Paeds · gastroenterology-hepatology-and-nutrition
Malnutrition: nutritional rehabilitation and monitoring
Also known as Severe acute malnutrition · SAM · Moderate acute malnutrition · MAM · Marasmus · Kwashiorkor · Oedematous malnutrition · Refeeding syndrome · Nutritional rehabilitation · Ready-to-use therapeutic food · F-75 · F-100 · Community-based management of acute malnutrition
Fellowship guide to acute malnutrition and its nutritional rehabilitation in children. The page covers the recognition of severe and moderate acute malnutrition by weight-for-height z-score, mid-upper arm circumference and bilateral pitting oedema; the split between complicated and uncomplicated SAM that sends a child to inpatient stabilisation or outpatient ready-to-use therapeutic food; the World Health Organization phased rehabilitation from F-75 stabilisation through transition to F-100 catch-up feeding; the mechanism and prevention of refeeding syndrome through phosphate, potassium and magnesium monitoring and thiamine; the use of ReSoMal rather than standard oral rehydration solution; the rational use of antibiotics; and a discharge and follow-up plan that prevents relapse.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A wasted toddler sits listless in his mother's lap, his arms thin as sticks and his mid-upper arm too small for the red zone of the measuring tape. The danger in front of you is not only the starvation that brought him here, but the harm that feeding him too quickly can do. This is the paradox at the heart of acute malnutrition: the treatment is food, yet food given wrongly can kill. [1] [3]
Acute malnutrition is a recent, rapid loss of nutritional status, marked by wasting (low weight for height) or by bilateral pitting oedema. It is "acute" because it reflects what has happened over weeks to a few months, in contrast to stunting, the chronic short stature of long-term undernutrition. The severe form, severe acute malnutrition (SAM), carries a high mortality when untreated, and most of the craft of managing it lies in refeeding the child safely. [1] [11]
The examiner's framework rests on four ideas. First, recognise and grade the malnutrition with anthropometry. Second, decide whether the child is sick enough to need a hospital bed. Third, refeed in the WHO's phased way, stabilising before you rehabilitate. Fourth, guard against refeeding syndrome at every step and watch for relapse after discharge. [1] [8]
Classification
Sort the child first by severity, because severity decides the setting and the risk. The three tools that measure acute malnutrition are the weight-for-height z-score, the mid-upper arm circumference (MUAC), and the presence of bilateral pitting oedema. Any one of the three, alone, can place a child in the severe category. [1] [12]
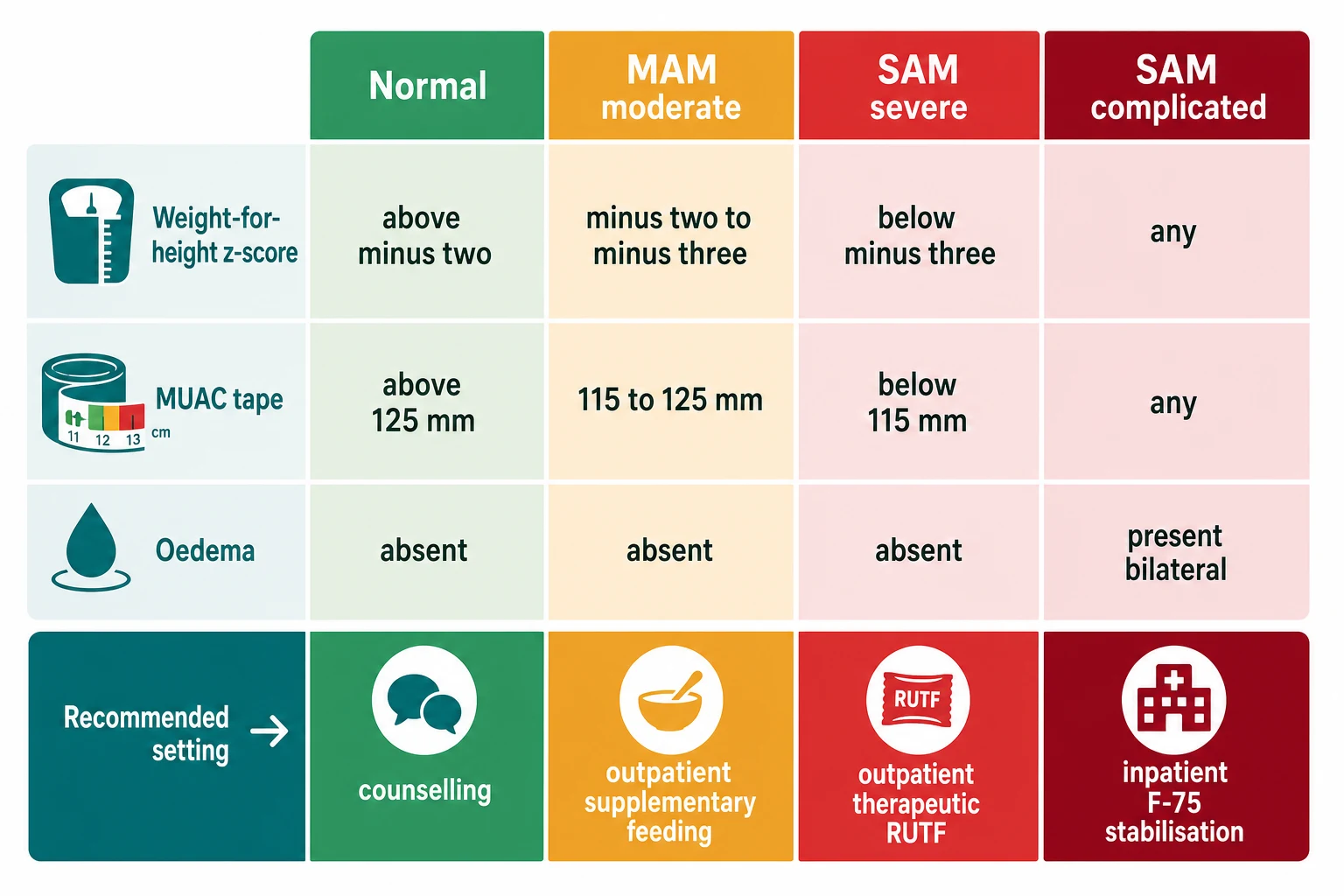
Severe acute malnutrition is a child with a weight-for-height z-score below minus three, a MUAC below 115 mm (for ages six to fifty-nine months), or bilateral pitting oedema. Moderate acute malnutrition is a z-score between minus two and minus three, or a MUAC between 115 and 125 mm. The figure lays the cut-offs side by side, and the single most testable rule is that oedema on its own makes the child severe. [1] [12]
Severe acute malnutrition (SAM)
- Weight-for-height z-score below minus 3, OR
- MUAC below 115 mm (6 to 59 months), OR
- Bilateral pitting oedema (kwashiorkor)
- High untreated mortality; needs therapeutic feeding
Moderate acute malnutrition (MAM)
- Weight-for-height z-score minus 2 to minus 3, OR
- MUAC 115 to below 125 mm
- No oedema
- Outpatient supplementary feeding; prevent progression
No acute malnutrition
- Weight-for-height z-score at or above minus 2
- MUAC 125 mm or above
- No oedema
- Preventive counselling and growth monitoring
