of blood and mucus, appears in only a minority and is a late sign of mucosal ischaemia, so its absence must never be used to exclude the diagnosis. [2] [6]
As the hours pass the picture darkens. Dehydration accumulates from the vomiting and third-space losses, the child becomes increasingly lethargic, fever may appear, and the abdomen grows tender and distended as the bowel becomes ischaemic. Signs of peritonitis, with guarding and rigidity, or cardiovascular collapse, signal that the bowel is infarcting or has perforated, and they convert the plan from careful imaging and enema reduction to emergency surgery. [6] [2]
Differential Diagnosis
The differential clusters around the infant with vomiting and colicky or intermittent pain, and several common conditions mimic intussusception closely. Acute gastroenteritis causes vomiting and cramping and may produce a bloody stool, but the pain is usually less rhythmic and diarrhoea dominates. Colic in a thriving infant is a diagnosis of exclusion, made only after intussusception is ruled out in any baby whose crying pattern has changed. [1] [2]
The surgical mimics matter most because they share the urgency. Malrotation with midgut volvulus presents with bilious vomiting and must not be missed, an incarcerated inguinal hernia is found by examining the groins, and appendicitis in the young child can present with pain and vomiting before localising. A simple constipation or urinary tract infection can also deceive, and Meckel diverticulitis can cause pain and bleeding in its own right. The discipline is to reach for the ultrasound whenever the pattern even hints at the rhythmic colic of telescoping bowel. [2] [4]
Intussusception
- Rhythmic colicky pain with quiet intervals
- Sausage-shaped mass, target sign on ultrasound
- Vomiting, later redcurrant-jelly stool
- Air enema reduction is first-line
Gastroenteritis
- More continuous cramping, diarrhoea dominates
- Bloody stool may occur but pain less rhythmic
- No mass, no target sign
- Managed with oral or intravenous rehydration
Malrotation with volvulus
- Bilious vomiting in a previously well infant
- Upper gastrointestinal contrast study is key
- Emergency Ladd procedure for volvulus
- Distinct from the colicky rhythm of intussusception
Clinical & Bedside Assessment
The assessment runs alongside resuscitation, never after it. Confirm the pattern yourself by watching for an episode, look at the vomit and ask whether it has become bile-stained, and examine the groin hernial orifices in every case because an incarcerated hernia is a quickly reversible mimic. Assess the airway, breathing and circulation first, because an infant with intussusception may already be dehydrated or shocked from vomiting and third-space loss. [2] [1]
Complete the examination with the questions that set the plan. Weigh the child and compare with a recent weight to gauge dehydration, inspect the stool for blood and mucus, and examine specifically for tenderness, guarding or rigidity, because peritonitis is the absolute contraindication to enema reduction. Document the time of onset and the frequency of episodes, since the duration of symptoms informs both the likelihood of ischaemia and the urgency of imaging. [6] [2]
Investigations
Ultrasound is the first and usually the only investigation needed, and it is both sensitive and specific. A meta-analysis of ultrasonographic diagnosis reported a sensitivity in the high nineties, so a confident scan rules the disease in or out at the bedside without radiation. The transverse view shows concentric alternating rings of oedematous bowel wall, the target or doughnut sign, and the longitudinal view shows the oval pseudokidney sign, the telescoped segments seen end-on. [5] [4]
