Paeds · gastroenterology-hepatology-and-nutrition
Nutritional management of chronic disease
Also known as Nutritional management of chronic disease · Nutrition in chronic childhood illness · Chronic disease malnutrition · Disease-related malnutrition in children · Cystic fibrosis nutrition · Chronic kidney disease nutrition · Inflammatory bowel disease nutrition · Congenital heart disease nutrition · Paediatric oncology nutrition · Nutrition support in chronic disease
Fellowship guide to the nutritional management of chronic disease in children: the cystic fibrosis child who needs high calorie, high fat intake with pancreatic enzymes and fat-soluble vitamins, the chronic kidney disease child on a controlled phosphate and potassium diet with careful protein and growth hormone support, the Crohn disease child induced into remission with exclusive enteral nutrition, the cardiac infant with a large shunt who needs one hundred and fifty kilocalories per kilogram to grow, and the oncology child whose chemotherapy strips appetite and muscle, all unified by the four mechanisms of increased demand, decreased intake, nutrient loss and dietary restriction and the assess, screen, support and monitor pathway.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Disease-related malnutrition is the wasting and faltering growth that follows when a chronic illness raises what the body needs, lowers what the child can take in, steals nutrients through loss, or forces a diet so restricted that growth itself is curtailed. The cystic fibrosis child burning energy on the work of breathing and malabsorbing fat, the cardiac infant with a large shunt whose feeding calories barely cover the heart's oxygen bill, the Crohn disease teenager with abdominal pain and anorexia, the dialysis child leaking amino acids and held to a phosphate limit, and the oncology child nauseated and mucositic after chemotherapy are the same child seen through different lenses. The clinician's task is to recognise the faltering centiles and the thinning arm, confirm the degree of malnutrition with formal anthropometry, and build a nutrition support plan that protects growth as an outcome equal to disease control. [1]
The unifying idea is that chronic disease and nutrition move together, and that letting the child dwindle while the disease is treated is a failure of care. Growth is a vital sign in paediatrics, and a falling centile in any chronic illness is a signal that the balance of demand, intake, loss and restriction has tipped against the child. The framework the clinician holds in mind is the four mechanisms by which chronic disease drives malnutrition, the standardised anthropometry that quantifies it, the stepped nutrition support ladder that treats it, and the disease-specific requirements that fine-tune it, all delivered by a multidisciplinary team with the dietitian at its centre. [1] [12]
Classification
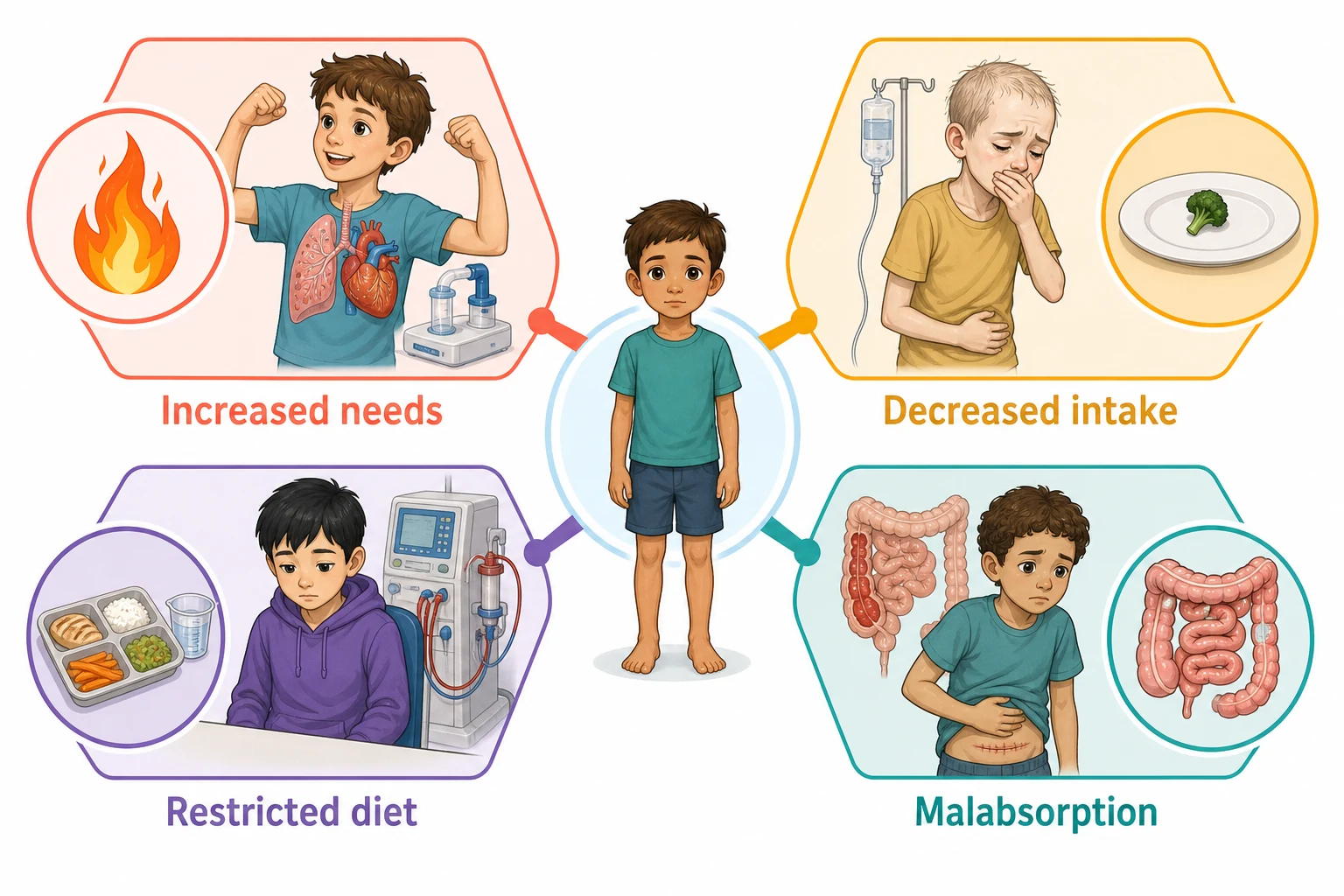
The most useful clinical frame is the mechanism by which the disease drives depletion, because the mechanism points to the nutrition intervention. Increased demand dominates in the catabolic and high-work diseases: cystic fibrosis burns energy on the work of breathing and on chronic infection, the large left-to-right cardiac shunt burns energy on volume overload, active Crohn disease and cancer drive inflammation-driven catabolism, and the oncology child on steroids and chemotherapy turns over protein and fat. The response is to raise the energy and protein delivered, often to one hundred and twenty to one hundred and fifty per cent of the standard for age, and to feed by the most reliable route. [2] [9]
Decreased intake dominates in the diseases that suppress appetite or make eating painful: the anorexia and early satiety of active inflammatory bowel disease, the nausea and taste change of chemotherapy, the fatigue and breathlessness of cardiac failure, and the anorexia of uraemia in advanced kidney disease. Nutrient loss dominates where the gut fails to absorb or the kidney fails to retain: the fat and fat-soluble vitamin malabsorption of pancreatic-insufficient cystic fibrosis, the protein and mineral losses of Crohn disease and short bowel, the proteinuria and dialysis amino-acid losses of chronic kidney disease. Dietary restriction dominates where the disease itself or its treatment demands it: the phosphate, potassium and fluid limits of chronic kidney disease, the sodium and fluid limits of heart failure, and the disease-specific exclusion of the Crohn disease diet. [3] [5]