The second fork, once severity is set, is complicated versus uncomplicated. This decides whether the child is managed as an inpatient or at home. A child with SAM who still has an appetite, no medical complications and no severe oedema has uncomplicated SAM and can be treated in the community with ready-to-use therapeutic food (RUTF). A child with loss of appetite, fever, severe oedema, or any serious infection or dehydration has complicated SAM and needs admission for stabilisation. This single judgement is the disposition pivot, and getting it wrong in either direction harms the child. [1] [11]
The bilateral pitting oedema of kwashiorkor is graded by the thumb-pressure test: grade one is feet only, grade two reaches the knees, and grade three extends to the face or is generalised. A higher grade signals a sicker child and a lower threshold for inpatient care. MUAC is favoured for community screening because a single colour-coded tape is cheap, fast and reproducible, and because it predicts mortality in young children better than weight alone. [12] [1]
Epidemiology & Risk Factors
Severe acute malnutrition remains one of the leading single causes of death in children under five worldwide, and most of those deaths are preventable with treatment that has existed for decades. Untreated SAM multiplies a child's risk of dying many times over, and the lethality comes as much from the accompanying infection and metabolic collapse as from the starvation itself. [1] [11]
The risk concentrates where food is scarce, infection is common, and care is far away. Infants and toddlers under two are the most vulnerable, because their rapid growth leaves a thin margin between adequate intake and wasting. Any intercurrent infection, particularly diarrhoea, measles and pneumonia, tips a borderline child into acute malnutrition, and HIV magnifies both the risk and the mortality. [11] [1]
In Australia and New Zealand, severe acute malnutrition is rare in the general community but is seen in specific groups: refugee and migrant children after arrival, Indigenous and remote children, and infants and children with chronic disease, neurodisability, or feeding disorders. In these settings malnutrition is often secondary, the child's wasting a symptom of an underlying illness or of social hardship, and the rehabilitation has to address the cause as well as the weight. [11] [1]
Relapse is part of the epidemiology too. A recovered child sent back into the same food insecurity or untreated illness has a real chance of returning, and discharge planning is therefore as much a treatment as the feeding itself. The children most likely to relapse are those discharged too early, those whose families cannot sustain feeding, and those with an unaddressed underlying illness. [1] [11]
Pathophysiology
To understand why refeeding a starved child can be dangerous, follow what starvation does to the cell. A malnourished child breaks down muscle and fat to survive, insulin falls, and the body shifts into a slow, catabolic mode. During this adaptation, total body stores of phosphate, potassium and magnesium are quietly depleted, even though the blood levels may still read normal. The danger is hidden until feeding restarts. [4] [6]
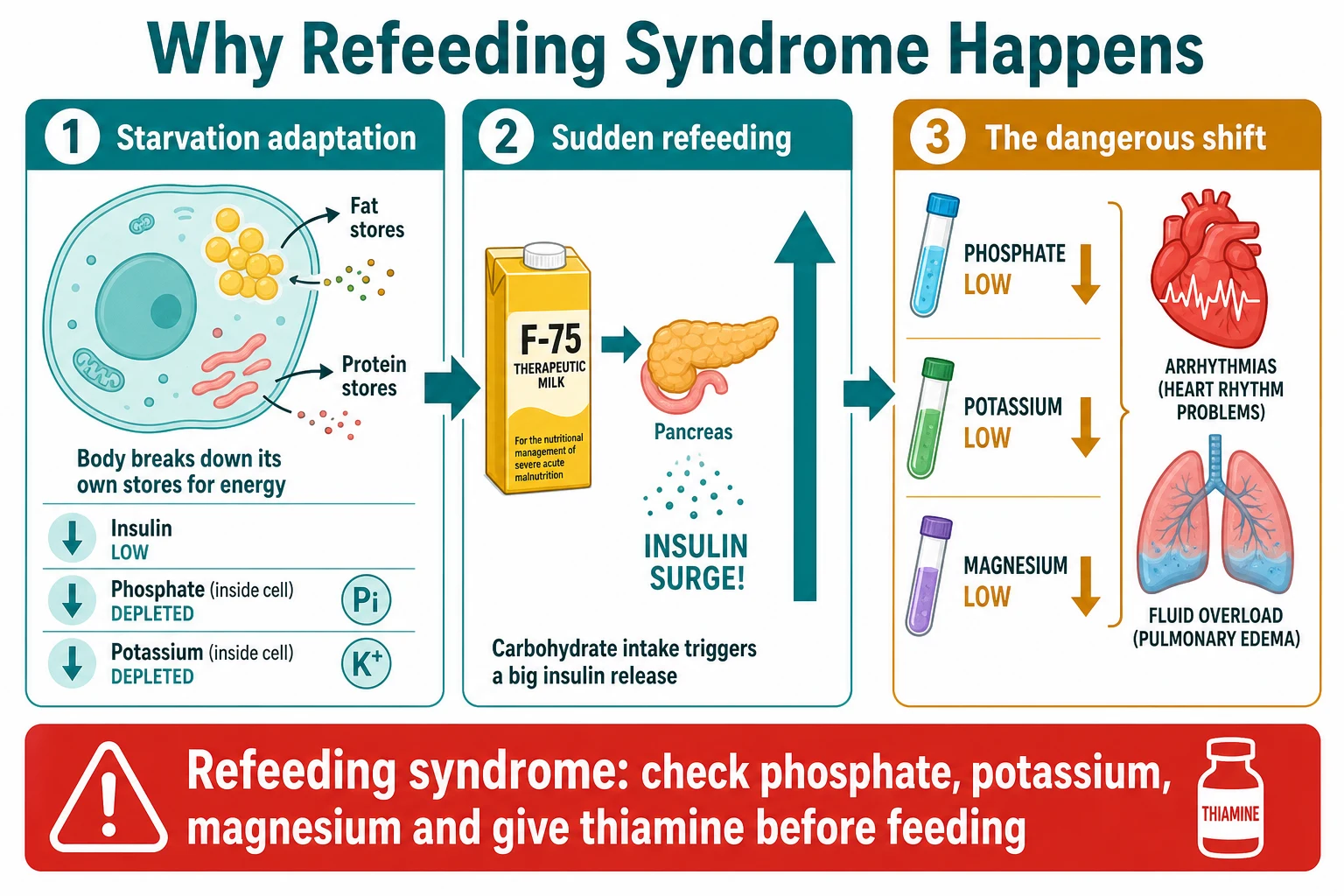
Refeeding syndrome is the biochemical storm that follows a carbohydrate load. Glucose triggers a sharp insulin release, and insulin drives phosphate, potassium and magnesium back into the cells. Because the intracellular stores were already drained by starvation, the serum levels fall faster than they can be replaced, producing hypophosphataemia, hypokalaemia and hypomagnesaemia within hours to days of starting feeds. Thiamine, consumed by the sudden carbohydrate metabolism, also runs short. [4] [5]
The consequences of these falls are what kill. Low phosphate weakens muscles and the diaphragm, impairs the heart, and can precipitate acute heart failure and respiratory failure; low potassium and magnesium drive dangerous arrhythmias. The insulin surge also retains sodium and water, so a malnourished heart, already wasted and stiff, may be tipped into fluid overload and congestive failure. This is why the malnourished heart tolerates sodium and fluid so poorly, and why a careless drip can be lethal. [4] [8]
