Paeds · gastroenterology-hepatology-and-nutrition
Oesophagitis, caustic ingestion and oesophageal injury
Also known as Oesophagitis, caustic ingestion and oesophageal injury · Button battery ingestion · Caustic (corrosive) oesophageal injury · Eosinophilic oesophagitis · Reflux oesophagitis · Oesophageal foreign body
Fellowship guide to paediatric oesophagitis and oesophageal injury, built around the button-battery emergency: the reflux, eosinophilic, infective and pill causes of oesophagitis; the liquefactive alkali versus coagulative acid mechanism of caustic ingestion with the Zargar endoscopic grading; and the lithium coin-cell button battery that generates hydroxide at its negative pole and burns through the oesophageal wall within two hours, with honey and sucralfate as the pre-removal mitigations, emergent endoscopic removal, and the aorto-oesophageal fistula that can exsanguinate a child days after the battery is out.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Oesophageal injury in a child spans two very different worlds that share one lumen. On one side is oesophagitis, the inflammation of the oesophageal lining from reflux, allergy, infection or medication — a chronic and usually treatable problem. On the other side is acute corrosive injury, where a swallowed caustic chemical or a lodged button battery burns the wall in real time. The whole skill lies in telling the slow inflammatory problem from the fast destructive one, because their timescales, dangers and management could not be more different. [7]
The single most important idea in this topic is that a lithium coin-cell button battery impacted in the oesophagus is a surgical emergency measured in hours, not days. Once lodged against the moist mucosa it completes an electrical circuit through the tissue, generates hydroxide at its negative pole, and produces a spreading liquefactive burn that begins within two hours. Everything else in this topic can wait for a clinic; a button battery in the oesophagus cannot. [1] [4]
Classification
Oesophageal injury is best sorted by the mechanism doing the damage, because the mechanism sets the urgency and the treatment. The first group is oesophagitis, the inflammatory disorders of the lining: reflux oesophagitis from acid exposure, eosinophilic oesophagitis from an allergic response, infective oesophagitis in the immunocompromised child, and pill oesophagitis from a tablet held against the wall. The second group is acute injury: a swallowed caustic chemical, an impacted button battery, or a mechanical foreign body such as a coin. [7] [11]
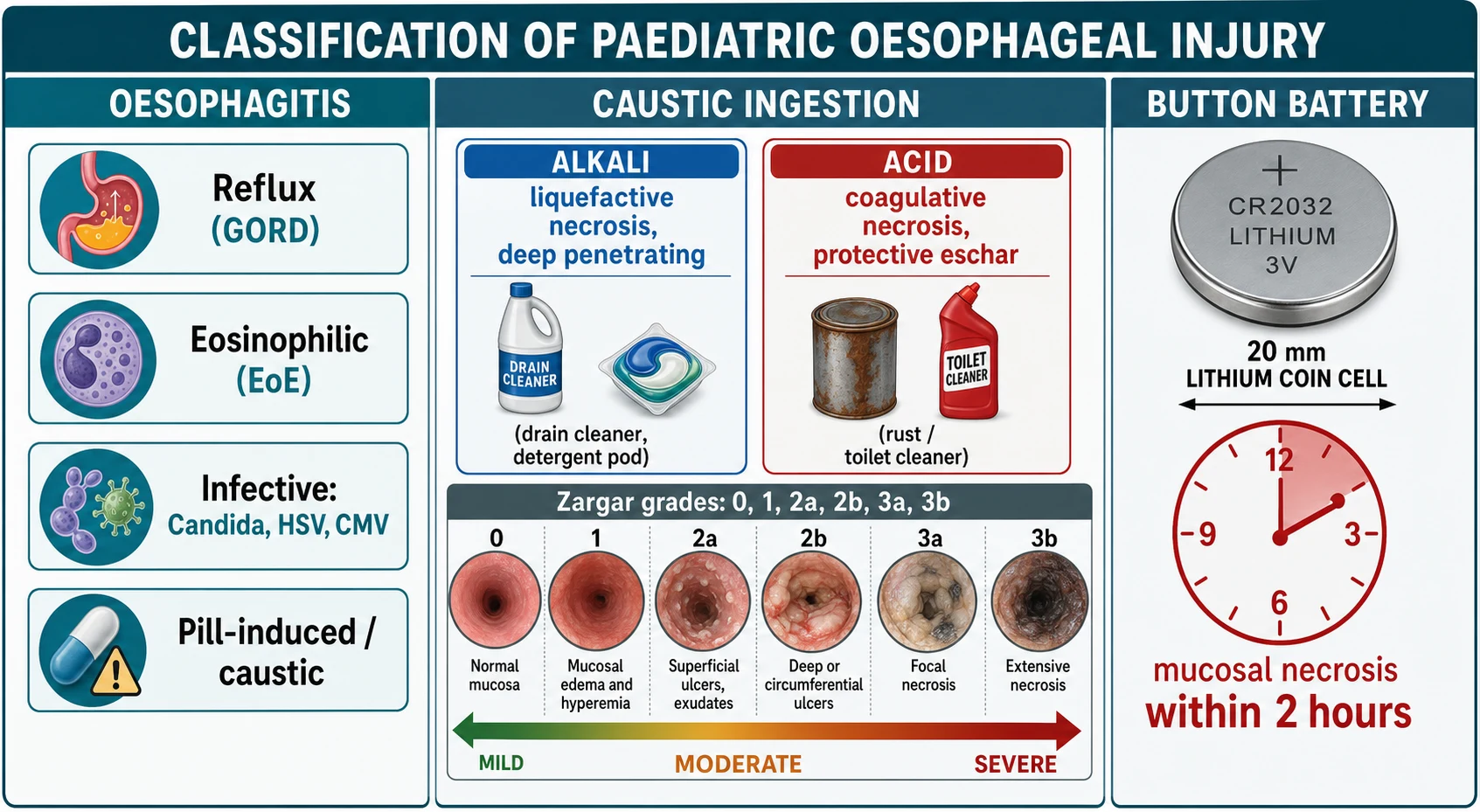
Caustic ingestion is then subdivided by the chemistry of the agent, which predicts the pattern of the burn. Alkalis such as drain cleaner, oven cleaner and dishwasher detergent produce liquefactive necrosis that penetrates deeply and can become transmural. Acids such as rust removers and toilet cleaners produce coagulative necrosis, where the eschar limits the depth of injury but the stomach is often hit harder. The severity of the burn, whatever the agent, is graded at endoscopy using the modified Zargar classification. [7] [9]
The Zargar endoscopic grading is the language examiners expect for caustic severity. Grade 0 is normal mucosa; grade 1 is mucosal oedema and hyperaemia; grade 2a is superficial ulceration, friability and exudate; grade 2b adds deep discrete or circumferential ulceration; grade 3a is focal necrosis; and grade 3b is extensive necrosis. The grade drives the plan, because a grade 2b or 3 burn carries a high risk of stricture and dictates a very different feeding and follow-up pathway from a grade 1 burn. [9] [7]
Epidemiology & Risk Factors