A second axis is severity, graded by the standardised anthropometry that the Academy of Nutrition and Dietetics and ASPEN consensus brought to paediatrics. Malnutrition is diagnosed when two or more of six indicators are abnormal, each graded mild, moderate or severe: the weight-for-length or height z-score, the body mass index for age z-score, the length or height for age z-score that marks stunting, the mid-upper arm circumference z-score, the rate of weight gain, and the rate of length gain. This shifts the assessment from an impression of thinness to a documented z-score trajectory, which is what the multidisciplinary team and the examiner expect. [1]
[2] [6]Epidemiology & Risk Factors
Disease-related malnutrition is common wherever chronic illness is managed, and the prevalence tracks the disease and its activity. In cystic fibrosis, the historical picture of severe wasting has improved with pancreatic enzymes, fat-soluble vitamin supplementation and energetic nutrition targets, but faltering growth and poor lung function still cluster in the malnourished, and the modern modulator era is reshaping nutritional needs. In chronic kidney disease, growth failure and protein-energy wasting accumulate with declining glomerular filtration rate and intensify on dialysis, where amino-acid and peptide losses and the anorexia of uraemia combine. [3] [5]
In inflammatory bowel disease, growth failure is a defining feature of paediatric Crohn disease and may precede the intestinal symptoms, which is why anthropometry is part of the diagnosis and the follow-up. In congenital heart disease, infants with large left-to-right shunts, univentricular physiology and pulmonary hypertension are the highest risk, their feeding calories consumed by the work of the over-circulated heart. In paediatric cancer, malnutrition and sarcopenia are common at diagnosis and through treatment, worsen with intensive chemotherapy and transplant, and carry prognostic weight for tolerance, infection and survival. [9] [11]
The shared risk factors are the company malnutrition keeps. Severe or active disease, polypharmacy including steroids and diuretics, repeated admissions, surgery, gut resection, dialysis, neutropenic and mucositic treatment cycles, food insecurity, restricted diets imposed without dietetic oversight, and the neurodevelopmental or feeding-disorder overlay all raise the risk and compound one another. The child with several of these at once is the one whose centiles quietly fall, which is why screening is repeated, not done once. [1]
Pathophysiology
Four pathophysiological streams empty the energy and protein reserves of the chronically ill child, and most diseases draw on more than one. Increased metabolic demand comes from the work of breathing, the caloric cost of an over-circulated heart, the catabolic drive of cytokines in active inflammation, the tumour and chemotherapy turnover of oncology, and the dialysis session itself, which is catabolic and inflammatory. The net effect is that the child burns more for the same weight, and the standard energy prescription for age is insufficient to keep the balance. [9] [12]
Decreased intake comes from the anorexia of cytokines and uraemia, the nausea and vomiting of chemotherapy and renal failure, the early satiety of gastroparesis and hepatosplenomegaly, the pain and fear of eating in active bowel disease, the taste distortion of zinc deficiency and chemo, and the fatigue of breathlessness. The child simply cannot or will not eat enough, and the gap between need and intake widens as the disease worsens. Nutrient loss comes from the steatorrhoea and fat-soluble vitamin loss of pancreatic insufficiency, the protein-losing enteropathy and malabsorption of inflamed or resected gut, the proteinuria and dialysis amino-acid and peptide losses of kidney disease, and the fistula, stoma and high-output losses of surgical gut. [3] [5]
Dietary restriction is the fourth stream and the iatrogenic face of good intentions. The kidney diet restricts phosphate, potassium, fluid and sometimes sodium to manage mineral and bone disorder, hyperkalaemia and volume; the cardiac diet restricts sodium and fluid to manage failure; the metabolic diet restricts the offending substrate. Each restriction is rational in isolation, but layered without dietetic balance they strip protein and energy until growth stops, and the child becomes malnourished by the treatment. The counterweight is that restriction is matched to requirement: protein is held near the recommended dietary allowance for age in kidney disease, not eliminated, and energy is protected even as phosphate is controlled. [4]
Clinical Presentation
