Paeds · gastroenterology-hepatology-and-nutrition
Parenteral nutrition and refeeding syndrome
Also known as Parenteral nutrition · Total parenteral nutrition · TPN · Refeeding syndrome · Refeeding hypophosphataemia · Intestinal failure-associated liver disease · IFALD · Parenteral nutrition-associated cholestasis · PNAC · Parenteral nutrition-associated liver disease
Fellowship guide to prescribing parenteral nutrition safely in children and to preventing refeeding syndrome when nutrition is restarted after starvation. The page covers the rule that the gut should be fed first and parenteral nutrition reserved for when it cannot, the four parenteral streams of glucose given as a glucose infusion rate, amino acids, lipid and electrolytes with trace elements, how to build the bag to an infant target of around 90 to 120 kcal per kilogram per day, the complications of metabolic disturbance, catheter sepsis and intestinal failure-associated liver disease, and the refeeding principle that a starved child restarted on nutrition needs thiamine, conservative starting calories, and correction and monitoring of phosphate, potassium and magnesium.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a premature baby whose gut is too immature to absorb milk, hanging a bag of parenteral nutrition from a central line and growing on it for weeks. Picture a malnourished adolescent with anorexia nervosa admitted for refeeding, whose phosphate crashes on day two. These two children sit at the heart of this topic, and they share one governing idea: nutrition saves starved children, but nutrition delivered the wrong way can kill them. Parenteral nutrition is the intravenous delivery of nutrients when the gut cannot be used, and refeeding syndrome is the metabolic collapse that follows when nutrition is reintroduced too quickly to a starved body. [3] [5]
The vocabulary must be held precisely because examiners trade in it. Parenteral nutrition delivers fluid, glucose, amino acids, lipid, electrolytes, vitamins and trace elements directly into the bloodstream, bypassing the gut entirely. Total parenteral nutrition means the regimen supplies all of the childs nutritional needs; partial parenteral nutrition supplements what the gut can still absorb. The older abbreviation TPN still appears on wards, but the modern term is simply parenteral nutrition. [3]
Refeeding syndrome is defined by the biochemical and fluid disturbances that appear when carbohydrate is reintroduced to a starved patient. The hallmark is a fall in serum phosphate, potassium and magnesium within the first 72 hours, driven by an insulin surge that pushes these ions into the cells, accompanied by thiamine depletion and sodium and fluid retention that can precipitate cardiac failure. It is not a rare curiosity; it is a predictable consequence of feeding the starved child too fast, and the prevention is entirely in the prescribers hands. [5] [6]
The governing principle of management, then, is to reserve the parenteral route for genuine gut failure, to build the bag carefully around the four nutrient streams, to protect the central line and the liver, and to treat every starved child as a refeeding risk before the first calorie goes in. [3] [5]
Classification
The first classification decision is whether the child needs parenteral nutrition at all, because the gut is always the preferred route. The child needs the vein when the gut cannot be used for a meaningful period: an infant after necrotising enterocolitis or volvulus with a shortened or resting bowel, a premature baby whose gut is too immature to tolerate milk, a child with an ileus or obstruction after surgery, or a severely malnourished child who cannot meet needs enterally. When the gut works even a little, trophic enteral feeding runs alongside the parenteral line, because the gut atrophies when it is starved and adapts when it is fed. [3] [12]
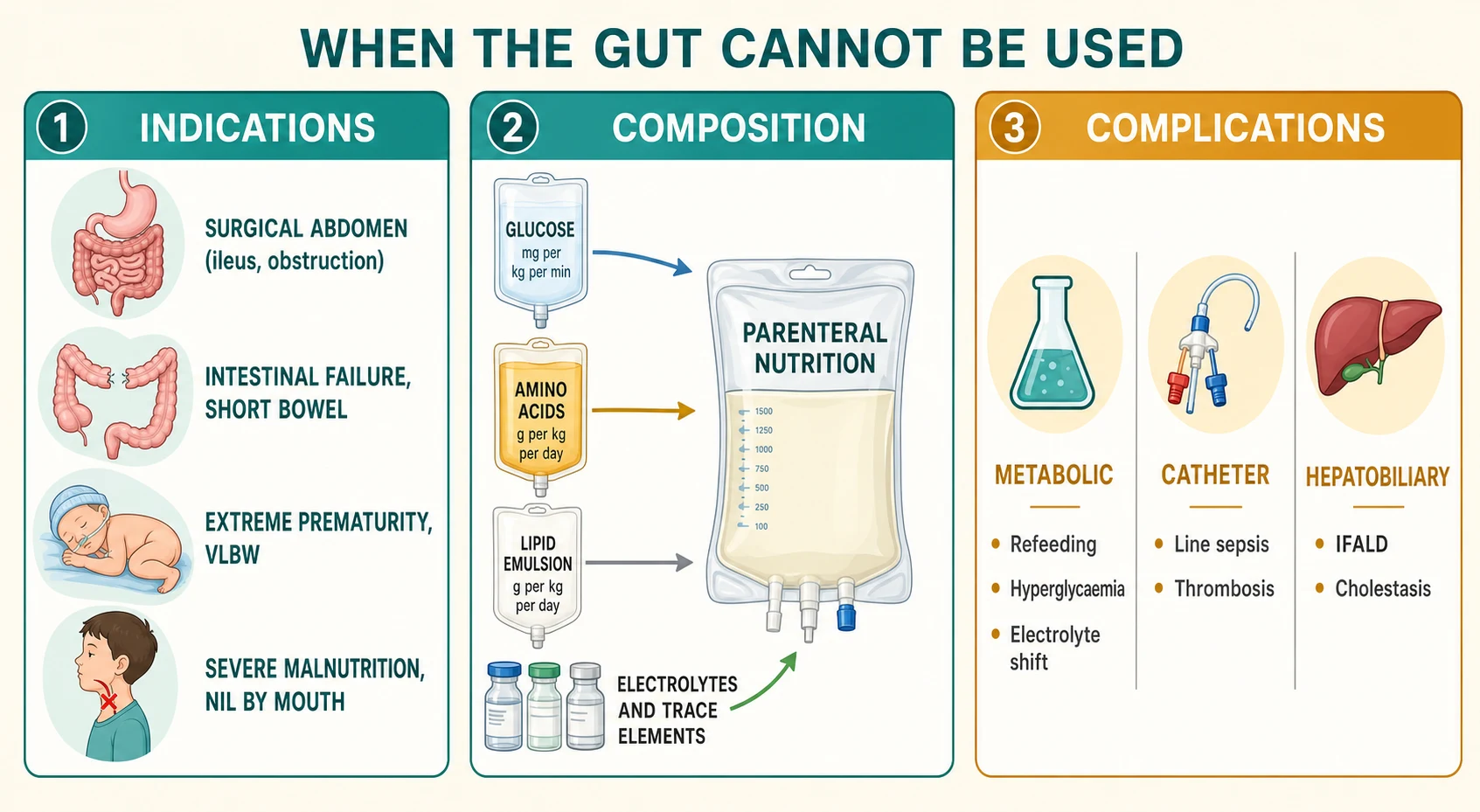
The composition of the bag sorts into four parenteral streams that the candidate must be able to name and dose. Glucose provides the bulk of the energy and is prescribed as a glucose infusion rate in milligrams per kilogram per minute. Amino acids supply the nitrogen for protein synthesis and growth. Lipid emulsion supplies dense calories and essential fatty acids. Electrolytes, vitamins and trace elements complete the bag, each with its own monitoring requirement. Knowing these four streams turns a blank bag order into a reasoned prescription. [1] [4]
A practical axis classifies parenteral nutrition by duration. Short-term parenteral nutrition, for days to a week, supports the child through an acute gut insult such as a postoperative ileus. Medium-term support, over weeks, carries the infant through an adapting short bowel. Long-term or home parenteral nutrition, running for months to years, sustains the child with irreversible intestinal failure and is a technology-dependent state with its own infrastructure of central access, home pumps and family training. The duration changes the complications you watch for, because the liver, the line and the psyche all pay a toll over time. [3] [12]
Glucose stream
- Bulk of the energy, prescribed as a glucose infusion rate in mg per kg per min
- Term infants oxidise up to about 11 to 12 mg per kg per min
- Excess causes hyperglycaemia, osmotic diuresis and hepatic lipogenesis
Amino acid stream