Button battery ingestions have risen sharply over the last two decades, driven by the spread of large, powerful 20 mm lithium coin cells in remote controls, key fobs, toys, hearing aids and greeting cards. Litovitz and colleagues, analysing thousands of cases from the National Battery Ingestion Hotline, showed that severe and fatal outcomes rose in step with the availability of these larger cells, and that the child at greatest risk is the toddler under four who swallows a 20 mm or larger battery. The battery that lodges in the oesophagus, rather than passing through, is the one that injures. [4] [5]
Caustic ingestion is likewise a disease of the exploring toddler, who drinks a decanted household chemical stored within reach, most often from an unlabelled drink bottle. A second, smaller peak occurs in adolescents, where ingestion may be deliberate and self-harm related, and these ingestions tend to involve larger volumes and more severe burns. Regulation of child-resistant packaging and the concentration of retail products has reduced but not eliminated the burden. [7] [8]
The chronic oesophagitides have their own epidemiology. Reflux oesophagitis is common across infancy and childhood and clusters in children with neurodisability, repaired oesophageal atresia and hiatus hernia. Eosinophilic oesophagitis has risen in incidence over the same period as the button battery, affects boys more than girls, and is strongly associated with a personal or family history of atopy — asthma, eczema, allergic rhinitis and food allergy. Infective oesophagitis is confined almost entirely to the immunocompromised child. [10] [11]
Pathophysiology
The button battery injures by electrolysis, not by leakage of its contents. When the two poles of an intact battery contact the moist mucosa on either side, the tissue completes the circuit and current flows. At the negative pole, the reduction of water generates hydroxide ions, the local pH climbs above 12, and a liquefactive alkaline burn begins that spreads into the wall exactly as an ingested alkali would. The narrow negative face of the coin cell is where the deepest injury occurs, which is why the orientation of the battery on the lateral X-ray predicts the side of maximal damage. [1] [2]
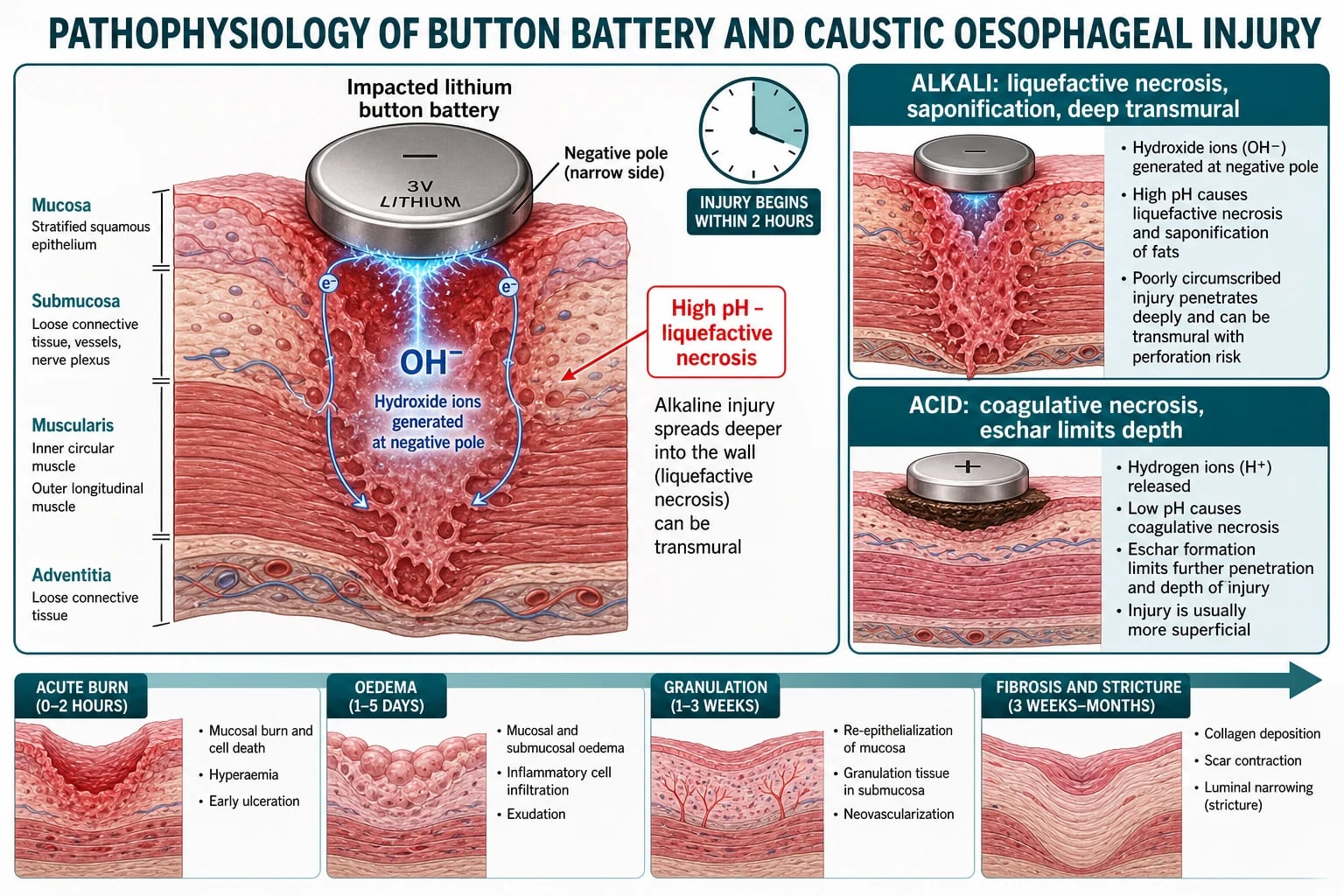
Ingested caustics injure by their chemistry. An alkali dissolves cell membranes and saponifies fats, producing liquefactive necrosis that keeps penetrating because there is no barrier to stop it, so alkali burns are deep and can become transmural with perforation. An acid coagulates surface proteins into a firm eschar that limits further penetration, so acid burns are often more superficial in the oesophagus, although the acid pools in and injures the stomach. Both agents cause the most severe injury at the sites of physiological narrowing where transit slows. [7] [8]
Whatever the initial insult, the wall heals through a predictable sequence, and understanding it explains the timing of every intervention. The acute burn and cell death occupy the first hours; mucosal and submucosal oedema and inflammation peak over one to five days; granulation and re-epithelialisation follow over one to three weeks; and collagen deposition, scar contraction and luminal narrowing — the stricture — develop from three weeks to months later. The tissue is weakest and most friable in the second week, which is precisely why endoscopy is done early or deferred, never in the middle. [7] [9]
Clinical Presentation
The button battery is dangerous precisely because it can be silent. Many ingestions are unwitnessed, and the toddler may have no symptoms at all while the burn is already under way. When symptoms do appear they are non-specific — drooling, refusal to feed, vomiting, cough, chest or throat pain, and irritability — and they are easily mistaken for a viral illness or croup. Any of these symptoms in a toddler, with or without a witnessed ingestion, should prompt an immediate X-ray to exclude a battery. [1] [4]
