Paeds · gastroenterology-hepatology-and-nutrition
Persistent and chronic diarrhoea
Also known as Persistent and chronic diarrhoea · Persistent diarrhoea in children · Chronic diarrhoea in children · Prolonged diarrhoea · Chronic nonspecific diarrhoea of childhood · Toddler's diarrhoea
Fellowship guide to persistent and chronic diarrhoea in children: the duration definitions that separate it from acute gastroenteritis, the osmotic, secretory, inflammatory and dysmotility mechanisms, the age-based causes from congenital diarrhoea and cow's milk protein allergy in infancy through toddler's diarrhoea to coeliac disease and inflammatory bowel disease in later childhood, the stool-osmotic-gap and fasting test, the coeliac serology and faecal calprotectin workup, and the management priorities of rehydration, nutritional rehabilitation, zinc and cause-specific therapy.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Diarrhoea that will not settle is one of the commonest reasons a child is referred to a paediatrician, and the whole task is to separate the child who is thriving and needs reassurance from the child whose loose stools are the first sign of coeliac disease, inflammatory bowel disease, a food allergy or a congenital enteropathy. The clue that tells them apart is not the stool itself but the company it keeps — the growth, the weight, the blood and the timing. [1]
The starting point is time. Acute gastroenteritis resolves within a week or two; when watery stools continue past fourteen days the episode has become persistent diarrhoea, and when loose stools have run for four weeks or more the problem is chronic diarrhoea. The distinction matters because it changes the differential completely: a child who has had loose stools for three days almost always has a self-limiting infection, whereas a child who has had them for six weeks needs a structured search for an underlying cause. [1] [11]
Classification
The most useful way to hold chronic diarrhoea in mind is to think along three lines at once: how long it has lasted, what the stool looks like, and how old the child is. Each line narrows the differential, and together they usually point to the diagnosis before a single test is sent. The duration line separates the acute episode (under fourteen days) from persistent diarrhoea (fourteen to twenty-nine days) and chronic diarrhoea (four weeks or more). [1]
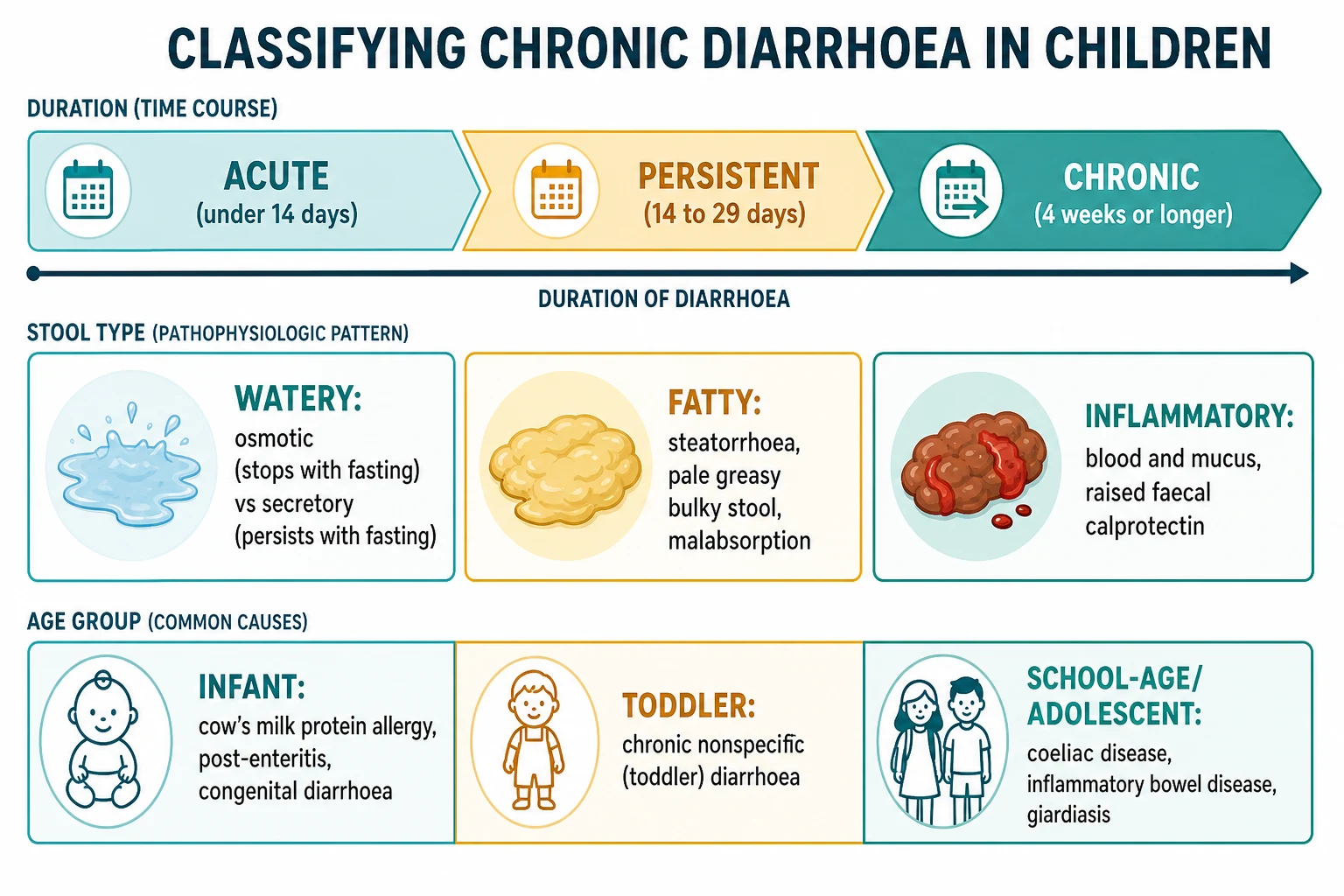
The stool line describes the physiology. A watery stool points to an osmotic or a secretory process; a pale, greasy, bulky, hard-to-flush stool points to fat malabsorption (steatorrhoea); and a stool with blood and mucus points to mucosal inflammation. This pattern is the single most useful piece of information from the history, because it maps directly onto the mechanism and therefore onto the workup. [1] [3]
The age line reorders the differential by likelihood. In the young infant the concerns are cow's milk protein allergy, post-enteritis enteropathy and the rare congenital diarrhoeal disorders; in the toddler the commonest diagnosis by far is chronic nonspecific (toddler's) diarrhoea; and in the school-age child and adolescent the priorities become coeliac disease, inflammatory bowel disease and infections such as giardiasis. [1] [4]
Epidemiology & Risk Factors
The burden of persistent and chronic diarrhoea falls unevenly. In high-resource settings the common causes are toddler's diarrhoea, coeliac disease, cow's milk protein allergy, post-infectious diarrhoea and inflammatory bowel disease, and severe outcomes are uncommon. In low- and middle-income settings persistent diarrhoea is a major cause of childhood death, because it feeds a vicious cycle of malabsorption, weight loss, immune impairment and repeated infection in an already undernourished child. The single most important risk factor for that spiral is pre-existing malnutrition. [9] [11]