The cystic fibrosis child presents with a body mass index that drifts down despite a large appetite, bulky greasy stools from fat malabsorption, and recurrent pulmonary exacerbations that raise the metabolic cost of the illness. Pancreatic-insufficient children lose fat and the fat-soluble vitamins A, D, E and K, so the picture may include fat-soluble vitamin deficiency, poor linear growth, and in the infant, failure to thrive with steatorrhoea. The modern modulator era is improving nutrition for many, but the principles of high energy, high fat, pancreatic enzyme replacement and vitamin supplementation remain. [2] [3]
The chronic kidney disease child presents with growth failure, and the reasons stack up: the anorexia of uraemia, the catabolism of dialysis, the protein and amino-acid losses of the dialysate, the energy cost of poorly controlled renal osteodystrophy and acidosis, and the dietary restriction of phosphate, potassium and fluid. The dialysis child is the archetypal case of malnutrition driven by restriction and loss together, and the challenge is to protect protein and energy while controlling the minerals. The cardiac infant presents with failure to thrive on the metabolic demand of the lesion: tachypnoea that makes feeding exhausting, sweating on feeds, a large left-to-right shunt, and weight that stalls despite an adequate volume of milk. [5] [9]
The Crohn disease child presents with growth failure that may precede the abdominal pain and diarrhoea, and this temporal order is the pearl examiners reward. Delayed puberty, weight loss, perioral and perianal disease, and a fallen growth centile at diagnosis are the signature of a disease whose inflammation is catabolic and whose anorexia deepens the deficit. The oncology child presents with weight loss, muscle wasting, anorexia, nausea and mucositis through the treatment cycle, with sarcopenia that predicts poorer tolerance of chemotherapy and transplant. Each disease has its face, but the shared presentation is the child who is not growing as they should. [6] [11]
[3] [6]Differential Diagnosis
The differential of the faltering centile in a chronically ill child splits into three questions: is the disease active, is the nutrition adequate, or is there a new problem compounding both. Active disease is the first fork, because cystic fibrosis exacerbation, active Crohn disease, a decompensating cardiac lesion, progressive kidney failure and relapsed cancer all raise demand and suppress intake, and no nutrition plan corrects growth while the disease burns. The clinician assesses disease activity alongside the nutrition, because the two are inseparable. [6] [9]
Inadequate or imbalanced nutrition is the second fork. The cardiac infant may simply not be getting enough calories, the dialysis child may be over-restricted on phosphate and protein, the cystic fibrosis child may be under-dosed on enzymes, and the oncology child may have untreated nausea. The dietetic history, the calculated intake against the target, and the enzyme and supplement review reveal these. The third fork is the new problem compounding both: an eating disorder in the adolescent with chronic disease, depression, thyroid dysfunction, a new infection, a drug side effect such as steroid myopathy, or a feeding disorder layered on the technology-dependent child. [1] [11]
The differential also distinguishes genuine malnutrition from oedema that masks it. The nephrotic and cardiac child may weigh more than they appear because of fluid, so the dry weight, the mid-upper arm circumference and the trend off fluid loading are what reveal the wasting beneath. Equally, steroid treatment redistributes and increases weight while catabolising muscle, so a stable or rising weight on steroids can hide sarcopenia, and the arm circumference and body composition are more honest than the scale. [5]
The four mechanisms of disease-related malnutrition — 'DILR'
Clinical & Bedside Assessment
Assessment begins with the growth chart and the diet history, because together they expose the trajectory and the gap. Plot the weight, the length or height, and the body mass index on the appropriate chart, ideally condition-specific where one exists, and read the trajectory across the centiles rather than a single point. A focused diet history asks what the child eats, how much, how often, what is excluded and why, whether oral nutritional supplements or enteral feeds are used, the pancreatic enzyme and fat-soluble vitamin doses in cystic fibrosis, the phosphate binder and potassium allowance in kidney disease, and the feeding route and tolerance in the cardiac and technology-dependent child. [1] [3]