Oedematous malnutrition, kwashiorkor, adds its own derangements. The leak of fluid into the tissues reflects a damaged gut barrier, low serum albumin, and disordered sodium transport, not simple hunger. These children look "puffy" rather than thin and are easily misjudged as better nourished than they are, which is exactly why oedema alone defines SAM. [1] [11]
Clinical Presentation
The wasted child, marasmus, is the picture most clinicians picture: obvious thinness, loss of muscle and fat, a face that looks old, loose skin folds, and an apathetic or irritable manner. The oedematous child, kwashiorkor, is the trap: weight may look preserved because of the fluid, the hair is often sparse and depigmented, the skin may show flaky paint dermatosis, and the abdomen is distended by an enlarged fatty liver. Both forms can sit in front of you looking deceptively stable. [1] [11]
The signs that mark complicated SAM, and that should send the child to inpatient care, are the dangerous ones. Loss of appetite is the pivotal sign and is tested directly by offering RUTF and seeing whether the child eats. Fever or hypothermia, severe oedema extending above the knees, lethargy, vomiting, dehydration, fast or difficult breathing, and any sign of sepsis each signal that this is no longer uncomplicated. [1] [11]
In high-resource settings the atypical presentations matter most, because classic marasmus is uncommon. A child with cerebral palsy or a feeding disorder who is quietly losing weight, a teenager with anorexia nervosa who is rapidly underweight, and an oncology or cystic fibrosis patient whose weight is falling are all at risk of refeeding syndrome and need the same cautious approach as the SAM child in a low-income ward. The setting changes; the metabolism does not. [4] [5]
Differential Diagnosis
The first task is to separate true acute malnutrition from its mimics, and within malnutrition to separate a primary (dietary) cause from a secondary one driven by disease. Bilateral pitting oedema, the hallmark of kwashiorkor, must be distinguished from other causes of oedema in a child: nephrotic syndrome (heavy proteinuria and hypoalbuminaemia), heart failure, liver disease, allergic or renal causes, and severe anaemia. The wasted, oedematous malnourished child is the one to recognise and not to miss behind another diagnosis. [1] [11]
Faltering growth and wasting can also be the presentation of an underlying organic illness rather than simple underfeeding. Inflammatory bowel disease, coeliac disease, cystic fibrosis, chronic liver disease, malignancy, chronic infection including tuberculosis and HIV, and endocrine causes such as hyperthyroidism or diabetes can all present with weight loss. The clue is a child who fails to recover with adequate feeding, or whose story does not fit a dietary cause, and in whom the weight loss is one symptom among others. [11] [1]
Primary (dietary) malnutrition
- History of inadequate intake or food insecurity
- No organ-specific symptoms or signs
- Improves with adequate feeding
- Often social determinants at the root
Secondary (disease-driven) malnutrition
- Faltering growth despite apparently adequate intake
- Organ-specific clues: diarrhoea, recurrent infections, organomegaly
- IBD, coeliac disease, cystic fibrosis, malignancy, HIV, TB
- Will not recover until the cause is treated
Oedema mimics (not kwashiorkor)
- Nephrotic syndrome: heavy proteinuria, hypoalbuminaemia
- Heart failure, liver disease, severe anaemia, allergy
- Usually no marked wasting
- Distinguished by urinalysis and the clinical context
Clinical & Bedside Assessment
The focused assessment answers three questions: how severe is the malnutrition, is it complicated, and what is driving it. Weigh the child, measure length or height, plot a weight-for-height z-score, and measure the MUAC at the midpoint of the relaxed left upper arm with a colour-coded tape. Then test for bilateral pitting oedema by pressing a thumb for a few seconds on the top of both feet and watching for a persistent pit. Any one of a low z-score, a red MUAC, or pitting oedema establishes SAM. [1] [12]