- Nitrogen substrate for protein synthesis and growth
- Infants advance to around 3 to 3.5 g per kg per day
- Preterm infants may need the higher end from early life
Lipid stream
- Dense calories and essential fatty acids
- Typically advanced to around 3 g per kg per day
- The stream most linked to intestinal failure-associated liver disease
Electrolytes and micronutrients
- Sodium, potassium, calcium, phosphate and magnesium
- Trace elements including zinc, copper and selenium
- Fat-soluble and water-soluble vitamins
Finally, classify the complications into three families, because this is how the examiner frames the danger. Metabolic complications include refeeding syndrome, hyperglycaemia and the electrolyte shifts of the bag itself. Catheter complications are central-line bloodstream infection and venous thrombosis. Hepatobiliary complications are intestinal failure-associated liver disease and biliary sludge. Sorting the complication by family tells you where to look and what to do. [3] [8]
Epidemiology & Risk Factors
Parenteral nutrition is common in modern paediatric practice because neonatal intensive care, complex surgery and the survival of fragile infants have all expanded the population that depends on the vein. Premature and very-low-birth-weight infants are the single largest group, because their immature guts tolerate little milk and their immature livers are exquisitely sensitive to cholestasis. Children with surgical short bowel, oncology patients after gut-toxic chemotherapy, and those with severe acute malnutrition make up much of the remainder. [3] [11]
The risk factors for refeeding syndrome describe the starved child, and they are the key to recognising who needs a cautious start. The ASPEN consensus names the central ones: a negligible intake for more than five days, evidence of malnutrition or rapid weight loss, a low body mass index, and pre-existing low phosphate, potassium or magnesium. In children specifically, the chronically undernourished, the child with anorexia nervosa, the child with cancer or a long intensive-care stay, and the child who has fasted preoperatively for longer than expected all carry real risk. The point is that risk is common and easily missed, because the child does not look refeedable until you start to feed. [5] [6]
The risk factors for intestinal failure-associated liver disease cluster in the premature infant on a sustained lipid load. Prematurity and low birth weight head the list, followed by the duration and dose of parenteral lipid, recurrent sepsis, the absence of enteral feeding, and the phytosterols carried in some soybean-based emulsions. Wang and colleagues showed that in very-low-birth-weight infants the duration of parenteral nutrition and the lipid load are among the strongest predictors of cholestasis. Knowing these factors lets you target prevention at the child who needs it most. [8] [11]
The epidemiology of catheter-related bloodstream infection follows the central line wherever it goes. Every child with a long-term central venous catheter for parenteral nutrition is at risk, and the risk rises with the number of lumens, the duration of use, the handling of the line, and the frequency of bloodstream infections in the unit. Sepsis prevention is therefore inseparable from nutrition safety, because a single line infection both threatens the child and worsens the cholestasis that threatens the liver. [3] [8]
Pathophysiology
The reason refeeding syndrome exists lies in the biochemistry of starvation and refeeding, and understanding it makes the prevention obvious. In starvation the body runs on fat and ketones, insulin stays low, and the intracellular stores of phosphate, potassium and magnesium are depleted even though the serum levels may look normal. When carbohydrate reappears, insulin surges. The insulin drives phosphate, potassium and magnesium out of the serum and into the cells just as those cells begin to consume them in huge quantities to rebuild adenosine triphosphate and handle the glucose load. The serum levels then plummet. [5] [7]
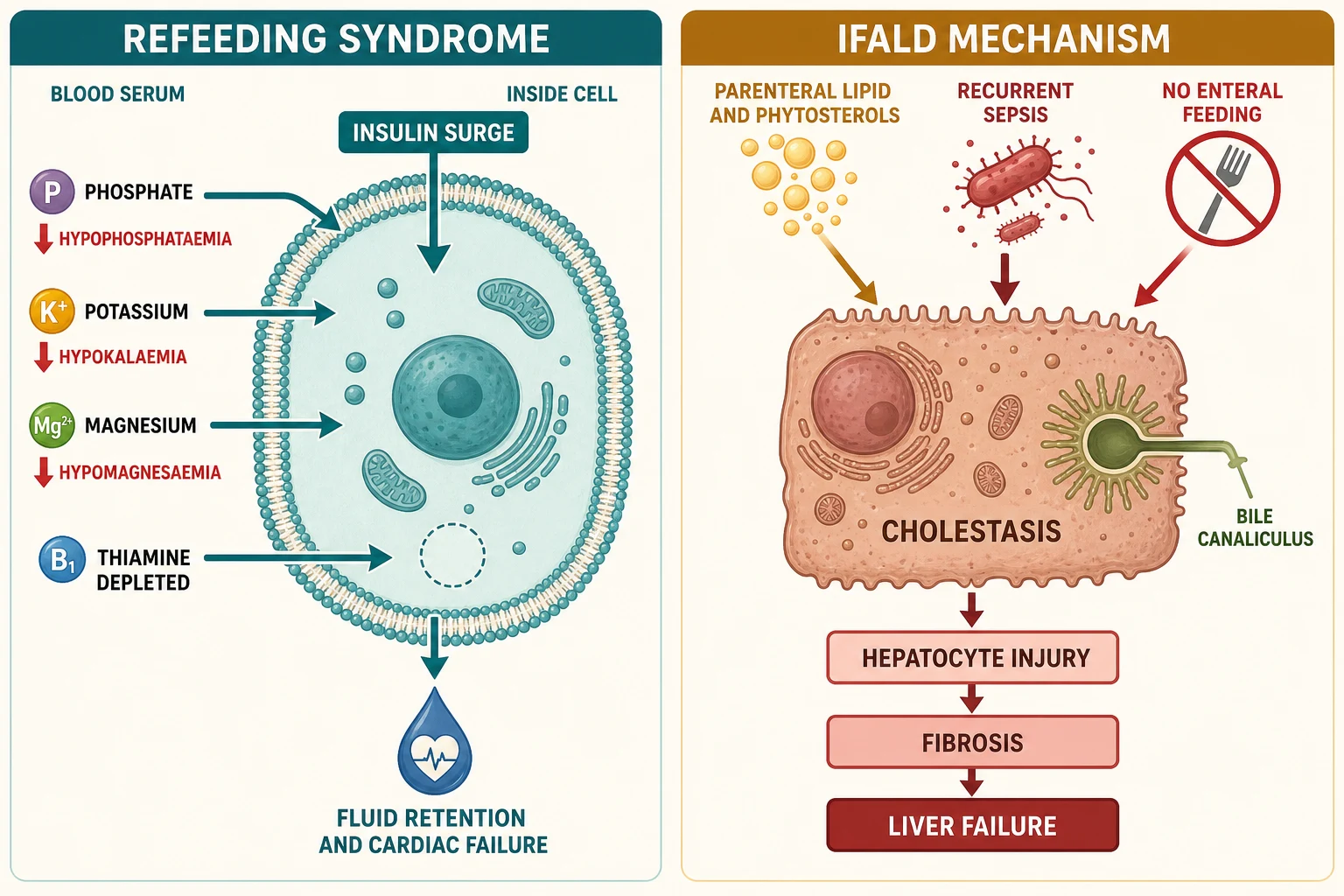
Thiamine depletion is the second half of the refeeding mechanism, and it is the one most often forgotten. Thiamine is a cofactor for the enzymes that metabolise carbohydrate, so a starved body with exhausted thiamine stores cannot handle the sudden glucose load. The result is functional thiamine deficiency, which contributes to cardiac failure, confusion and the lactic acidosis of refeeding. This is why thiamine is given before the first feed, not after the phosphate has fallen. [5] [7]
The third mechanism is fluid and sodium retention. Insulin retains sodium at the kidney, the renin-angiotensin-aldosterone system is reactivated by refeeding, and the starved heart with its wasted myocardium cannot handle the extra volume. A child who is rapidly rehydrated and refed can therefore tip into acute cardiac failure from fluid overload before the electrolyte shifts have even been documented. The principle is that refeeding is a low-and-slow process, never a rapid one. [6]