Other tests serve the child rather than the diagnosis. A plain abdominal radiograph is not required when the ultrasound is positive, but it may show a soft-tissue mass, absent bowel gas in the right lower quadrant, or free air if the bowel has perforated. Blood tests, including a gas, electrolytes, glucose, full blood count and a group and save, are taken when the child is unwell or dehydrated or when surgery is likely, both to correct derangement and to prepare for theatre. The enema itself, whether air or contrast, is the next step and is both diagnostic and therapeutic. [4] [6]
Intussusception — the mnemonic TARGET
Management — Resuscitation
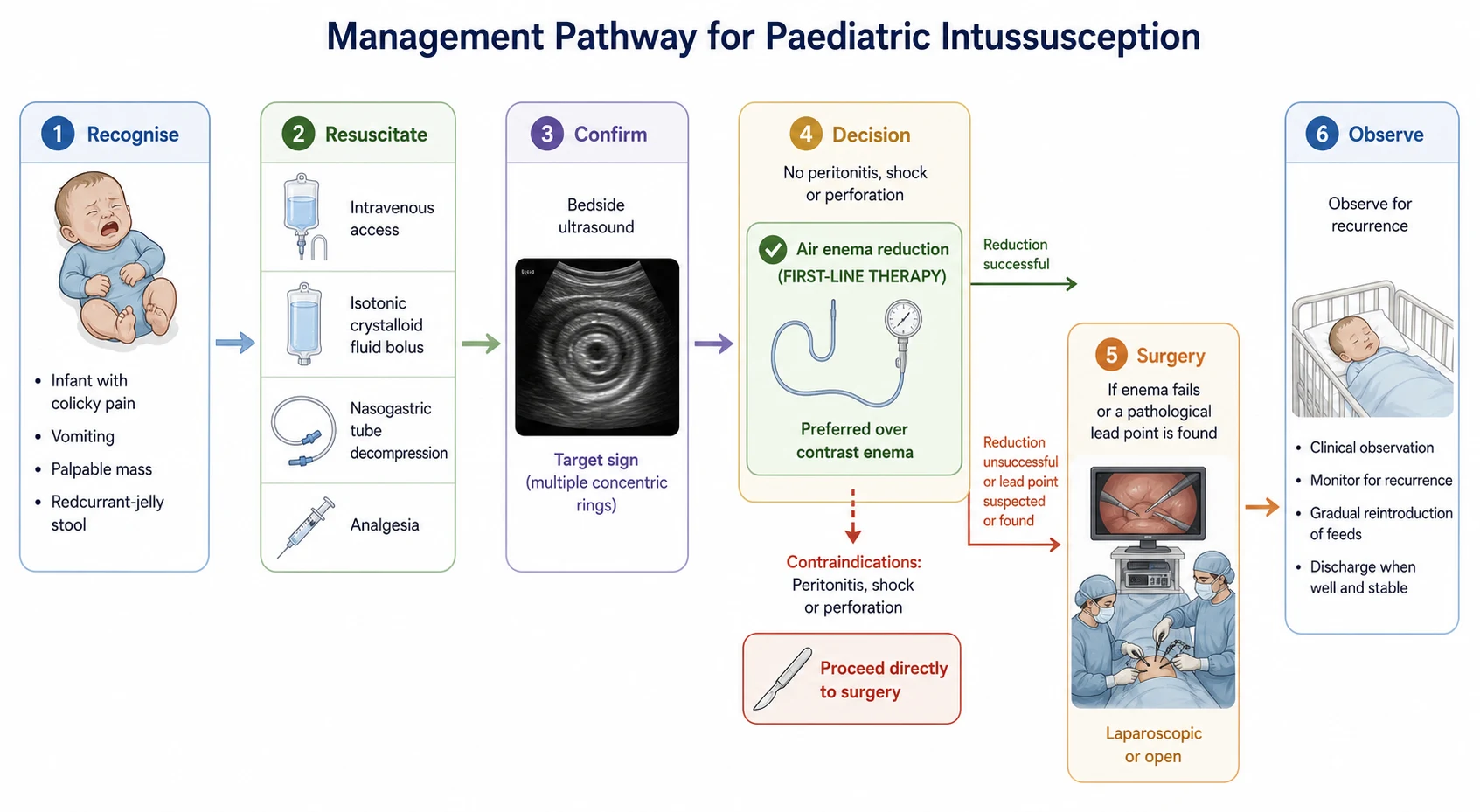
Resuscitation precedes imaging and reduction in every case, and it runs in parallel with the surgical and radiological referral. Keep the child nil by mouth, secure intravenous access, and pass a nasogastric tube on free drainage to decompress the obstructed stomach and reduce the risk of aspiration. These steps make the child safe for the ultrasound and the enema. [2] [6]
Correct the fluid deficit briskly. Give an intravenous bolus of 10 to 20 mL per kilogram of isotonic crystalloid and reassess, repeating as needed for shock or significant dehydration, then move to maintenance fluid with electrolyte correction guided by the bloods. Provide analgesia, because the colicky pain is severe, and check the glucose in any unwell young infant, who is at risk of hypoglycaemia. [2] [1]
Involve the paediatric surgeon and the radiologist early and together, because the reduction is a shared procedure that needs both present. Start broad-spectrum intravenous antibiotics when surgery is likely or perforation is suspected, and continue resuscitation throughout transfer if the child is being retrieved from a rural or remote centre. The aim of this phase is to deliver a well-resuscitated, decompressed child to the enema suite or the theatre, not a dry, vomiting infant in shock. [6] [2]
Management — Definitive & Stepwise
Definitive treatment follows one rule: reduce the intussusception without an operation whenever it is safe to do so, and operate only when enema fails, when the bowel is compromised, or when a pathological lead point is suspected. The whole pathway runs from recognition and resuscitation, through ultrasound confirmation, to the enema and its decision branches, and finally to surgery and observation for recurrence. [3] [6]
Non-operative enema reduction is the treatment of choice for the stable child without peritonitis. Air enema reduction is preferred over liquid or contrast enema, because a meta-analysis found air reduction achieved a higher success rate, was faster, used less radiation and avoided the mess and barium risk of contrast, while making any perforation easier to manage. The procedure is performed under fluoroscopic or ultrasound guidance with controlled, sustained pressure, and it succeeds in roughly three-quarters to four-fifths of attempts. [3] [4]
Air enema reduction
Dose
Controlled sustained insufflation under imaging guidance, beginning at a low pressure and escalating only as needed, with a defined maximum and a finite number of attempts
Surgery is reserved for the failures and the contraindications. If the enema cannot reduce the intussusception, or if the child presents with peritonitis, shock or perforation, the child proceeds to a laparoscopic or open manual reduction, with resection of any non-viable bowel and of any pathological lead point that is found. After a successful enema reduction the child is observed for a short period to feed and to watch for recurrence, which happens in roughly one in ten. [6] [7]
