Paeds · gastroenterology-hepatology-and-nutrition
Malrotation and volvulus
Also known as Intestinal malrotation · Midgut volvulus · Rotational abnormality · Ladd bands · Ladd procedure · Non-rotation · Corkscrew sign · Whirlpool sign · Duodenojejunal flexure · Short gut syndrome from volvulus · Intermittent volvulus
Fellowship guide to intestinal malrotation and midgut volvulus, the one rotational anomaly that turns a well neonate into a surgical catastrophe within hours. The page follows the embryology that builds the narrow mesenteric stalk, the bilious vomiting that demands an upper gastrointestinal contrast study, the whirlpool and corkscrew signs, and the Ladd procedure that untwists the volvulus, divides the bands and widens the base so the midgut cannot twist again.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a three-day-old baby who fed and stooled normally, then suddenly vomits a mouthful of bright green fluid. That single colour changes everything, because in a neonate it points first and fastest to malrotation with midgut volvulus, the one condition that can strangle the entire small bowel within hours. Bile is green because it enters the gut beyond the ampulla of Vater, so green vomit places the obstruction at or below the second part of the duodenum, and the diagnosis you must exclude before any other is a midgut that is twisting on an abnormally narrow mesenteric stalk. [1] [2]
Intestinal malrotation is an abnormality of the gut's embryological rotation and fixation in which the bowel is not anchored on the broad, stable mesenteric base that normally holds it. The midgut, which runs from the distal duodenum to the proximal two-thirds of the transverse colon and is supplied by the superior mesenteric artery, normally settles with the duodenojejunal flexure fixed high on the left and the caecum fixed low on the right, creating a wide diagonal base that cannot twist. When rotation is incomplete the base stays short and narrow, the midgut dangles from a pedicle around the artery, and a clockwise twist of that pedicle is a midgut volvulus. [2] [8]
The task in the emergency is therefore to act on the pattern of bilious vomiting, not to wait for proof of the anatomy. You keep the child nil by mouth, decompress the stomach, resuscitate and involve a surgeon at once, because the cost of treating a benign cause as an emergency is small while the cost of missing a volvulus is the loss of the entire midgut. Most neonates with bilious vomiting turn out to have something less dangerous, yet every episode earns the same urgent respect, and a normal plain film never closes the question. [1] [3]
Classification
Rotational anomalies are best understood as a spectrum of incomplete rotation, and what matters clinically is whether the narrow base that results has twisted. A child may carry a malrotation silently for years, present acutely with a strangulating volvulus in the first weeks of life, or surface in adolescence with intermittent symptoms from repeated partial twisting. The figure separates these three presentations so the urgency of each is clear before the anatomy is named. [8] [2]
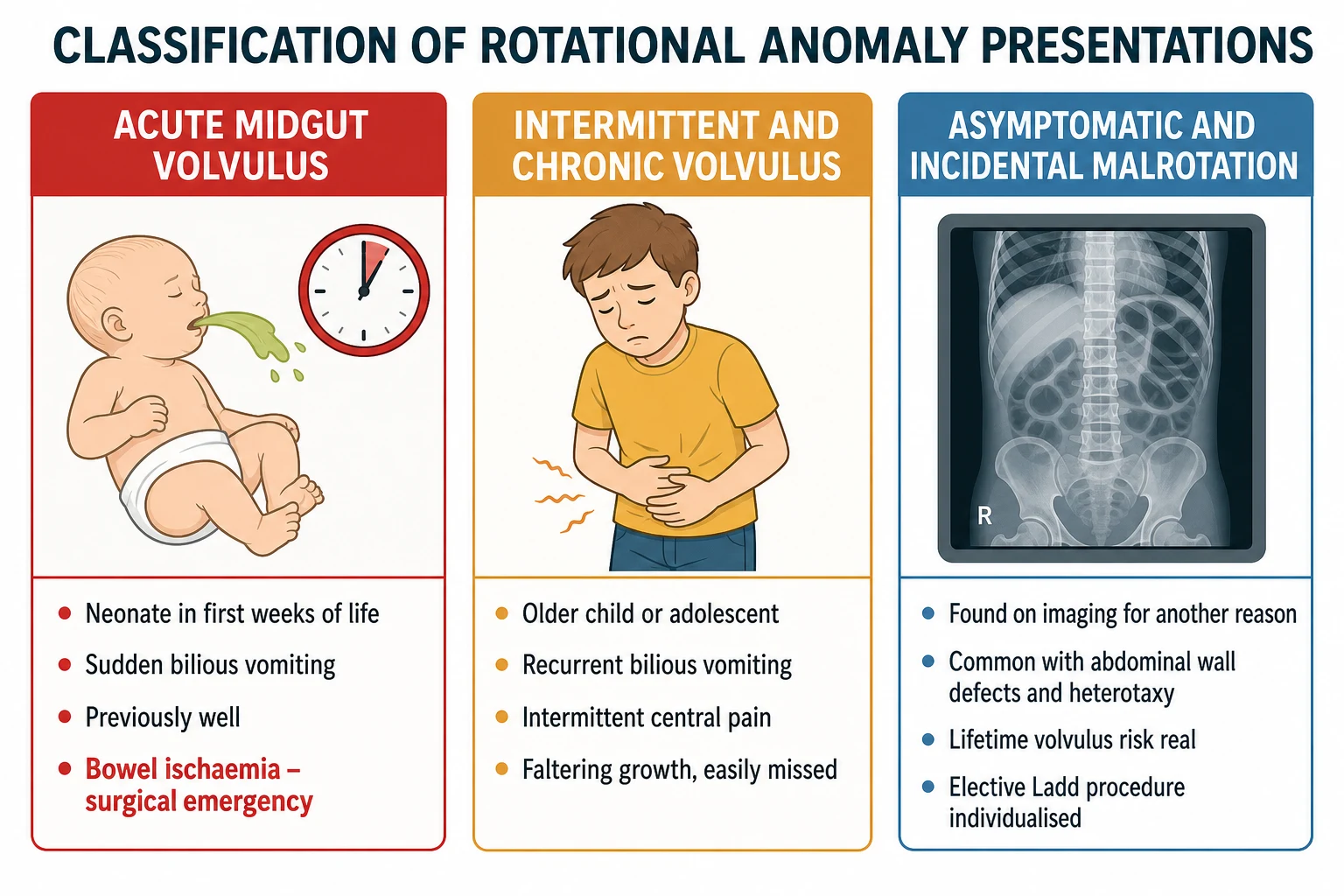
The acute presentation dominates the emergency and the exam. A previously well term neonate, most often in the first month of life, vomits bile and may still look comfortable, which is precisely why the colour of the vomit must drive the plan rather than the reassuring examination. The intermittent presentation is subtler and easily mislabelled as functional, with recurrent bilious vomiting, colicky central pain and faltering growth from repeated partial obstruction. The incidental presentation arrives when rotational anomaly is found on imaging done for another reason and poses the question of whether to operate electively. [3] [5]