The pathogenesis of intestinal failure-associated liver disease weaves together several insults that the bedside team can modify. The load of parenteral lipid is central: a sustained high lipid dose, together with the phytosterols carried in some soybean-based emulsions, injures the hepatocyte and impairs bile flow. Recurrent sepsis, common because of the long-term central line, multiplies the cholestatic injury. The absence of enteral feeding removes the normal trophic and prokinetic stimulus to bile flow. The result is cholestasis that, if unchecked, progresses to fibrosis, portal hypertension and liver failure. The encouraging news is that each of these drivers is modifiable. [8] [9]
The glucose stream carries its own pathophysiology when it is pushed too fast. When the glucose infusion rate exceeds the maximal oxidative capacity of the child, the excess carbon cannot be burned and is converted to fat in the liver. This hepatic lipogenesis causes steatosis, raises the carbon dioxide load on the lungs, and produces osmotic diuresis from hyperglycaemia that dehydrates the child the bag is meant to nourish. Matching the glucose infusion rate to the childs tolerance is the daily art of the prescription. [1] [3]
Clinical Presentation
The child who needs parenteral nutrition usually presents with the problem that took the gut out of service, not with a nutrition complaint. A premature infant who cannot tolerate milk, a neonate after bowel surgery, a child with severe mucositis from chemotherapy, or a malnourished adolescent admitted for refeeding are the typical faces of this topic. The parenteral line is the response to their primary illness, and the task is to sustain them without adding the complications of the therapy. [3]
Refeeding syndrome declares itself in the days after nutrition restarts, and the alert clinician watches for it actively. Within the first 72 hours the phosphate, potassium and magnesium fall, and the child develops weakness, irritability, paraesthesia or, in the severest cases, respiratory failure, seizures and arrhythmia. Fluid retention produces oedema, a rising heart rate and, in the worst cases, frank cardiac failure. The trap is that these signs are easy to attribute to the underlying illness unless the refeeding clock is running in your mind. [5] [7]
Intestinal failure-associated liver disease declares itself in the bloods before it declares itself at the bedside. The first sign is a rising conjugated bilirubin in an infant on parenteral nutrition, followed by raised gamma-glutamyl transferase and alkaline phosphatase. Clinically the child may become jaundiced, with hepatomegaly and, as disease advances, pruritus and splenomegaly from portal hypertension. Because the cholestasis of a sick premature baby has many causes, the key clinical act is to measure the conjugated bilirubin serially and act on a rising trend early. [8] [9]
The child with catheter-related bloodstream infection presents in the way every febrile child with a central line presents, and the cardinal rule is not to wait. Fever, or sometimes instability without fever in the smallest infant, in a child with a central venous catheter is a line infection until blood cultures prove otherwise. The presentation ranges from a well-looking child with a temperature to a child in septic shock, and the seriousness is what makes a low threshold for culturing and treating so important. [3]
The metabolic presentation to hold in mind is the child who becomes hyperglycaemic on a bag pushed too hard. The glucose spills into the urine, drawing water with it, the child becomes dehydrated despite the infusion, and an osmotic diuresis can tip a small infant into intraventricular haemorrhage or electrolyte chaos. Slowing the glucose infusion rate and treating the hyperglycaemia, rather than simply adding insulin, is the safer first response. [1]
Differential Diagnosis
When an infant on parenteral nutrition becomes cholestatic, you must first decide whether the cholestasis is the parenteral nutrition itself or something else, because a missed biliary atresia is a catastrophic error. The picture of pale stools and a raised conjugated bilirubin could be biliary atresia, alpha-1-antitrypsin deficiency, a metabolic liver disease, or a congenital infection, any of which needs its own urgent work-up. The rule is that any infant with conjugated jaundice has biliary atresia actively excluded by ultrasound, liver biopsy and, if doubt remains, intraoperative cholangiogram, in parallel with managing the suspected intestinal failure-associated liver disease. [8] [9]
When a refed child develops a low phosphate, refeeding is the leading explanation but not the only one. Sepsis, respiratory alkalosis, renal tubular losses, paracetamol toxicity, diuretic use and refeeding itself can all drop the phosphate. The distinguishing feature is the timing: a phosphate that falls within the first days of reintroducing nutrition in a starved child is refeeding until shown otherwise. The other causes remain on the list, but they do not displace the prevention and treatment of refeeding. [5] [6]
IFALD cholestasis
- Rises in an infant on sustained parenteral lipid
- Driven by lipid load, sepsis and no enteral feeding
- Falls with lipid modification and enteral advance
Biliary atresia
- Pale stools and conjugated jaundice in a term infant
- Triangular cord sign on ultrasound
- Needs urgent cholangiogram, not a nutrition change
Sepsis cholestasis
- Bilirubin rises with a bloodstream infection
- Resolves as the infection is treated
- The line is the usual source