A recent prospective cohort of children with prolonged diarrhoea confirmed that a preceding acute infection, young age and disturbance of the gut microbiota are prominent contributors, and that the aetiology is frequently multifactorial rather than a single clean diagnosis. Prior antibiotic exposure, formula feeding, crowding and poor sanitation all raise the risk, and the child who has had a severe or a rotavirus gastroenteritis is at particular risk of a post-enteritis enteropathy with transient carbohydrate malabsorption. [11] [1]
Environmental enteric dysfunction is the chronic, subclinical enteropathy of children living with poor sanitation and repeated enteric infection: a flattened, inflamed small-bowel mucosa with malabsorption that need not produce overt diarrhoea but drives stunting and blunts oral vaccine responses. It is a population-level cause of poor growth in disadvantaged communities, and it links chronic gut injury to the wider problem of childhood undernutrition. [9]
Pathophysiology
Diarrhoea occurs when the balance between the fluid the gut secretes and the fluid it absorbs tips towards the lumen, so that more water leaves the body in the stool than the colon can reclaim. Four mechanisms produce that imbalance, and although they overlap in real disease, keeping them distinct is what makes the workup logical. The first is osmotic: an unabsorbed solute — lactose behind a deficient lactase, or the fructose and sorbitol of excessive fruit juice — holds water osmotically in the lumen, so the diarrhoea appears with feeding and stops with fasting. [3] [5]
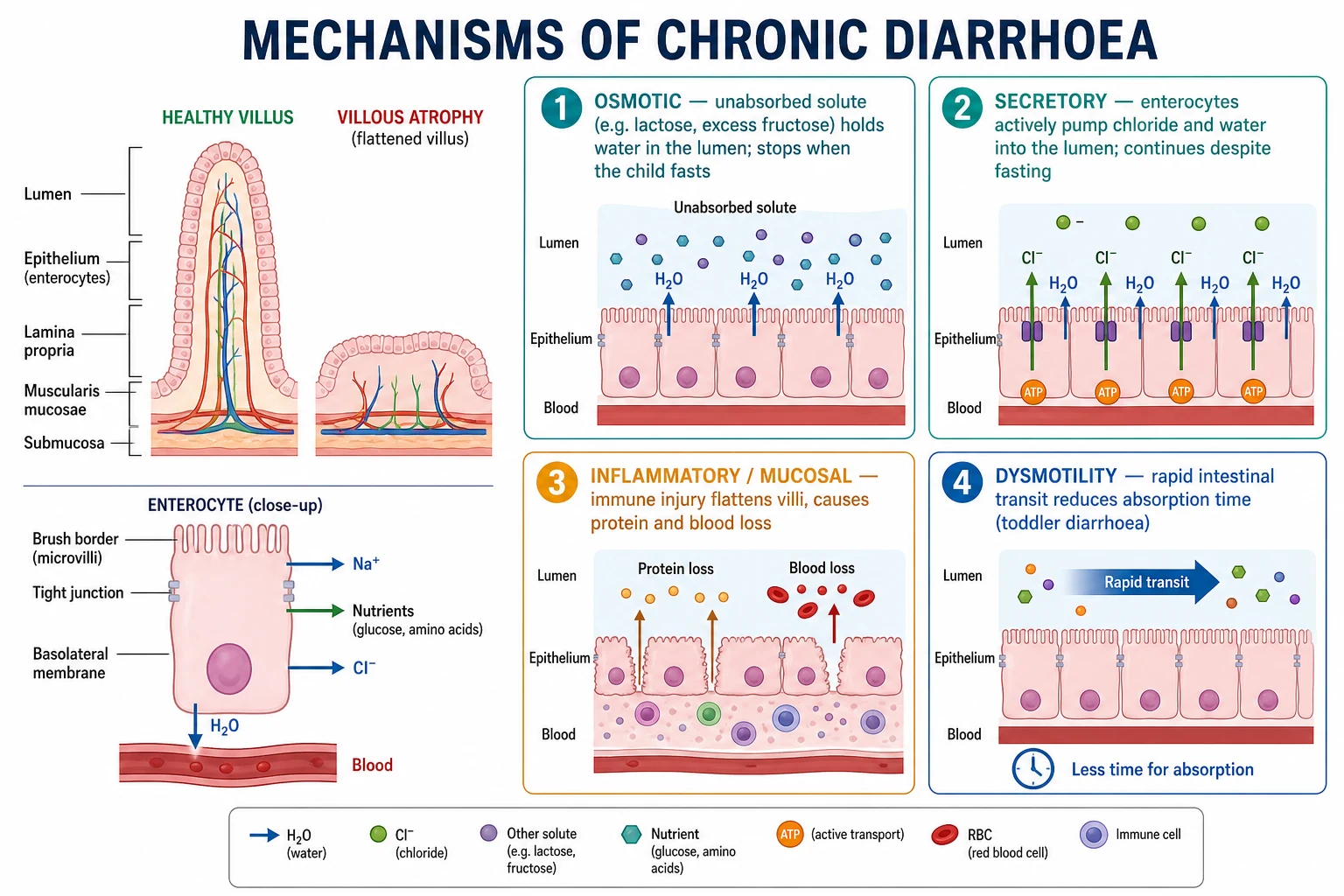
The second mechanism is secretory: the enterocyte actively pumps chloride into the lumen and water follows, driven by a bacterial toxin, a neuroendocrine hormone or a congenital transporter defect. Because the drive is intrinsic to the cell and not dependent on luminal contents, secretory diarrhoea is high-volume, watery, and continues through a fast — the property that separates it from osmotic diarrhoea at the bedside. Field's work on intestinal ion transport established this secretion-versus-absorption model that still frames the physiology. [3] The third mechanism is inflammatory: an immune injury to the mucosa, as in inflammatory bowel disease or allergic colitis, flattens the villi, exudes protein and blood into the lumen, and impairs absorption, producing the bloody, mucoid stool with systemic inflammation. [7] [1]
The fourth mechanism is dysmotility: the gut moves its contents too quickly, giving the enterocyte too little contact time to absorb water and nutrients, which is the physiology of toddler's diarrhoea. Villous atrophy is the shared final pathway of the malabsorptive enteropathies — coeliac disease, cow's milk protein enteropathy, post-enteritis syndrome and the congenital disorders all flatten the absorptive surface, so that the tall, finger-like healthy villus becomes a blunt, atrophic ridge with a reduced brush-border enzyme capacity and secondary carbohydrate malabsorption layered on top of the primary disease. [2] [4]
Clinical Presentation
The presentation that reassures is the thriving toddler. A child between six months and five years passes three to more than ten loose stools a day, often containing recognisable undigested food ("peas and carrots"), the first stool of the day being the largest and the stools becoming looser as the day goes on. Crucially the child is well, active, growing along their centiles and gaining weight, and there is no blood, no pain and no nocturnal diarrhoea. This is chronic nonspecific diarrhoea of childhood — toddler's diarrhoea — and the presentation itself is the diagnosis. [4] [5]