Caustic ingestion usually declares itself quickly. The child may have oral and lip burns, drooling and refusal to swallow, retrosternal or abdominal pain, vomiting and haematemesis. The most feared early feature is airway involvement — stridor, hoarseness, a change in voice or respiratory distress — which signals a laryngeal or supraglottic burn and impending obstruction. The absence of oral burns does not exclude significant oesophageal injury, and the presence of oral burns does not reliably predict its severity. [7] [8]
The chronic oesophagitides present over a longer arc. Reflux oesophagitis causes regurgitation, heartburn, feeding aversion, irritability and, when severe, haematemesis and iron-deficiency anaemia. Eosinophilic oesophagitis presents in an age-dependent way: infants and young children have feeding difficulty, food refusal and failure to thrive, while older children and adolescents have dysphagia and the classic food bolus impaction that brings them to the emergency department. Infective oesophagitis presents with odynophagia and dysphagia in a child known to be immunocompromised. [10] [11]
Differential Diagnosis
The first differential in the drooling, distressed toddler is the one that must not be missed: is this a button battery, a caustic ingestion, a foreign body, or an infective cause such as epiglottitis or croup. The history of access to batteries or chemicals, the presence of oral burns, and above all an urgent X-ray separate these quickly. In a child with any suspicion of ingestion, imaging comes before reassurance, because a battery gives the same drooling and feed refusal as a viral illness. [1] [6]
A button battery must be distinguished from a coin on imaging, because the management diverges completely: a coin in the oesophagus can often be observed briefly or removed semi-electively, whereas a battery must come out within two hours. The halo or double-ring sign on the frontal film and the step-off on the lateral film identify the battery. When there is genuine doubt, the object is treated as a battery until proven otherwise. [1] [6]
Among the chronic causes, dysphagia and food impaction in a child raise eosinophilic oesophagitis, a peptic or caustic stricture, an oesophageal web or ring, and a motility disorder such as achalasia. Reflux oesophagitis and eosinophilic oesophagitis overlap clinically and can only be separated by endoscopy and biopsy, since eosinophilic disease requires fifteen or more eosinophils per high-power field on histology to be confirmed. Infective oesophagitis is separated by its context of immunocompromise and its endoscopic appearance. [11] [12]
Clinical & Bedside Assessment
Assessment begins with the airway and breathing, because both a caustic burn and a large impacted foreign body can obstruct. Listen for stridor and a change in voice, look for drooling and the inability to swallow secretions, and assess the work of breathing. A child who cannot handle their own saliva has a high-grade obstruction or a significant airway burn and needs urgent senior and anaesthetic involvement before anything else is done. [7] [8]
The focused history is the diagnostic engine here. Establish exactly what was swallowed, how much, when, and whether it was witnessed; ask specifically about access to button batteries, decanted chemicals and medications; and for the chronic presentations, ask about dysphagia, food impaction, heartburn, feeding aversion, growth and atopy. The single most valuable number is the time since ingestion, because it drives the two-hour battery clock and the twelve-to-twenty-four-hour endoscopy window for caustics. [1] [6]
Bedside approach to the child with suspected oesophageal injury
Assess and secure the airway first: stridor, voice change, drooling and work of breathing
Take a focused ingestion history: what, how much, when, witnessed or not
Ask specifically about access to button batteries, decanted chemicals and medications
Examine the mouth and lips for burns, and the chest and abdomen for pain or peritonism
Obtain an urgent X-ray of the neck, chest and abdomen to locate and identify any object
If a battery is suspected, escalate for removal within two hours in parallel with assessment