When a child on parenteral nutrition fails to gain weight, the differential runs from an inadequate prescription to ongoing losses, malabsorption, recurrent sepsis, an electrolyte or micronutrient deficit, or simply an error in the bag. Each is found by going back to the measurements: the weight trend, the input and output, the bloods, and the bag itself. The temptation to chase a rare cause before confirming the calorie and electrolyte adequacy of the prescription is the commonest blind alley. [3] [12]
When a child with a central line becomes unstable, the differential is infection, thrombosis, an embolus, an electrolyte derangement, or a metabolic complication of the bag. The disciplined approach is to culture the blood, draw the electrolytes, examine the line and the limb, and treat empirically while the results return, because the cost of waiting on a line infection is far higher than the cost of a day of broad-spectrum cover. [3]
Clinical & Bedside Assessment
The bedside assessment of a child on parenteral nutrition rests on three measurements that tell you more than any single blood test: the daily weight, the fluid balance, and the growth trajectory. Weigh the child daily on the same scale at the same point in the cycle, because the weight reflects fluid balance, calorie adequacy and electrolyte status at once. A child who is not gaining, or who is falling across centiles, has a problem to solve before the ward round ends. [3]
Record the input and output meticulously. Every millilitre of urine, stool, drain and ostomy output is accounted for, because the parenteral prescription must match the losses. A child in positive balance is accumulating fluid toward refeeding overload or cardiac strain, and a child in negative balance is losing more than the bag provides. These numbers convert an impressionistic doing well into a managed variable. [3]
Examine the central line and its exit site every day. Look for redness, discharge or tenderness at the tunnel and exit site, any of which may herald a line infection. Examine the limb for swelling that suggests a venous thrombosis, and check the dressing is intact and clean. A line that is handled by everyone with strict asepsis, and inspected at every opportunity, is the line that survives longest without infection. [3]
Examine the abdomen and the liver. Palpate for hepatosplenomegaly, the stigmata of advancing cholestasis and portal hypertension, and assess the abdomen for distension that might signal a return of ileus, bacterial overgrowth, or an intra-abdominal problem. In the infant, watch the colour of the stool and the skin, because pale stool and yellow skin are the bedside signs that send you to the conjugated bilirubin. [8]
Assess the child for the clinical features of refeeding before it becomes dangerous. In the first week of refeeding, look daily for oedema, a rising heart rate, weakness, irritability and breathlessness, and pair the examination with the daily electrolytes. The child who is being refed is never left to the biochemistry alone; the bedside signs of fluid overload and cardiac strain are the early warning that the calories are climbing too fast. [5] [7]
Investigations
The investigation of a child on parenteral nutrition is a standing panel repeated at defined intervals, because the child is exposed to a therapy that itself causes the complications you monitor for. The routine bloods include a full blood count, urea and electrolytes, magnesium, phosphate and calcium, and a liver panel with a conjugated bilirubin, alanine aminotransferase and gamma-glutamyl transferase. Blood glucose is checked frequently while the glucose infusion rate is being established. These panels are not optional; they are how you catch toxicity before it becomes clinical. [3]
In the child at risk of refeeding, the single most important investigation is the daily electrolyte panel for the first week. Check phosphate, potassium and magnesium at baseline before feeding starts, then at least daily, and more often if a level is falling. The defining biochemical event is a drop in phosphate within the first 72 hours, and a falling trend must be treated even before it crosses a numerical threshold. Paired with the electrolytes, a baseline and repeat electrocardiogram is wise in the severely malnourished child. [5] [6]
Trace elements and vitamins are checked at longer intervals in the child on long-term parenteral nutrition. Zinc, selenium, copper and manganese, and the fat-soluble vitamins A, D, E and K, accumulate or deplete over weeks to months, and their deficiency or toxicity is silent until it is not. A standing schedule of surveillance prevents the rickets, the night blindness and the marrow failure that long-term deficiency can produce. [3]
Imaging and microbiology are targeted rather than routine. Blood cultures, from the line and a peripheral site, are drawn for any fever in a child with a central line. Abdominal ultrasound looks for biliary sludge and stones, which are common in the child on long-term parenteral nutrition, and for signs of portal hypertension when the liver disease advances. A liver biopsy is reserved for the cholestatic infant in whom biliary atresia or another cause cannot be excluded non-invasively. [8] [9]
Management — Resuscitation