A second axis worth holding is the mechanism of obstruction, because malrotation can block the gut in two ways. Peritoneal Ladd bands running from the abnormally placed caecum across the duodenum compress the duodenum without any twist, while a true volvulus twists the midgut on its narrow pedicle and threatens the blood supply. The bands produce obstruction; the twist produces ischaemia, and only the second is a race against infarction. [2] [6]
Acute midgut volvulus
- Previously well neonate, most often in the first month
- Sudden bilious vomiting, may look well early
- Blood in stool, distension and shock are late
- Emergency: resuscitate, image or operate, then a Ladd procedure
Intermittent volvulus
- Older child or adolescent, often missed
- Recurrent bilious vomiting and colicky central pain
- Faltering growth from repeated partial twisting
- Needs an upper gastrointestinal contrast study
Asymptomatic malrotation
- Found incidentally on imaging for another reason
- Common with heterotaxy and abdominal wall defects
- Real lifetime risk of volvulus
- Elective Ladd procedure, individualised to risk
Epidemiology & Risk Factors
Malrotation is common, which is what makes the rare but catastrophic volvulus a constant threat. It is present in roughly one in five hundred live births, yet most carriers never know they have it, and only a minority ever twist. What concentrates the danger is that when volvulus does occur it falls heavily on the very young, with most acute presentations in the first month of life and the great majority within the first year. [2] [3]
Malrotation also travels with other congenital anomalies, and these associations raise a child's baseline risk sharply. It is almost universal alongside congenital diaphragmatic hernia, omphalocele and gastroschisis, and it is common in the heterotaxy syndromes, in which the organs are arranged ambiguously and the gut is poorly fixed. Intestinal atresias and some cardiac lesions carry a higher rate too, so a child with any of these earns a low threshold for investigating bilious vomiting and often screening for rotational anomaly. [9] [8]
The epidemiology of harm is driven by time, not by frequency. The children who lose bowel are those in whom the volvulus is not relieved before the midgut infarcts, and studies of care timelines show that delay, rather than rarity of the disease, is what produces short gut syndrome and death. This is why the epidemiology translates into one clinical rule: any neonate with bilious vomiting is managed as a volvulus until an urgent contrast study or an operation says otherwise. [12] [1]
Pathophysiology
To understand why malrotation is so dangerous, follow the embryology of normal rotation. The midgut herniates into the umbilical cord at about six weeks, returns to the abdomen at about ten weeks, and in between rotates a total of two hundred and seventy degrees counterclockwise around the superior mesenteric artery. The result of that rotation is fixation: the duodenojejunal flexure comes to lie to the left of the spine at the level of the duodenal bulb, and the caecum settles low in the right iliac fossa, and together they anchor the mesentery on a broad diagonal base that cannot twist. [2] [8]
When rotation is incomplete that broad base never forms. The duodenojejunal flexure stays low and to the right, the caecum lies high and medial, and the mesentery is left hanging from a short, narrow pedicle around the superior mesenteric vessels, like a stem holding a heavy bunch of bowel. Two things then go wrong. Peritoneal Ladd bands stretch from the misplaced caecum across the duodenum and compress it, and the whole midgut, balanced on its narrow stalk, is free to twist. [2] [6]
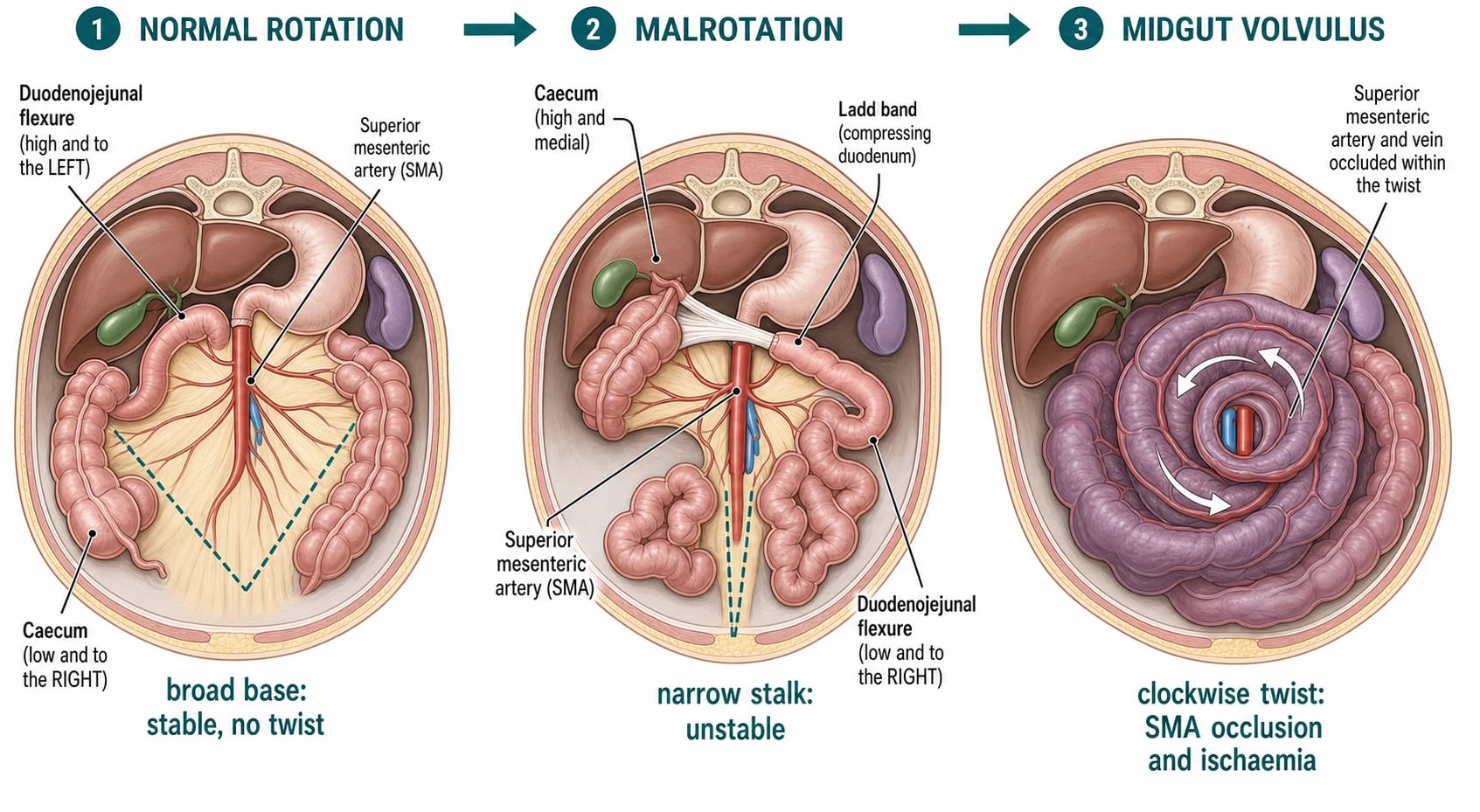