Specific Subtypes & Scenarios
The pathological-lead-point scenario is the one every candidate must own. In a child under three months or over about three years, intussusception is far more likely to harbour a discrete lesion such as a Meckel diverticulum, a juvenile polyp, an intestinal lymphoma or an enteric duplication cyst, and these lead points both resist enema reduction and require surgical removal. The reflex is therefore a lower threshold for surgery and an active search for the lead point at operation. [7] [2]
Henoch-Schonlein purpura occupies a special niche because it both mimics and causes intussusception. The intussusception of IgA vasculitis is typically ileoileal rather than ileocolic, because the submucosal haemorrhage and oedema of the inflamed small bowel act as a lead point, and it may present alongside the characteristic palpable purpura, abdominal pain and joint swelling. Many of these reduce with medical management of the vasculitis, but obstruction or a worsening abdomen still needs surgical assessment. [2] [4]
Recurrent intussusception and the post-reduction child round out the set. Recurrence after a successful enema reduction occurs in about ten percent of infants, usually within days to weeks, and it is almost always reducible by a further enema, so a repeat ultrasound for any recurrence of colicky symptoms after reduction is the correct reflex. Surgery for recurrence is reserved for the child with multiple recurrences or a suspected lead point. [8] [7]
Complications & Pitfalls
The complications follow the twin threats of ischaemia and delay. If the intussusception is not reduced in time, the trapped segment infarcts, leading to perforation, peritonitis and sepsis, and extensive small-bowel necrosis leaves the child with short-bowel syndrome and lifelong parenteral nutrition. Enema reduction itself carries a small risk of perforation, estimated at around one percent, which is why the surgeon and the means to operate must be immediately available during every attempt. [6] [3]
The pitfalls cluster around underestimating the early presentation. The commonest error is to dismiss the colicky, vomiting infant as having colic or gastroenteritis and to delay the ultrasound, allowing the telescoping to progress to ischaemia. A second error is to wait for the redcurrant-jelly stool, which is a late sign. A third is to attempt enema reduction in a child with peritonitis or shock, and a fourth is to forget that an older or very young child may have a pathological lead point that needs surgery. [2] [1]
Prognosis & Disposition
Outcome is dominated by the speed of recognition and reduction. When intussusception is diagnosed early and reduced by enema, the great majority of children recover fully with an excellent prognosis, a short hospital stay and only the small risk of recurrence to counsel about. When diagnosis is delayed and the bowel is lost, the child faces resection, possible short-gut syndrome and a far harder course, which is why time to reduction is the single most important prognostic lever. [6] [8]
Geography and resources bend the outcome sharply. In well-resourced settings where ultrasound and enema reduction are available within hours, mortality is very low. In resource-limited settings, late presentation, limited access to imaging and surgery, and delayed referral drive much higher rates of bowel resection, complication and death, a pattern documented across low- and middle-income cohorts. [12] [10]