The immediate priority in the child who will receive parenteral nutrition is to secure safe venous access and to correct the fluid and electrolyte deficits before the first bag runs. A central venous catheter is placed with full aseptic technique, and the smallest number of lumens that will do the job is used, because every lumen is a route for infection. The child who is dehydrated or electrolyte-depleted is resuscitated with isotonic fluid first, and the parenteral nutrition is built up only once the circulation is stable. [3]
In the child at risk of refeeding, resuscitation actually means restraint. The instinct to rapidly rehydrate and refuel a starved child is exactly the instinct that causes refeeding syndrome, so the resuscitation is deliberately gentle. Correct any severe phosphate, potassium or magnesium deficit before feeding begins, give thiamine before the first calorie, restrict the sodium and fluid, and only then start nutrition at a low level. The starved child is resuscitated slowly, because the starved heart cannot tolerate a rapid load. [5] [6]
Catheter-related bloodstream infection is the commonest acute threat, and preventing it begins at the moment the line goes in. Strict aseptic line care by everyone, a single lumen dedicated to the parenteral nutrition, and a low threshold for culturing and treating fever are the cornerstones. When infection recurs, ethanol or taurolidine line locks are added to suppress intraluminal organisms, and a tunnelled or infected line is removed and replaced rather than salvaged at the cost of recurring sepsis. [3] [8]
The metabolic emergencies that arise on parenteral nutrition are handled by adjusting the bag rather than fighting the body. Severe hyperglycaemia is met by lowering the glucose infusion rate before reaching for insulin, because insulin can worsen the intracellular phosphate shift. A falling phosphate, potassium or magnesium during refeeding is corrected with intravenous replacement, and the rate of calorie escalation is slowed or paused. The bag is a dynamic prescription, adjusted every day to what the child actually needs. [1] [5]
Management — Definitive & Stepwise
Definitive management is the daily craft of building and adjusting the parenteral nutrition prescription, and the guiding aim is always the same: to deliver enough energy, nitrogen and micronutrients for growth, while protecting the liver, the line and the starved metabolism. Every decision in this section serves one of those aims. The team of nutrition, pharmacy, nursing and the treating unit works together, because the prescription is too complex for one person to hold alone. [3]
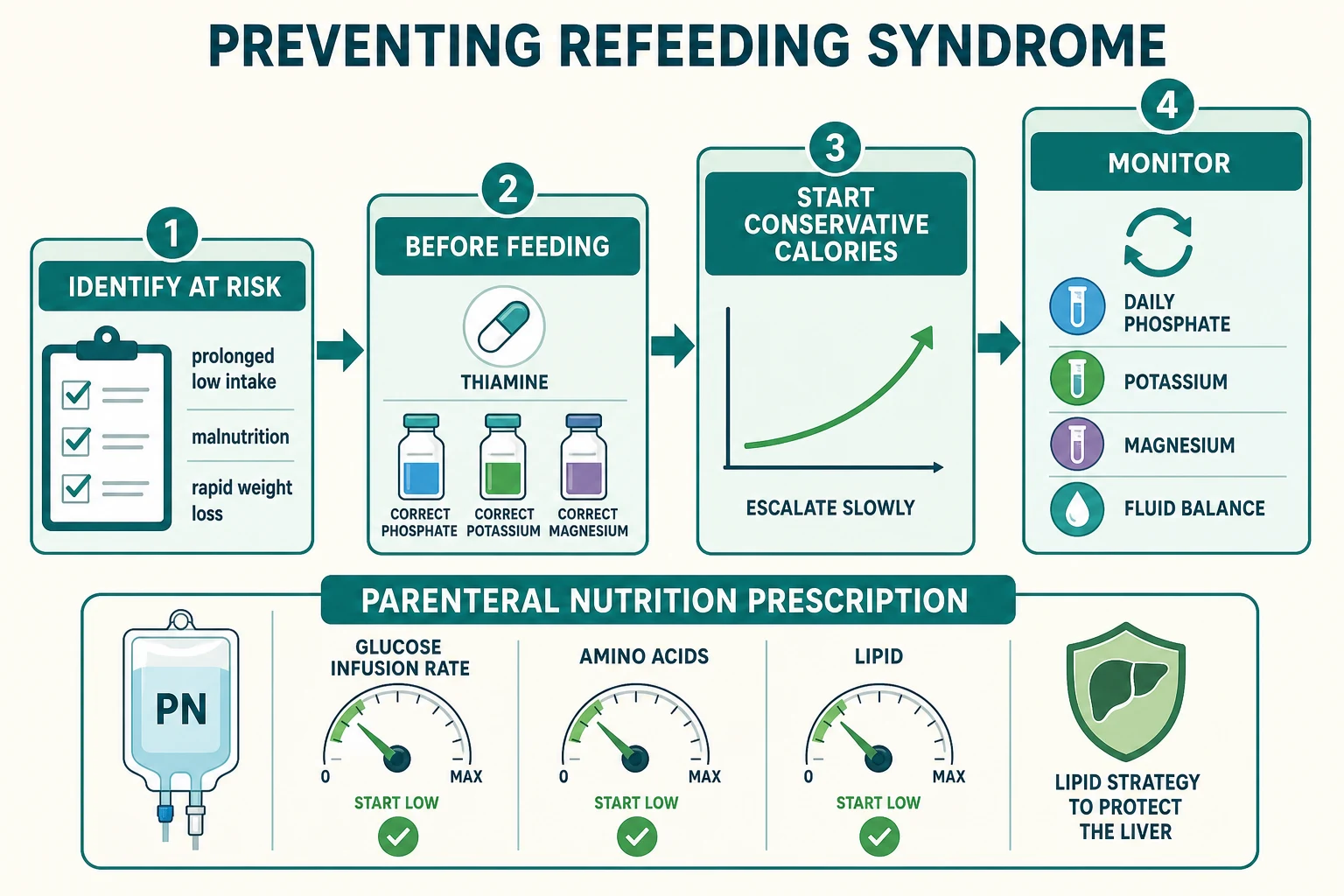
Build the prescription stream by stream. Set the glucose infusion rate first, advancing it gradually to meet the energy target while monitoring the blood glucose, because the term infant oxidises glucose up to about 11 to 12 mg per kg per min and excess beyond that spills into lipogenesis. Add the amino acids, advancing in infants to around 3 to 3.5 g per kg per day for nitrogen and growth. Add the lipid, advancing to around 3 g per kg per day but keeping it lower in the infant at risk of cholestasis. Complete the bag with electrolytes, vitamins and trace elements tailored to the bloods and the losses. [1] [4]
Assess risk
Identify the child at risk of refeeding or IFALD before the first calorie: starvation, malnutrition, prematurity, sustained lipid
Prepare
Give thiamine, correct phosphate, potassium and magnesium, secure a single-lumen central line under full asepsis
Start low
Begin nutrition at a low level, conservative calories in the refed child, glucose infusion rate advanced slowly with blood glucose checks
Build and balance
Advance glucose, amino acids and lipid to target, match fluid and electrolytes to measured losses and daily bloods
Protect and wean
Prevent IFALD with a lipid strategy and enteral advance, protect the line, and wean parenteral nutrition as the gut takes over
The energy target is lower than the enteral target because every parenteral calorie is absorbed. For a growing infant the aim is commonly around 90 to 120 kcal per kg per day, met gradually from glucose and lipid, with the nitrogen running alongside. Pushing to the full target on day one is the error that causes hyperglycaemia, fluid overload and, in the starved child, refeeding syndrome. The target is approached over days, paced by tolerance and the bloods. [1]
Parenteral lipid (for IFALD prevention)
Dose
Restrict to around 1 g per kg per day
The lipid strategy is the cornerstone of preventing and treating intestinal failure-associated liver disease, and it works because the lipid is the most modifiable driver of the cholestasis. The approach is to reduce or modify the lipid, using lipid restriction to around 1 g per kg per day in the at-risk infant, a mixed emulsion such as SMOFlipid, or an omega-3 fish-oil-based emulsion, while controlling line infection and advancing enteral feeding. The shared aim is to lower the phytosterol load and the total cholestatic burden. [2] [8]
The preferred lipid emulsion to prevent and treat intestinal failure-associated liver disease differs by region. In North America the omega-3 fish-oil emulsion Omegaven has been widely adopted, often with lipid restriction, reflecting the evidence that fish-oil-based emulsions reverse cholestasis in many infants. In Europe and Australasia mixed emulsions such as SMOFlipid, and lipid-sparing regimens that keep the soy load down, are more commonly used. The shared aim is to lower the phytosterol load and the total cholestatic burden; the preferred emulsion is the regional variation. [2] [8]