The volvulus itself is the catastrophe, and its mechanics are worth knowing precisely. The midgut rotates clockwise around the narrow pedicle, and as it tightens it first kinks the duodenum to cause bilious obstruction and then occludes the superior mesenteric artery and vein within the twist. The timeline of ischaemia drives every decision: at first the bowel is obstructed but viable and the baby vomits bile while still looking well, then venous congestion makes the bowel boggy and passes blood per rectum, and finally arterial occlusion infarcts the midgut, bringing peritonitis, shock and, unrelieved, the loss of the entire small bowel. [2] [8]
The link between the anatomy and the outcome is therefore vascular, and it explains why a well-looking baby can be minutes from disaster. The entire midgut depends on a single artery that runs through the twist, so a tight volvulus converts a clean obstruction into whole-gut ischaemia far faster than any fixed block such as an atresia ever could. This is the core teaching: malrotation is dangerous not because it obstructs, but because the obstruction sits on the mesenteric blood supply. [8] [12]
Clinical Presentation
The neonatal presentation is deceptively gentle at the start, and that gentleness is the trap. A baby who has fed and stooled normally suddenly vomits bile, and on first inspection may be alert with a soft, only slightly full abdomen. The finding that should change the plan is the green vomit, not the calm baby, because in early volvulus the bowel is obstructed but not yet infarcted and tenderness has not yet appeared. As the twist tightens the baby becomes irritable then lethargic, feeds poorly, develops distension and tenderness, and may pass blood in the stool as the bowel becomes ischaemic. [1] [2]
Beyond the newborn period the presentation broadens and is more often missed. An older child or an adolescent with an undiagnosed malrotation may have recurrent bilious vomiting, intermittent colicky central pain and faltering growth from repeated partial volvulus, a pattern that is easily written off as cyclic vomiting, reflux or functional pain. The clue that lifts it out of the functional bin is the bile, because recurrent green vomiting in any child is not functional and earns a contrast study. Some children present between attacks with non-specific dyspepsia and are only diagnosed after a volvulus finally tightens. [5] [3]
The incidental presentation has its own pitfalls. Malrotation is sometimes found on an upper gastrointestinal study, a contrast swallow or a CT done for another reason, and the question becomes whether the lifetime risk of volvulus justifies an operation. Because the risk is real and the operation is effective, the usual advice in a fit child is an elective Ladd procedure, weighed against operative risk in each case and considered especially carefully in the child with heterotaxy, where imaging alone does not predict who will twist. [4] [9]
Differential Diagnosis
The first fork in bilious vomiting is whether the cause is a surgical obstruction of the gut or not, and the safe habit is to assume it is until imaging proves otherwise. Non-surgical bilious vomiting does occur, for example transient bile-stained aspirates in a preterm baby or the slowed gut of an unwell neonate, but these are labels of exclusion reached only after a surgical cause has been actively sought and, where doubt remains, imaged. The default reflex in any neonate with green vomit is to exclude volvulus first. [1] [8]
Once a surgical cause is assumed, the level of obstruction narrows the list, and here malrotation sits firmly among the high obstructions. A high obstruction vomits bile early with little distension, and the main candidates are malrotation with volvulus, duodenal atresia and jejunal atresia. The plain film helps separate them in part, showing a double bubble in duodenal atresia and a few dilated loops in jejunal atresia, but only the upper gastrointestinal contrast study confirms or excludes malrotation, and a normal plain film never does. [7] [2]
