Paeds · gastroenterology-hepatology-and-nutrition
Non-alcoholic fatty liver disease in children
Also known as Paediatric NAFLD · Metabolic dysfunction-associated steatotic liver disease in children · Paediatric MASLD · Paediatric MASH · Fatty liver disease in children
Fellowship guide to paediatric fatty liver disease, now named metabolic dysfunction-associated steatotic liver disease (MASLD): the multisociety 2023 nomenclature and the steatosis-plus-cardiometabolic-criteria definition, the insulin-resistance and PNPLA3-driven pathophysiology, the distinctive paediatric zone-1 histology, the NASPGHAN 2017 screening strategy with the sex-specific alanine aminotransferase upper limits of 22 units per litre for girls and 26 for boys from age nine to eleven, family-based lifestyle therapy as the cornerstone, the limited role of vitamin E shown in the TONIC trial, and the cardiovascular morbidity that dominates long-term outcome.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
An overweight ten-year-old found on routine screening to have a mildly raised alanine aminotransferase is the everyday face of paediatric fatty liver disease, now the commonest chronic liver condition of childhood in the developed world. The condition is defined by excess triglyceride accumulation within hepatocytes, termed hepatic steatosis, in the setting of overweight or obesity and insulin resistance, and it exists on a spectrum from simple steatosis through steatohepatitis to fibrosis and, rarely, cirrhosis. [1]
A 2023 multisociety Delphi consensus renamed the disorder to reflect this metabolic basis. Non-alcoholic fatty liver disease became metabolic dysfunction-associated steatotic liver disease, and non-alcoholic steatohepatitis became metabolic dysfunction-associated steatohepatitis. The diagnosis now requires hepatic steatosis together with at least one of overweight or obesity, prediabetes or type 2 diabetes, hypertension, hypertriglyceridaemia, or low high-density lipoprotein cholesterol, in the absence of significant alcohol consumption. The new name is more than cosmetic, because it ties the liver disease to the cardiometabolic risk it travels with and aligns paediatric and adult practice. [4]
What makes the paediatric disease distinct is its behaviour over a lifetime. A child diagnosed today carries the condition for decades, and although cirrhosis in childhood is uncommon, the cardiovascular and metabolic consequences are what shape long-term outcome. This is why management is built not around a liver tablet but around sustained family-based change in nutrition, activity, and weight, and why the hepatology assessment is inseparable from a full cardiovascular and metabolic risk evaluation. [1]
Classification
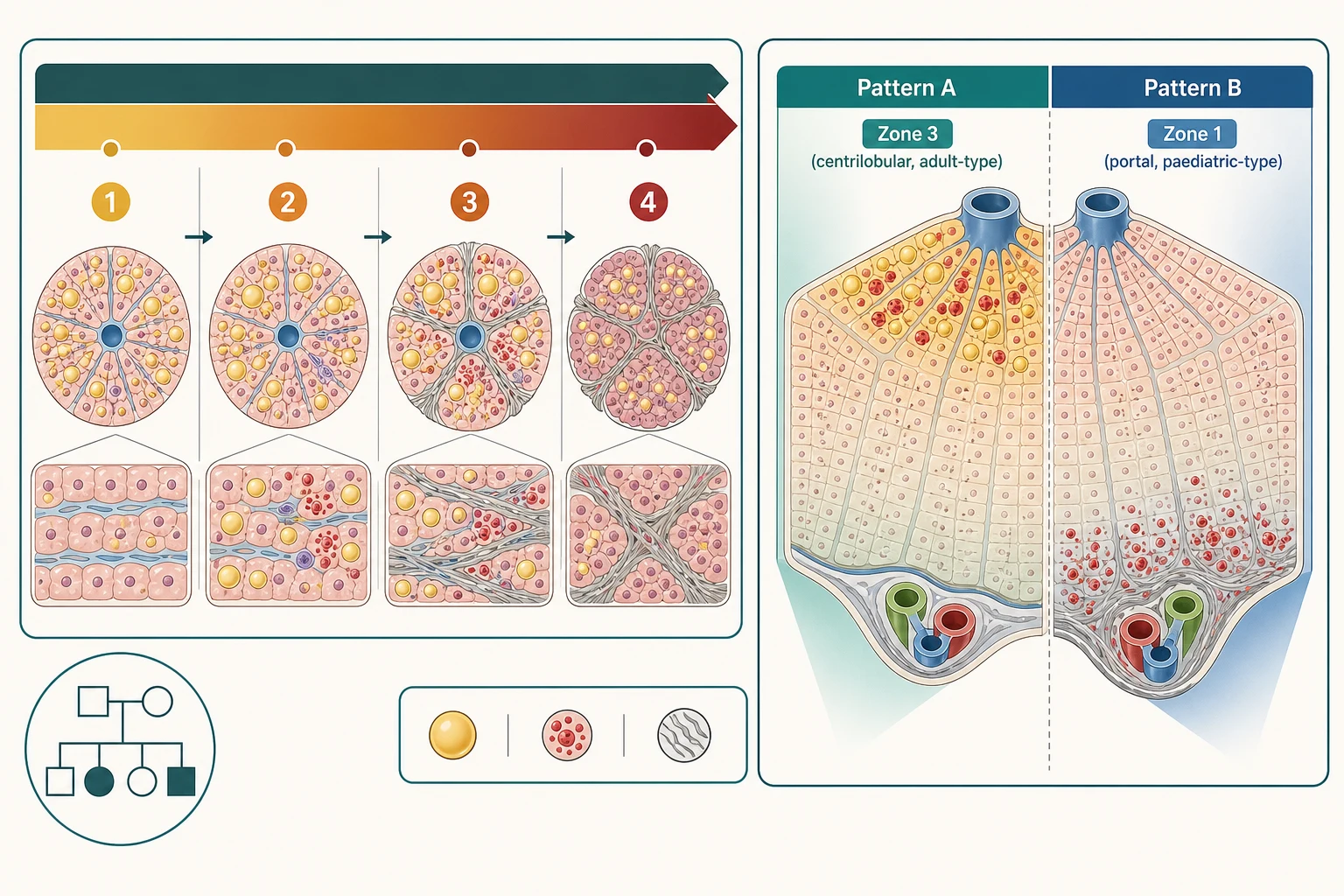
Classification follows two axes: the histological spectrum of liver injury, and the metabolic context. On the histological axis, the disease progresses from simple steatosis, where triglyceride accumulates in hepatocytes without inflammation or fibrosis, through steatohepatitis, where ballooning of hepatocytes and lobular inflammation appear, to fibrosis, and ultimately, in a minority, to cirrhosis. Where the histological criteria for steatohepatitis are met, the term metabolic dysfunction-associated steatohepatitis applies, and this subtype carries the greater risk of progression. [1]
On the metabolic axis, the 2023 nomenclature classifies disease by the cardiometabolic criteria that define it. A child with steatosis who meets at least one of overweight or obesity, prediabetes or type 2 diabetes, hypertension, hypertriglyceridaemia, or low high-density lipoprotein cholesterol has metabolic dysfunction-associated steatotic liver disease, while a child with steatosis driven by another cause does not. This criterion-based approach replaced the older definition, which hinged on excluding alcohol and competing diagnoses, and it reframes the condition as a metabolic disease with a hepatic footprint. [4]
