Paeds · gastroenterology-hepatology-and-nutrition
Peptic disease and Helicobacter pylori
Also known as Peptic ulcer disease in children · Helicobacter pylori infection · H. pylori gastritis · Duodenal ulcer · Gastric ulcer · Paediatric dyspepsia
A fellowship approach to peptic disease and Helicobacter pylori in children: separate primary H. pylori-associated ulceration from NSAID and stress-related injury and from functional dyspepsia, understand why test-and-treat is rejected in paediatrics, diagnose with endoscopy and biopsy plus susceptibility testing, deliver susceptibility-guided eradication, and confirm cure non-invasively at least four weeks later.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A ten-year-old is referred with three months of gnawing epigastric pain, sometimes waking her at night, and one episode of black stool. Her father had a duodenal ulcer. Before you reach for a breath test or a course of antibiotics, decide what you are actually looking for and how paediatric practice differs from the adult clinic next door. [1] [10]
This page owns the presentation and management logic for peptic disease and H. pylori in childhood. Sister pages carry the deeper algorithms for recurrent and functional abdominal pain, upper gastrointestinal bleeding, and gastro-oesophageal reflux disease. [10] [11]
P.E.P.T.I.C.
Overview & Definition
Peptic disease means mucosal injury of the stomach and duodenum driven by acid and pepsin acting on a defence that has been breached. The breach in children comes most often from Helicobacter pylori infection or from drugs and physiological stress, rather than from acid excess alone. A peptic ulcer is a mucosal break that penetrates the muscularis mucosae; a shallower lesion is an erosion or gastritis. [1] [2]
Helicobacter pylori is a spiral, flagellated, gram-negative bacterium that colonises the gastric mucus layer. It is acquired in early childhood, usually by faecal-oral or oral-oral spread within the household, and it persists for decades if untreated. Most infected children never develop an ulcer, which is exactly why indiscriminate testing causes harm. [1] [3]
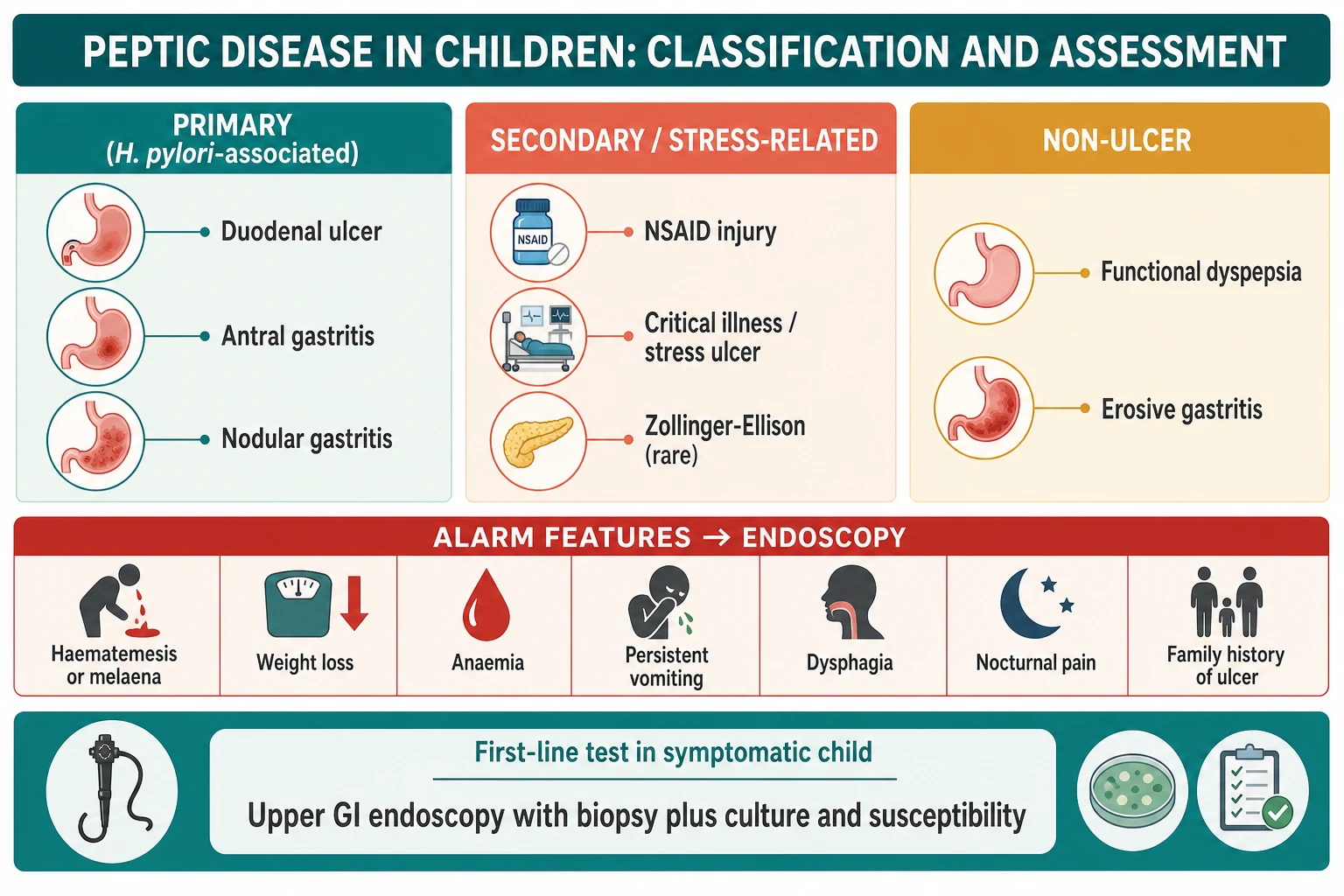
The decisive paediatric distinction is between primary peptic disease, where H. pylori drives antral gastritis and duodenal ulceration, and secondary disease from NSAIDs, critical-illness stress, or a hypersecretory state. A third and larger group of children has functional dyspepsia with normal mucosa, and they must not be mislabelled or given antibiotics. [2] [10]