Enteral feeding is advanced in parallel at every opportunity, because the gut is the route the liver and the line both prefer. Trophic feeding, even in tiny volumes that contribute little to the calorie count, stimulates bile flow, protects the mucosa, and signals the start of weaning. The trigger to advance enteral feeding is stable output and rising weight, and the trigger to hold is a rising output or falling weight. Every child on parenteral nutrition carries a weaning plan, because the line is a bridge, not a destination. [3] [12]
Specific Subtypes & Scenarios
The malnourished adolescent with anorexia nervosa is the classic refeeding scenario, and it is the one most likely to appear in a written paper. The starved body has depleted its intracellular phosphate, potassium and magnesium and its thiamine, so the moment nutrition restarts the serum electrolytes collapse. The management is to identify the risk, give thiamine, correct the electrolytes, start at a conservative intake around 10 to 20 kcal per kg per day in the high-risk adolescent, and escalate slowly over several days while checking the electrolytes daily. The discipline of the slow start is what keeps these children safe. [5] [6]
The premature infant on long-term parenteral nutrition is the classic intestinal failure-associated liver disease scenario. The immature liver is exquisitely sensitive to the cholestatic injury of sustained lipid and recurrent sepsis, so the conjugated bilirubin begins to rise after weeks of the bag. The management is a lipid strategy, strict infection control, advancing trophic enteral feeding, and the vigilant exclusion of biliary atresia. The principle is that cholestasis caught early is reversible, and cholestasis missed is the road to liver failure. [9] [11]
The child with a surgical short bowel on home parenteral nutrition is the technology-dependent scenario, and it sits at the junction of this topic and the short-bowel leaf. The prescription must sustain growth over months to years, the central line must be protected from recurrent infection, the lipid must be managed to spare the liver, and the enteral route must be advanced to drive adaptation and weaning. The disposition is toward a specialist intestinal rehabilitation centre, because concentrated expertise keeps these children alive and moving toward enteral autonomy. [12]
The critically ill child in the paediatric intensive care unit who needs short-term parenteral nutrition is the scenario most trainees meet. The gut is resting after surgery or severe illness, the line is already in, and the bag is built to bridge the days until feeding restarts. The principles are the same: assess refeeding risk in the chronically starved child, build the bag to tolerance, protect the line, and wean to enteral as soon as the gut recovers. The short duration lowers the risk of liver disease but does not abolish the risk of metabolic and catheter complications. [3]
Complications & Pitfalls
The complications of parenteral nutrition fall into the three families named earlier, and an examiner expects all three. The metabolic complications are refeeding syndrome, hyperglycaemia, the electrolyte shifts of the bag, and the trace-element deficiencies and toxicities of long-term use. The catheter complications are central-line bloodstream infection and venous thrombosis. The hepatobiliary complications are intestinal failure-associated liver disease and biliary sludge and stones. Naming the family of a new complication tells you where to look and what to do. [3] [8]
Refeeding syndrome deserves its own scrutiny as the complication that is entirely preventable. Its drivers are a starved body fed too fast, without thiamine, without electrolyte correction, and without daily monitoring. The prevention is therefore the mirror image: identify the at-risk child, give thiamine, correct the phosphate, potassium and magnesium, start at conservative calories, and check the electrolytes daily for the first week. The pitfall is treating refeeding as a rare event and skipping the slow start, because the starved child is common and the slow start is the whole point. [5] [6]
Intestinal failure-associated liver disease is the complication most likely to end the race in the long-term infant. Its two dominant modifiable drivers are the parenteral lipid load and recurrent sepsis, and the prevention is the lipid strategy and the line-care strategy already described. The encouraging news is that early cholestasis is reversible with lipid modification, infection control and enteral advance, which is why a rising conjugated bilirubin is acted on early rather than observed. [8] [9]
PNBAG
The classic management pitfalls recur and are worth naming. Starting a starved child at full calories causes refeeding syndrome. Pushing the glucose infusion rate too fast causes hyperglycaemia and lipogenesis. Carrying a lipid load too high for too long drives cholestasis. Leaving an infected central line in place too long perpetuates sepsis. And failing to advance enteral feeding or to write a weaning plan normalises dependence and delays the move to the gut. Each is avoidable with a clear, paced plan. [3]