The presentation that worries is the child who is not thriving. Weight loss or a fall across the growth centiles, pallor and lethargy from anaemia, abdominal pain and distension, mouth ulcers, perianal disease, delayed puberty and clubbing all point towards an organic enteropathy. In coeliac disease the classic infant picture is the miserable, wasted toddler with a distended abdomen, wasted buttocks and irritability after weaning onto gluten, though older children more often present with subtler features of anaemia, short stature or fatigue. [6] [1]
The presentation that alarms is the infant with diarrhoea from birth. A congenital diarrhoeal disorder presents in the first days to weeks of life with profuse watery diarrhoea, dehydration, electrolyte derangement and failure to thrive, and the family history or consanguinity may be the clue. In older children, inflammatory bowel disease declares itself with bloody diarrhoea, abdominal pain, weight loss, nocturnal symptoms and extraintestinal features such as arthritis, erythema nodosum or uveitis, often with a striking discrepancy between how unwell the child feels and how well they look. [10] [7]
Differential Diagnosis
The differential is best built by age, because age reorders the probabilities more than any other single factor. In the infant, the leading diagnoses are cow's milk protein allergy (often with blood and mucus in an otherwise well breastfed baby, or with eczema and vomiting), post-enteritis enteropathy with secondary lactose malabsorption, and — rarely but not to be missed — a congenital diarrhoeal disorder presenting from birth. Overfeeding and the osmotic effect of concentrated or excessive feeds also cause loose stools in this age group. [8] [10]
In the toddler, chronic nonspecific diarrhoea dominates the differential and is essentially a clinical diagnosis in a thriving child; the main task is to exclude excessive fruit-juice and fluid intake, which loads the gut with fructose and sorbitol and produces an osmotic diarrhoea that resolves when the juice is stopped. Coeliac disease must remain on the list because it can present at any age after gluten is introduced, and giardiasis is an important, treatable infective mimic. [4] [5]
In the school-age child and adolescent, the priorities shift to coeliac disease, inflammatory bowel disease and chronic infection, with irritable bowel syndrome and functional diarrhoea as common non-organic diagnoses once the red flags are excluded. Across all ages the must-not-miss diagnoses are inflammatory bowel disease (blood, weight loss, inflammation), coeliac disease (a treatable cause of faltering growth), cystic fibrosis with pancreatic insufficiency (steatorrhoea and poor growth), and the congenital enteropathies in the young infant. [7] [6]
Age-based differential for chronic diarrhoea — 'ABCDE by age'
Clinical & Bedside Assessment
Assessment begins and ends with growth. Plot the weight, the height and the head circumference on the growth chart and read the trend, because a child tracking normally along their centiles almost never has a serious organic enteropathy, while a child crossing centiles downward has an organic disease until proven otherwise. Quantify the diarrhoea itself: the number, volume, consistency, colour, the presence of blood, mucus, fat or undigested food, the relationship to feeding and to fasting, and whether it wakes the child at night. This history alone separates most benign from organic disease. [1] [4]
The focused history then hunts for the cause. Ask about the diet in detail — the introduction of gluten, the volume of fruit juice and squash, the formula and its concentration, and any food that triggers symptoms — because the diet is often the diagnosis and always the first thing to modify. Ask about the birth and the onset, the travel and water exposure, the family history of coeliac disease, inflammatory bowel disease or atopy, and the drug history including antibiotics. A three-day stool and food diary quantifies both the diarrhoea and the intake and frequently clinches the diagnosis of a dietary or a functional problem. [5] [1]