Assessing hydration is harder in malnutrition than in a well-fed child, because the wasted child's signs are blunted and the oedematous child's signs are misleading. Look for thirst, sunken eyes, a slow skin pinch, dry mouth and reduced urine, but weigh the whole picture rather than any single sign. Critically, a malnourished child with dehydration is rehydrated with ReSoMal, not standard oral rehydration solution, because the wasted heart cannot handle the sodium load. [1] [11]
Take a history that probes the feeding itself, the social context, and any underlying illness. Ask about the child's diet and intake, breastfeeding and weaning, recent illness, diarrhoea and infections, the family's food security, and any chronic condition, disability or surgery that limits intake or absorption. Examine for fever or hypothermia, signs of respiratory infection, a distended or tender abdomen, and the dermatosis and hair changes of kwashiorkor, and screen for HIV and tuberculosis where relevant. Each finding feeds back into the complicated-versus-uncomplicated decision. [1] [11]
Investigations
Anthropometry is the primary investigation, and in uncomplicated outpatient SAM managed with RUTF it is often the only one needed. The diagnosis rests on the weight-for-height z-score, the MUAC, and the oedema assessment, not on blood tests, and over-investigation of a stable child adds nothing. Confirming the severity correctly and plotting it over time is the test that matters. [1] [12]
For the child admitted with complicated SAM, blood tests become essential, and their purpose is twofold: to find the dangerous biochemical states and to monitor the refeeding. On admission check blood glucose, electrolytes including phosphate, potassium and magnesium, a full blood count, and tests for infection such as malaria, blood culture and HIV depending on the setting. Hypoglycaemia is common and lethal, so a bedside glucose is done immediately in any drowsy or cold child. [1] [11]
Infection screening follows the setting. In endemic areas, test for malaria and HIV and consider tuberculosis; blood cultures and a chest radiograph are part of evaluating the febrile or severely oedematous child, because bacteraemia and pneumonia are common in SAM and often contribute to death. The point of investigation in SAM is to find the treatable threats early, not to catalogue the malnutrition, which the tape and the scale have already measured. [11] [9]
Management — Resuscitation
The immediate threats in a child with complicated SAM are hypoglycaemia, hypothermia, dehydration, infection and electrolyte derangement, and these are addressed before any weight gain is attempted. The whole stabilisation phase, which usually lasts several days, is deliberately a holding operation: you correct the acute dangers and keep the child alive, and you do not try to make the child grow. [1] [11]
Prevent and treat hypoglycaemia first. A malnourished child has low glycogen and little fat, so glucose runs out fast during illness. Check a bedside glucose, give feeds every few hours day and night, and treat proven hypoglycaemia with intravenous dextrose followed by oral or nasogastric feeds. Keep the child warm to prevent hypothermia, because a cold malnourished child becomes hypoglycaemic, and the two reinforce each other. [1] [11]
Treat infection early and empirically, because nearly every child with complicated SAM has infection, and it may be occult. Give broad-spectrum antibiotics to the sick, febrile or severely oedematous child, add antimalarial treatment where relevant, and correct the electrolyte deficits of potassium and magnesium that are routine in SAM. Give thiamine before feeding begins, because the coming carbohydrate load will consume it. Iron is deliberately withheld in this phase, because early iron can worsen infection and oxidative stress, and it is introduced only later in rehabilitation. [1] [9]