The psychosocial complications are real and under-recognised. The family of a child on home parenteral nutrition carries an enormous burden of line care, night-time infusions, repeated admissions and constant vigilance, and the child is at risk of feeding aversion, developmental delay and disrupted schooling. Acknowledging this burden, connecting the family to peer support and home-care services, and protecting the childs oral feeding and development are part of the management, not an optional extra. [3] [12]
Prognosis & Disposition
The prognosis of a child on parenteral nutrition is governed by the underlying diagnosis and by how well the complications are prevented. A child who needs short-term support for a postoperative ileus weans as the gut recovers and does well. A child with a short bowel that adapts reaches enteral autonomy over months to years. A child with irreversible intestinal failure and uncontrolled cholestasis faces a far harder course and may need a liver or intestinal transplant. The prognosis is not a single number; it is a function of the gut, the liver and the line. [3] [12]
The prognosis of refeeding syndrome is excellent when it is prevented or caught early, and it can be fatal when it is ignored. A child whose phosphate, potassium and magnesium are corrected and monitored, who receives thiamine and a slow calorie escalation, recovers without sequelae. A child who is refed rapidly without monitoring can die of arrhythmia or cardiac failure. The difference is entirely in the prevention, which is why refeeding risk is assessed before the first calorie. [5] [7]
The prognosis of intestinal failure-associated liver disease is favourable when the cholestasis is caught early and the lipid and sepsis drivers are modified. Many infants see their conjugated bilirubin fall with a lipid strategy, infection control and enteral advance, and the cholestasis resolves as the child weans toward enteral autonomy. The child whose disease has progressed to fibrosis, portal hypertension or synthetic failure faces a harder course and the question of transplant. The lesson is that the liver is protectable, but only if the conjugated bilirubin is watched and acted on. [8] [10]
Disposition is governed by the principle that complex and long-term parenteral nutrition does best in a specialist centre. A child with new intestinal failure is referred to a specialist nutrition or intestinal rehabilitation service for assessment, while the local team continues supportive care. For the child established on home parenteral nutrition, the safety-net is a clear escalation plan: families know when to present, the local hospital has a protocol for the febrile central-line child, and retrieval is arranged early rather than late. [3] [12]
Special Populations
The extremely preterm neonate is the population in whom every complication of parenteral nutrition is amplified. The immature liver is exquisitely sensitive to the cholestatic injury of sustained lipid and sepsis, so intestinal failure-associated liver disease develops faster and more severely than in the older child. The immature gut tolerates little milk and needs cautious advancement, and the immature kidney struggles with the sodium and water shifts of the bag. Management is therefore more conservative and more intensive at once: a liver-protective lipid strategy, tighter infection control, and a lower threshold for specialist referral. [9] [11]
The child who is technology-dependent on home parenteral nutrition in a rural or remote community faces a genuine equity gap. The expertise, the lipid preparations and the home-care support cluster in tertiary centres, often far from where the child lives. Telehealth, shared-care partnerships with regional hospitals, funded travel and accommodation, and home-care nursing support are the mechanisms that narrow this gap. A childs postcode should not decide whether they receive safe parenteral nutrition. [3]
The malnourished adolescent, whether from anorexia nervosa, chronic illness, food insecurity or neglect, is the refeeding population at the sharpest risk. The combination of a starved body, a wasted myocardium and a long fast means that the refeeding insulin surge can precipitate cardiac failure within days. These young people need structured refeeding with thiamine, conservative starting calories, daily electrolytes and psychological support, and the medical and the mental-health needs are managed together. [5] [6]
The migrant, refugee or socioeconomically disadvantaged child may arrive malnourished after a period of food insecurity, and carries the same refeeding risk as any starved child. The additional needs are language-appropriate education, attention to micronutrient deficiencies acquired before presentation, and a discharge plan that does not return the child to the conditions that caused the starvation. Failing to address the social context sends a child home to re-starve. [5]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric parenteral nutrition rests on the ESPGHAN, ESPEN, ESPR and CSPEN guideline series published in 2018. The energy guideline sets the calorie targets and the glucose infusion rate principles, the amino acid guideline sets the nitrogen targets, the lipid guideline sets the lipid and essential fatty acid strategy, and the umbrella guideline frames the safe use of the bag. Together these four references carry the framework an examiner expects, and a candidate should know them by topic if not by PMID. [1] [3] [4]