For caustics, keep nil by mouth, give nothing to induce emesis or neutralise, and plan endoscopy
Examine the mouth and lips for burns, remembering that their absence does not exclude oesophageal injury, and examine the chest and abdomen for signs of perforation — surgical emphysema, peritonism, or a rigid abdomen. In the child with chronic symptoms, plot growth, look for signs of atopy, and assess hydration and nutrition, because eosinophilic oesophagitis and severe reflux both cause faltering growth. The bedside examination frames the urgency, but in acute injury the definitive assessment is endoscopic. [7] [11]
Investigations
The plain radiograph is the first and most urgent investigation in any suspected ingestion. A frontal and lateral film of the neck, chest and abdomen locates a radio-opaque object and, crucially, distinguishes a button battery from a coin by the halo or double-ring sign on the frontal view and the step-off on the lateral view. The lateral view also shows the orientation of the battery, identifying the negative pole and therefore the wall at greatest risk. A battery that has already reached the stomach in an asymptomatic older child is managed very differently from one lodged in the oesophagus. [1] [6]
Endoscopy is the definitive investigation for both acute and chronic injury, but its timing differs by cause. For an oesophageal button battery it is immediate and therapeutic — the scope removes the battery within two hours. For a caustic ingestion it is diagnostic and staged, performed at twelve to twenty-four hours to allow the burn to declare itself but before the wall becomes dangerously friable, and it grades the injury on the Zargar scale that drives the plan. Endoscopy before twelve hours underestimates the depth, and endoscopy between two and about fifteen days is avoided because the softened tissue perforates easily. [9] [7]
For the chronic oesophagitides the definitive test is endoscopy with biopsy. Eosinophilic oesophagitis is confirmed histologically by fifteen or more eosinophils per high-power field, together with the clinical picture of oesophageal dysfunction and after other causes are considered, and its endoscopic hallmarks are longitudinal furrows, oedema, white exudates, concentric rings and, in longstanding disease, strictures. Reflux oesophagitis shows distal erosions. When perforation is suspected after a caustic injury, a water-soluble contrast study or a CT of the chest defines the leak and the transmural extent. [12] [11]
Management — Resuscitation
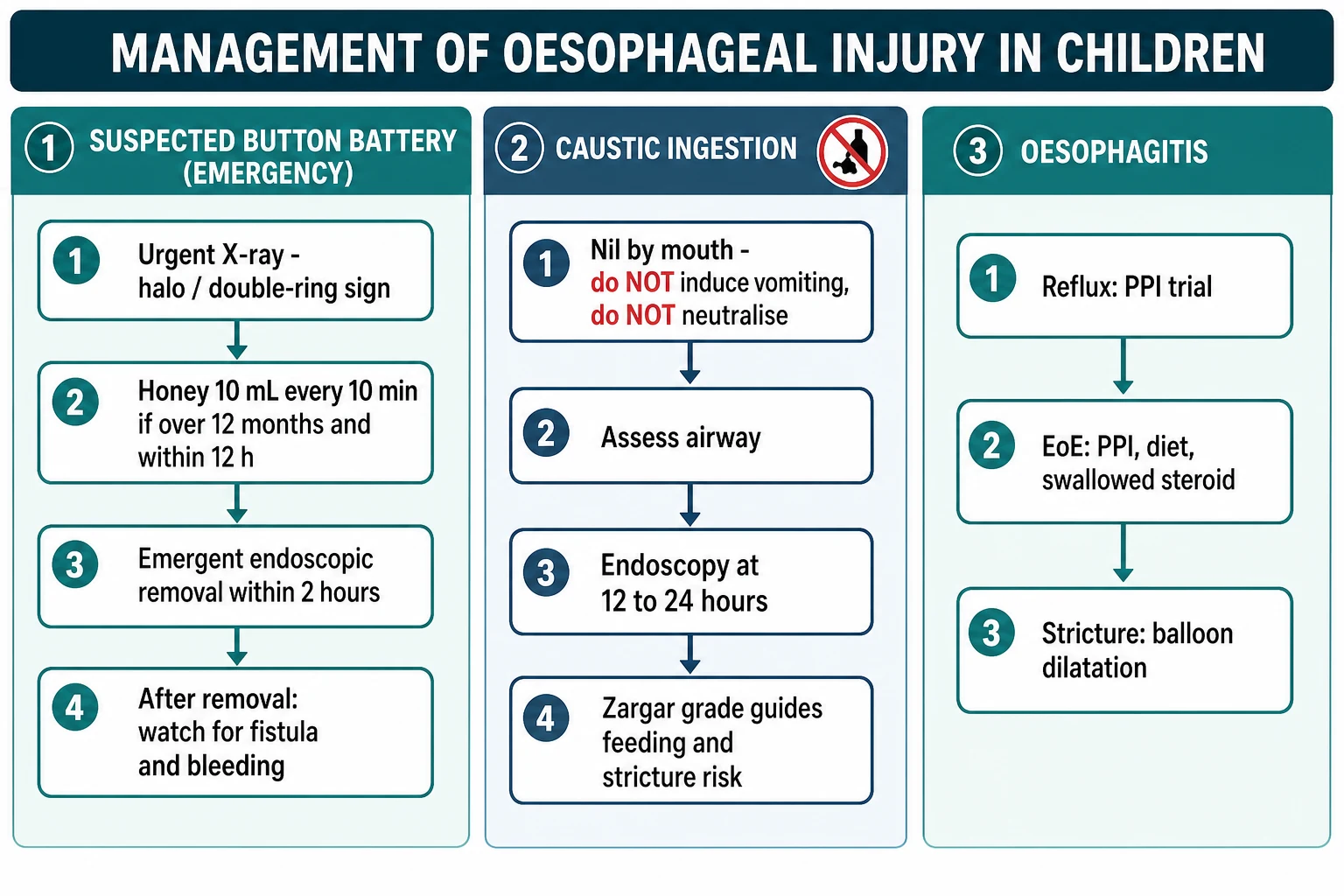
The resuscitation of a caustic ingestion starts and often ends with the airway. Stridor, hoarseness or respiratory distress signals a laryngeal or supraglottic burn, and the airway must be secured early, by an experienced operator, before progressive oedema makes intubation impossible. Alongside this, the child is kept strictly nil by mouth, given analgesia and intravenous fluids, and never made to vomit, given a neutralising chemical, or have a nasogastric tube passed blindly — each of these re-injures the oesophagus or risks perforation. Dilution with water or milk has no proven benefit and is not recommended once the child is in hospital. [8] [7]
The button battery resuscitation is a race to removal. The moment an oesophageal battery is confirmed or strongly suspected, the child is escalated for emergent endoscopic removal within two hours while pre-removal mitigation is started. In a child older than twelve months who ingested the battery within the preceding twelve hours and can swallow, honey ten millilitres is given every ten minutes for up to six doses while the theatre is prepared; the honey coats the battery and buffers the alkaline burn without delaying removal. Sucralfate suspension is the in-hospital alternative. Neither honey nor sucralfate is given if there are signs of perforation or sepsis, or if the airway is at risk. [1] [2]
Honey (pre-removal mitigation for an oesophageal button battery)
Loading dose