Classification
Sort peptic disease in a child along two axes: what caused it, and whether it has ulcerated. [1] [2]
Primary, H. pylori-associated disease is the classic pattern: antral-predominant gastritis, often with a nodular ("cobblestone") antrum on endoscopy, and duodenal ulceration in a subset. This is the group in which eradication changes the natural history. [1] [3]
Secondary disease covers NSAID-induced injury, stress-related mucosal damage in critically ill children, and rare hypersecretory states such as Zollinger-Ellison syndrome or systemic mastocytosis. Curling and Cushing ulcers describe stress ulceration after burns and central nervous system injury respectively. [2] [11]
Non-ulcer disease includes erosive and reactive gastritis and, most importantly, functional dyspepsia with normal histology. This last group is the commonest reason a child presents with "ulcer-like" pain and is defined by Rome symptom criteria, not by endoscopy. [10]
Epidemiology & Risk Factors
Helicobacter pylori prevalence in children tracks socioeconomic conditions closely. Rates are low in high-income settings and much higher where crowding, shared bedrooms, and limited sanitation are common. Infection is usually acquired before the age of five, and household transmission from an infected mother or sibling is the dominant route. [1] [3]
Prevalence is falling in many high-income countries as living conditions improve, and endoscopy series show a declining proportion of infected children over recent decades. Even so, migrant, refugee, and Indigenous children, and those living with socioeconomic disadvantage, carry a disproportionately higher burden. [3] [4]
Risk factors for H. pylori acquisition include household crowding, an infected parent, birth or early childhood in a high-prevalence region, and poor water and sanitation access. Risk factors for secondary peptic disease are quite different: NSAID or corticosteroid use, critical illness, major burns, head injury, and severe systemic disease. [2] [11]
Not every infected child develops disease. The minority who ulcerate tend to carry more virulent strains and host factors that favour mucosal injury, which is why population screening is neither useful nor recommended. [1] [12]
Pathophysiology