The histological pattern in children differs from adults and is worth knowing for the exam. Adult disease typically injures zone three, the centrilobular region nearest the hepatic venule, with steatosis, ballooning, and perisinusoidal chicken-wire fibrosis. Children more often show a zone-one or portal-based pattern, termed type two paediatric steatohepatitis, with periportal inflammation and portal fibrosis and relatively little ballooning, whereas the adult-like zone-three pattern, termed type one, is the minority in children. Recognising this paediatric pattern matters because fibrosis in children can be portal rather than perisinusoidal and may be under-graded by frameworks built for adults. [11]
[1]Epidemiology & Risk Factors
Paediatric fatty liver disease is common, and its prevalence tracks the childhood obesity epidemic. The landmark autopsy study of American children and adolescents found fatty liver in around nine point six per cent of all comers, rising to around thirteen per cent in adolescents, and to over a third of those who were obese, with the condition rare before age ten and peaking in early adolescence. These figures have only grown as obesity has become more prevalent, and in contemporary clinics a substantial minority of children with obesity have imaging or histological evidence of steatosis. [2]
The risk factors are those of the metabolic syndrome. Overweight and obesity are central, and the risk rises steeply with body mass index percentile and with central adiposity. Male sex, puberty, and certain ethnicities carry higher risk, with the highest prevalence reported in Hispanic populations, followed by Asian and Pacific Islander, then European, then African ancestry in the American data. A family history of fatty liver disease, type 2 diabetes, or the metabolic syndrome, and the presence of insulin resistance, prediabetes, dyslipidaemia, hypertension, polycystic ovary syndrome, and obstructive sleep apnoea all increase the likelihood that an overweight child has the condition. [1]
Genetic susceptibility contributes and explains some of the familial and ethnic clustering. The patatin-like phospholipase domain-containing protein 3 gene variant, known as PNPLA3 and identified by the rs738409 single nucleotide polymorphism, is the strongest common genetic determinant of steatosis severity and fibrosis in children, and a paediatric four-polymorphism risk score that includes PNPLA3, transmembrane 6 superfamily member 2, and other variants predicts which children with steatosis progress to steatohepatitis. These variants do not cause disease alone but tilt a susceptible child toward more severe injury when obesity and insulin resistance are present. [9]
Pathophysiology
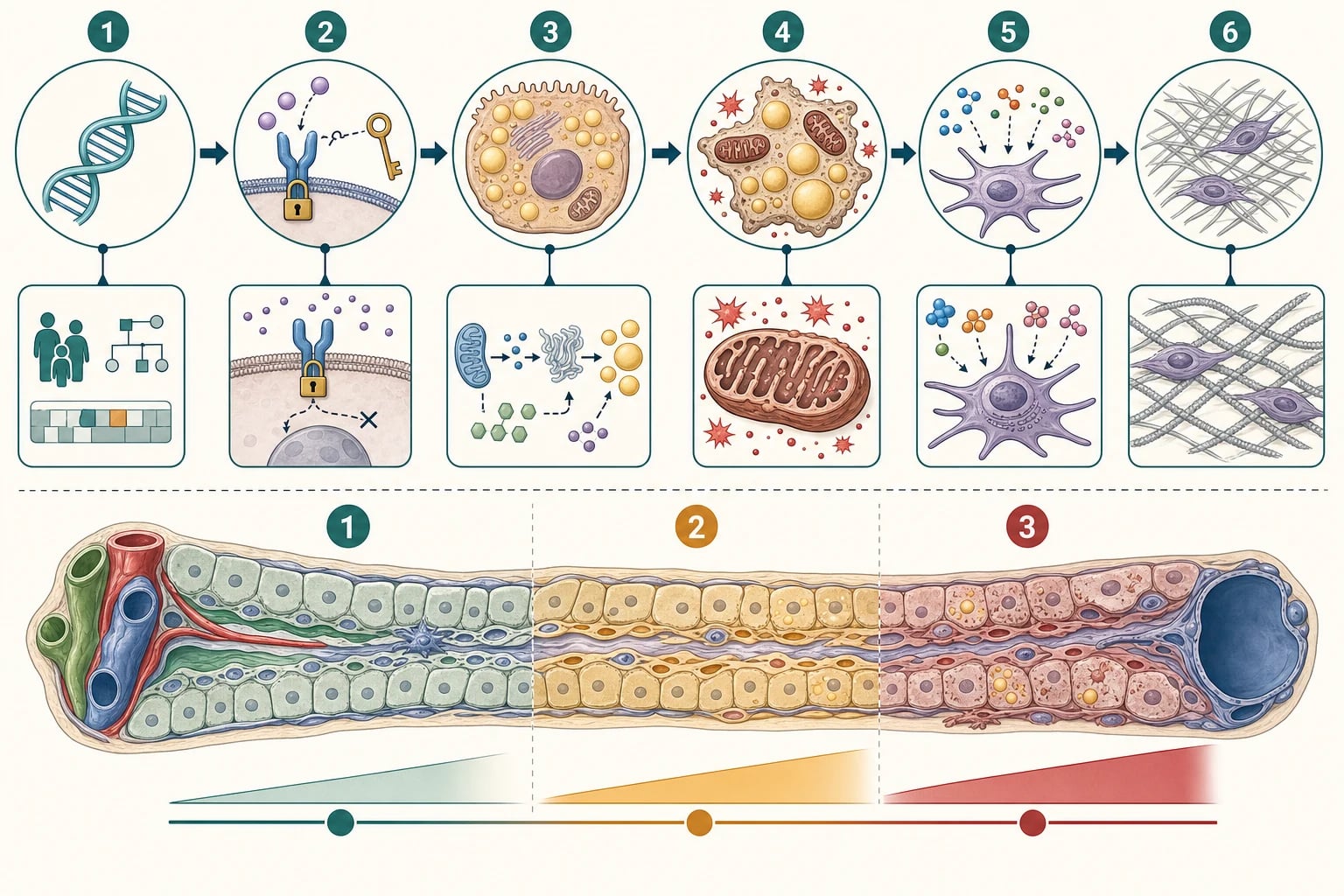
The disease arises from a sequence of events that begins with insulin resistance and culminates, in some children, in fibrosis. Insulin-resistant adipose tissue releases free fatty acids and fails to suppress their release appropriately, while insulin-resistant liver upregulates de novo lipogenesis, the conversion of dietary carbohydrate, especially fructose, into fat. The hepatocyte is flooded with fatty acids and synthesises more, and the surplus is esterified into triglyceride that accumulates as the visible steatosis. Fat accumulation is therefore the hepatic echo of a systemic metabolic disturbance. [1]
Steatosis alone is relatively benign, and progression to steatohepatitis requires additional injury, conceptualised as the multiple-hit model. Lipotoxicity, oxidative stress from overwhelmed mitochondria, endoplasmic reticulum stress, and dysbiosis of the gut microbiome generate reactive oxygen species and damage hepatocytes, which balloon and die. The dying cells release signals that recruit Kupffer cells and other inflammatory cells, which in turn release cytokines such as tumour necrosis factor alpha and interleukin 6, sustaining inflammation and activating hepatic stellate cells. [7]