Malrotation with volvulus
- Previously well neonate with sudden bilious vomiting
- May look well; blood and shock are late
- Upper gastrointestinal contrast is the key test
- Emergency Ladd procedure if volvulus confirmed
Duodenal atresia
- Vomiting from the first hours, often antenatal polyhydramnios
- Double bubble on the plain abdominal film
- Strong association with trisomy 21
- Planned duodenoduodenostomy, not a race against ischaemia
Intussusception
- Older infant with colicky pain and drawing up of the legs
- Sausage-shaped mass and redcurrant-jelly stool
- Ultrasound target or pseudokidney sign
- Usually reduced by air or liquid enema
In the older child the differential shifts towards intussusception, adhesional obstruction after previous surgery, an incarcerated hernia and intermittent volvulus. Intussusception classically brings colicky pain, a sausage-shaped mass and redcurrant-jelly stool and is usually reduced without an operation, while volvulus threatens the blood supply and needs surgery. The discipline throughout is to attribute the vomiting to a level and a mechanism confirmed by imaging, rather than to settle on a comfortable non-surgical label too early and let a twisting midgut go untreated. [8] [5]
Clinical & Bedside Assessment
The assessment runs in parallel with resuscitation, not after it. Look first at the vomit and confirm for yourself that it is truly bile-stained green rather than milky or yellow, because a reported colour is often softer than the reality and the bile is the finding that must drive the plan. Then assess the airway, breathing and circulation, since a child with obstruction may already be shocked from third-space and gastric losses, and examine the abdomen for distension, tenderness, guarding, visible peristalsis and any discolouration of the wall. [1] [7]
The bedside then completes the picture that guides urgency and replaces what the child is losing. Weigh the baby, chart the passage or absence of meconium, and record the losses from the nasogastric tube, because these numbers drive the fluid replacement as much as they support the diagnosis. Look for the mass of an intussusception, feel for an incarcerated hernia, and note any peritonism that would shift the plan from imaging straight to theatre, since a rigid or discoloured abdomen means the bowel may already be infarcting. [7] [8]
Investigations
Investigation is deliberately fast and targeted, because in suspected volvulus the imaging must never delay the surgeon. The first film is the plain supine abdominal radiograph, which may be entirely normal in an early volvulus, may show a gasless abdomen, a distended loop, or a paucity of bowel gas, and is most useful for what it excludes by pattern, such as the double bubble of duodenal atresia. A normal plain film never excludes malrotation, so it reassures about nothing when the suspicion is volvulus. [7] [2]
Ultrasound has a growing role and a particular strength in the neonate, where it can be done at the cot side. The whirlpool sign is the clockwise spiralling of the superior mesenteric vein around the artery, and the inversion of the normal artery-vein relationship is the sonographic fingerprint of malrotation. Sonography has good sensitivity for volvulus in skilled hands, but it does not replace the contrast study as the reference test, and a negative ultrasound in a child with bilious vomiting must not delay a contrast study or a surgical opinion. [11] [7]