The bedside examination then quantifies the body composition and the micronutrient state. Measure the mid-upper arm circumference as a muscle and fat marker less confounded by oedema than the weight, look for the temporal and gluteal wasting of protein-energy malnutrition, and examine for the fat-soluble vitamin deficiency of cystic fibrosis, the oedema of nephrotic and cardiac overload, the short stature of chronic kidney disease, and the mucositis and muscle loss of the oncology child. Developmental and pubertal staging matters, because delayed puberty in Crohn disease and chronic kidney disease is both a sign and a target. [9] [6]
The company the malnutrition keeps directs the workup. Ask about disease activity and the recent admission, surgery or transplant cycle that raised demand; about polypharmacy with steroids, diuretics and chemotherapy; about gut function, stoma output and dialysis losses; about the social determinants of food security, the cost of supplements and feeds, and the carer capacity to deliver a complex nutrition plan. The child whose growth falters on a stable disease plan is pointing to the diet, the access, or the family's ability to deliver it, and the answer often lies as much in the social history as in the blood tests. [1]
Investigations
The nutrition workup rests on serial anthropometry interpreted as a trajectory. The weight, the length or height and the body mass index are plotted on the condition-specific or standard growth chart and converted to z-scores, and the mid-upper arm circumference is tracked as the muscle and fat marker that oedema least confounds. The Academy of Nutrition and Dietetics and ASPEN consensus asks for two or more of six indicators to diagnose malnutrition, each graded mild, moderate or severe, which converts an impression of thinness into a documented, repeatable and comparable measure that the multidisciplinary team can track. [1]
The blood panel screens for the micronutrient and metabolic consequences of the disease and its diet. A full blood count and iron studies catch the iron deficiency of inflammatory bowel disease and chronic kidney disease; the fat-soluble vitamin levels, the international normalised ratio for vitamin K and the 25-hydroxyvitamin D catch the deficiencies of cystic fibrosis; the calcium, phosphate, parathyroid hormone and vitamin D catch the mineral and bone disorder of chronic kidney disease; and the albumin and prealbumin, read with caution as they are negative acute-phase reactants, round out the panel. The electrolytes and acid-base are monitored in the kidney, cardiac and dialysis child whose diets and drugs shift them. [3] [5]
The disease-specific tests quantify the mechanism and the need. The faecal elastase confirms pancreatic insufficiency in cystic fibrosis and guides the enzyme dose; the calprotectin and inflammatory markers gauge the Crohn disease activity that is driving the catabolism; the echocardiogram and the cardiac lesion define the energy demand of the cardiac infant; and the dialysis adequacy and the residual renal function set the protein and fluid prescription for the kidney child. The aim is to match the energy and protein prescription to the measured demand and loss, not to apply a generic formula. [4] [9]
Management — Resuscitation
Most nutritional management is elective and preventive, but a few presentations need urgent action. The child who presents with severe acute malnutrition superimposed on chronic disease is at risk of refeeding syndrome, and the response is cautious, monitored refeeding rather than aggressive catch-up. Refeeding starts at a conservative energy intake, roughly ten kilocalories per kilogram per day in the highest-risk child and escalated over days to the target, with phosphate, potassium and magnesium checked and corrected before and during refeeding, and thiamine given before the first feed. [12]
The cardiac infant with severe failure to thrive and a decompensating lesion may need fluid restriction and diuretic optimisation alongside the nutrition, because feeding a volume-overloaded heart worsens the failure, and the two must be balanced together. The dialysis child with hyperkalaemia or fluid overload needs the electrolyte and fluid emergency managed first, then the diet rebalanced to prevent recurrence. The oncology child with neutropenic enterocolitis or severe mucositis may need nothing by mouth and parenteral nutrition while the gut heals. [9] [11]
Refeeding in the chronically malnourished child
Loading dose
Start at roughly 10 kcal/kg/day in the highest-risk, severely wasted child and escalate over four to seven days toward the full target; give oral or intravenous thiamine before the first feed
Maintenance dose
Correct and monitor serum phosphate, potassium and magnesium daily in the first week, and supplement as needed; escalate energy toward the disease-specific target once biochemistry is stable