Activated stellate cells are the fibrosis engine. They transdifferentiate into myofibroblast-like cells that lay down collagen, and if the insult persists the collagen accumulates as fibrosis that, over years, can bridge and distort the architecture into cirrhosis. The pace is highly variable and modulated by genetics, with the PNPLA3 and TM6SF2 variants accelerating the cycle, and by environment, with dietary fructose and a sedentary lifestyle fuelling de novo lipogenesis. Understanding this cascade is what underpins the treatment logic: reduce the substrate, reverse insulin resistance, and the downstream inflammation and fibrosis can subside. [9]
Clinical Presentation
Most children with fatty liver disease are asymptomatic, and the condition is discovered through screening rather than symptoms. The typical presentation is an overweight or obese child in whom an alanine aminotransferase checked at a routine visit is mildly elevated, often incidentally during evaluation for something else. A minority describe vague right upper quadrant discomfort or fatigue, and hepatomegaly may be found on examination, but the liver itself is usually silent, which is exactly why structured screening rather than waiting for symptoms is the gateway to diagnosis. [1]
The examination should be read as a metabolic examination as much as a hepatic one. Plot height and weight and body mass index, assess for central adiposity, look for acanthosis nigricans as a cutaneous marker of insulin resistance, and measure blood pressure, because the liver finding is one manifestation of a cluster that also includes insulin resistance, dyslipidaemia, and hypertension. Signs of advanced liver disease such as jaundice, spider naevi, palmar erythema, splenomegaly, ascites, or easy bruising are uncommon at presentation but, when present, signal longstanding disease and portal hypertension and demand urgent referral. [6]
Because the condition is metabolic and often familial, the history must capture the wider picture. Ask about sugar-sweetened beverage intake, fast food, portion sizes, screen time and physical activity, sleep duration and snoring, and a family history of type 2 diabetes, the metabolic syndrome, cardiovascular disease, and known fatty liver disease or cirrhosis. These elements shape both the probability of disease and the management plan, since the whole family's environment, not the child's willpower, is usually what needs to change. [1]
Features that should prompt screening for fatty liver disease
Obesity, body mass index at or above the ninety-fifth percentile, from age nine to eleven
Overweight, eighty-fifth to ninety-fourth percentile, with a cardiometabolic risk factor
Persistently raised alanine aminotransferase above the sex-specific threshold
Acanthosis nigricans, central adiposity, or elevated blood pressure
Family history of type 2 diabetes, metabolic syndrome, or fatty liver disease
Hepatomegaly or, rarely, signs of chronic liver disease
Differential Diagnosis
The first task when an overweight child has a raised alanine aminotransferase is to confirm the finding is persistent and then to exclude other causes of chronic hepatitis, because steatosis on imaging plus obesity does not by itself secure the diagnosis of fatty liver disease. Repeat the alanine aminotransferase to confirm persistence beyond three months, and if it remains above twice the sex-specific upper limit of normal, evaluate for other causes while keeping fatty liver disease at the top of the differential. [1]
The exclusion workup covers the common and the must-not-miss. Infective causes include hepatitis B and C and, in the right context, Epstein-Barr virus, while autoimmune hepatitis is screened with autoantibodies and immunoglobulins. Wilson disease is excluded with caeruloplasmin and a slit-lamp examination for Kayser-Fleischer rings, and alpha-1-antitrypsin deficiency and cystic fibrosis are considered in younger children or those with atypical features. Drug-induced liver injury, including from herbal and weight-loss preparations, and alcohol-related liver disease must be asked about directly, the last now explicitly reconsidered in the new nomenclature through the alcohol criterion. [6]