Disposition reflects the acuity and the access. A confirmed or suspected intussusception needs a centre with paediatric surgery and interventional radiology, so a child presenting in a rural or remote hospital is resuscitated, decompressed and retrieved while the receiving team is mobilised. After a successful reduction the child is observed briefly to ensure feeding and to watch for recurrence, then discharged with clear safety-netting. The child who has had surgery stays for recovery and for management of any lead point found. [2] [6]
Special Populations
The age extremes deserve a separate suspicion. In the neonate and the young infant under three months, intussusception is uncommon but, when it occurs, is more likely to have a pathological lead point and to present atypically with lethargy, refusal of feeds or bleeding rather than the classic rhythmic colic, so a low threshold for ultrasound is essential. In the older child over about three years, the same logic applies and the search for a lead point such as a lymphoma or polyp moves to the foreground. [7] [2]
Resource-limited and remote communities face the steepest gradient. In eastern Ethiopia and similar settings, late presentation and limited surgical access mean many children reach hospital with established ischaemia, and outcomes are correspondingly worse. In Australia and New Zealand, an Indigenous or remote child with intussusception may be hours from imaging and reduction, so early recognition, resuscitation, nasogastric decompression and prompt retrieval are what protect the bowel, making the reflex to treat rhythmic colic as intussusception an equity issue as much as a clinical one. [12] [11]
The child with Henoch-Schonlein purpura and abdominal symptoms is a population in its own right. Because the vasculitis can produce an ileoileal intussusception alongside its typical purpura and pain, any deterioration in the abdominal picture of a child with known IgA vasculitis warrants imaging and surgical liaison, balanced against the fact that many such episodes settle with medical management. [2] [4]
Evidence, Guidelines & Regional Differences
The evidence base blends systematic reviews of imaging and reduction with epidemiological surveillance. The meta-analysis of air versus liquid enema established air reduction as the preferred first-line technique on the strength of higher success, lower radiation and safer perforation management, while the meta-analysis of ultrasound confirmed its near-perfect sensitivity as the diagnostic test of choice. These two reviews anchor the modern pathway of ultrasound confirmation followed by air enema reduction. [3] [5]
The rotavirus vaccine story is the most important and most examined piece of guideline-level evidence. Post-marketing surveillance confirmed a small excess risk of intussusception in the week after the first vaccine dose, but international consensus, reflected in position statements from immunisation authorities, holds that the overwhelming benefit in preventing severe rotavirus disease far outweighs the small risk, and universal infant rotavirus vaccination continues to be recommended in Australia, New Zealand and worldwide. [9] [10]
Regional practice is consistent in principle but uneven in access. The pathway of recognise, resuscitate, ultrasound, air enema and surgery is universal in high-income settings, but the capacity to deliver prompt imaging and reduction varies, and the epidemiology before and after vaccine introduction has been mapped in countries such as Australia. In resource-limited settings, the same disease carries a far heavier burden of late presentation and adverse outcome, which is why the guideline principles matter most where access is least. [11] [12]