The remaining tests prepare the child for theatre rather than confirm the diagnosis. Bloods for a gas, lactate, electrolytes, glucose and a group and save quantify the metabolic disturbance and the losses, and a rising lactate warns of ischaemic bowel. In the older child a CT with intravenous contrast can show the whirlpool sign of the twisted mesentery when the presentation is atypical, but the same rule holds: the unstable child is operated on, not scanned, and the imaging serves the decision rather than replacing it. [8] [12]
A neonate with bilious vomiting — the mnemonic TWIST
Management — Resuscitation
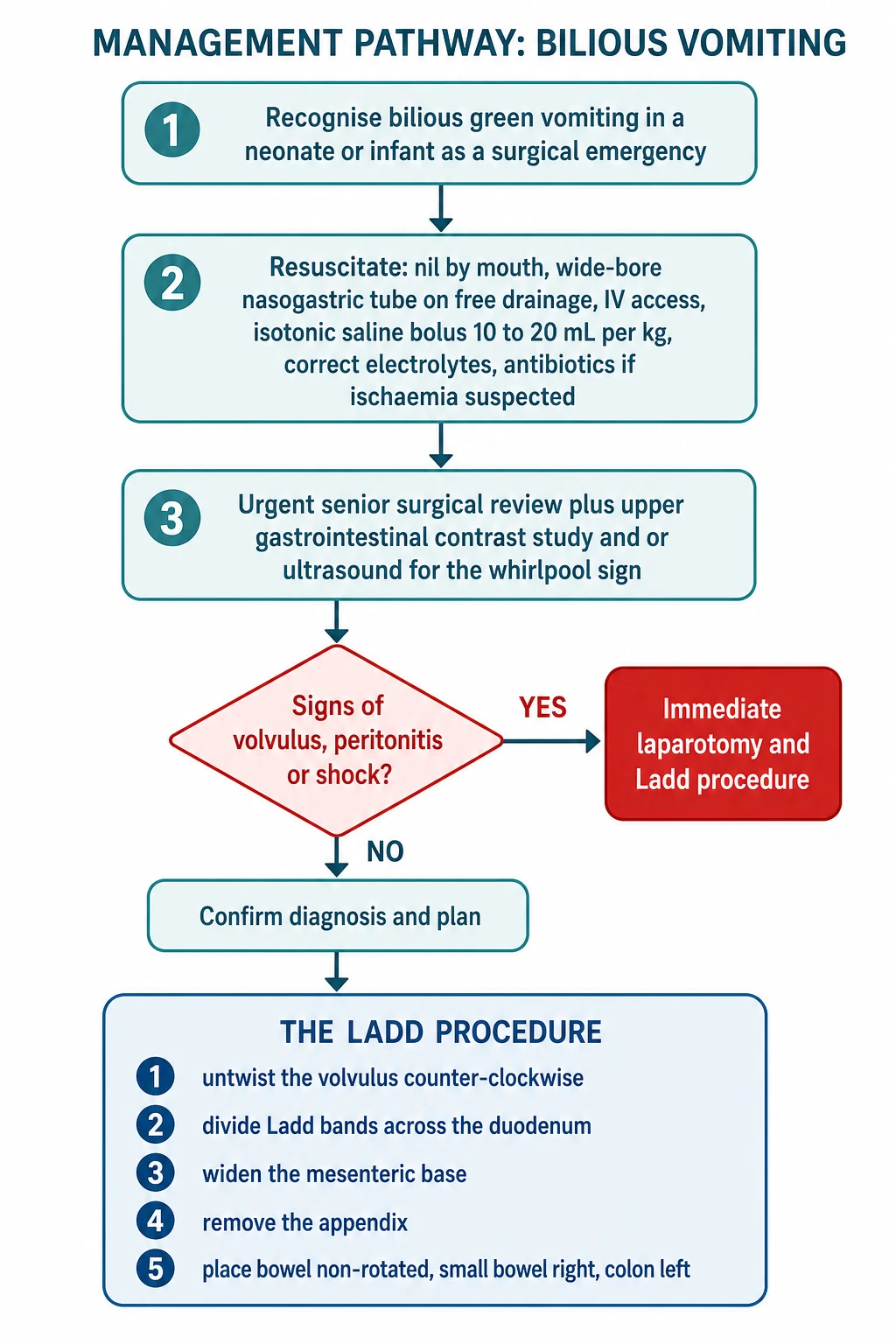
Resuscitation follows one governing rule: stabilise and decompress while you summon the surgeon, and never let a scan delay a child who is already peritonitic or shocked. Keep the child nil by mouth, secure intravenous access, and pass a wide-bore nasogastric tube on free drainage to decompress the stomach and reduce the risk of aspiration. These first minutes make the child safe for imaging or for theatre, and they begin the fluid correction that the obstruction has already made necessary. [1] [8]
Correct the circulation with volume and the biochemistry alongside it. Give a fluid bolus of 10 to 20 mL per kilogram of isotonic saline and repeat it as needed for shock, then run maintenance fluids with added potassium once urine flows, replacing the nasogastric losses millilitre for millilitre with saline and potassium because they are rich in electrolytes. Start broad-spectrum intravenous antibiotics when ischaemia, perforation or sepsis is suspected, and monitor the gas, lactate and urine output to judge the response, because these are the signs that tell you whether the bowel is still viable. [1] [12]
Management — Definitive & Stepwise
Definitive care for a confirmed volvulus is surgical, and the operation is the Ladd procedure. The figure sets out the whole route from recognition and resuscitation, through urgent imaging and the emergency decision, to the operation itself. The art is to run recognition and resuscitation together, and to escalate to surgery the moment volvulus or peritonitis is suspected rather than after it is proven, because time to untwisting is the single most important prognostic lever. [6] [12]
The Ladd procedure is the operation every candidate must be able to describe step by step. The surgeon delivers the bowel and untwists the volvulus counter-clockwise, the direction opposite to the clockwise twist, to restore perfusion. Then the Ladd bands that cross and compress the duodenum are divided, the mesenteric base is widened by straightening the duodenum along the right flank, the appendix is removed because the caecum will now lie in an atypical position on the left, and the bowel is left in a non-rotated position with the small bowel on the right and the colon on the left. Frankly necrotic bowel is resected, and when viability is borderline a second-look laparotomy is planned rather than committing to a massive resection at the first operation. [6] [2]
The choice between an open and a laparoscopic approach depends on the setting. The acute volvulus with possible ischaemia is generally managed by open laparotomy, which allows full assessment of bowel viability and rapid detorsion. For the asymptomatic or chronic malrotation found electively, the laparoscopic Ladd procedure is increasingly used and is safe in experienced hands, with similar low rates of recurrent volvulus, though the open operation remains the standard against which it is measured. The decision rests with the surgeon and is shaped by stability, habitus and expertise. [10] [4]
Specific Subtypes & Scenarios
Acute midgut volvulus in the neonate is the scenario every candidate must own. The classic case is a term neonate in the first weeks who vomits bile, and the correct reflex is resuscitation, decompression, urgent surgical referral and an upper gastrointestinal contrast study, moving straight to laparotomy if the child is unstable. The prize for speed is a viable midgut and a Ladd procedure, and the penalty for delay is short gut syndrome from a necrotic small bowel, which is why the time from onset of bilious vomiting to untwisting is the outcome that matters most. [2] [12]