Several conditions mimic fatty liver disease by producing steatosis itself. These include mitochondrial and glycogen storage disorders, lysosomal storage diseases, lipodystrophy, total parenteral nutrition, and the steatosis of severe malnutrition or rapid weight loss. The metabolic dysfunction-associated steatotic liver disease label applies only when steatosis coexists with the metabolic criteria and these alternative drivers are excluded, which is why a careful history and a targeted exclusion panel are part of every evaluation. [4]
Clinical & Bedside Assessment
A structured assessment combines the anthropometric, the metabolic, and the hepatic. Plot height, weight, and body mass index on age- and sex-appropriate charts and calculate the body mass index percentile, because overweight and obesity are the entry criteria for screening and the principal targets of treatment. Measure waist circumference as a marker of central adiposity, take a seated blood pressure, and assess pubertal stage, since puberty is when prevalence peaks and insulin resistance worsens. [1]
The abdominal examination looks for hepatomegaly, which is the commonest abdominal sign, and for the stigmata of chronic liver disease and portal hypertension, including splenomegaly, ascites, and caput medusae. Examine the skin for acanthosis nigricans, which confirms insulin resistance at the bedside, and for signs of the associated metabolic and endocrine conditions such as polycystic ovary syndrome. A complete examination matters because fatty liver disease is a multisystem metabolic disorder and the findings reshape both the differential and the management. [6]
The history completes the metabolic picture and sets up the lifestyle plan. Quantify sugar-sweetened beverage intake, meals eaten away from home, portion sizes, snacking, daily screen time, structured exercise, sleep duration, and snoring or witnessed apnoea. Explore the family's understanding of the diagnosis, their readiness to change, food security, and the practical barriers they face, because a plan built without this context will fail at implementation. [1]
Investigations
Screening rests on the alanine aminotransferase, and the threshold is deliberately lower than the values most laboratories report as normal. The 2017 North American guideline defines the upper limit of normal as 22 units per litre for girls and 26 units per litre for boys, reflecting the healthy ninety-fifth percentile of a metabolically normal reference population, and recommends screening with alanine aminotransferase between ages nine and eleven years for all children with obesity and for children with overweight who have additional risk factors. Persistence above twice this threshold for more than three months, or a value above 80 units per litre at any time, is the trigger to evaluate for fatty liver disease and to exclude alternative causes. [1]
Confirmation of steatosis and staging of fibrosis increasingly rely on non-invasive tools rather than biopsy. Liver ultrasound is widely available and will show a bright hyperechoic liver, but it is operator-dependent and insensitive for lesser degrees of fat, so magnetic resonance imaging-derived proton density fat fraction is the preferred quantitative measure where available. Transient elastography, including the controlled attenuation parameter for fat, stages fibrosis non-invasively, and liver biopsy, the reference standard for steatohepatitis and fibrosis, is reserved for cases where the diagnosis is uncertain, other causes cannot be excluded, or staging will change management. [6]
The blood and metabolic workup serves two purposes: to exclude alternative diagnoses and to define the cardiometabolic milieu. A full liver panel, full blood count, coagulation, glucose and glycated haemoglobin, lipid profile, and exclusion tests for hepatitis, autoimmune, Wilson, and alpha-1-antitrypsin disease are routine, alongside assessment of insulin resistance. Thyroid function, vitamin D, and, where indicated, polysomnography complete the picture, because the metabolic comorbidities are as important to detect and treat as the liver disease itself. [1]
Management — Resuscitation