An ulcer forms when aggressive factors overwhelm mucosal defence. Helicobacter pylori tips this balance through a set of coordinated tricks. Its flagella drive it through the viscous mucus to the epithelial surface, and its urease enzyme splits urea into ammonia, buffering the acid immediately around the bacterium and letting it survive a hostile stomach. This same urease is what the urea breath test exploits. [1] [12]
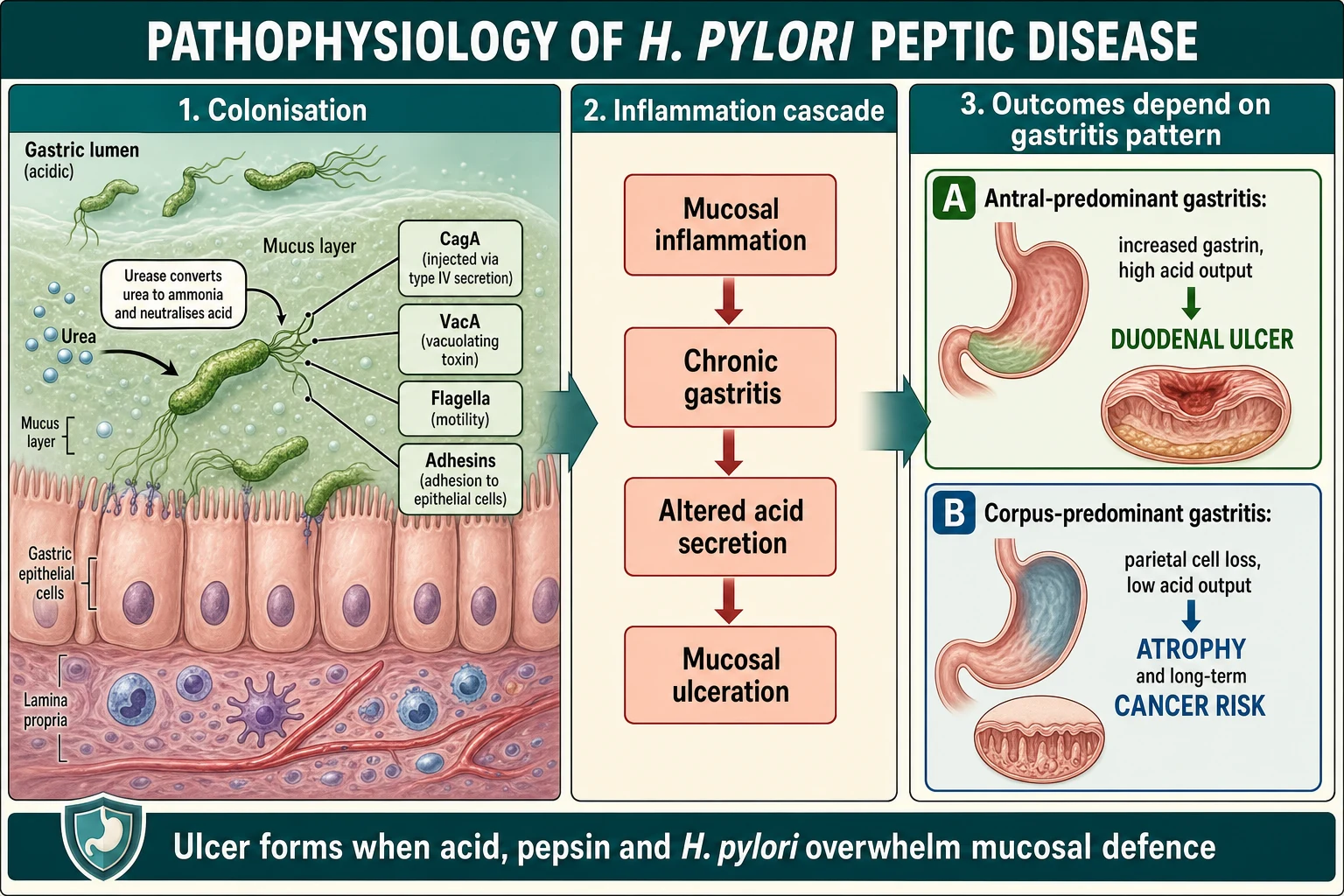
Virulence factors then amplify the damage. The CagA protein, injected into epithelial cells through a type IV secretion system, disrupts cell signalling and drives inflammation, while the VacA vacuolating toxin injures epithelial cells and modulates the immune response. Strains carrying these factors are more strongly associated with ulceration and, over a lifetime, with gastric cancer. [12]
The pattern of gastritis decides the outcome. Antral-predominant gastritis increases gastrin and acid output, delivering more acid to the duodenum and favouring duodenal ulceration. Corpus-predominant or pangastritis instead reduces acid over time and, across decades, predisposes to atrophy, intestinal metaplasia, and cancer. This is why the same organism produces opposite acid states in different hosts. [1] [12]
Secondary disease follows simpler mechanics. NSAIDs inhibit cyclo-oxygenase and strip the mucosa of protective prostaglandins, while critical illness reduces mucosal blood flow and defence. Both leave acid and pepsin free to injure an undefended surface. [2] [11]
Clinical Presentation
The textbook adult picture of burning epigastric pain relieved by food is unreliable in children, and especially so in the young. Symptoms are often vague: epigastric or periumbilical pain, nausea, early satiety, and poor appetite. The younger the child, the less localising the story. [10] [2]
School-age children and adolescents can sometimes describe epigastric pain, nocturnal waking, and a relationship to meals, which raises suspicion of organic peptic disease rather than a functional disorder. A positive family history of ulcer disease adds weight. [1] [10]
Infants and toddlers with peptic disease present non-specifically with irritability, feeding refusal, vomiting, or poor growth, and secondary or stress ulceration dominates this age group. A previously well infant who suddenly bleeds may have a stress ulcer or a drug injury rather than H. pylori disease. [2] [11]
Complicated disease announces itself with bleeding. Haematemesis, coffee-ground vomiting, or melaena signals an eroded vessel, and iron-deficiency anaemia may be the only clue to chronic slow loss. Perforation causes sudden severe pain with peritonism and is a surgical emergency. [11] [1]