10 mL orally every 10 minutes, up to 6 doses
Maintenance dose
Stop at endoscopic removal; do not delay removal to give honey
Perforation and haemorrhage are the resuscitation emergencies that override everything else. A child with a caustic or battery injury who develops signs of perforation — mediastinitis, peritonism, surgical emphysema or shock — needs urgent surgical and intensive-care involvement and does not go for elective endoscopy. A child who bleeds after a battery injury may have an aorto-oesophageal fistula and can exsanguinate within minutes, requiring immediate resuscitation with blood and emergency surgery. [1] [8]
Management — Definitive & Stepwise
Definitive management of an oesophageal button battery is emergent endoscopic removal within two hours, followed by inspection of the burn and a plan for the delayed complications that removal does not prevent. At removal, some centres irrigate the injured mucosa with dilute sterile acetic acid to neutralise residual alkali. Because the aorto-oesophageal fistula can present up to three weeks later, a child with a significant oesophageal burn is admitted, kept under close observation, and has imaging of the great vessels considered before feeding is advanced. The family is warned explicitly about the delayed bleeding risk. [1] [2]
Definitive management of a caustic ingestion follows the Zargar grade obtained at the twelve-to-twenty-four-hour endoscopy. Grade 1 and 2a burns heal well; the child is fed as tolerated and discharged with follow-up. Grade 2b and 3 burns are the high-risk group for stricture and are managed with prolonged nutritional support, sometimes nasojejunal or parenteral, and a planned surveillance programme. The role of corticosteroids to prevent stricture remains controversial and is not routine, though high-dose steroids for grade 2b burns are used in some centres; antibiotics are added when steroids are used or perforation is suspected. Surgery is reserved for perforation and for the destroyed oesophagus that requires later replacement. [7] [9]
Definitive management of the oesophageal button battery
Confirm oesophageal location on X-ray and read the negative-pole orientation
Start honey or sucralfate mitigation if eligible, without delaying removal
Remove the battery endoscopically within two hours and inspect the burn
Consider dilute acetic acid irrigation of the injured mucosa at removal
Admit and observe for delayed complications; keep nil by mouth if the burn is deep
Image the great vessels and consider fistula risk before advancing feeds
Warn the family of the aorto-oesophageal fistula and bleeding risk for up to three weeks
The chronic oesophagitides are managed by cause. Reflux oesophagitis is treated with a proton pump inhibitor and reflux-reduction measures along the lines of the joint NASPGHAN and ESPGHAN guideline. Eosinophilic oesophagitis is treated with one of three first-line strategies — a proton pump inhibitor, dietary elimination, or a swallowed topical corticosteroid such as fluticasone or budesonide — with the biologic dupilumab and endoscopic dilatation of strictures for refractory disease. A caustic or peptic stricture, once formed, is managed with a programme of endoscopic balloon dilatation, repeated as the stricture recurs. [10] [11]
The stricture surveillance and dilatation programme examiners expect
A grade 2b or 3 caustic burn scars over weeks to months. The child is followed with an awareness that dysphagia signals a developing stricture, and a contrast swallow or endoscopy confirms it. Established strictures are treated with endoscopic balloon or bougie dilatation, often needing repeated sessions over months to years, with stents or, in the worst cases, oesophageal replacement by gastric pull-up or colonic interposition when dilatation fails. The long-term counselling must also cover the lifelong, roughly thousandfold increased risk of oesophageal squamous cell carcinoma decades later, which warrants late endoscopic surveillance. [7] [8]