Paediatric fatty liver disease rarely presents as an acute emergency, but decompensated cirrhosis and its complications are the exceptions that demand resuscitation. A child with fatty liver disease who presents with jaundice, coagulopathy, encephalopathy, ascites, or variceal bleeding has decompensated chronic liver disease and must be assessed immediately for airway, breathing, and circulation, with early involvement of a paediatric hepatologist and intensivist. [6]
The specific emergencies are portal hypertensive bleeding and the decompensation of an unrecognised cirrhosis. Suspected variceal bleeding is managed with airway protection, fluid resuscitation and blood transfusion, an octreotide infusion, and urgent endoscopy for band ligation, while ascites and spontaneous bacterial peritonitis are managed with antibiotics and albumin. These scenarios are uncommon in paediatric fatty liver disease but, when they occur, they signal that the disease has been silent for years and that the child now needs tertiary hepatology and possible transplant assessment. [6]
The more common resuscitation need is the symptomatic child with very high alanine aminotransferase or newly recognised advanced fibrosis who requires prompt, organised referral rather than emergency intervention. Confirm the persistence and degree of the abnormality, exclude alternative and treatable causes, assess for portal hypertension with elastography and blood count, and refer to paediatric gastroenterology or hepatology, while beginning the lifestyle conversation that will be the long-term foundation of care. [1]
Management — Definitive & Stepwise
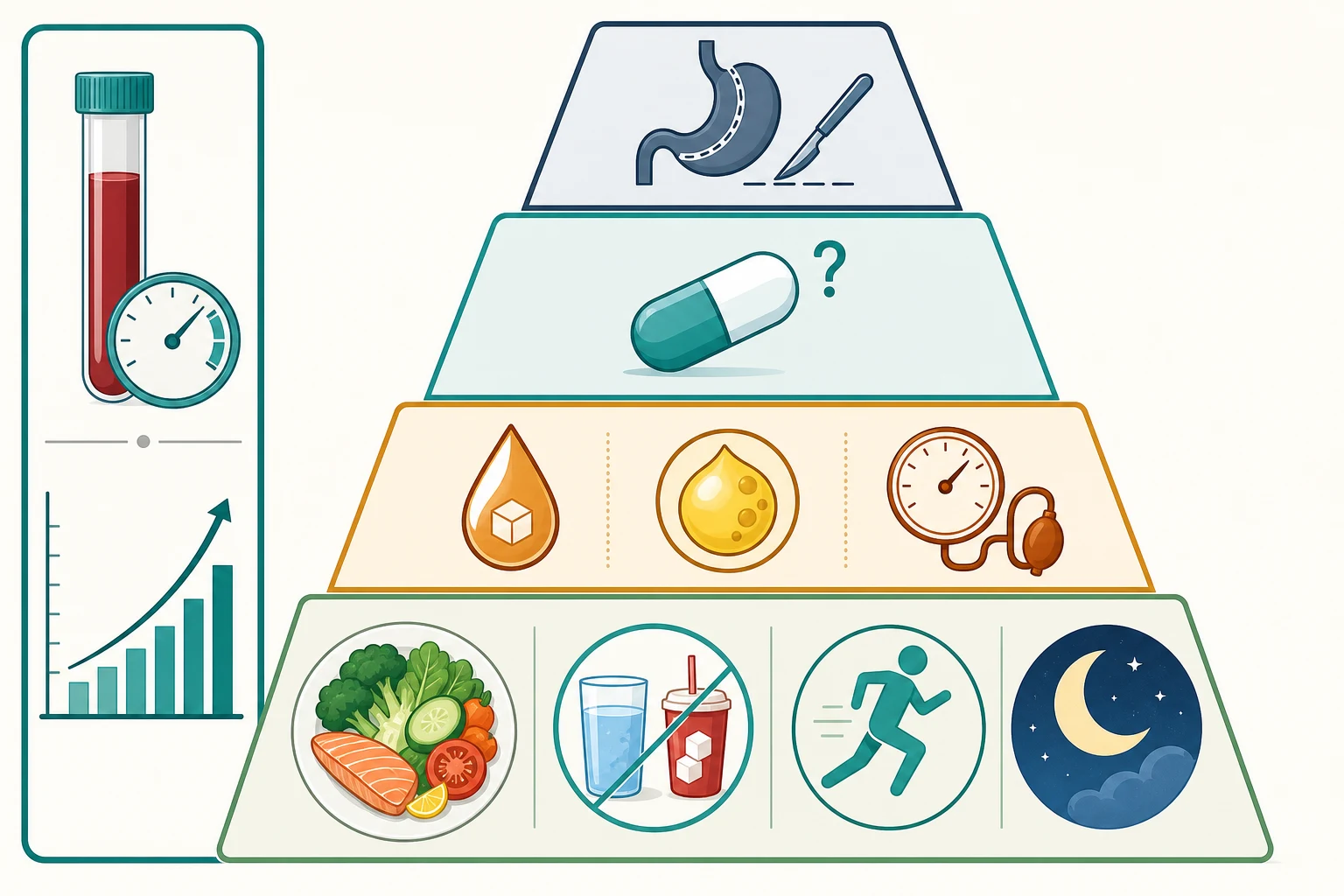
The cornerstone of treatment is sustained, family-based lifestyle change, and no medication replaces it. A weight reduction of around 7 to 10 per cent is associated with histological improvement of steatohepatitis, and the practical prescription is a calorie-appropriate diet with sharp reduction of sugar-sweetened beverages and fructose, an increase in fruits, vegetables, and fibre, portion control, at least one hour of moderate to vigorous physical activity daily, and reduction of sedentary screen time. Crucially, these changes must engage the whole household, because a child cannot eat differently from the family around them. [1]
Pharmacotherapy has a limited and disappointing role. The randomised TONIC trial showed that 800 IU per day of vitamin E for 96 weeks improved the histological features of steatohepatitis compared with placebo in biopsy-proven paediatric non-alcoholic steatohepatitis, but did not improve fibrosis, while metformin at up to 1000 mg per day was no better than placebo for histology. On this basis vitamin E may be considered in selected children with biopsy-proven steatohepatitis, with informed discussion of its risks and benefits, while metformin is not recommended for the liver disease itself, and no drug is currently approved specifically for paediatric fatty liver disease. [3]
Vitamin E (considered for biopsy-proven paediatric steatohepatitis)
Dose
800 IU orally once daily, as studied over 96 weeks in the TONIC trial
Comorbidity control is inseparable from liver management. Insulin resistance and prediabetes or type 2 diabetes are treated on their own merits, dyslipidaemia is managed with dietary change and, in selected older adolescents, lipid-lowering therapy under guidance, and hypertension is treated to target. For adolescents with severe obesity who have not responded to intensive lifestyle and medical management, metabolic and bariatric surgery in a specialised centre is an effective option that can reverse steatohepatitis, and it is increasingly part of the treatment ladder for carefully selected patients. [8]
The multidisciplinary team is the vehicle for delivery. A dietitian, exercise professional, psychologist, and nurse educator, working with the primary paediatrician and the hepatology service, give the family the sustained support that lifestyle change requires, and structured follow-up monitors weight trajectory, alanine aminotransferase trend, comorbidity control, and adherence. The model is chronic-disease management, not a single intervention, and realistic, family-centred goals outperform rigid targets that families cannot meet. [1]