Examination looks for the systemic footprint of an enteropathy. Assess hydration and nutrition, look for pallor, clubbing, mouth ulcers, an abdominal mass or tenderness, a distended abdomen with wasted buttocks in coeliac disease, and perianal skin tags, fissures or fistulae in Crohn disease. Inspect the perineum and, where appropriate, examine the stool. Examination of the growth chart and the perineum together often does more than any laboratory test to direct the workup. [7] [6]
Investigations
Investigation is directed by the stool pattern and the growth, not scattered as a screen. In the thriving toddler with a classic history, no tests may be needed at all beyond a review of the diet. When testing is warranted, first-line non-invasive stool studies answer the mechanistic question: stool pH and reducing substances detect carbohydrate malabsorption; the stool osmotic gap distinguishes osmotic from secretory diarrhoea; faecal calprotectin flags mucosal inflammation and helps decide who needs endoscopy; faecal elastase screens for pancreatic insufficiency; and stool microscopy, culture and antigen or molecular testing identify Giardia and other pathogens. [2] [1]
Coeliac disease has its own defined pathway. The ESPGHAN 2020 guideline is built on immunoglobulin A anti-tissue-transglutaminase antibody with a total immunoglobulin A to exclude deficiency, and it permits a no-biopsy diagnosis in a symptomatic child when the anti-transglutaminase titre is at or above ten times the upper limit of normal and endomysial antibody on a separate sample is positive; otherwise duodenal biopsy remains the standard. The serology must be taken while the child is still eating gluten, because a gluten-free diet normalises the antibodies and invalidates the test. [6]
Blood tests support and stage. A full blood count and film may show iron-deficiency anaemia or thrombocytosis; ferritin, folate, vitamin B12 and fat-soluble vitamins assess malabsorption; C-reactive protein, erythrocyte sedimentation rate and albumin gauge inflammation and protein loss; and electrolytes, renal and liver function guide fluid and nutritional therapy. A sweat test diagnoses cystic fibrosis when steatorrhoea and poor growth suggest pancreatic insufficiency. When faecal calprotectin, blood and inflammatory markers point to inflammatory bowel disease, the child proceeds under the revised Porto criteria to ileocolonoscopy with upper endoscopy and biopsies, with small-bowel imaging by magnetic resonance enterography. [7] [2]
Management — Resuscitation
Although most chronic diarrhoea is managed in clinic, a subset of children present acutely unwell and need resuscitation first. The infant with a congenital secretory diarrhoea, the malnourished child with persistent diarrhoea, and the child with a severe flare of inflammatory bowel disease can all arrive dehydrated, hyponatraemic or hypokalaemic and acidotic. Assess the airway, breathing and circulation, quantify the dehydration, and correct the circulating volume and the electrolyte and acid-base derangement before turning to the diagnosis. Restore potassium carefully, because chronic diarrhoea depletes total-body potassium and the deficit is often larger than the plasma level suggests. [1] [2]
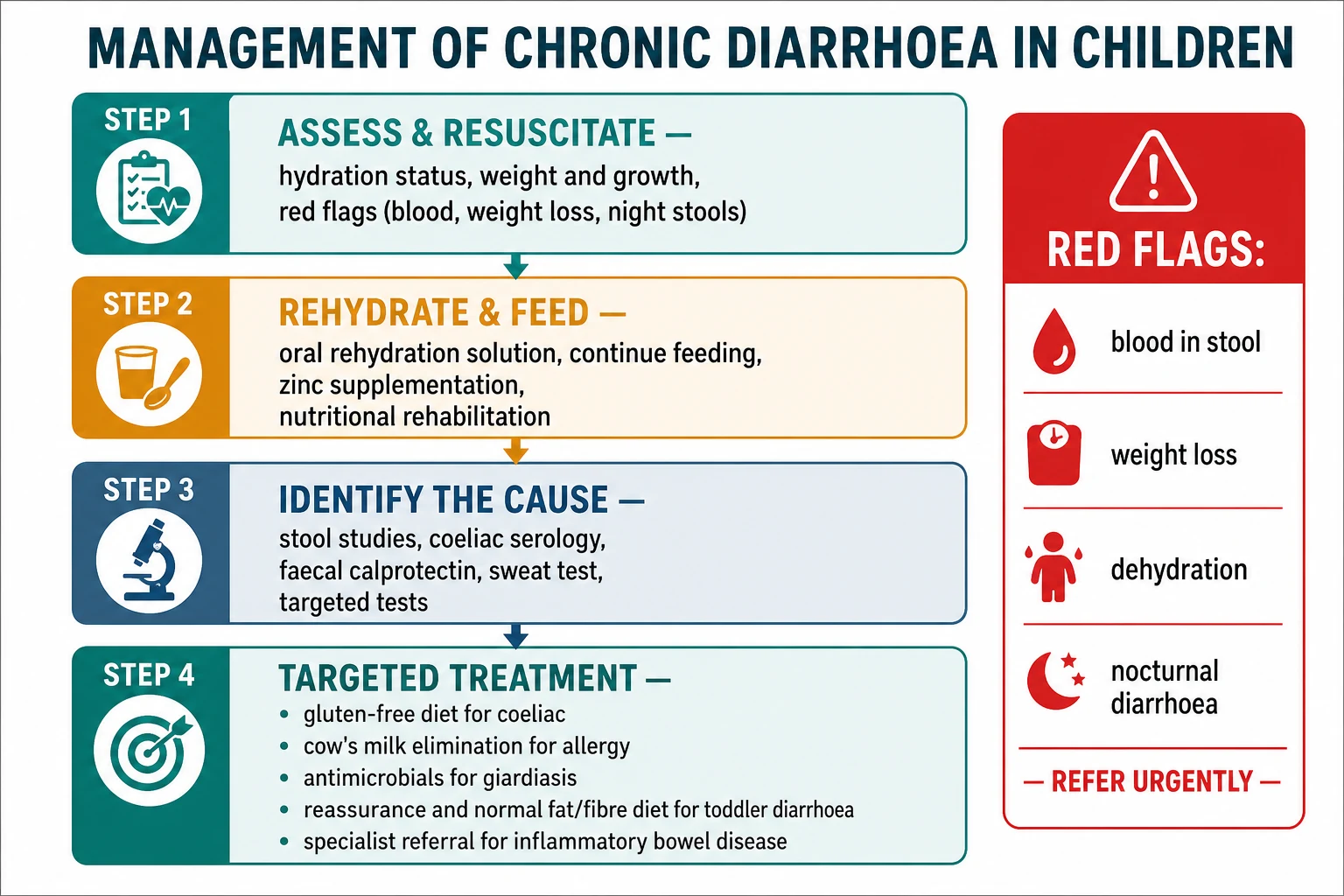
Rehydration and continued feeding are the two pillars, and they work together. Oral rehydration solution corrects and prevents dehydration and is the first-line fluid; the child who cannot tolerate oral or nasogastric fluids, or who is shocked, needs intravenous resuscitation. Feeding is continued and never withheld, because the malnourished gut heals only when it is fed and starvation deepens the mucosal injury that perpetuates the diarrhoea. In the malnourished child, cautious refeeding with attention to the refeeding syndrome and to micronutrients is central. [1] [9]
Zinc (persistent and acute diarrhoea in children)