Intermittent and chronic volvulus is the missed diagnosis that examiners love to probe. Older children and adolescents present with recurrent bilious vomiting, intermittent central or epigastric pain, and sometimes faltering growth, and the symptoms resolve between attacks, so the label of functional or cyclic vomiting is often applied first. The finding that should prompt imaging is the bile, because bilious vomiting is never functional, and an upper gastrointestinal contrast study in a well interval can still show the abnormal duodenojejunal flexure or a corkscrew that betrays the twist. [5] [3]
Asymptomatic and incidentally found malrotation raises a genuine management question. Because the lifetime risk of volvulus is real and the Ladd procedure is effective, the usual advice for a fit child is an elective operation, and this is the recommendation of the American Pediatric Surgical Association systematic review, which weighs the risk of volvulus against operative risk in each child. In heterotaxy the decision is harder, because imaging does not predict which child will twist, so a prospective strategy of risk-stratified surveillance and selective surgery is increasingly favoured over universal operation. [4] [9]
Complications & Pitfalls
The complications follow the twin threats of ischaemia and delay. A volvulus that is not relieved in time infarcts the midgut and leaves the child with short gut syndrome, lifelong dependence on parenteral nutrition and its liver and line complications, and in the worst case death from loss of the entire small bowel. Perforation seeds peritonitis and sepsis, and the metabolic cost of vomiting and third-space loss is dehydration and electrolyte derangement that can cause collapse before the abdomen ever looks dramatic. [2] [8]
The pitfalls cluster around underestimating bilious vomiting and trusting the wrong reassurance. The classic error is to be reassured by a well-looking baby with a soft abdomen and to delay imaging or referral, allowing an early volvulus to progress to infarction. A second error is to accept a normal plain film as evidence against malrotation, when only the upper gastrointestinal contrast study or the operation can exclude it. A third is to under-resuscitate, treating the diagnosis while ignoring the shock the losses have already caused. [1] [12]
Prognosis & Disposition
Outcome is dominated by how quickly a volvulus is relieved. When the diagnosis is made and the Ladd procedure performed before infarction, the great majority of children recover fully with an excellent long-term prognosis and a low, though real, risk of recurrent volvulus or later adhesional obstruction. When diagnosis is delayed and extensive midgut is lost, the child faces short gut syndrome, prolonged parenteral nutrition and a far harder course, which is why time to theatre is the single most important prognostic lever and why care timelines have become a quality measure. [3] [12]
The elective and chronic presentations generally do well with timely surgery. Children operated on for asymptomatic malrotation or intermittent volvulus have low morbidity and a low rate of recurrence when the Ladd procedure is complete, and their long-term outlook is that of a child with normally functioning bowel. The children who face the hardest road are those who present with established infarction, for whom the question shifts from saving the midgut to optimising life with short gut through nutrition, intestinal rehabilitation and, in some, transplantation. [4] [10]