Specific Subtypes & Scenarios
The oesophageal button battery is the defining scenario of this topic. A toddler with a witnessed or suspected ingestion, or with unexplained drooling and feed refusal, has an urgent X-ray; a battery in the oesophagus triggers emergent removal within two hours with honey or sucralfate mitigation on the way to theatre. The battery that has passed into the stomach in an asymptomatic child older than five with a cell under twenty millimetres can often be managed with observation and a repeat film, whereas a large cell, a symptomatic child, or a co-ingested magnet changes the plan to removal. [1] [4]
The magnet-plus-battery and the multiple-magnet ingestion is a distinct surgical scenario. Two or more high-powered magnets, or a magnet with a battery, attract across bowel walls, trap the tissue between them, and cause pressure necrosis, fistula and perforation. These ingestions are managed aggressively with endoscopic or surgical removal rather than observation, because the damage is done by attraction across loops of bowel and will not resolve spontaneously. [6] [4]
Across Australia, New Zealand, the United Kingdom and North America, button batteries are managed through a combination of prevention and rapid response. Australia introduced mandatory safety and information standards for button batteries after high-profile child deaths, requiring secure battery compartments and child-resistant packaging. Poisons information centres in every jurisdiction give immediate advice, and tertiary paediatric centres run emergency pathways for removal within two hours. The unified message is prevention at the point of product design and an emergency response measured in hours. [1] [5]
Eosinophilic oesophagitis is the chronic subtype most often examined. The adolescent who arrives with a food bolus stuck in the oesophagus, or the young child with longstanding feeding difficulty and failure to thrive, is investigated with endoscopy and biopsy showing fifteen or more eosinophils per high-power field. First-line treatment is a proton pump inhibitor, an elimination diet, or a swallowed topical steroid, with dupilumab and dilatation reserved for refractory or fibrostenotic disease. The pill oesophagitis scenario — an adolescent with sudden retrosternal pain after taking doxycycline, a bisphosphonate or a potassium tablet with too little water at bedtime — is the benign mimic that resolves with stopping the drug and taking future tablets upright with fluid. [11] [12]
Complications & Pitfalls
The complications of oesophageal injury are dominated by the delayed catastrophes of the button battery. An oesophageal burn can erode into the trachea to form a tracheo-oesophageal fistula, or into the aorta or a great vessel to form an aorto-oesophageal fistula that exsanguinates the child, and both can present days to weeks after the battery is removed. Other complications include oesophageal perforation and mediastinitis, oesophageal stricture, vocal cord paralysis from recurrent laryngeal nerve injury, and spondylodiscitis. The lesson is that removing the battery ends the burn but not the risk. [1] [3]
Caustic ingestion shares the perforation, mediastinitis and stricture complications and adds its own long tail. The stricture that forms over weeks to months is the commonest late problem and drives a dilatation programme. The most sinister late complication is oesophageal squamous cell carcinoma, whose risk is increased roughly a thousandfold or more decades after a severe alkali burn, justifying lifelong awareness and late endoscopic surveillance. Antral or pyloric stricture follows acid ingestion where the stomach bore the brunt. [7] [8]