Immediate management of the severely malnourished child with chronic disease
Assess the airway, breathing and circulation, the fluid and electrolyte status, and the disease activity driving the depletion
Check phosphate, potassium, magnesium and thiamine before refeeding, and correct any deficit
Start cautious refeeding at a low energy intake in the highest-risk child, escalating over days, with daily electrolyte monitoring
Optimise the disease, because active inflammation, a decompensating heart or inadequate dialysis will defeat any nutrition plan
Escalate along the nutrition support ladder once the child is biochemically stable, choosing the most reliable feeding route
Set a growth target and a review date with the dietitian, because recovery is measured on the growth chart over weeks
Management — Definitive & Stepwise
The definitive strategy is to match the energy and protein prescription to the measured demand and loss, deliver it by the most reliable route, and monitor the growth response. The energy target is disease-specific: the cystic fibrosis child commonly needs one hundred and twenty to one hundred and fifty per cent of the standard energy for age with a high fat intake that is not restricted; the cardiac infant with a large shunt may need one hundred and thirty to one hundred and fifty kilocalories per kilogram per day; the dialysis child needs adequate energy to protect growth despite the anorexia of uraemia; and the oncology child needs protein at roughly one and a half times the baseline to counter the catabolism of treatment. [2] [11]
Protein is prescribed to the disease. The cystic fibrosis, Crohn disease and oncology child need high protein to rebuild tissue lost to catabolism, while the chronic kidney disease child needs protein held near the recommended dietary allowance for age when not on dialysis, and higher on dialysis to replace the amino-acid and peptide losses, the opposite of the historical instinct to restrict. The KDOQI guideline is explicit: maintain the recommended dietary allowance for age for children with chronic kidney disease stages two to five not on dialysis, avoiding both the excess that worsens uraemia and the restriction that stops growth, and increase it on dialysis to offset losses. [4]
Disease-specific interventions anchor the plan. In cystic fibrosis, pancreatic enzyme replacement at roughly five hundred to one thousand units of lipase per kilogram per meal with fat-soluble vitamin supplementation and adequate salt lets the high fat diet be absorbed; the dose is titrated to the symptoms and the weight. In Crohn disease, exclusive enteral nutrition for six to eight weeks, a polymeric or semi-elemental liquid formula as the sole source of nutrition, induces remission in around four in five children while restoring nutrition and avoiding the growth-suppressing steroids, and the Crohn disease exclusion diet with partial enteral nutrition extends the principle into maintenance. [3] [7]
The stepped nutrition support ladder moves from the least to the most invasive effective route. The first step is food fortification and oral nutritional supplements, adding energy and protein through fat, carbohydrate modules and ready-made supplements. The second is enteral nutrition by nasogastric or gastrostomy tube when intake is inadequate, intake is unsafe, or the gut works but the appetite does not, as in the cardiac infant, the cystic fibrosis child and the oncology child. The third is parenteral nutrition when the gut is unusable, as in short bowel syndrome, severe mucositis or post-operative ileus, delivered to the ESPGHAN energy and amino-acid guidelines. The route is chosen by the gut, the goal and the expected duration, not by preference. [8] [12]
The disease-specific doses examiners probe
The high-yield numbers anchor the plan. Cystic fibrosis energy is commonly one hundred and twenty to one hundred and fifty per cent of the standard for age, with a high fat intake and pancreatic enzymes at roughly five hundred to one thousand units of lipase per kilogram per meal. The cardiac infant with a large shunt may need one hundred and thirty to one hundred and fifty kilocalories per kilogram per day. Exclusive enteral nutrition for Crohn disease runs six to eight weeks and induces remission in around four in five children. The KDOQI protein target in chronic kidney disease is the recommended dietary allowance for age off dialysis, higher on dialysis. The oncology child needs protein at roughly one and a half times baseline. Refeeding starts at a conservative energy intake in the severely wasted child, with phosphate, potassium, magnesium and thiamine monitored.