Exam Pearls
Hold one sentence above all others: a previously well infant with intermittent colicky screaming, vomiting and a sausage-shaped mass has intussusception until proven otherwise, confirmed by the target sign on ultrasound and reduced by air enema. State the reflex that follows: resuscitate with intravenous fluids and a nasogastric tube, confirm with ultrasound, attempt air enema reduction as first-line treatment, and reserve surgery for failure, peritonitis and pathological lead points. [2] [3]
Get the frequently tested facts exactly right. The diagnostic ultrasound sign is the target sign transversely and the pseudokidney sign longitudinally, and the commonest type is ileocolic. Idiopathic intussusception dominates from three months to three years with a peak at five to nine months, while a pathological lead point such as a Meckel diverticulum, polyp or lymphoma rises under three months and over three years. [1] [5]
The high-yield pairings do the work in a viva. A rhythmic colicky infant with a mass needs an ultrasound for the target sign and an air enema for reduction; peritonitis or shock converts the plan straight to surgery; recurrence after reduction happens in about ten percent and is usually reducible again; and the rotavirus vaccine carries a small intussusception risk that is overwhelmed by its benefit, so vaccination continues to be recommended. Always resuscitate before you reduce. [8] [9]
References
- [1]Jiang J; Jiang B; Parashar U Childhood intussusception: a literature review. PLoS One, 2013.PMID 23894308
- [2]Applegate KE Intussusception in children: evidence-based diagnosis and treatment. Pediatr Radiol, 2009.PMID 19308373
- [3]Sadigh G; Zou KH; Razavi SA; et al Meta-analysis of Air Versus Liquid Enema for Intussusception Reduction in Children. AJR Am J Roentgenol, 2015.PMID 26496576
- [4]Ko HS; Schenk JP; Tröger J Current radiological management of intussusception in children. Eur Radiol, 2007.PMID 17308922
- [5]Li XZ; Wang H; Song J; et al Ultrasonographic Diagnosis of Intussusception in Children: A Systematic Review and Meta-Analysis. J Ultrasound Med, 2021.PMID 32936473
- [6]Kaiser AD; Applegate KE; Ladd AP Current success in the treatment of intussusception in children. Surgery, 2007.PMID 17950338
- [7]Fisher JG; Sparks EA; Turner CG; et al Operative indications in recurrent ileocolic intussusception. J Pediatr Surg, 2015.PMID 25598108
- [8]Justice FA; Nguyen LT; Tran SN Recurrent intussusception in infants. J Paediatr Child Health, 2011.PMID 21435072
- [9]Buttery JP; Standish J; Bines JE Intussusception and rotavirus vaccines: consensus on benefits outweighing recognized risk. Pediatr Infect Dis J, 2014.PMID 24732449
- [10]Yen C; Healy K; Tate JE; et al Rotavirus vaccination and intussusception - Science, surveillance, and safety: A review of evidence and recommendations for future research priorities in low and middle income countries. Hum Vaccin Immunother, 2016.PMID 27322835
- [11]Palupi-Baroto R; Lee KJ; Carlin JB Intussusception in Australia: epidemiology prior to the introduction of rotavirus vaccine. Aust N Z J Public Health, 2015.PMID 25558780
- [12]Tesfaye DD; Adem BM; Ketema I; et al Clinical profile and treatment outcome of acute intussusception among children in eastern Ethiopia: A seven years retrospective study. Front Pediatr, 2022.PMID 36518776