Specific Subtypes & Scenarios
The adolescent with severe obesity represents the highest-risk subtype and the one most likely to be considered for escalation. In this group the disease is more often steatohepatitis with fibrosis, the comorbidity burden of type 2 diabetes and dyslipidaemia is greater, and the window for lifestyle change before adult disease is narrowing. For the carefully selected adolescent with severe obesity and persistent disease despite intensive lifestyle and medical therapy, bariatric surgery in a specialised multidisciplinary centre can achieve substantial weight loss with reversal of steatohepatitis, and it should be discussed without stigma as part of the ladder rather than as a last resort. [8]
The child with type 1 diabetes presents a diagnostic nuance. Steatosis can occur in type 1 diabetes through insulin resistance in the setting of overweight, but the metabolic context and the absence of the typical type 2 milieu mean that the cardiometabolic-criteria definition must be applied carefully, and other causes of elevated liver enzymes excluded. These children are managed jointly with the diabetes team, with attention to glycaemic control and weight, rather than automatically labelled with metabolic dysfunction-associated steatotic liver disease. [1]
The child with established fibrosis or compensated cirrhosis needs hepatology-led surveillance. Elastography and non-invasive scores track fibrosis, a full blood count watches for the thrombocytopaenia of portal hypertension, and variceal and hepatocellular carcinoma surveillance begin according to cirrhosis protocols. Although progression to cirrhosis in childhood is uncommon, it is well described, and the goal of early identification is to prevent this trajectory through effective lifestyle and comorbidity intervention. [6]
[8]Complications & Pitfalls
The complications span the liver and the wider metabolic system, and for most children the systemic complications matter more than the hepatic ones. Within the liver, a minority progress from steatohepatitis to fibrosis and, rarely, to cirrhosis and its sequelae of portal hypertension, liver failure, and hepatocellular carcinoma, the last an uncommon but recognised outcome even in youth. The cardiovascular system carries the greatest long-term burden, with childhood fatty liver disease associated with subclinical atherosclerosis, increased carotid intima-media thickness, and a higher lifetime risk of cardiovascular events, and reversal of the liver disease appears to improve these early vascular changes. [10]
Metabolic complications run alongside. Insulin resistance progresses to prediabetes and type 2 diabetes, dyslipidaemia and hypertension compound cardiovascular risk, and the cluster of which the liver disease is one element raises the lifetime probability of a major cardiovascular event. Recognising fatty liver disease as a marker of elevated cardiometabolic risk, rather than as an isolated liver problem, is the conceptual shift that determines whether the child receives the cardiovascular and metabolic prevention they need. [1]
The classic pitfalls are diagnostic delay, false reassurance, and over-reliance on medication. Because the disease is silent, an elevated alanine aminotransferase in an overweight child is often dismissed as trivial or attributed to recent illness, and the opportunity for early lifestyle intervention is lost. Conversely, once recognised, families and clinicians may expect a tablet to fix it, and the harder but effective work of family-based lifestyle change is under-delivered. A proactive, non-judgemental, family-centred plan that treats the condition as serious, common, and lifestyle-responsive avoids both errors. [1]
Prognosis & Disposition