[2][7][4][9]Specific Subtypes & Scenarios
The cystic fibrosis child is the archetype of malnutrition from increased demand and malabsorption, and the modern management is proactive. The energy prescription is high, the fat intake is liberal, and the fat malabsorption is managed with pancreatic enzyme replacement titrated to the meals and the symptoms, fat-soluble vitamin supplementation to prevent the deficiencies of vitamins A, D, E and K, and attention to salt losses in hot weather and exercise. The nutritional status is tracked against the body mass index and the lung function, because the two move together, and aggressive nutrition support, including overnight gastrostomy feeds, is used early rather than late. [2] [3]
The chronic kidney disease child is the archetype of malnutrition from restriction and loss, and the challenge is to protect growth while controlling the minerals. The energy is kept adequate, the protein is held near the recommended dietary allowance for age off dialysis and raised on dialysis, the phosphate is controlled with dietary restriction and binders rather than by starving the child of protein, the potassium is restricted only when genuinely high, the fluid matches the urine output and the dialysis, and the acidosis and renal osteodystrophy are treated. Recombinant human growth hormone is added for the child whose nutrition is optimised and whose stature remains poor, because it improves final height in chronic kidney disease. [4] [5]
The Crohn disease child is the archetype of nutrition as therapy, not just support. Exclusive enteral nutrition, six to eight weeks of a liquid formula as the sole source of nutrition, induces disease remission in around four in five children while rebuilding the nutritional deficit and sparing the growth-suppressing effect of steroids, and it is a first-line induction option in paediatric Crohn disease. The Crohn disease exclusion diet with partial enteral nutrition extends the dietary principle into maintenance for those who sustain remission on food, and iron deficiency is treated alongside the nutrition with oral or intravenous iron. [6] [8]
Across Australia, New Zealand and the United Kingdom, the Academy of Nutrition and Dietetics and ASPEN z-score framework underpins the diagnosis of disease-related malnutrition, condition-specific growth charts guide the cystic fibrosis and renal child, and the stepped support ladder is delivered by multidisciplinary teams with the dietitian central. The ESPGHAN and ESPEN guidelines shape parenteral nutrition, the KDOQI guideline shapes the kidney diet, and the ECCO and ESPGHAN consensus shapes the Crohn disease nutrition. Regional practice differs chiefly in access to dietitians, supplements, fortified feeds, growth hormone and home parenteral nutrition, which is why the burden of disease-related malnutrition falls hardest where access to specialised nutrition support is thin.
[1][3][6][12]Complications & Pitfalls
The complications of untreated disease-related malnutrition are the loss of the future the chronic illness was being treated to secure. Untreated malnutrition in cystic fibrosis worsens the lung function, in chronic kidney disease stunts the final height, in Crohn disease impairs the response to therapy and the pubertal growth spurt, in congenital heart disease raises the surgical and perioperative risk, and in paediatric cancer reduces the tolerance of chemotherapy and transplant and the chance of survival. Growth itself is an outcome, and a child treated for the disease but left malnourished has been half treated. [9] [11]
The treatment pitfalls are the failures the examiner rewards for naming. The first is refeeding a severely wasted chronic disease child to full target on day one, precipitating the phosphate, potassium and magnesium shifts and the thiamine depletion of refeeding syndrome. The second is over-restricting the kidney or cardiac diet until protein and energy fall and growth stops, treating the biochemistry at the cost of the child. The third is missing the iron, the fat-soluble vitamins or the trace elements that the disease silently depletes. The fourth is relying on the weight in the oedematous or steroid-treated child, where fluid and fat redistribution mask the sarcopenia that the mid-upper arm circumference reveals. [1] [5]