Management — Definitive & Stepwise
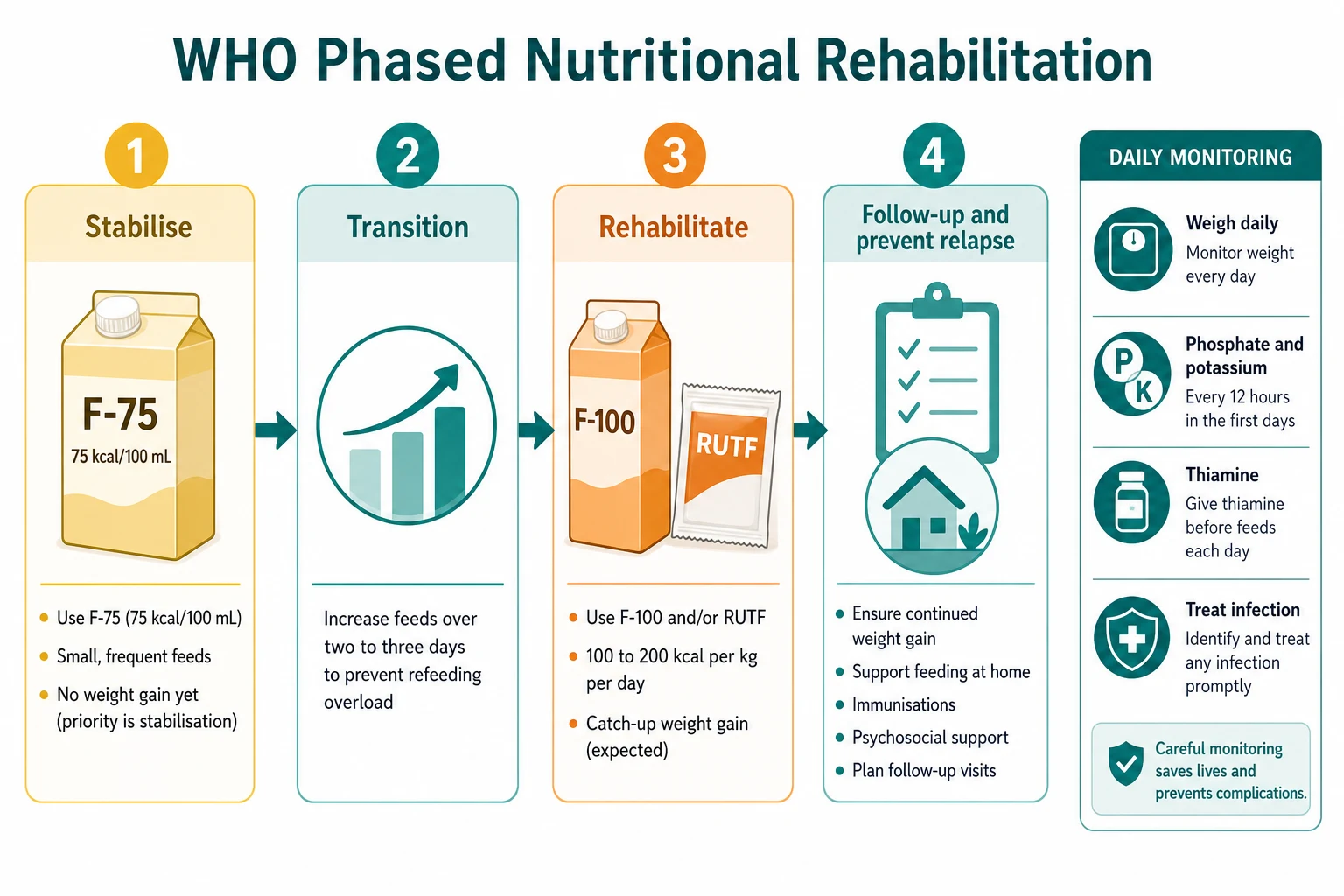
Once the acute threats are controlled, rehabilitation proceeds in the WHO's phased way: stabilise, transition, rehabilitate, and follow up. The figure shows the whole arc, and the principle behind it is that you do not rush. The stabilisation phase uses F-75 to keep the child safe without weight gain; the transition phase increases the feed cautiously to prepare the metabolism; the rehabilitation phase switches to F-100 or RUTF to drive catch-up growth; and the follow-up phase sustains recovery and prevents relapse. [1] [2]
[1] [2]F-75 is the stabilisation formula. It supplies about 75 kcal per 100 mL, is low in protein and sodium, and is given as small, frequent feeds (often by nasogastric tube in the very weak child) to provide roughly 100 kcal per kg per day. The deliberate aim of this phase is stability, not growth, because the metabolism cannot yet handle the demands of catch-up. F-100 and ready-to-use therapeutic food come later, once the child is stable and hungry, to supply the energy and protein needed for rapid weight gain. [1] [10]
Therapeutic feeds and rehydration in SAM
The transition from stabilisation to rehabilitation is the moment of greatest refeeding danger, because the feed changes from the cautious F-75 to the energy-dense F-100 or RUTF. Increase the feed gradually over a few days, keep checking phosphate and potassium, and watch for the oedema of fluid overload or the rapid breathing of heart failure. Studies of inpatient SAM units have found a high incidence of refeeding syndrome during exactly this transition from F-75 to ready-to-use therapeutic feeds, which is why vigilance rises here rather than falling. [8] [3]
Severity of acute malnutrition and its setting
Complicated SAM
Appetite loss, severe oedema, infection or dehydration; inpatient F-75 stabilisation with full monitoring
Out in the community, uncomplicated SAM is treated with ready-to-use therapeutic food through the community-based management of acute malnutrition. RUTF is an energy-dense, lipid-based paste that needs no preparation or refrigeration, so a carer can give it at home, and the child returns periodically for weight, MUAC and oedema checks until recovery. This community model has transformed SAM treatment by bringing it out of the hospital for the majority of children who are well enough to eat. [1] [11]
Specific Subtypes & Scenarios
The infant under six months with SAM is a special case, because the older child's MUAC cut-offs and RUTF regimens do not directly apply. Management prioritises re-establishing effective breastfeeding or providing expressed breast milk or an appropriate infant formula, with very cautious feeding and close inpatient monitoring, because these tiny infants are at high risk of hypoglycaemia, hypothermia and refeeding problems. Admission and specialist input are the rule for the severely malnourished young infant. [1] [11]
Oedematous malnutrition, kwashiorkor, needs the same phased care as marasmus but carries its own warnings. These children are more fragile during refeeding, the fluid shifts are treacherous, and the skin and liver involvement demand gentle handling. The oedema itself is a marker of severity, and its gradual resolution as the child recovers is one of the signs that rehabilitation is working. [1] [11]
Refeeding syndrome in the high-resource setting is most often seen not in classic SAM but in adolescents with anorexia nervosa and in children with oncology or chronic-disease malnutrition. The ASPEN consensus and the WHO SAM guidance share the same biology but differ in detail: the WHO pathway refeeds SAM with cautious F-75 and electrolyte monitoring, while ASPEN and NICE guidance for at-risk patients in high-resource settings start at reduced energy and advance only as phosphate and potassium remain stable, with thiamine given beforehand. Either way, the rule is the same: start low, go slow, and watch the electrolytes. [5] [4]