For most children the prognosis is favourable in hepatic terms but demands lifelong attention to cardiometabolic risk. Steatosis and steatohepatitis can regress with sustained weight loss of around 7 to 10 per cent, alanine aminotransferase trends downward, and the early vascular changes of atherosclerosis appear to improve when the liver disease is reversed, which means the diagnosis is an opportunity as well as a warning. The minority who progress to advanced fibrosis or cirrhosis require hepatology-led care and surveillance, and timely lifestyle intervention early in the course is the single most important determinant of a good hepatic outcome. [10]
Disposition depends on severity and resources. Children with simple steatosis and mild enzyme elevation can be co-managed by primary care and general paediatrics with lifestyle support and periodic alanine aminotransferase monitoring, while those with persistent elevation above twice the upper limit of normal, suspected advanced fibrosis, or decompensation are referred to paediatric gastroenterology or hepatology. A multidisciplinary weight-management programme, with dietitian, exercise, and psychology input, underpins care at every tier, and the primary paediatrician usually coordinates the cardiovascular and metabolic comorbidity screening. [1]
The condition is chronic, so continuity and transition matter. The child diagnosed at ten will need the same family-based habits at twenty and thirty, and a planned handover to adult metabolic and primary care in late adolescence preserves the gains made in childhood. Poor transition is a recognised cause of relapse and disengagement in young adulthood, and building the young person's own knowledge, motivation, and self-management through adolescence is as important as any individual intervention. [8]
Special Populations
Adolescents carry the highest burden and the most complex needs. Puberty intensifies insulin resistance, identity and body image shape adherence and motivation, and the competing demands of school, work, and independence challenge the consistency that lifestyle change requires. A confidential, non-judgemental, adolescent-friendly approach that builds the young person's own agency, addresses mental health, and plans transition to adult care is essential, and for selected adolescents with severe obesity, bariatric surgery is a legitimate and effective option to discuss without stigma. [8]
Children from socioeconomically disadvantaged families, and those in rural and remote areas, face disproportionate barriers. Food insecurity, the lower cost and higher availability of energy-dense processed food, limited safe spaces for physical activity, and reduced access to specialist and multidisciplinary services all increase prevalence and worsen outcomes, and the families least able to afford the recommended diet are those most affected. Practical support, culturally safe shared-care pathways, telehealth-supported monitoring, and subsidy of programme access help close the gap, and a named coordinator can prevent the fragmentation that disadvantages vulnerable families. [1]
Indigenous, migrant, and refugee children are over-represented among those affected and among those with barriers to care, reflecting both a higher underlying cardiometabolic risk and structural obstacles to diagnosis and treatment. Culturally safe, community-based programmes that work with families in their language and context, and that address the social determinants of diet and activity alongside the medical management, are more effective than generic advice, and they are the route to equity in a condition whose burden falls hardest on those with the fewest resources. [8]
[4]Evidence, Guidelines & Regional Differences
The evidence base has evolved through three phases. The 2006 autopsy study defined the prevalence and demography of childhood fatty liver disease and remains the epidemiological foundation, while the histological studies of the following decade established the distinctive paediatric zone-one pattern and the role of fibrosis staging. The randomised TONIC trial in 2011 defined the pharmacological evidence, showing a histological benefit for vitamin E but not metformin, and set the expectation that lifestyle, not a drug, would remain first-line. [3]