Disposition reflects the acuity. A child with confirmed or suspected volvulus needs a paediatric surgical centre and often retrieval from a smaller hospital, with resuscitation and decompression continued throughout transfer. After surgery the child needs monitoring for anastomotic and feeding progress, nutritional support where bowel has been lost, and long-term follow-up for those left with short gut, so that clear safety-netting is given to families whenever bilious vomiting is assessed and a benign cause is accepted. [1] [3]
Special Populations
Children with heterotaxy and complex congenital anatomy carry a higher baseline risk and a harder decision. Malrotation is common in heterotaxy syndromes, in which the gut is poorly fixed alongside the cardiac and splenic anomalies, so these children warrant a low threshold for investigating bilious vomiting and are often screened for rotational anomaly. The management is debated, because imaging does not predict who will twist, and a prospective strategy of risk-stratified surveillance and selective surgery is increasingly used rather than operating on every child. [9] [8]
Children with abdominal wall defects and congenital diaphragmatic hernia travel with malrotation almost by default. The bowel is externally herniated or compressed during development, normal fixation fails, and the narrow base persists after repair, so these children deserve a low threshold for imaging any bilious vomiting and often a planned assessment of rotation. The same vigilance applies to children with intestinal atresias and some cardiac lesions, in whom malrotation is found more often than in the general population. [8] [4]
Geography shapes safety for many families. In Australia and New Zealand a neonate with bilious vomiting in a rural, remote or Indigenous community may be hours from a paediatric surgical centre, so early recognition, resuscitation, nasogastric decompression and prompt discussion with a retrieval service are what protect the midgut. Building the reflex to treat bilious vomiting as an emergency into every rural and general setting is therefore an equity issue as much as a clinical one, because the midgut does not wait for geography. [1] [3]
Evidence, Guidelines & Regional Differences
The evidence base blends classic anatomical and clinical series with modern imaging and surgical reviews. The principle that bilious vomiting in a neonate is a surgical emergency until proven otherwise comes from clinical series that showed only a minority of such babies have a surgical cause, yet that the surgical causes are dangerous, and it underpins the safe default of treating every episode as an emergency. Historical and contemporary reviews of malrotation establish the upper gastrointestinal contrast study as the reference test and the Ladd procedure as the definitive operation. [1] [2]
Where evidence is softer, controversy remains. The management of incidentally discovered asymptomatic malrotation is debated, and the American Pediatric Surgical Association systematic review supports an individualised approach that weighs the real risk of volvulus against operative risk rather than mandating surgery for all. In heterotaxy, prospective data show that imaging does not predict the need for surgery, so a surveillance strategy is increasingly favoured, and the identification of malrotation in older children, whose intermittent symptoms are easily mislabelled, is an area where a higher index of suspicion and readier contrast imaging are advocated. [4] [9]
Regional practice is consistent in principle and variable in logistics. The rule that bilious vomiting in a neonate is a surgical emergency is universal, but access to paediatric surgery, interventional radiology and rapid retrieval differs between and within countries. The laparoscopic Ladd procedure has widened the options for the elective case, and modern reviews of care timelines have made time to surgery a measured quality indicator, so that the evidence now serves not only the diagnosis but the system that surrounds it. [10] [12]