The HIV-exposed or HIV-positive malnourished child combines two dangers, because HIV both causes and worsens malnutrition and raises the mortality of SAM. Management integrates nutritional rehabilitation with HIV testing and antiretroviral treatment, while watching for the interactions between infection, refeeding and drug therapy. These children need a longer and more intensive course and a multidisciplinary team. [1] [11]
A child who relapses after recovery is the failure that follow-up is designed to prevent. Relapse usually means the child went home to the same food insecurity or untreated illness, so the response is to re-evaluate the cause, re-treat the malnutrition, and strengthen the discharge plan with realistic feeding support and closer review. Each relapse should prompt a search for an underlying driver that was missed the first time. [1] [11]
Complications & Pitfalls
The dominant complications of SAM and its treatment are the metabolic and infectious ones. Refeeding syndrome, with its hypophosphataemia, hypokalaemia, hypomagnesaemia, fluid overload and thiamine depletion, is the signature iatrogenic danger and can cause arrhythmia, heart failure, respiratory failure and death within days of starting feeds. Intercurrent infection, hypoglycaemia, hypothermia, and congestive heart failure during transition round out the threats that kill malnourished children in hospital. [4] [3]
REFEED
The classic pitfalls are the errors of rushing and of treating a malnourished child like a well-nourished one. Giving standard ORS or a rapid intravenous bolus, advancing the feed too fast, introducing iron during stabilisation, missing an occult infection, or assuming a normal admission phosphate makes the child safe, are each avoidable mistakes that turn a recoverable child into a dying one. Each is prevented by discipline and by the monitoring bundle, not by any investigation. [1] [6]
Congestive heart failure during transition or rehabilitation is the feared cardiac complication, and it presents as increasing respiratory rate, a gallop, an enlarging liver and spreading oedema as the feeds become energy-dense. The response is to stop or reduce the feed, give a cautious diuretic, and manage the fluid and electrolytes, because the wasted heart has little reserve. Recognising it early and never over-feeding is what prevents it. [8] [4]
Prognosis & Disposition
With correct rehabilitation the prognosis of SAM is good, and most children recover fully and resume growth, which is why the WHO phased approach exists. The outcome worsens sharply when treatment is delayed, when infection or HIV complicates the picture, or when refeeding syndrome, hypoglycaemia or heart failure go unrecognised. A prospective cohort of inpatient SAM found that the risk factors for death during treatment centred on infection and metabolic collapse, underlining that survival hinges on the resuscitation and monitoring, not on the calories alone. [11] [1]
The disposition between inpatient and outpatient care turns on the complicated-versus-uncomplicated judgement. Admit the child with appetite loss, severe oedema, fever, dehydration, significant infection, or any instability, and treat the stable, hungry child with uncomplicated SAM in the community with RUTF. The threshold for admission is lower for the young infant, the HIV-positive child, and the child whose family cannot safely manage at home. [1] [11]
Discharge and follow-up are themselves treatment. Discharge only when the child is eating well, gaining weight, free of oedema, and medically stable, and link the family to a clear follow-up plan with periodic weight and MUAC checks until sustained recovery. Sustained weight gain, resolution of oedema, and a MUAC moving out of the danger zone are the targets that confirm recovery, and follow-up is what prevents the relapse that otherwise follows discharge into unchanged circumstances. [1] [11]