The guideline landscape now spans several societies. The 2017 North American clinical practice guideline codified screening with the sex-specific alanine aminotransferase thresholds of 22 units per litre for girls and 26 for boys from age nine to eleven, and endorsed family-based lifestyle therapy as the cornerstone, while the British guidelines on abnormal liver blood tests framed the investigation pathway and the threshold to refer. The Asian Pacific and Indian paediatric society recommendations have adapted the metabolic-criteria approach to local epidemiology and resources, emphasising opportunistic screening and lifestyle intervention. [7]
[5]The defining recent change is the 2023 multisociety nomenclature and its rapid adoption. The Delphi consensus replaced the alcohol-exclusion definition with positive metabolic criteria and the names metabolic dysfunction-associated steatotic liver disease and steatohepatitis, and the subsequent American, Asian Pacific, and paediatric society guidance incorporated the change, with the caveat that paediatric-specific thresholds for the metabolic criteria and the alcohol definition remain areas of active refinement. Regional differences persist chiefly in access to elastography, specialist services, and adolescent bariatric surgery, but the metabolic, lifestyle-first management principle is now globally consistent. [4]
Exam Pearls
SCREEN for paediatric fatty liver disease
References
- [1]Vos MB, Abrams SH, Barlow SE, Caprio S, Daniels SR, Kohli R, et al NASPGHAN Clinical Practice Guideline for the Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children: Recommendations from the Expert Committee on NAFLD (ECON) and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN). J Pediatr Gastroenterol Nutr, 2017.PMID 28107283
- [2]Schwimmer JB, Deutsch R, Kahen T, Lavine JE, Stanley C, Behling C Prevalence of fatty liver in children and adolescents. Pediatrics, 2006.PMID 17015527
- [3]Lavine JE, Schwimmer JB, Van Natta ML, Molleston JP, Murray KF, Rosenthal P, et al Effect of vitamin E or metformin for treatment of nonalcoholic fatty liver disease in children and adolescents: the TONIC randomized controlled trial. JAMA, 2011.PMID 21521847
- [4]Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, et al A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol, 2023.PMID 37364790
- [5]Kanwal F, Neuschwander-Tetri BA, Loomba R, Rinella ME Metabolic dysfunction-associated steatotic liver disease: Update and impact of new nomenclature on the American Association for the Study of Liver Diseases practice guidance on nonalcoholic fatty liver disease. Hepatology, 2024.PMID 38445559
- [6]Newsome PN, Cramb R, Davison SM, Dillon JF, Foulerton M, Godfrey EM, et al Guidelines on the management of abnormal liver blood tests. Gut, 2018.PMID 29122851
- [7]Eslam M, Fan JG, Yu ML, Wong VW, Cua IH, Liu CJ, et al The Asian Pacific association for the study of the liver clinical practice guidelines for the diagnosis and management of metabolic dysfunction-associated fatty liver disease. Hepatol Int, 2025.PMID 40016576
- [8]Sood V, Alam S, Nagral A, Srivastava A, Deshmukh A, Bavdekar A, et al Practice Recommendations for Metabolic Dysfunction-Associated Steatotic Liver Disease by the Indian Society of Pediatric Gastroenterology, Hepatology and Nutrition (ISPGHAN). Indian Pediatr, 2024.PMID 39297398
- [9]Nobili V, Donati B, Panera N, Vongsakulyanon A, Alisi A, Dallapiccola B, et al A 4-polymorphism risk score predicts steatohepatitis in children with nonalcoholic fatty liver disease. J Pediatr Gastroenterol Nutr, 2014.PMID 24345846
- [10]Li M, Shu W, Zou Y, Xiao H, Asihaer Y, Guan M, et al Reversing Metabolic Dysfunction-Associated Steatotic Liver Disease Promotes Healthy Pediatric Cardiovascular Structures: The PROC Study. Am J Gastroenterol, 2024.PMID 38775939
- [11]Carter-Kent C, Brunt EM, Yerian LM, Alkhouri N, Angulo P, Kohli R, et al Relations of steatosis type, grade, and zonality to histological features in pediatric nonalcoholic fatty liver disease. J Pediatr Gastroenterol Nutr, 2011.PMID 21240012