Exam Pearls
Hold one sentence above all others: bilious vomiting in a neonate is malrotation with midgut volvulus until proven otherwise. State the reflex that follows without hesitation, which is to keep the child nil by mouth, pass a nasogastric tube, secure intravenous access, call the surgeon, and arrange an urgent upper gastrointestinal contrast study, going straight to laparotomy if the child is unstable or peritonitic. This is the answer that saves both marks and midguts. [1] [2]
Get the frequently tested facts exactly right. The normal midgut rotates two hundred and seventy degrees counterclockwise, and a volvulus twists clockwise, so the surgeon detorses it counterclockwise. The diagnostic imaging sign of malrotation is an abnormally placed duodenojejunal flexure low and to the right, with a corkscrew or bird-beak in volvulus, and the ultrasound clue is the whirlpool sign of the superior mesenteric vein twisting around the artery. The operation is the Ladd procedure, whose steps are detorse, divide the bands, widen the base, remove the appendix and place the bowel non-rotated. [7] [6]
The high-yield pairings do the work in a viva. A previously well neonate with sudden bilious vomiting needs a Ladd procedure for midgut volvulus; a baby vomiting from birth with a double bubble has duodenal atresia; an older child with recurrent bilious vomiting and central pain has intermittent volvulus on a missed malrotation; and a child found to have malrotation by chance faces an elective Ladd procedure once the risk is weighed. Always resuscitate and decompress before you image, and never let a normal plain film reassure you. [5] [4]
References
- [1]Godbole P; Stringer MD Bilious vomiting in the newborn: How often is it pathologic? J Pediatr Surg, 2002.PMID 12037761
- [2]Lampl B; Levin TL; Berdon WE; Cowles RA Malrotation and midgut volvulus: a historical review and current controversies in diagnosis and management. Pediatr Radiol, 2009.PMID 19241073
- [3]Salehi Karlslätt K; Husberg B; Ullberg U; Nordenskjöld A Intestinal Malrotation in Children: Clinical Presentation and Outcomes. Eur J Pediatr Surg, 2024.PMID 36882104
- [4]Graziano K; Islam S; Dasgupta R; Lopez ME Asymptomatic malrotation: Diagnosis and surgical management: An American Pediatric Surgical Association outcomes and evidence based practice committee systematic review. J Pediatr Surg, 2015.PMID 26205079
- [5]Dekonenko C; Sujka JA; Weaver K; Sharp SW The identification and treatment of intestinal malrotation in older children. Pediatr Surg Int, 2019.PMID 30810798
- [6]Ingoe R; Lange P The Ladd's procedure for correction of intestinal malrotation with volvulus in children. AORN J, 2007.PMID 17292689
- [7]Choi G; Je BK; Kim YJ Gastrointestinal Emergency in Neonates and Infants: A Pictorial Essay. Korean J Radiol, 2022.PMID 34983099
- [8]Svetanoff WJ; Srivatsa S; Diefenbach K; Nwomeh BC Diagnosis and management of intestinal rotational abnormalities with or without volvulus in the pediatric population. Semin Pediatr Surg, 2022.PMID 35305800
- [9]Collins GL; Hargis-Villanueva AE; Jayaraman MS; Lai K A Prospective Management Strategy for Heterotaxy Syndrome with Intestinal Rotation Abnormalities: Imaging Does Not Predict Need for Surgery. J Pediatr Surg, 2023.PMID 36740478
- [10]Johnston WR; Hwang R; Mattei P Laparoscopic Versus Open Ladd Procedure for Midgut Malrotation. J Pediatr Surg, 2024.PMID 39209687
- [11]Zhang W; Sun H; Luo F The efficiency of sonography in diagnosing volvulus in neonates with suspected intestinal malrotation. Medicine, 2017.PMID 29049228
- [12]Sabac D; Briatico D; Fitzgerald P Assessment of care timelines in intestinal malrotation with volvulus: A retrospective chart review. J Pediatr Surg, 2023.PMID 36805138