Loading dose
10 mg elemental zinc daily for infants under 6 months
Maintenance dose
20 mg elemental zinc daily for 10–14 days for children 6 months and older
Zinc supplementation is the specific adjunct with the best evidence in persistent watery diarrhoea. A 2024 systematic review and meta-analysis confirmed that zinc reduces the duration and severity of acute and persistent watery diarrhoea in children and lowers the risk of recurrence, and it is a World Health Organization-endorsed part of the management package alongside oral rehydration and continued feeding, most strongly in low- and middle-income settings where deficiency is prevalent. [12]
Immediate management of the acutely unwell child with persistent diarrhoea
Assess ABC, hydration and nutritional status; send electrolytes, glucose, a blood gas and a septic screen if unwell
Correct dehydration with oral rehydration solution, or intravenous fluids if shocked or intolerant
Replace potassium carefully — total-body depletion exceeds the plasma level in chronic diarrhoea
Continue feeding; never starve the gut, and watch for refeeding syndrome in the malnourished child
Give zinc (10 mg under 6 months, 20 mg from 6 months) for 10 to 14 days as an adjunct
Correct micronutrient deficiencies and treat any concurrent infection
Escalate the malnourished or the birth-onset infant to specialist care early
Management — Definitive & Stepwise
Definitive management is cause-specific, and the whole stepwise approach converges on naming the mechanism and treating it. For toddler's diarrhoea the treatment is dietary and reassuring: normalise the intake by cutting excessive fruit juice, fructose and sorbitol, ensure an adequate dietary fat intake (the low-fat, high-fluid pattern many families adopt actually worsens it), and provide firm reassurance that the child is well and will grow out of it, usually by school age. No drugs are needed and antidiarrhoeals are avoided. [4] [5]
For coeliac disease the treatment is a strict, lifelong gluten-free diet, which resolves the symptoms, heals the mucosa and restores growth, delivered with dietitian support and monitored by falling antibody titres and by growth. For cow's milk protein allergy the treatment is elimination of cow's milk protein — maternal dietary exclusion in the breastfed infant, or an extensively hydrolysed (or, if that fails, an amino-acid-based) formula in the formula-fed infant — with a planned reintroduction to confirm the diagnosis and to detect the development of tolerance, which is usual by early childhood. [6] [8]
For giardiasis the treatment is an antimicrobial such as metronidazole or tinidazole; for post-enteritis lactose malabsorption a temporary lactose-reduced feed while the mucosa recovers; and for inflammatory bowel disease a specialist, staged regimen — exclusive enteral nutrition or corticosteroids to induce remission in Crohn disease, aminosalicylates and immunomodulators or biologics to maintain it, tailored to disease location and severity under the revised Porto framework. The congenital diarrhoeal disorders require specialist management that may include parenteral nutrition and, in some, intestinal transplantation, guided by the specific genetic defect. [7] [10]
[6] [7]The no-biopsy pathway for coeliac disease — the detail examiners probe
The ESPGHAN 2020 guideline allows coeliac disease to be diagnosed without a duodenal biopsy in a child with symptoms when the immunoglobulin A anti-tissue-transglutaminase antibody is at or above ten times the upper limit of normal and a separate blood sample shows positive endomysial antibody, with a normal total immunoglobulin A confirming the anti-transglutaminase result is valid. Human leukocyte antigen typing and symptoms are no longer required for the no-biopsy route in the 2020 revision. The critical practical rule is that all serology must be taken while the child is still eating gluten, because a gluten-free diet normalises the antibodies and makes the diagnosis impossible to confirm. [6]