Extra-digestive associations are frequently overstated. The strongest paediatric links are between H. pylori and unexplained iron-deficiency anaemia and, in some children, chronic immune thrombocytopenia, which is why the guidelines say to look for and treat the organism in those specific situations. [1] [2]
Differential Diagnosis
Hold the common mimic and the dangerous cause together at once. [10] [1]
Functional dyspepsia is the single most common alternative and the one most often confused with peptic disease. It is diagnosed positively on Rome symptom criteria in a child without alarm features and with normal investigations, and it does not respond to H. pylori eradication when the organism is an innocent bystander. [10] [2]
Gastro-oesophageal reflux disease produces heartburn, regurgitation, and epigastric discomfort, and can coexist with peptic disease. Eosinophilic oesophagitis causes dysphagia and food impaction, particularly in atopic children, and needs oesophageal biopsies to diagnose. [10]
Other organic causes of epigastric pain include biliary and pancreatic disease, coeliac disease, inflammatory bowel disease, constipation, and, rarely, malignancy. A child with weight loss, anaemia, or nocturnal symptoms deserves an organic work-up rather than reassurance. [10] [11]
Acute severe presentations such as bleeding or perforation broaden the differential to variceal bleeding, Mallory-Weiss tears, vascular malformations, and swallowed foreign bodies or caustics. Endoscopy discriminates most of these. [11]
Clinical & Bedside Assessment
1. Screen for alarm features first. Ask about and look for gastrointestinal bleeding, weight loss or faltering growth, persistent vomiting, dysphagia, nocturnal pain, unexplained anaemia, a family history of peptic ulcer or gastric cancer, and a palpable mass. Any of these shifts the child toward prompt endoscopy. [1] [10]
2. Characterise the pain. Site, timing, relationship to meals, night waking, and duration all help separate organic peptic pain from a functional disorder. Periumbilical pain with normal growth and no alarm features points toward a functional abdominal pain disorder. [10]
3. Take a drug and exposure history. Ask specifically about NSAIDs, aspirin, and corticosteroids, about critical illness or recent burns, and about household members with H. pylori or ulcer disease. Ask about migration from a high-prevalence country. [2] [3]