Prognosis & Disposition
The prognosis for the malnourished chronic disease child is good when the nutrition is recognised, measured and treated early, and poor when it is allowed to drift. Nutritional repletion restores the immune competence, the wound healing and the treatment tolerance that the depletion eroded, and the growth velocity recovers toward the genetic potential when the energy and protein balance is corrected before the epiphyses close. The cystic fibrosis child whose body mass index is sustained has better lung function, the Crohn disease child induced into remission with exclusive enteral nutrition catches up on growth, and the cardiac infant who reaches surgical repair well grown has the better perioperative course. [3] [7]
Disposition follows the disease and the severity of the malnutrition. The stable chronic disease child with mild malnutrition is managed in the medical home or the general paediatric clinic with a dietitian, a written nutrition plan and a serial growth review. The child with moderate or severe malnutrition, complex disease, technology-dependent feeding, or a failing plan is managed in the tertiary centre with the relevant subspecialty, the specialist dietitian and the nutrition support team, and the child on home parenteral nutrition needs a dedicated intestinal failure or nutrition support service. Transition to adult care carries the nutrition plan with it, because the faltering centile does not respect the age of transfer. [1] [11]
Special Populations
The technology-dependent child is the first special population, because the feeding tube and the pump that sustain life can also silently under-deliver nutrition. The child with a gastrostomy on overnight bolus or continuous feeds, the child on home parenteral nutrition for short bowel or intestinal failure, and the ventilator-dependent child with high energy needs all need a nutrition plan that is written, calculated, reviewed and adjusted as they grow, because the feed prescription written a year ago no longer matches the child today. The dietitian-led surveillance of the technology-dependent child prevents the slow drift into underfeeding that the family cannot detect. [1] [12]
The adolescent with chronic disease and the overlay of an eating disorder, body image distress or treatment fatigue is the second. The adolescent with Crohn disease, cystic fibrosis, chronic kidney disease or cancer may restrict intake for weight, appearance or control, and the disease and the disordered eating compound one another, so the nutrition plan is paired with a mental-health pathway that respects the adolescent's autonomy while protecting the growth. The transition to adult care is the third, because the nutrition support, the dietitian and the growth monitoring that paediatrics delivers must be handed over to an adult service that may not track growth, and the faltering centile reappears in the gap. [6] [11]
The remote, Indigenous, migrant and socioeconomically disadvantaged child is the fourth, because disease-related malnutrition clusters where access to dietitians, supplements, fortified feeds, growth hormone and home nutrition support is thin, and where food insecurity compounds the disease. Culturally safe shared care, telehealth support for the local team, subsidised access to feeds and supplements, and attention to the cost and availability of the prescribed nutrition are what make the plan deliverable for families far from the specialist centre, and the principles of the management are the same across regions even when the access is not. [1]
Evidence, Guidelines & Regional Differences
The evidence base is anchored on the consensus that brought standardised anthropometry to paediatric malnutrition and the disease-specific guidelines that shaped each domain. The Academy of Nutrition and Dietetics and ASPEN consensus established the six z-score indicators and the two-or-more rule for diagnosing paediatric malnutrition, grounding the assessment in a documented trajectory rather than an impression, and this framework underpins the diagnosis of disease-related malnutrition across all chronic conditions. [1]