Specific Subtypes & Scenarios
Toddler's diarrhoea is the scenario an examiner most often uses to test judgement, because the skill is to make a positive clinical diagnosis and resist over-investigation. The thriving one-to-three-year-old with loose stools containing undigested food, worse as the day goes on, with normal growth and no red flags, needs a dietary review and reassurance rather than a battery of tests. The frequent contributor is excessive fruit juice, whose fructose and sorbitol overwhelm absorptive capacity and draw water into the colon; reducing it, and correcting the counterproductive low-fat diet, usually settles the stools. [4] [5]
Cow's milk protein allergy is the infant scenario. The non-IgE-mediated form presents with chronic diarrhoea, blood and mucus in the stool of an otherwise well, often breastfed infant, or with vomiting, eczema and faltering growth; the diagnosis is confirmed by resolution on elimination and recurrence on a supervised reintroduction. The BSACI guideline sets out the diagnostic and management pathway, including the choice between an extensively hydrolysed and an amino-acid formula and the timing of reintroduction, with tolerance developing in most children by early childhood. [8]
Inflammatory bowel disease is the older-child scenario and the one where delay causes harm. Bloody diarrhoea, abdominal pain, weight loss, nocturnal symptoms, perianal disease and raised faecal calprotectin and inflammatory markers should prompt prompt paediatric gastroenterology referral for diagnosis under the revised Porto criteria, which require ileocolonoscopy and upper endoscopy with multiple biopsies plus small-bowel imaging. Very-early-onset inflammatory bowel disease under six years of age carries a higher likelihood of an underlying monogenic immune defect and warrants immunological and genetic evaluation. [7]
Across Australia, New Zealand and the United Kingdom, the child with chronic diarrhoea and red flags is worked up in primary care with coeliac serology, faecal calprotectin, stool studies and bloods, and referred to paediatric gastroenterology for endoscopy where inflammation or malabsorption is confirmed. Rural, remote and Indigenous children face longer distances to endoscopy and a higher burden of infection and undernutrition, so shared-care pathways and telehealth support the local team. In low- and middle-income settings the World Health Organization package of oral rehydration, continued feeding and zinc is the backbone of persistent-diarrhoea care, where the priority is to break the malnutrition-infection cycle. [9] [12]
Complications & Pitfalls
The dominant complication of persistent and chronic diarrhoea is its effect on nutrition and growth. Ongoing malabsorption and enteric protein loss produce weight loss, faltering linear growth and stunting, micronutrient deficiencies (iron, zinc, folate, vitamin B12 and the fat-soluble vitamins), and, in the malnourished child, a self-reinforcing cycle of malabsorption, immune impairment and repeated infection that carries real mortality in low-resource settings. Dehydration and electrolyte disturbance are the acute complications, particularly in the secretory diarrhoeas of infancy. [9] [1]
The pitfalls are mainly diagnostic. The first is over-investigating the thriving toddler, subjecting a well child to unnecessary tests when the history is diagnostic of toddler's diarrhoea. The second is the mirror error of under-investigating the child with red flags, reassuring away blood, weight loss or nocturnal diarrhoea as "just a tummy bug" and delaying the diagnosis of inflammatory bowel disease or coeliac disease. The third is testing coeliac serology after gluten has already been withdrawn, which normalises the antibodies and forces a gluten challenge to reach a diagnosis. [6] [1]