4. Examine for growth and danger. Plot weight and height. Examine the abdomen for epigastric tenderness, a mass, and organomegaly. Look for pallor of anaemia and, in the acutely unwell child, for signs of bleeding or peritonism. A normal examination is common and does not exclude an ulcer. [10] [11]
5. Assess the bleeding child rapidly. In a child with haematemesis or melaena, the first job is haemodynamic assessment and resuscitation, not diagnosis. Heart rate, perfusion, and serial haemoglobin guide urgency. [11]
6. Do not order a breath test to make the diagnosis. In children, non-invasive H. pylori testing has a role only for confirming eradication after treatment, not for the initial diagnosis of disease. Bedside temptation to test-and-treat is the classic paediatric error. [1] [2]
Investigations
Investigations in a symptomatic child should establish whether an ulcer is present, whether H. pylori is responsible, and what the organism is susceptible to. [1] [5]
Upper gastrointestinal endoscopy with biopsy is the diagnostic cornerstone in children with troubling symptoms. Take biopsies from the antrum and corpus for histology and for a rapid urease test, and, crucially, take samples for culture and antibiotic susceptibility testing or molecular resistance testing whenever H. pylori is suspected. Endoscopy also identifies the ulcer, gastritis pattern, and complications directly. [1] [5]
Diagnosing H. pylori at endoscopy requires more than one positive test to be confident. A reliable diagnosis rests on either a positive culture, or positive histology plus a positive rapid urease test, so that a single false-positive does not commit a child to antibiotics. [1] [2]
Non-invasive tests — the urea breath test and the monoclonal stool antigen test — are validated in children but are reserved for confirming eradication after treatment. Serology is not recommended, because antibodies persist after clearance and do not indicate active infection. [1] [6]
Susceptibility testing before treatment is now strongly advised, because it markedly improves eradication compared with empiric regimens. Chan and colleagues showed susceptibility-guided treatment is superior to empiric therapy in children, and Vécsei and colleagues demonstrated the same principle a decade earlier. [5] [6]
Bloods and adjuncts include a full blood count for anaemia, iron studies where indicated, and coeliac serology if the picture fits. A child with unexplained iron-deficiency anaemia and no other cause should be evaluated for H. pylori at endoscopy. [1] [10]