The disease-specific guidelines fill in the requirements. The Stallings cystic fibrosis nutrition recommendations and the ESPEN-ESPGHAN-ECFS cystic fibrosis nutrition guideline set the high energy, high fat, enzyme and fat-soluble vitamin strategy and the growth targets. The KDOQI nutrition in children with chronic kidney disease guideline set the protein, energy, phosphate, potassium and growth hormone approach, and the Mak review framed the modern synthesis of how to help the kidney child thrive. [2] [4]
The ECCO and ESPGHAN consensus on paediatric Crohn disease integrated nutrition into the disease management, and the Cochrane review of enteral nutrition for induction, together with the Crohn disease exclusion diet trial, established exclusive enteral nutrition as a first-line induction therapy. The Mills and Tsintoni reviews framed the nutrition of the neonate with congenital heart disease, the Liu scoping review set the protein needs of the transplant child, and the ESPGHAN parenteral nutrition energy guideline anchored the parenteral component of the support ladder. Regional practice differs chiefly in access to dietitians, fortified feeds, growth hormone and home nutrition support rather than in the principles. [6] [9]
[1] [7]Exam Pearls
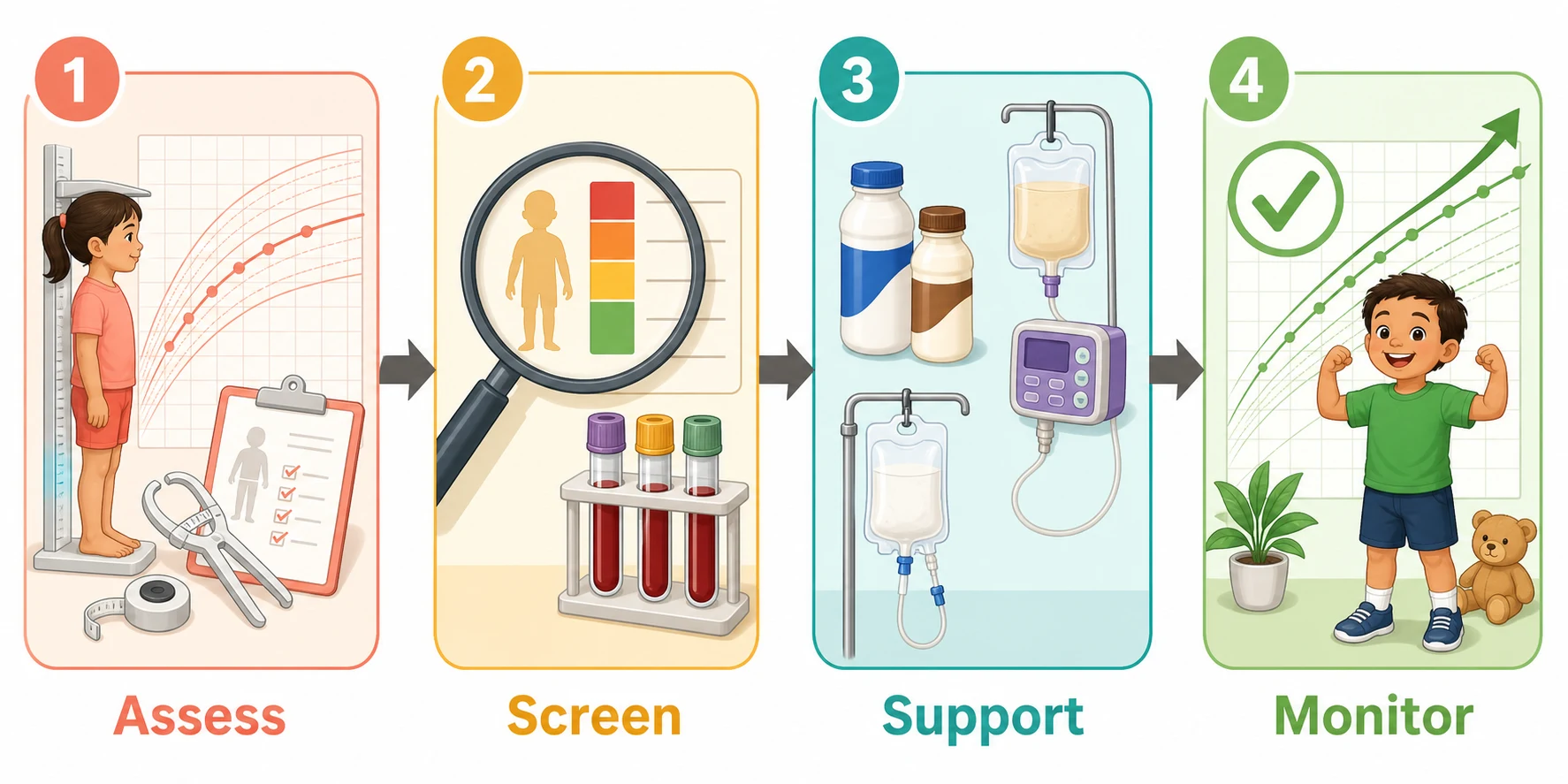
The nutrition management pathway — 'ASSM'
References
- [1]Becker P; Carney LN; Corkins MR; Monczka J; Smith E; Smith SE; Spear BA; White JV Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: indicators recommended for the identification and documentation of pediatric malnutrition (undernutrition). Nutr Clin Pract, 2015.PMID 25422273
- [2]Stallings VA; Stark LJ; Robinson KA; Feranchak AP; Quinton H Evidence-based practice recommendations for nutrition-related management of children and adults with cystic fibrosis and pancreatic insufficiency. J Am Diet Assoc, 2008.PMID 18442507
- [3]Turck D; Braegger CP; Colombo C; Declercq D; Morton A; Pancheva R; Robberecht E; Stern M; Toddenroth D; Van Dyck P ESPEN-ESPGHAN-ECFS guidelines on nutrition care for infants, children, and adults with cystic fibrosis. Clin Nutr, 2016.PMID 27068495
- [4]KDOQI Work Group KDOQI Clinical Practice Guideline for Nutrition in Children with CKD: 2008 update. Executive summary. Am J Kidney Dis, 2009.PMID 19231749
- [5]Mak RH; Iyengar A; Lai WM Nutrition in Children With Chronic Kidney Disease: How to Thrive? J Ren Nutr, 2023.PMID 37558172
- [6]Ruemmele FM; Veres G; Kolho KL; Griffiths A; Levine A; Escher JC; Amil Dias J; Barabino A; Braegger CP; Bronsky J; et al Consensus guidelines of ECCO/ESPGHAN on the medical management of pediatric Crohn's disease. J Crohns Colitis, 2014.PMID 24909831
- [7]Narula N; Dhillon A; Zhang D; Sherlock ME; Tondeur M; Zachos M Enteral nutritional therapy for induction of remission in Crohn's disease. Cochrane Database Syst Rev, 2018.PMID 29607496
- [8]Levine A; Wine E; Assa A; Sigall Boneh R; Shaoul R; Kori M; Cohen S; Peleg S; Shamaly H; On A; et al Crohn's Disease Exclusion Diet Plus Partial Enteral Nutrition Induces Sustained Remission in a Randomized Controlled Trial. Gastroenterology, 2019.PMID 31170412
- [9]Mills KI; Kim JH; Fogg K; Vricella L; McFadden D; Tobias JD Nutritional Considerations for the Neonate With Congenital Heart Disease. Pediatrics, 2022.PMID 36317972
- [10]Tsintoni A; Dimitriou G; Karatza AA Nutrition of neonates with congenital heart disease: existing evidence, conflicts and concerns. J Matern Fetal Neonatal Med, 2020.PMID 30608033
- [11]Liu K; Sharma P; Bartle J; Yap J; Fraser C; Newbould E; Sgouropoulou C; Foo J; Ha Y; Kennedy B; et al Protein intake and requirements in children and adolescents undergoing Hematopoietic Stem Cell Transplant (HSCT): An international benchmarking survey and a scoping review. Clin Nutr ESPEN, 2024.PMID 38972038
- [12]Joosten K; Embleton N; Yan W; Senterre T; Braegger CP; Bronsky J; Cai W; Campoy C; Colomb V; Domellof M; et al ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Energy. Clin Nutr, 2018.PMID 30078715