Prognosis & Disposition
The prognosis depends almost entirely on the cause, and for the common diagnoses it is excellent. Toddler's diarrhoea is self-limiting and resolves by school age with no long-term consequence. Coeliac disease responds completely to a lifelong gluten-free diet, with resolution of symptoms, mucosal healing and catch-up growth. Cow's milk protein allergy is usually outgrown by early childhood. Giardiasis and post-enteritis diarrhoea resolve with treatment and time. The child who is thriving and has a functional or dietary diagnosis needs reassurance and follow-up rather than escalation. [4] [6]
The prognosis is more guarded for the chronic organic diseases and for the malnourished child. Inflammatory bowel disease is a lifelong relapsing-remitting condition requiring ongoing specialist care, with the goals of mucosal healing, normal growth and pubertal progression, and transition to adult services in adolescence. The congenital diarrhoeal disorders range from manageable with dietary or medical therapy to lifelong intestinal failure requiring parenteral nutrition and, in some, transplantation. In low-resource settings persistent diarrhoea in the malnourished child carries significant mortality, which the oral-rehydration, feeding and zinc package is designed to reduce. [10] [9]
Disposition follows the diagnosis and the growth. The thriving child with a dietary or functional diagnosis is managed in primary care with dietary advice and a safety net. The child with faltering growth, red flags or an organic diagnosis is referred to general paediatrics or paediatric gastroenterology; the child with inflammatory bowel disease, a congenital enteropathy or intestinal failure is managed in a tertiary centre with dietetic, surgical and, where needed, nutrition-support and transplant services. The malnourished child needs structured nutritional rehabilitation and close monitoring of weight and micronutrients. [7] [1]
Special Populations
The young infant is the first special population, because diarrhoea from the first days of life carries a different and more urgent differential. A congenital diarrhoeal disorder — a defect of an ion transporter, an enterocyte structural protein, an enteroendocrine pathway or the enteric immune system — can be rapidly life-threatening through dehydration and electrolyte loss, and it needs urgent electrolyte correction and specialist genetic evaluation. Consanguinity and a family history of infant deaths or diarrhoea raise the suspicion, and early molecular diagnosis increasingly guides prognosis and management. [10] [2]
The immunocompromised child is the second. Primary immunodeficiency can present with chronic diarrhoea, and very-early-onset inflammatory bowel disease under six years is more likely than later-onset disease to reflect a monogenic immune defect, so immunological and genetic evaluation is part of the workup at this age. Children with immunodeficiency or on immunosuppression are also susceptible to opportunistic and persistent enteric infections that would clear quickly in an immunocompetent child. [7] [10]
The child in a disadvantaged or a low-resource setting is the third. Poor sanitation, repeated enteric infection and undernutrition combine to produce environmental enteric dysfunction, a subclinical malabsorptive enteropathy that drives stunting and blunts oral vaccine responses even without overt diarrhoea. Indigenous, remote and refugee children carry a higher burden of both infection and undernutrition, and their care depends on culturally safe, shared-care pathways, attention to the social determinants, and the World Health Organization package of rehydration, feeding and zinc. [9] [12]
Evidence, Guidelines & Regional Differences