Management — Resuscitation
Most peptic disease is managed electively, but the bleeding or perforated ulcer is a genuine emergency. [11]
In a child with significant upper gastrointestinal bleeding, start with airway, breathing, and circulation. Secure large-bore intravenous access, send a crossmatch and full blood count, and give fluid resuscitation and blood products guided by perfusion and haemoglobin rather than by a single number. Involve senior paediatric and surgical teams early. [11]
An intravenous proton-pump infusion is the standard acid-suppression step for a bleeding peptic ulcer and supports clot stability while endoscopy is arranged. State the intent and route rather than inventing a weight-based dose you cannot source, and follow local protocols for paediatric dosing. [11] [9]
Endoscopy is both diagnostic and therapeutic in the bleeding child, allowing injection, thermal, or clip haemostasis of a visible vessel. Perforation, uncontrolled bleeding, or haemodynamic instability despite resuscitation moves the child to surgery. [11]
Management — Definitive & Stepwise
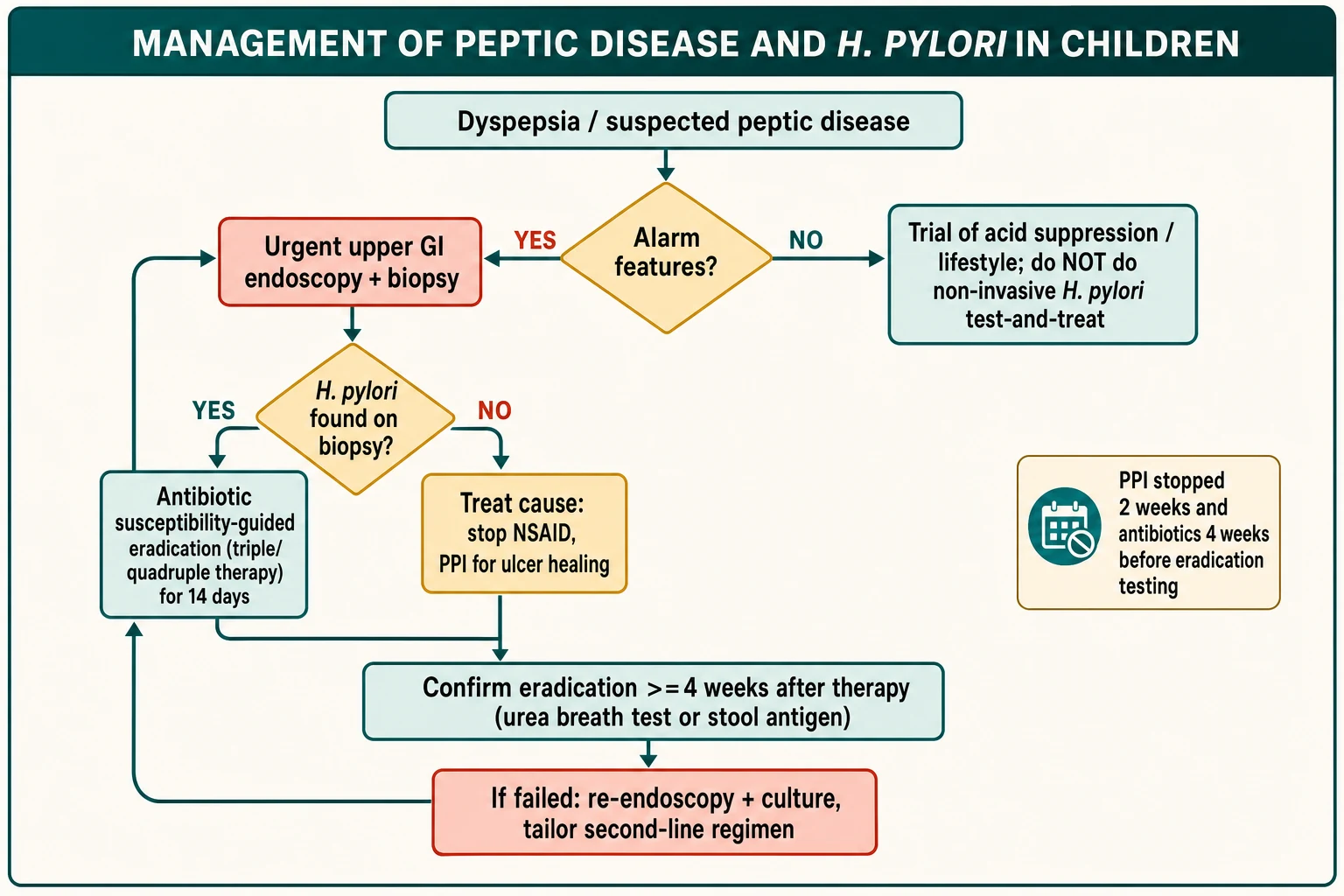
Step 1 — Triage on alarm features. A child with bleeding, weight loss, anaemia, persistent vomiting, dysphagia, or nocturnal pain goes to prompt endoscopy. A child with periumbilical pain, normal growth, and no alarm features is far more likely to have a functional disorder and does not need antibiotics or a breath test. [1] [10]
Step 2 — Diagnose at endoscopy before treating. Confirm the ulcer and confirm H. pylori by culture or by histology plus rapid urease test. Send tissue for susceptibility testing. Do not start eradication on a non-invasive test alone in a child. [1] [5]
Step 3 — Choose eradication by susceptibility. When the organism is found and disease is present, treat with a susceptibility-guided regimen for 14 days, because 7-day courses and empiric clarithromycin regimens fail too often. A common option is a proton-pump inhibitor with amoxicillin and clarithromycin when the strain is clarithromycin-susceptible, and bismuth-based quadruple therapy when resistance is present or unknown. [1] [5]
Triple or bismuth quadruple therapy for 14 days
Dose
Use twice-daily proton-pump inhibitor plus two antibiotics (for example amoxicillin and clarithromycin) tailored to susceptibility; substitute metronidazole or add bismuth when clarithromycin resistance is present. Follow local paediatric weight-based dosing tables and do not use unverified doses.