Special Populations
The young infant under six months is the most fragile, with little metabolic reserve and a dependence on breast milk. These infants need admission for stabilisation, re-establishment of breastfeeding or careful formula feeding, and close monitoring for hypoglycaemia and refeeding problems, because the older child's protocols do not transfer directly. Specialist paediatric and dietetic input are essential. [1] [11]
Children with cerebral palsy, neurodisability or feeding disorders form a growing share of the malnutrition seen in high-resource settings. Their wasting is often a consequence of unsafe swallowing, inadequate intake, or increased needs, and their rehabilitation combines careful enteral feeding, sometimes via a feeding tube, with management of the underlying condition. These children are also at risk of refeeding syndrome and warrant the same cautious approach and electrolyte monitoring as any SAM child. [4] [5]
For Indigenous, remote, refugee and socioeconomically disadvantaged children in Australia and New Zealand, malnutrition is as much a social disease as a medical one, and effective care must address food security, access to care, and cultural safety alongside the feeding. Closing the equity gap means bringing growth monitoring, oral and therapeutic feeding, and reliable follow-up to the children furthest from care, and recognising that relapse is often a signal of unmet social need rather than treatment failure. [11] [1]
The child with a chronic disease, such as cystic fibrosis, inflammatory bowel disease, chronic liver disease or malignancy, has secondary malnutrition that will not resolve until the underlying illness is controlled. Their rehabilitation is integrated with disease treatment, and they are a high-risk group for refeeding syndrome, so the same principles of cautious feeding and electrolyte monitoring apply, adjusted to the disease. [4] [5]
Evidence, Guidelines & Regional Differences
The evidence base for SAM treatment is strong and unusually consistent in its principles, though some details remain contested. International guidance, anchored in the WHO framework, converges on the phased approach: stabilise with F-75, correct electrolytes and infection, transition cautiously, rehabilitate with F-100 or RUTF, and monitor for refeeding syndrome throughout. The community-based model with RUTF has brought effective treatment to most uncomplicated SAM children. [1] [3]
The energy targets have been the subject of recent debate. A commentary on the updated WHO guideline argued that the requirement for therapeutic feeding may overestimate what is needed, highlighting that even the bedrock numbers in this field are still being refined and that careful, individualised feeding matters more than a single target. The principle of cautious, monitored advancement, however, is not in dispute. [2] [1]
Antibiotics in SAM illustrate how evidence shapes practice. WHO recommends empirical antibiotics for SAM, and trials comparing agents, such as azithromycin against amoxicillin for uncomplicated SAM, have refined the choice without overturning the principle that infection is pervasive and must be treated or covered. Thiamine adequacy in F-75 has also been questioned, supporting the practice of giving thiamine before refeeding rather than assuming the formula alone suffices. [9] [10]
Regional differences are practical rather than definitional. In low-resource, high-burden settings the emphasis is on the community RUTF model, scaling treatment to the many, and managing refeeding within resource-limited inpatient units. In Australia and New Zealand the disease is rarer and more often secondary, so the emphasis shifts to recognising malnutrition in chronic disease, disability and eating disorders, and to applying the same refeeding-syndrome safeguards that ASPEN and NICE guidance set out for at-risk patients. The biology is the same everywhere; the setting changes the priorities. [4] [5]