The pitfalls are pitfalls of recognition and of the first response. The great recognition pitfall is mistaking a battery for a coin and observing it, or attributing a battery's drooling and feed refusal to a viral illness and not imaging. The great treatment pitfalls are inducing vomiting or neutralising after a caustic ingestion, passing a blind nasogastric tube through a burned oesophagus, feeding a child before the airway and burn are assessed, and discharging a child after battery removal without warning the family about delayed bleeding. [7] [1]
Prognosis & Disposition
Prognosis is set by the depth of the burn and the speed of the response. A button battery removed within two hours, before a deep burn is established, can have an excellent outcome, whereas a battery lodged for many hours can cause fatal fistula formation regardless of how skilfully it is later removed — which is the entire rationale for the two-hour rule. Mild caustic burns (Zargar grade 1 and 2a) heal without sequelae, while deep burns (grade 2b and 3) carry a high risk of stricture and a lifelong, small risk of malignancy. [1] [9]
Disposition follows the injury. A suspected oesophageal button battery goes immediately to a centre capable of emergency endoscopic removal, with retrieval arranged in parallel for a rural or remote child rather than waiting. A significant caustic or battery burn is admitted for observation, airway monitoring, nutritional support and surveillance for delayed complications. The chronic oesophagitides are managed in paediatric gastroenterology outpatients with endoscopic follow-up, and a child with a caustic stricture enters a long-term dilatation and surveillance programme with the surgical, gastroenterology and nutrition teams. [6] [7]
Special Populations
The child with neurodisability is at higher risk across the whole topic. Impaired swallow and communication mean ingestions may be unwitnessed and symptoms hard to interpret, gastro-oesophageal reflux and reflux oesophagitis are far more common, and the child may already be gastrostomy-fed with an altered anatomy. A low threshold for imaging and endoscopy, and close attention to the carer's report of a change, protect this group. [10] [6]
The immunocompromised child — with malignancy, transplantation, HIV or primary immunodeficiency — is the population in whom infective oesophagitis occurs. Candida produces white plaques and is the commonest; herpes simplex produces vesicles and small ulcers; cytomegalovirus produces large deep ulcers. Odynophagia and dysphagia in such a child warrant endoscopy with biopsy and culture, and targeted antifungal or antiviral therapy, because the cause cannot be assumed. [11] [12]
The adolescent is a special population in two ways. Deliberate caustic ingestion as an act of self-harm involves larger volumes and more severe burns and mandates a mental-health assessment alongside the physical management. Pill oesophagitis clusters in adolescents taking doxycycline, bisphosphonates, non-steroidal anti-inflammatories, iron or potassium tablets with too little water, often at bedtime, and is prevented by counselling to take tablets upright with a full glass of water. Socioeconomic disadvantage and unsafe storage of decanted chemicals and loose batteries increase the risk of accidental ingestion across all ages. [7] [8]
Evidence, Guidelines & Regional Differences
The button-battery evidence base is anchored on the Litovitz analyses of the National Battery Ingestion Hotline, which quantified the rising hazard of the large lithium coin cell and defined the highest-risk child, and on the Jatana task-force update, which turned that epidemiology into prevention and management recommendations. The ESPGHAN position paper by Mubarak and colleagues is the modern paediatric guideline that codifies the two-hour removal rule, the honey and sucralfate mitigation, and the surveillance for delayed complications. The Anfang laboratory work established the pH-neutralising irrigation concept that underpins the honey and sucralfate strategy. [4] [1]