Step 4 — Support healing and remove the cause. Give a proton-pump inhibitor to heal the ulcer, stop any NSAID or offending drug, and treat contributing conditions. Rogalidou and colleagues stress that paediatric PPI use must be purposeful and time-limited given its own risks. [9] [1]
Step 5 — Confirm eradication. Test for cure with a urea breath test or monoclonal stool antigen test at least four weeks after finishing antibiotics and after stopping the proton-pump inhibitor for two weeks, so that suppressed but living organisms are not missed. [1] [8]
Step 6 — Manage failure deliberately. If eradication fails, repeat endoscopy with culture and susceptibility testing and select a tailored second-line regimen, reinforcing adherence. Empirically cycling antibiotics without susceptibility data is how treatment-resistant infection is created. [5] [7]
Specific Subtypes & Scenarios
Primary H. pylori duodenal ulcer. Confirm at endoscopy, treat with susceptibility-guided eradication for 14 days, heal with a PPI, and confirm cure at four weeks. This is the scenario where treatment changes the natural history. [1] [5]
NSAID-induced peptic disease. Stop the drug, heal with a proton-pump inhibitor, and consider gastroprotection if an NSAID is unavoidable. H. pylori is not the cause here, so eradication is not the primary treatment. [2] [9]
Stress ulceration in critical illness. Curling and Cushing ulcers arise from mucosal ischaemia in burns and neurological injury. Management centres on resuscitation, acid suppression, and treating the underlying illness. [11] [2]
Unexplained iron-deficiency anaemia. When no dietary or other cause is found, evaluate for H. pylori at endoscopy and treat it if present, because eradication can resolve the anaemia. [1] [2]
Chronic immune thrombocytopenia. In selected children, look for and treat H. pylori, as eradication improves platelet counts in a subset. [1]
Incidental H. pylori without disease. A child found to carry H. pylori incidentally, without an ulcer or clear disease, may reasonably be treated after discussion, but the benefit is weaker and the decision is shared with the family. [1] [2]
The child from a high-prevalence background. Migrant, refugee, and Indigenous children have higher infection rates, but the same rule applies — diagnose at endoscopy, do not screen asymptomatically, and treat confirmed disease. [3] [4]
Complications & Pitfalls
- Using a non-invasive test-and-treat strategy in a child, contrary to paediatric guidelines. [1]
- Treating H. pylori found incidentally without an ulcer as if it explained functional pain. [10] [2]
- Prescribing empiric clarithromycin triple therapy without susceptibility data, driving failure and resistance. [5] [7]
- Using a 7-day course when 14 days is needed for reliable eradication. [1]
- Confirming cure too early or while the child is still on a proton-pump inhibitor, producing a false-negative. [1] [8]
- Relying on serology, which cannot distinguish active from past infection. [6]
- Missing a bleeding or perforated ulcer by anchoring on a functional label. [11]
- Prolonged, unmonitored PPI use with its own adverse-effect profile. [9]
Prognosis & Disposition
Successfully eradicated H. pylori duodenal ulcers rarely recur, and eradication changes the long-term trajectory in a way that acid suppression alone does not. Reinfection after childhood eradication is uncommon in low-prevalence settings but more likely where household transmission continues. [1] [3]
Secondary ulcers heal well once the cause is removed and acid suppression is given, and stress ulceration resolves with recovery from the underlying illness. Functional dyspepsia has a good prognosis but a fluctuating course, and its outcome depends on a positive diagnosis and a biopsychosocial explanation rather than repeated invasive testing. [10] [11]
Most children are managed as outpatients through gastroenterology. The bleeding, perforated, or haemodynamically unstable child needs inpatient and often surgical care. Long-term follow-up focuses on confirming cure, monitoring growth, and, in the rare high-risk child, considering the lifetime cancer implications of persistent infection. [11] [12]
Special Populations
Immunocompromised children: infection may be harder to eradicate and drug interactions with immunosuppressants must be checked, so susceptibility-guided, carefully chosen regimens matter most. [5] [1]
Migrant and refugee children: higher prevalence and possible prior antibiotic exposure raise resistance rates, reinforcing the need for culture and susceptibility rather than empiric treatment. [3] [4]
Indigenous children: disproportionately higher infection burden and access barriers require equity-focused, culturally safe care and the same endoscopy-first diagnostic standard. [3] [4]
Children living with socioeconomic disadvantage: crowding and sanitation drive transmission and reinfection, so family-level assessment and support matter alongside the child's treatment. [3] [4]
Evidence, Guidelines & Regional Differences