The evidence base is anchored on a small set of guidelines and reviews. The Zella and Israel review and the Thiagarajah review of chronic diarrhoea in infants provide the modern diagnostic framework — the duration definitions, the osmotic-secretory-inflammatory-dysmotility mechanisms, and the stepwise, stool-directed workup — and remain the references for the syndrome as a whole. Field's work on intestinal ion transport underpins the secretion-versus-absorption physiology that separates osmotic from secretory diarrhoea. [1] [2] [3]
The disease-specific guidelines define the diagnostic pathways. The ESPGHAN 2020 coeliac guideline established the antibody-based no-biopsy route for the symptomatic child with a high anti-transglutaminase titre and positive endomysial antibody, and reaffirmed that serology must be taken on a gluten-containing diet. The revised Porto criteria standardised the diagnosis of paediatric inflammatory bowel disease around ileocolonoscopy, upper endoscopy and small-bowel imaging. The BSACI guideline set out the diagnosis and management of cow's milk allergy, including the formula choice and the reintroduction plan. [6] [7] [8]
The management evidence and the regional differences converge on nutrition. The 2024 zinc meta-analysis confirmed the benefit of zinc in persistent watery diarrhoea, and the World Health Organization package of oral rehydration, continued feeding and zinc is the backbone of persistent-diarrhoea care in low- and middle-income settings, where the Keusch and colleagues account of environmental enteric dysfunction links chronic gut injury to stunting. The Lo Vecchio cohort of prolonged diarrhoea highlighted the multifactorial aetiology and the role of the microbiota. Across all settings the strategy is uniform in principle: define the duration and the mechanism, separate the thriving from the failing child, feed the gut, and treat the specific cause. [12] [9] [11]
Exam Pearls
Workup of chronic diarrhoea — 'GROWTH'
References
- [1]Zella GC; Israel EJ Chronic diarrhea in children. Pediatr Rev, 2012.PMID 22550264
- [2]Thiagarajah JR; Kamin DS; Acra S; Goldsmith JD; Roland JT; Lencer WI Advances in Evaluation of Chronic Diarrhea in Infants. Gastroenterology, 2018.PMID 29654747
- [3]Field M Intestinal ion transport and the pathophysiology of diarrhea. J Clin Invest, 2003.PMID 12671039
- [4]Kneepkens CM; Hoekstra JH Chronic nonspecific diarrhea of childhood: pathophysiology and management. Pediatr Clin North Am, 1996.PMID 8614606
- [5]Dennison BA Fruit juice consumption by infants and children: a review. J Am Coll Nutr, 1996.PMID 8892177
- [6]Husby S; Koletzko S; Korponay-Szabó I; Kurppa K; Mearin ML; Ribes-Koninckx C European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J Pediatr Gastroenterol Nutr, 2020.PMID 31568151
- [7]Levine A; Koletzko S; Turner D; Escher JC; Cucchiara S; de Ridder L ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J Pediatr Gastroenterol Nutr, 2014.PMID 24231644
- [8]Luyt D; Ball H; Makwana N; Green MR; Bravin K; Nasser SM BSACI guideline for the diagnosis and management of cow's milk allergy. Clin Exp Allergy, 2014.PMID 24588904
- [9]Keusch GT; Denno DM; Black RE; Duggan C; Guerrant RL; Lavery JV Environmental enteric dysfunction: pathogenesis, diagnosis, and clinical consequences. Clin Infect Dis, 2014.PMID 25305288
- [10]Berni Canani R; Terrin G; Cardillo G; Tomaiuolo R; Castaldo G Congenital diarrheal disorders: improved understanding of gene defects is leading to advances in intestinal physiology and clinical management. J Pediatr Gastroenterol Nutr, 2010.PMID 20216094
- [11]Lo Vecchio A; Quitadamo P; Poeta M; Buccigrossi V; Siani P; Cioffi V Aetiology, risk factors and microbiota composition in children with prolonged diarrhoea: A prospective case-controlled cohort study. Acta Paediatr, 2024.PMID 38129967
- [12]Ali AA; Naqvi SK; Hasnain Z; Zubairi MBA; Sharif A; Salam RA Zinc supplementation for acute and persistent watery diarrhoea in children: A systematic review and meta-analysis. J Glob Health, 2024.PMID 39641338