Exam Pearls
Hold one sentence for the viva: a child with severe acute malnutrition, defined by a weight-for-height z-score below minus three, a MUAC below 115 mm, or bilateral pitting oedema, is rehabilitated in the WHO phased way, stabilising with F-75 at about 100 kcal per kg per day, transitioning cautiously, then driving catch-up growth with F-100 or ready-to-use therapeutic food, while monitoring phosphate, potassium and magnesium and giving thiamine to prevent refeeding syndrome. [1] [3]
State the frequently tested facts correctly. SAM is WHZ below minus 3, MUAC below 115 mm, or bilateral pitting oedema. F-75 is 75 kcal per 100 mL for stabilisation; F-100 is 100 kcal per 100 mL for catch-up. The refeeding bundle is phosphate, potassium, magnesium plus thiamine. Use ReSoMal, not standard ORS, for the dehydrated malnourished child. Iron is withheld in stabilisation and introduced in rehabilitation. Appetite loss means complicated SAM and inpatient care. [1] [6]
The high-yield pairings carry the reasoning: a wasted child with appetite loss or infection is complicated SAM, admit; a wasted child who eats RUTF and is otherwise well is uncomplicated SAM, treat in the community; a child whose phosphate falls after feeding starts has refeeding syndrome, slow the feed and correct electrolytes; and an oedematous child has SAM regardless of weight. Always refeed cautiously and watch the electrolytes, because the treatment is food but food given wrongly can kill. [8] [5]
References
- [1]Lenters LM; Wazny K; Webb P; et al Treatment of severe and moderate acute malnutrition in low- and middle-income settings: a systematic review, meta-analysis and Delphi process. BMC Public Health, 2013.PMID 24564235
- [2]Sachdev HS; Kurpad AV The recent WHO guideline on acute malnutrition overestimates therapeutic energy requirement. Lancet Reg Health Southeast Asia, 2024.PMID 38807646
- [3]Mogase T; Van Onselen A; Rodriguez-Sanchez N; et al The Identification and Management of Refeeding Syndrome in Inpatient Severely Acutely Malnourished Children Aged 6 to 59 Months in Sub-Saharan African Countries: A Systematic Review and Meta-Analysis. Children (Basel), 2025.PMID 41007088
- [4]Corsello A; Trovato CM; Dipasquale V; et al Refeeding Syndrome in Pediatric Age, An Unknown Disease: A Narrative Review. J Pediatr Gastroenterol Nutr, 2023.PMID 37705405
- [5]da Silva JSV; Seres DS; Sabino K; et al ASPEN Consensus Recommendations for Refeeding Syndrome. Nutr Clin Pract, 2020.PMID 32115791
- [6]Namusoke H; Hother AL; Rytter MJ; et al Changes in plasma phosphate during in-patient treatment of children with severe acute malnutrition: an observational study in Uganda. Am J Clin Nutr, 2016.PMID 26739034
- [7]Hother AL; Girma T; Rytter MJ; et al Serum phosphate and magnesium in children recovering from severe acute undernutrition in Ethiopia: an observational study. BMC Pediatr, 2016.PMID 27814707
- [8]Muzeyi W; Ochieng Andra T; Oriokot L; et al High Incidence of Refeeding Syndrome during the Transition from F75 to Ready-to-Use Therapeutic Feeds among Children 6 to 59 Months with Severe Acute Malnutrition at the Pediatric Nutritional Unit of Mulago Hospital. J Nutr Metab, 2024.PMID 39372094
- [9]O'Brien KS; Sie A; Dah C; et al Comparing Azithromycin to Amoxicillin in the Management of Uncomplicated Severe Acute Malnutrition in Burkina Faso: A Pilot Randomized Trial. Am J Trop Med Hyg, 2022.PMID 35008055
- [10]Hiffler L; Adamolekun B; Fischer PR; et al Thiamine content of F-75 therapeutic milk for complicated severe acute malnutrition: time for a change? Ann N Y Acad Sci, 2017.PMID 28905406
- [11]Rytter MJ; Babirekere-Iriso E; Namusoke H; et al Risk factors for death in children during inpatient treatment of severe acute malnutrition: a prospective cohort study. Am J Clin Nutr, 2017.PMID 28031190
- [12]Lamsal KP; Parajuli KR; Pun BK; et al Accuracy of Using Mid-Upper Arm Circumference to Detect Wasting Among Children Aged 6-59 Months in Nepal. Glob Health Sci Pract, 2021.PMID 34933983