The caustic-injury evidence rests on the Zargar endoscopic classification, which remains the reference grading tool three decades on, and on comprehensive reviews such as Contini and Scarpignato and the Hoffman clinical review in the New England Journal of Medicine, which set out the airway-first, no-emesis, no-neutralisation, graded-endoscopy approach. The controversy that persists is the role of corticosteroids in preventing stricture, which is not established and not routine, and the exact timing of endoscopy, which converges on a twelve-to-twenty-four-hour window. [7] [8]
The oesophagitis guidelines complete the picture. The joint NASPGHAN and ESPGHAN paediatric reflux guideline by Rosen and colleagues frames the diagnosis and proton pump inhibitor treatment of reflux oesophagitis, the Lucendo European guideline and the Dellon AGREE consensus define the diagnosis and three first-line treatments of eosinophilic oesophagitis, and the Kramer NASPGHAN clinical report covers the wider management of ingested foreign bodies. Across ANZ, the United Kingdom, Europe and North America the principles are uniform, with regional differences confined to product-safety regulation and the precise thresholds for observing a battery that has already reached the stomach. [10] [12]
The clinical response to oesophageal injury is essentially uniform across high-resource settings; the meaningful regional difference is prevention. Australia's mandatory button-battery safety and information standards, introduced after child deaths, are among the most stringent in the world, requiring secure compartments and child-resistant packaging. Elsewhere, regulation of battery packaging and of the concentration and storage of household caustics varies, and this variation, more than any difference in acute treatment, shapes the incidence and the outcomes. [5] [1]
Exam Pearls
Button battery emergency — 'BATTERY'
References
- [1]Mubarak A; Benninga MA; Broekaert I; Dolinsek J; Homan M; Mas E; Miele E; Pienar C; et al Diagnosis, Management, and Prevention of Button Battery Ingestion in Childhood: A European Society for Paediatric Gastroenterology Hepatology and Nutrition Position Paper. J Pediatr Gastroenterol Nutr, 2021.PMID 33555169
- [2]Anfang RR; Jatana KR; Linn RL; Rhoades K; Fry J; Jacobs IN pH-neutralizing esophageal irrigations as a novel mitigation strategy for button battery injury. Laryngoscope, 2019.PMID 29889306
- [3]Jatana KR; Litovitz T; Reilly JS; Koltai PJ; Rider G; Jacobs IN Pediatric button battery injuries: 2013 task force update. Int J Pediatr Otorhinolaryngol, 2013.PMID 23896385
- [4]Litovitz T; Whitaker N; Clark L; White NC; Marsolek M Emerging battery-ingestion hazard: clinical implications. Pediatrics, 2010.PMID 20498173
- [5]Litovitz T; Whitaker N; Clark L Preventing battery ingestions: an analysis of 8648 cases. Pediatrics, 2010.PMID 20498172
- [6]Kramer RE; Lerner DG; Lin T; Manfredi M; Shah M; Stephen TC; Gibbons TE; Pall H; et al Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee. J Pediatr Gastroenterol Nutr, 2015.PMID 25611037
- [7]Contini S; Scarpignato C Caustic injury of the upper gastrointestinal tract: a comprehensive review. World J Gastroenterol, 2013.PMID 23840136
- [8]Hoffman RS; Burns MM; Gosselin S Ingestion of Caustic Substances. N Engl J Med, 2020.PMID 32348645
- [9]Zargar SA; Kochhar R; Mehta S; Mehta SK The role of fiberoptic endoscopy in the management of corrosive ingestion and modified endoscopic classification of burns. Gastrointest Endosc, 1991.PMID 2032601
- [10]Rosen R; Vandenplas Y; Singendonk M; Cabana M; DiLorenzo C; Gottrand F; Gupta S; Langendam M; et al Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr, 2018.PMID 29470322
- [11]Lucendo AJ; Molina-Infante J; Arias Á; von Arnim U; Bredenoord AJ; Bussmann C; Amil Dias J; Bove M; et al Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterol J, 2017.PMID 28507746
- [12]Dellon ES; Liacouras CA; Molina-Infante J; Furuta GT; Spergel JM; Zevit N; Spechler SJ; Attwood SE; et al Updated International Consensus Diagnostic Criteria for Eosinophilic Esophagitis: Proceedings of the AGREE Conference. Gastroenterology, 2018.PMID 30009819