The 2023 updated joint ESPGHAN and NASPGHAN guidelines are the authoritative paediatric reference, and they set the endoscopy-first, susceptibility-guided, test-and-treat-rejecting framework used throughout this page. [1]
The 2016 update established the same core principles, and the two documents together explain why paediatric practice diverges deliberately from adult test-and-treat. [2]
Chan and Vécsei provide the paediatric evidence that susceptibility-guided treatment outperforms empiric therapy, while Thung and the paediatric resistance meta-analysis by Menbari document why clarithromycin and metronidazole resistance has made empiric regimens unreliable. [5] [6] [7] [4]
The adult Maastricht VI/Florence consensus frames global testing and treatment strategy, including the confirm-cure timing that paediatrics adopts, even though its test-and-treat approach does not transfer to children. [8]
Rogalidou and colleagues summarise the balance of benefit and risk for proton-pump inhibitors in children, a reminder that acid suppression is not free of harm. Işık and colleagues document the falling but unequal prevalence of infection in children over time. [9] [3]
Australian and New Zealand paediatric gastroenterology follows the ESPGHAN and NASPGHAN endoscopy-first framework, with local antibiotic-susceptibility patterns guiding eradication. Care for Aboriginal and Torres Strait Islander, Māori, and Pasifika children must be culturally safe and equity-aware, given a higher infection burden and access barriers. [1] [3]
UK practice aligns with the paediatric ESPGHAN and NASPGHAN guidance, distinct from adult NICE test-and-treat dyspepsia pathways. Endoscopy with biopsy remains the diagnostic route in symptomatic children, with susceptibility-guided eradication. [1] [8]
US paediatric practice follows NASPGHAN, and the ABP content outline includes gastroenterology and peptic disease. Rising clarithromycin resistance drives the shift toward susceptibility-guided and bismuth-based regimens. [2] [7]
Canadian paediatric gastroenterology aligns with the joint guidelines, and the RCPSC competencies anchor gastroenterology and communication in the care of children with peptic disease. [1] [5]
Exam Pearls
- In children, do not use a non-invasive test-and-treat strategy; diagnose peptic disease and H. pylori at endoscopy with biopsy. [1]
- Confirm H. pylori by culture, or by histology plus rapid urease test, before treating. [1]
- Treat confirmed disease with susceptibility-guided eradication for 14 days, not empiric 7-day clarithromycin triple therapy. [5]
- Confirm cure with a urea breath or stool antigen test at least four weeks after antibiotics and two weeks off the PPI. [1] [8]
- Serology cannot distinguish active from past infection and is not recommended. [6]
- Antral-predominant gastritis raises acid and causes duodenal ulcers; corpus gastritis lowers acid and risks long-term atrophy. [12]
- Evaluate unexplained iron-deficiency anaemia and selected chronic ITP for H. pylori. [1]
- Functional dyspepsia is the common mimic; a positive Rome-based diagnosis prevents unnecessary antibiotics. [10]
High-yield anchors
Diagnosing versus confirming cure in H. pylori
References
- [1]Homan M Updated joint ESPGHAN/NASPGHAN guidelines for management of Helicobacter pylori infection in children and adolescents (2023). J Pediatr Gastroenterol Nutr, 2024.PMID 39148213
- [2]Jones NL Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016). J Pediatr Gastroenterol Nutr, 2017.PMID 28541262
- [3]Işık K Temporal trends and correlates of Helicobacter pylori prevalence in children undergoing upper gastrointestinal endoscopy. Eur J Pediatr, 2026.PMID 41954671
- [4]Menbari S Global Profile of Drug Resistance Related to Helicobacter pylori Infection in Children: A Systematic Review and Meta-Analysis. Health Sci Rep, 2025.PMID 40959185
- [5]Chan C Antimicrobial susceptibility-guided treatment is superior to empiric therapy for Helicobacter pylori infection in children. J Pediatr Gastroenterol Nutr, 2025.PMID 40778419
- [6]Vécsei A Helicobacter pylori eradication rates in children upon susceptibility testing based on noninvasive stool polymerase chain reaction versus gastric tissue culture. J Pediatr Gastroenterol Nutr, 2011.PMID 21694538
- [7]Thung I Review article: the global emergence of Helicobacter pylori antibiotic resistance. Aliment Pharmacol Ther, 2016.PMID 26694080
- [8]Malfertheiner P Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut, 2022.PMID 35944925
- [9]Rogalidou M Balancing therapeutic benefits and hidden risks of proton pump inhibitors in pediatric practice: a narrative review and update. Clin Exp Pediatr, 2026.PMID 41736231
- [10]Seetharaman J Recurrent Abdominal Pain in a Child - Evaluation and Management. Indian J Pediatr, 2025.PMID 40148656
- [11]Xu QC Advances in standardized diagnosis and management of pediatric gastrointestinal bleeding. World J Pediatr, 2025.PMID 41045337
- [12]Merola E Helicobacter pylori and Cancer: What's the Link? Clin Exp Gastroenterol, 2026.PMID 41531650