The refeeding syndrome evidence was codified by the 2020 ASPEN consensus recommendations, which set out the risk stratification, the thiamine, the conservative calorie start and the electrolyte monitoring that define modern practice. The Corsello 2023 paediatric narrative review and the Runde 2019 paediatric summary bring the same principles to children specifically, and they are the references to cite for the paediatric refeeding question. The controversy is the exact starting calorie, with protocols ranging from a very low 5 to 10 kcal per kg per day up to 40 to 60 per cent of the target, but the shared principle of a deliberately low and slow start is universal. [5] [6] [7]
The intestinal failure-associated liver disease evidence has moved toward lipid modification as the central preventive and therapeutic tool. The Lee 2020 and Pironi 2019 reviews set out the pathogenesis and the management framework, Fundora 2020 brings the neonatal focus, and Wang 2020 quantifies the risk factors for cholestasis in very-low-birth-weight infants. The Norsa 2023 ESPGHAN position paper places the lipid and weaning strategy in the broader intestinal rehabilitation pathway. The shared conclusion is that the liver is protectable when the lipid load, the sepsis and the enteral route are all managed. [8] [9] [12]
The regional differences cluster around the preferred lipid emulsion and the organisation of home parenteral nutrition. Omega-3 fish-oil emulsions are prominent in North America, while mixed and lipid-sparing strategies are common in Europe and Australasia. The professional guidelines agree on the principles of strict catheter-care standards, the multidisciplinary team, and the early identification and modification of the lipid load, while differing in the preferred emulsion. A candidate who names the principle and acknowledges the regional variation is well placed. [2] [3]
Exam Pearls
The single highest-yield fact in this topic is that refeeding syndrome is prevented, not treated after the fact. Give thiamine, correct the phosphate, potassium and magnesium, start at a conservative calorie level, and check the electrolytes daily for the first week. The hallmark biochemical event is a fall in phosphate within the first 72 hours of restarting nutrition in a starved child. State this clearly and you anchor the refeeding half of the topic. [5] [6]
The composition fact to own is the four parenteral streams and their targets. Glucose is prescribed as a glucose infusion rate, up to about 11 to 12 mg per kg per min in the term infant. Amino acids advance to around 3 to 3.5 g per kg per day. Lipid advances to around 3 g per kg per day, but is restricted to around 1 g per kg per day to protect the liver. The infant energy target is around 90 to 120 kcal per kg per day, lower than the enteral target because every calorie is absorbed. [1] [2]
The liver fact is that a rising conjugated bilirubin in an infant on parenteral nutrition for over two weeks is intestinal failure-associated liver disease until proven otherwise, and the two modifiable drivers are the lipid load and recurrent sepsis. The line fact is that a fever in a child with a central line is a line infection until cultures prove otherwise. [8] [9]
The disposition pearl is that complex and long-term parenteral nutrition does best in a specialist centre, and the weaning pearl is that the gut is always preferred, advanced at every chance, and carried toward enteral autonomy. The prognostic pearl is that refeeding and the early liver disease are both reversible when caught early, which is why the slow start, the daily electrolytes and the serial conjugated bilirubin are not optional. [3] [12]
References
- [1]Joosten K; Embleton N; Yan W; et al ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Energy. Clin Nutr, 2018.PMID 30078715
- [2]Lapillonne A; Fidler Mis N; Goulet O; et al ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Lipids. Clin Nutr, 2018.PMID 30143306
- [3]Mihatsch WA; Braegger C; Bronsky J; et al ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition. Clin Nutr, 2018.PMID 30471662
- [4]van Goudoever JB; Carnielli V; Darmaun D; et al ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Amino acids. Clin Nutr, 2018.PMID 30100107
- [5]da Silva JSV; Seres DS; Sabino K; et al ASPEN Consensus Recommendations for Refeeding Syndrome. Nutr Clin Pract, 2020.PMID 32115791
- [6]Corsello A; Trovato CM; Dipasquale V; et al Refeeding Syndrome in Pediatric Age, An Unknown Disease: A Narrative Review. J Pediatr Gastroenterol Nutr, 2023.PMID 37705405
- [7]Runde J; Sentongo T Refeeding Syndrome. Pediatr Ann, 2019.PMID 31710364
- [8]Lee WS; Chew KS; Ng RT; et al Intestinal failure-associated liver disease (IFALD): insights into pathogenesis and advances in management. Hepatol Int, 2020.PMID 32356227
- [9]Fundora J; Aucott SW Intestinal Failure-Associated Liver Disease in Neonates. Neoreviews, 2020.PMID 32873652
- [10]Pironi L; Sasdelli AS Intestinal Failure-Associated Liver Disease. Clin Liver Dis, 2019.PMID 30947877
- [11]Wang N; Yan W; Hong L; et al Risk factors of parenteral nutrition-associated cholestasis in very-low-birthweight infants. J Paediatr Child Health, 2020.PMID 32100397
- [12]Norsa L; Goulet O; Alberti D; et al Nutrition and Intestinal Rehabilitation of Children With Short Bowel Syndrome: A Position Paper of the ESPGHAN Committee on Nutrition. Part 1: From Intestinal Resection to Home Discharge. J Pediatr Gastroenterol Nutr, 2023.PMID 37256827